
Abstract
The human gastrointestinal (GI) tract contains communities of microbes (bacteria, fungi, viruses) that vary by anatomic location and impact human health. Microbial communities differ in composition based on age, diet, and location in the gastrointestinal tract. Differences in microbial composition have been associated with chronic disease states. In terms of function, microbial metabolites provide key signals that help maintain healthy human physiology. Alterations of the healthy gastrointestinal microbiome have been linked to the development of various disease states including inflammatory bowel disease, diabetes, and colorectal cancer. While the definition of a healthy GI microbiome cannot be precisely identified, features of a healthy gut microbiome include relatively greater biodiversity and relative abundances of specific phyla and genera. Microbes with desirable functional profiles for the human host have been identified, in addition to specific metabolic features of the microbiome. This article reviews the composition and function of the healthy human GI microbiome, including the relative abundances of different bacterial taxa and the specific metabolic pathways and classes of microbial metabolites contributing to human health and disease prevention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.

Wenly Ruan

Melinda A. Engevik

Jennifer K. Spinler

James Versalovic
Introduction
The healthy human microbiome consists of 30-plus trillion microorganisms per person including mostly bacteria, viruses (bacteriophages and human viruses), and yeast [1]. Human microbes reside on the skin, in the oral cavity, and in the gastrointestinal (GI), respiratory, and genitourinary tracts, accounting for 1–3% of our total body weight. The human GI tract contains relatively rich and complex microbial communities in healthy individuals. Intestinal microbes harbor genes that encode for thousands of microbial enzymes and metabolites [2, 3]. These metabolic pathways and microbial compounds facilitate digestion and assimilation of dietary nutrients, while fostering maturation and proper function of the immune and nervous systems.
The Human Microbiome Project (HMP) and the Metagenomics of the Human Intestinal Tract (MetaHIT) initiatives were the first large-scale microbiome projects defining composition and function of the healthy human microbiome [4, 5]. These endeavors provided the foundation for understanding of the physiology and functional properties of host-associated microbial communities. With the advent of new technologies like next-generation sequencing, whole-genome shotgun sequencing, global metabolomics, and advanced computational strategies along with humanized animal models and culture-based human organoid systems, understanding of the microbiome is rapidly progressing [6].
The GI microbiome is a dynamic and functional interface between the external environment, food, and the human body [7]. Distinct luminal- and mucus-associated ecosystems found throughout the length of the GI tract are influenced by various factors including age, diet, antibiotic/medication ingestion, and other exposures. Alterations in GI microbiome diversity have been attributed to disease phenotypes such as colorectal cancer, inflammatory bowel disease (IBD), irritable bowel syndrome (IBS), and diabetes [8,9,10,11,12]. Here we review how GI microbiome composition and function affect human health and consider future investigations to further elucidate the healthy human GI microbiome.
Characteristics of a Healthy GI Microbiome
The microbiome is dynamic and changes spatially and temporally, and in relation to an individual’s health status. Microbes colonize the human body and shift in composition as humans age, with a gradual increase in microbial diversity during childhood and relative stabilization during adolescence and adulthood [13]. Breastfeeding seems to play a significant role in the formation of early-life microbiome with a predominance of Bifidobacterium and Bacteroides species in breastfed infants [14, 15]. Breastfeeding appears to have long-term effects on the microbiome and its effects on the immune system and GI tract [16, 17]. The childhood/adolescent microbiome is enriched in Bifidobacterium spp., Faecalibacterium spp., and members of the Lachnospiraceae family [13]. Interestingly, children’s gut communities were enriched in functions that may support ongoing development. In contrast to infant and childhood microbiomes, the adult microbiome is more stable and is shaped more by environment than by genetics. As humans age, microbial diversity increases steadily in healthy individuals [17,18,19]. Decreased microbial diversity has been associated with various disease states [20,21,22].
Much of the initial focus on the microbiome has been centered around the understanding of its impact in disease leading to the concept of dysbiosis or shifts in the normal gut microbiome structure. Shifts in the microbiome are influenced by diet, antibiotics, socioeconomic status, and geography [23, 24]. However, it is still unclear whether these changes in microbiome composition are a cause or consequence of epithelial function alteration and disease. One of the features of a healthy microbiome is its resilience, its ability to return to an equilibrium state, and resistance to perturbations. A significant degree of interpersonal diversity even in the absence of disease in the human microbiome makes defining an idealized community of specific microbes difficult [25, 26]. The variation of the microbiome between the individuals is thought to be driven by ecological processes that shape various ecosystems [27, 28]. Rather than an idealized community of microbes, a healthy microbiome can be characterized by a shared set of metabolic modules or functions [18, 29].
Structural Composition of the GI Microbiome
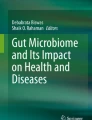
The human GI tract is a complex system that begins at the esophagus and ends at the anus with most data obtained to date from the distal colonic microbiota due to the practical considerations of specimen collection. Important physiologic conditions like pH, bile content, and transit time vary along the GI tract and contribute to distinct microbial communities inhabiting the upper and lower GI tract [30]. In this section, we review what is known about the composition of healthy bacterial communities in the oral cavity, esophagus, stomach, small intestine, and colon (Fig. 1).

Human microbiome composition varies by location in the GI tract. Predominant bacterial genera in the oral cavity, esophagus, stomach, small intestine, and colon are delineated in this figure
Oral Cavity
The oral cavity is comprised of several microbial environments including the tonsils, teeth, gums, tongue, cheeks, hard and soft palates. It is the opening to the GI tract where food enters and is mixed with saliva. More than 1000 taxa have been found in the oral cavity so it has its own database known as the Human Oral Microbiome Database [31]. Six major phyla comprise 96% of the taxa including Firmicutes, Bacteroidetes, Proteobacteria, Actinobacteria, Spirochaetes, and Fusobacteria [31]. In saliva of healthy patients, the predominant genera are Gemella, Veillonella, Neisseria, Fusobacterium, Streptococcus, Prevotella, Pseudomonas, and Actinomyces [32]. Different locations within the oral cavity have varying degrees of biological diversity [33].
Esophagus
Food is transported down the esophagus from the oral cavity to the stomach. Similar to the oral cavity, the most abundant bacteria in the human esophagus belong to the phylum Firmicutes and the genus Streptococcus [34], likely derived from the oral cavity [30, 35]. Shotgun sequencing has revealed three distinct community types in the esophagus of healthy subjects [36]. Communities are dominated either by Streptococcus (Streptococcus mitis/oralis/pneumoniae), Prevotella (Prevotella melaninogenica and Prevotella pallens) and Veillonella, or Haemophilus (Haemophilus parainfluenzae) and Rothia (Rothia mucilaginosa). Similar to other GI sites, age contributes to the structure of the esophageal microbiome, but interestingly composition appears to be independent of proton-pump inhibitor use or gender [36]. Overall, there are limited studies to suggest altered microbiome composition associated with esophageal diseases so further studies are necessary to better elucidate disease pathogenesis.
Stomach
The stomach is the first digestive organ of the body. It contains proteolytic enzymes and gastric acid that processes the food that is ingested. Due to its acidic environment, the growth of many bacteria is inhibited. The harsh environment is thought to serve as a protective mechanism against pathogens. Despite the low pH, a diverse microbiota can be found in the stomach. The genera commonly found in the corpus and antrum include Bacillales incertae sedis, Streptococcaceae, Enterobacteriaceae, Leptotrichiaceae, Veillonellaceae, and Pseudomonadaceae [32, 35]. Individuals can be divided into the two major groups: groups with and without Helicobacter pylori. In patients with abundant H. pylori, a greater number of bacteria belonged to the phylum Proteobacteria and the gastric microbiomes yielded lower overall alpha diversity [32, 37]. When looking at the gut microbiome of individuals with H. pylori, there is increased abundance of Succinivibrio, Coriobacteriaceae, Enterococcaceae, and Rikenellaceae [38].
Small Intestine
The small intestine consists of the duodenum, jejunum, and the ileum and is the location where most nutrient digestion and absorption occur. The duodenum is the portion of the small intestine where the food bolus enters from the stomach, and bile salts from the gallbladder along with pancreatic enzymes start digestion. The intestinal epithelium of the jejunum and ileum is then responsible for nutrient absorption. Metabolism favors simple sugar and amino acid metabolism, so the small intestine is dominated by rapidly dividing facultative anaerobes such as Proteobacteria and Lactobacillales [39]. This finding was supported by studies analyzing jejunal samples obtained via enteroscopy. One study showed that Streptococcus, Prevotella, Veillonella, Fusobacterium, Escherichia, Klebsiella, and Citrobacter were abundant, whereas extreme anaerobes like Alistipes, Ruminococcus, and Faecalibacterium were not present [40]. Also, when the jejunum and ileum contents from three individuals were analyzed, the most common communities consisted of streptococci, lactobacilli, Gammaproteobacteria, the Enterococcus group, and the Bacteroides group [41]. As the small intestine progresses distally in the ileum, the microbial composition becomes more complex and approaches that of the colon in terms of diversity and richness. Vaspapolli et al. found that the duodenum harbored similar genera as the stomach (Bacillales incertae sedis, Streptococcaceae, Enterobacteraceae, Leptorichiaeceae, Veillonellaceae, and Pseudomonadaceae), while the terminal ileum exhibited a composition closer to that of the colon (Clostridiaceae, Lachnospiraceae, Peptostreptococcaceae, Ruminococcaceae, Enterobacteriaceae, and Bacteroidaceae) [32]. These findings demonstrate unique microbial compositional profiles along the length of the small intestine.
Colon
The colon consists of the cecum, ascending, transverse, descending, and sigmoid colon, as well as the rectum. It is the location where water and minerals are absorbed and complex carbohydrate fermentation occurs [42]. Complex foods that have not been digested by the host reach the colon and feed the colonic microbiota. The healthy human colon yields a relatively rich abundance of microbes in the colon, and these communities are highly diverse. The predominant colonic bacterial phyla in the healthy human are Bacteroidetes, Firmicutes, Verrucomicrobia, Proteobacteria, and Actinobacteria [35]. Few differences have been observed between the ascending and descending colon in terms of microbiome composition, with families from the colon including Clostridiaceae, Lachnospiraceae, and Bacteroidaceae dominating the microbiome structure [32].
A major difference between the small and large intestine is the structure of the mucus layer. In the colon, the mucus forms a stratified layer that is more defined than in the small intestine. The colonic mucus layer consists of an inner mucus layer, physically excludes bacteria, and contains immune effectors that target the microbiota [43]. In contrast, the outer mucus layer is loose and serves as a colonization site for numerous microbes. Due to the structural makeup of the colon, it has been observed that bacteria are organized along the transverse axis of the colon, from the lumen to the mucosa. Microbes that prioritize dietary starches and nutrients reside within the colonic lumen. Organisms that can utilize mucin such as Akkermansia, Ruminococcus, and some Bacteroides species reside within the outer intestinal mucus layer [44,45,46,47]. In addition to nutrient sources, oxygen gradients exist from the intestinal lumen to the mucosa as well as moving down the colon, with consequent effects on microbial composition of the colon. For example, Proteobacteria and Actinobacteria phyla are found closer to the rectum than feces as a result [48].
Several studies have attempted to define a human intestinal core microbiota. Longitudinal analysis and cross-sectional comparisons of fecal 16S rRNA have revealed that a significant fraction of bacterial phylotypes is continuously present and thus comprises a stable microbial core [49,50,51,52,53,54]. These core microbes include Bacteroides, Eubacterium, Faecalibacterium, Alistipes, Ruminococcus, Clostridium, Roseburia, and Blautia; with Faecalibacterium prausnitzii, Oscillospira guillermondii, and Ruminococcus obeum as the top three taxa shared by all adults [55].
Alterations of the colonic microbiota and breaches in the colonic structure have been associated with various disease states. Recent microbiome genome-wide association studies revealed multiple alterations in gut microbiome composition in metabolic disorders and disorders of immunity [56]. Inflammatory bowel disease (IBD) is characterized by immune activation and disrupted intestinal epithelial mucosal barrier function, which can culminate in the inappropriate immune activation against commensal bacteria. Affected sites in IBD are locations with relatively greater bacterial densities such as the distal ileum and cecum. In addition, mucus-degrading bacteria were increased in relative abundance in IBD patients leading to the an increase in available substrates to sustain mucosa-associated bacteria during colitis [57], and large increases in Ruminococcus gnavus have been noted in mucosal samples of IBD patients [56]. In colorectal cancer patients, Coriobacteriaceae were found in greater abundance in tumors [8]. Obesity is associated with lower abundances of Christensenella minuta, Akkermansia muciniphila, and Methanobrevibacter smithii and an overabundance of Blautia [56]. The colonic microbiome plays a pivotal role in maintaining intestinal epithelial homeostasis and overall human health.
Microbial Functions in the GI Tract
Although microbiome structure varies among healthy individuals, microbial functions are well-conserved [32]. One important function of the microbiome is the generation of microbial metabolites which influence both microbes and host. This section details the functional capacity of the GI microbiota and specifically touches on microbial-derived metabolites that modulate both intra- (microbe–microbe) and inter-kingdom (microbe-host) interactions that impact human health (Fig. 2).

Microbial metabolites produced in the gastrointestinal tract have diverse functions. The gastrointestinal microbiome can modulate both intra- (microbe–microbe) and inter-kingdom (microbe-host) interactions that can influence human health. Bacteria are involved in quorum sensing and can release bacteriocins, hydrogen peroxide, and lactic acid, which yield effects on the gut microbiome and pathogens. In addition, bacteria can produce gamma-aminobutyric acid (GABA), tryptophan metabolites, histamine, polyamines, serpins, lactocepin, vitamins, short chain fatty acids (SCFA), long chain fatty acids (LCFA), and outer membrane vesicles (OMVs), which can have effects on the human host epithelium, immune cells, mesenchyme, and enteric neurons
Microbial Metabolites
Secreted microbial compounds can target the microbiome by acting as signaling molecules for inter-bacterial communication. These molecules, known as quorum sensors, can influence bacterial homeostasis, growth, spore formation, programmed cell death, virulence, and biofilm formation [58,59,60,61,62]. Quorum sensing offers advantages to biofilm communities by allowing them to adapt to environmental changes [58,59,60, 63]. Quorum sensing compounds are grouped into three classes: (1) LuxI/LuxR-type; (2) oligopeptide-two-component-type; and (3) luxS-encoded autoinducer 2 (AI-2) quorum sensing [58]. In intestinal communities, the levels of the quorum sensing compound AI-2 were associated with relatively decreased abundance in Bacteroidetes and increased abundance in Firmicutes [64]. Additionally, AI-2 also promoted Firmicutes that encoded a LuxS homolog, indicating that a positive feedback loop might exist within the microbiota, whereby AI-2 signaling and downstream responses drive increases in abundance of the AI-2 producers, which then further increases signal levels and amplifies the response throughout the community.
While quorum sensing compounds typically encourage bacterial growth of similar microbes, bacteria also secrete compounds that inhibit the growth of competitors. These antibiotic compounds can be proteins (bacteriocins) or small molecules (lactic acid, hydrogen peroxide (H2O2), and reactive aldehydes) and effectively enhance host health through colonization resistance [65, 66]. Bacteriocins target phosphate groups on bacterial cell membranes, deplete the transmembrane potential (Δѱ), and form membrane pores. These events result in membrane disruption, cellular leakage, and cell death [67,68,69]. Interestingly, bacteriocins have a synergistic effect with lactic acid, produced commonly by probiotics, and exhibit greater antibacterial activity at lower pH. Lactic acid bacteria (LAB) produce lactic acid as an end product of glucose fermentation [70], which (1) reduces local pH and suppresses colonization and proliferation of potential pathogens, and (2) can penetrate the bacterial cytoplasmic membrane, lower the intracellular pH, and suppress the electron transport system, leading to oxidative stress, DNA damage, and cell death [71,72,73,74]. Lactic acid also works synergistically with H2O2 to inhibit pathogens and shape microbial communities [71, 75, 76] by damaging bacterial nucleic acids and preventing chromosomal replication [77,78,79,80]. Apart from intra-kingdom interactions, L-lactic acid can directly impact host health by suppressing pro-inflammatory responses of immune cells [81]. An isomeric mixture of 3-hydroxypropionaldehyde (3-HPA) also known as reuterin is produced by LAB [82, 83] and inhibits enteric pathogen growth [84,85,86]. Reuterin is the by-product of glycerol fermentation [87, 88], which is hypothesized to stem from the breakdown of a prevalent bacterial membrane phospholipid phosphatidylethanolamine into glycerol and ethanolamine, suggesting that glycerol is abundant in the GI tract. Like lactic acid, reuterin also mediates inter-kingdom interactions; recent studies have linked reuterin production with iron homeostasis in the host [89, 90].
Microbial Metabolites/Compounds and Their Impact on Host Processes
Bacterial metabolites can also mediate host processes and functionally complement host metabolic capabilities. Certain microbes can generate biologically active compounds including but not limited to, gamma-aminobutyric acid (GABA), tryptophan metabolites, polyamines, and histamine [91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107]. Microbial neuromodulators like GABA may participate in communication with the enteric and central nervous systems, while microbial-derived immunomodulators like histamine interact with intestinal immune cells. Serpins, another example of microbial-derived immunomodulators, are similar to eukaryotic serine protease inhibitors which suppress inflammatory responses by inhibiting elastase activity [108,109,110,111,112]. Similarly, lactocepins are bacterial enzymes which can degrade pro-inflammatory signals [113,114,115]. For example, Lactobacillus-secreted lactocepin selectively degrades lymphocyte recruiting chemokine IP-10, I-TAC and eotaxin, thereby suppressing pro-inflammatory signaling cascades [116, 117].
Short-chain fatty acids (SCFAs) implicated in immune regulation, pH regulation, sodium and water absorption, and mucus secretion [66, 118, 119] are an important microbial by-product of complex carbohydrate fermentation in the intestine. The most abundant and well-studied SCFAs are acetate, propionate, and butyrate; however, the intestinal composition of SCFAs is contingent on microbial composition, diet, and intestinal pH [120,121,122,123]. SCFAs are absorbed by host epithelial cells and diminished in concentration from the proximal to the distal colon [124,125,126,127,128]. In addition to epithelial cells, SCFA transporters are found on immune, enteroendocrine, kidney and brain cells [127,128,129,130,131,132,133,134,135,136,137] reflecting the diverse effects of SCFAs on host physiology. In addition to SCFAs, microbes can produce long-chain fatty acids (LCFAs) [138,139,140,141] known to reduce hepatic triacylglycerols and inhibit atherosclerosis [142, 143].
Select intestinal microbes are able to produce vitamins, essential nutrients required for growth and immune function, which are primarily absorbed in the colon [144,145,146,147,148,149,150,151]. Genomes of gut microbes yield enzymatic pathways involved in vitamin synthesis for eight different B complex vitamins: biotin (B7), cobalamin (B12), folate (B9), niacin (B3), pantothenic acid (B5), pyridoxine (B6), and riboflavin (B2) [152]. Metagenomic studies have also indicated the enrichment of microbial enzymatic pathways for vitamin precursors in the gut and have emphasized the production of vitamins through coordinated bacterial cross-feeding [153]. Interestingly, recent studies have linked vitamin deficiencies with antibiotic-diminished gut microbiota, solidifying a distinct contribution of microbial vitamins to host health that differs from vitamin supplementation in the diet [154]. Key modifications of microbial vitamins like mono- and polyglutamylated folate influence their absorption and function in the host [155,156,157], which further supports the significance of microbial micronutrients in host health.
Outer membrane vesicles (OMVs) are another key immunomodulatory factor produced by our gut microbiota [158,159,160]. OMVs typically harbor a number of soluble proteins which can signal to multiple cell types, including cells in the innate and adaptive immune systems [161]. Bacteroides fragilis OMV delivery of polysaccharide capsular antigen (PSA) has been widely studied for its immunomodulatory effects. B.fragilis OMVs were found to modulate CD4+ T cell homeostasis and cytokine production [162] and directly modulate dendritic cells (DCs) [163, 164]. These immunomodulatory functions have been shown to benefit intestinal inflammation [165] and CNS inflammation [166,167,168].
Conclusions
The human gastrointestinal microbiome is essential to maintaining human health. Despite technological advances in human microbiome research, the individual composition, functional features, and interactions between human host and microbes remain to be elucidated. These studies emphasize the importance of a healthy GI microbiome and the key roles of bacterial metabolites in fine-tuning the host response. Additional studies may provide more precise etiologic explanations for the interactions between the host and human microbiome. As we begin to understand the composition and function of the healthy microbiome, we may be able to identify individual species and strains which can be tailored for specific targets of interest.
Abbreviations
- GI:
-
Gastrointestinal
- HMP:
-
Human Microbiome Project
- MetaHIT:
-
Metagenomics of the Human Intestinal Tract
- IBD:
-
Inflammatory bowel disease
References
Sender R, Fuchs S, Milo R. Revised estimates for the number of human and bacteria cells in the body. PLoS Biol. 2016;14:e1002533.
Bull MJ, Plummer NT. Part 1: The human gut microbiome in health and disease. Integr Med. 2014;13:17–22.
Rath CM, Dorrestein PC. The bacterial chemical repertoire mediates metabolic exchange within gut microbiomes. Curr Opin Microbiol. 2012;15:147–154.
Turnbaugh PJ, Ley RE, Hamady M, Fraser-Liggett CM, Knight R, Gordon JI. The human microbiome project. Nature. 2007;449:804–810.
Ehrlich SD. MetaHIT: the European Union Project on metagenomics of the human intestinal tract. In: Nelson KE, ed. Metagenomics of the Human Body, City. Springer: New York; 2011:307–316.
Arnold JW, Roach J, Azcarate-Peril MA. Emerging technologies for gut microbiome research. Trends Microbiol. 2016;24:887–901.
Flint HJ. The impact of nutrition on the human microbiome. Nutr Rev. 2012;70:S10–S13.
Marchesi JR, Dutilh BE, Hall N, et al. Towards the human colorectal cancer microbiome. PLoS ONE. 2011;6:e20447.
Halfvarson J, Brislawn CJ, Lamendella R, et al. Dynamics of the human gut microbiome in inflammatory bowel disease. Nat Microbiol. 2017;2:17004.
Chong PP, Chin VK, Looi CY, Wong WF, Madhavan P, Yong VC. The microbiome and irritable bowel syndrome: a review on the pathophysiology. Curr Res Future Ther Front Microbiol. 2019;10:1136.
Chumpitazi BP, Cope JL, Hollister EB, et al. Randomised clinical trial: gut microbiome biomarkers are associated with clinical response to a low FODMAP diet in children with the irritable bowel syndrome. Aliment Pharmacol Ther. 2015;42:418–427.
Sharma S, Tripathi P. Gut microbiome and type 2 diabetes: where we are and where to go? J Nutrit Biochem. 2019;63:101–108.
Hollister EB, Riehle K, Luna RA, et al. Structure and function of the healthy pre-adolescent pediatric gut microbiome. Microbiome. 2015;3:36.
Marcobal A, Sonnenburg JL. Human milk oligosaccharide consumption by intestinal microbiota. Clin Microbiol Infect. 2012;18:12–15.
Matamoros S, Gras-Leguen C, Le Vacon F, Potel G, de La Cochetiere MF. Development of intestinal microbiota in infants and its impact on health. Trends Microbiol. 2013;21:167–173.
Aagaard K, Petrosino J, Keitel W, et al. The Human Microbiome Project strategy for comprehensive sampling of the human microbiome and why it matters. FASEB J. 2013;27:1012–1022.
McBurney MI, Davis C, Fraser CM, et al. Establishing what constitutes a healthy human gut microbiome: state of the science, regulatory considerations, and future directions. J Nutr. 2019;149:1882–1895.
Lloyd-Price J, Abu-Ali G, Huttenhower C. The healthy human microbiome. Genome Med. 2016;8:51.
Lloyd-Price J, Mahurkar A, Rahnavard G, et al. Strains, functions and dynamics in the expanded Human Microbiome Project. Nature. 2017;550:61–66.
Dobbler PT, Procianoy RS, Mai V, et al. Low microbial diversity and abnormal microbial succession is associated with necrotizing enterocolitis in preterm infants. Front Microbiol. 2017;8:2243.
Ni J, Wu GD, Albenberg L, Tomov VT. Gut microbiota and IBD: causation or correlation? Nat Rev Gastroenterol Hepatol. 2017;14:573–584.
Ding RX, Goh WR, Wu RN, et al. Revisit gut microbiota and its impact on human health and disease. J Food Drug Anal. 2019;27:623–631.
Fragiadakis GK, Smits SA, Sonnenburg ED, et al. Links between environment, diet, and the hunter-gatherer microbiome. Gut Microbes. 2019;10:216–227.
Dethlefsen L, Huse S, Sogin ML, Relman DA. The pervasive effects of an antibiotic on the human gut microbiota, as revealed by deep 16S rRNA sequencing. PLoS Biol. 2008;6:e280.
Human Microbiome Project C. Structure, function and diversity of the healthy human microbiome. Nature. 2012;486:207–214.
Tuddenham S, Sears CL. The intestinal microbiome and health. Curr Opin Infect Dis. 2015;28:464–470.
Martinez I, Maldonado-Gomez MX, Gomes-Neto JC, et al. Experimental evaluation of the importance of colonization history in early-life gut microbiota assembly. Elife. 2018;7:e36521.
Rothschild D, Weissbrod O, Barkan E, et al. Environment dominates over host genetics in shaping human gut microbiota. Nature. 2018;555:210–215.
Backhed F, Fraser CM, Ringel Y, et al. Defining a healthy human gut microbiome: current concepts, future directions, and clinical applications. Cell Host Microbe. 2012;12:611–622.
Berg RD. The indigenous gastrointestinal microflora. Trends Microbiol. 1996;4:430–435.
Dewhirst FE, Chen T, Izard J, et al. The human oral microbiome. J Bacteriol. 2010;192:5002–5017.
Vasapolli R, Schutte K, Schulz C et al. Analysis of transcriptionally active bacteria throughout the gastrointestinal tract of healthy individuals. Gastroenterology. 2019.
Li K, Bihan M, Yooseph S, Methé BA. Analyses of the microbial diversity across the human microbiome. PloS One. 2012;7:e32118.
May M, Abrams JA. Emerging insights into the esophageal microbiome. Curr Treat Options Gastroenterol. 2018;16:72–85.
Hillman ET, Lu H, Yao T, Nakatsu CH. Microbial ecology along the gastrointestinal tract. Microbes Environ. 2017;32:300–313.
Deshpande NP, Riordan SM, Castano-Rodriguez N, Wilkins MR, Kaakoush NO. Signatures within the esophageal microbiome are associated with host genetics, age, and disease. Microbiome. 2018;6:227.
Bik EM, Eckburg PB, Gill SR, et al. Molecular analysis of the bacterial microbiota in the human stomach. Proc Natl Acad Sci US A. 2006;103:732–737.
Dash NR, Khoder G, Nada AM, Al Bataineh MT. Exploring the impact of Helicobacter pylori on gut microbiome composition. PloS One. 2019;14:e0218274.
Gu S, Chen D, Zhang JN, et al. Bacterial community mapping of the mouse gastrointestinal tract. PloS one. 2013;8:e74957.
Sundin OH, Mendoza-Ladd A, Zeng M, et al. The human jejunum has an endogenous microbiota that differs from those in the oral cavity and colon. BMC Microbiol. 2017;17:160.
Hayashi H, Takahashi R, Nishi T, Sakamoto M, Benno Y. Molecular analysis of jejunal, ileal, caecal and recto-sigmoidal human colonic microbiota using 16S rRNA gene libraries and terminal restriction fragment length polymorphism. J Med Microbiol. 2005;54:1093–1101.
Scheithauer TP, Dallinga-Thie GM, de Vos WM, Nieuwdorp M, van Raalte DH. Causality of small and large intestinal microbiota in weight regulation and insulin resistance. Mol Metab. 2016;5:759–770.
Johansson ME, Larsson JM, Hansson GC. The two mucus layers of colon are organized by the MUC2 mucin, whereas the outer layer is a legislator of host-microbial interactions. Proc Natl Acad Sci USA. 2011;108:4659–4665.
Tropini C, Earle KA, Huang KC, Sonnenburg JL. The gut microbiome: connecting spatial organization to function. Cell Host Microbe. 2017;21:433–442.
Berry D, Stecher B, Schintlmeister A, et al. Host-compound foraging by intestinal microbiota revealed by single-cell stable isotope probing. Proc Natl Acad Sci USA. 2013;110:4720–4725.
Crost EH, Tailford LE, Monestier M, et al. The mucin-degradation strategy of Ruminococcus gnavus: the importance of intramolecular trans-sialidases. Gut Microbes. 2016;7:302–312.
Yasuda K, Oh K, Ren B, et al. Biogeography of the intestinal mucosal and lumenal microbiome in the rhesus macaque. Cell Host Microbe. 2015;17:385–391.
Albenberg L, Esipova TV, Judge CP, et al. Correlation between intraluminal oxygen gradient and radial partitioning of intestinal microbiota. Gastroenterology. 2014;147:e1058.
Faith JJ, Guruge JL, Charbonneau M, et al. The long-term stability of the human gut microbiota. Science. 2013;341:1237439.
Rajilic-Stojanovic M, Heilig HG, Tims S, Zoetendal EG, de Vos WM. Long-term monitoring of the human intestinal microbiota composition. Environ Microbiol. 2012.
Hamady M, Knight R. Microbial community profiling for human microbiome projects: tools, techniques, and challenges. Genome Res. 2009;19:1141–1152.
Zoetendal EG, Rajilic-Stojanovic M, de Vos WM. High-throughput diversity and functionality analysis of the gastrointestinal tract microbiota. Gut. 2008;57:1605–1615.
Qin J, Li R, Raes J, et al. A human gut microbial gene catalogue established by metagenomic sequencing. Nature. 2010;464:59–65.
Kolmeder CA, de Been M, Nikkila J, et al. Comparative metaproteomics and diversity analysis of human intestinal microbiota testifies for its temporal stability and expression of core functions. PloS One. 2012;7:e29913.
Shetty SA, Hugenholtz F, Lahti L, Smidt H, de Vos WM. Intestinal microbiome landscaping: insight in community assemblage and implications for microbial modulation strategies. FEMS Microbiol Rev. 2017;41:182–199.
Hall AB, Tolonen AC, Xavier RJ. Human genetic variation and the gut microbiome in disease. Nat Rev Genet. 2017;18:690–699.
Png CW, Linden SK, Gilshenan KS, et al. Mucolytic bacteria with increased prevalence in IBD mucosa augment in vitro utilization of mucin by other bacteria. Am J Gastroenterol. 2010;105:2420–2428.
Li YH, Tian X. Quorum sensing and bacterial social interactions in biofilms. Sensors (Basel). 2012;12:2519–2538.
Miller MB, Bassler BL. Quorum sensing in bacteria. Annu Rev Microbiol. 2001;55:165–199.
Waters CM, Bassler BL. Quorum sensing: cell-to-cell communication in bacteria. Annu Rev Cell Dev Biol. 2005;21:319–346.
Parsek MR, Greenberg EP. Sociomicrobiology: the connections between quorum sensing and biofilms. Trends Microbiol. 2005;13:27–33.
Thompson JA, Oliveira RA, Xavier KB. Chemical conversations in the gut microbiota. Gut Microbes. 2016;7:163–170.
Cvitkovitch DG, Li YH, Ellen RP. Quorum sensing and biofilm formation in Streptococcal infections. J Clin Invest. 2003;112:1626–1632.
Thompson JA, Oliveira RA, Djukovic A, Ubeda C, Xavier KB. Manipulation of the quorum sensing signal AI-2 affects the antibiotic-treated gut microbiota. Cell Rep. 2015;10:1861–1871.
Dobson A, Cotter PD, Ross RP, Hill C. Bacteriocin production: a probiotic trait? Appl Environ Microbiol. 2012;78:1–6.
Ventura M, Turroni F, Motherway MO, MacSharry J, van Sinderen D. Host-microbe interactions that facilitate gut colonization by commensal bifidobacteria. Trends Microbiol. 2012;20:467–476.
Chen Y, Ludescher RD, Montville TJ. Electrostatic interactions, but not the YGNGV consensus motif, govern the binding of pediocin PA-1 and its fragments to phospholipid vesicles. Appl Environ Microbiol. 1997;63:4770–4777.
Gut IM, Blanke SR, van der Donk WA. Mechanism of inhibition of Bacillus anthracis spore outgrowth by the lantibiotic nisin. ACS Chem Biol. 2011;6:744–752.
Li J, Aroutcheva AA, Faro S, Chikindas ML. Mode of action of lactocin 160, a bacteriocin from vaginal Lactobacillus rhamnosus. Infect Dis Obstet Gynecol. 2005;13:135–140.
Devi M, Rebecca LJ, Sumathy S. Bactericidal activity of the lactic acid bacteria Lactobacillus delbreukii. J Chem Pharm Res. 2013;5:176–180.
Alakomi HL, Skytta E, Saarela M, Mattila-Sandholm T, Latva-Kala K, Helander IM. Lactic acid permeabilizes gram-negative bacteria by disrupting the outer membrane. Appl Environ Microbiol. 2000;66:2001–2005.
Kong Y-J, Park B-K, Oh D-H. Antimicrobial activity of quercus mongolica leaf ethanol extract and organic acids against food-borne microorganisms. Korean J Food Sci Technol. 2001;33:178–183.
Ray B, Sandine WE. Acetic, Propionic, and Lactic Acids of Starter Culture Bacteria as Biopreservatives. London: CRC Press; 1992.
Mani-Lópeza E, Garcíaa HS, López-Malo A. Organic acids as antimicrobials to control Salmonella in meat and poultry products. Food Res Int. 2012;45:713–721.
Atassi F, Servin AL. Individual and co-operative roles of lactic acid and hydrogen peroxide in the killing activity of enteric strain Lactobacillus johnsonii NCC933 and vaginal strain Lactobacillus gasseri KS120.1 against enteric, uropathogenic and vaginosis-associated pathogens. FEMS Microbiol Lett. 2010;304:29–38.
Nikaido H. Molecular basis of bacterial outer membrane permeability revisited. Microbiol Mol Biol Rev. 2003;67:593–656.
Ananthaswamy HN, Eisenstark A. Repair of hydrogen peroxide-induced single-strand breaks in Escherichia coli deoxyribonucleic acid. J Bacteriol. 1977;130:187–191.
Freese EB, Gerson J, Taber H, Rhaese HJ, Freese E. Inactivating DNA alterations induced by peroxides and peroxide-producing agents. Mutat Res. 1967;4:517–531.
Di Mascio P, Wefers H, Do-Thi HP, Lafleur MV, Sies H. Singlet molecular oxygen causes loss of biological activity in plasmid and bacteriophage DNA and induces single-strand breaks. Biochim Biophys Acta. 1989;1007:151–157.
Florence TM. The production of hydroxyl radical from the reaction between hydrogen peroxide and NADH. J Inorg Biochem. 1986;28:33–37.
Watanabe T, Nishio H, Tanigawa T, et al. Probiotic Lactobacillus casei strain Shirota prevents indomethacin-induced small intestinal injury: involvement of lactic acid. Am J Physiol Gastrointest Liver Physiol. 2009;297:G506–G513.
Vollenweider S, Grassi G, Konig I, Puhan Z. Purification and structural characterization of 3-hydroxypropionaldehyde and its derivatives. J Agric Food Chem. 2003;51:3287–3293.
Walter J, Britton RA, Roos S. Host-microbial symbiosis in the vertebrate gastrointestinal tract and the Lactobacillus reuteri paradigm. Proc Natl Acad Sci USA. 2011;108(Suppl 1):4645–4652.
Cleusix V, Lacroix C, Vollenweider S, Duboux M, Le Blay G. Inhibitory activity spectrum of reuterin produced by Lactobacillus reuteri against intestinal bacteria. BMC Microbiol. 2007;7:101.
Spinler JK, Auchtung J, Brown A et al. Next-generation probiotics targeting clostridium difficile through precursor-directed antimicrobial biosynthesis. Infect Immun. 2017;85.
Spinler JK, Taweechotipatr M, Rognerud CL, Ou CN, Tumwasorn S, Versalovic J. Human-derived probiotic Lactobacillus reuteri demonstrate antimicrobial activities targeting diverse enteric bacterial pathogens. Anaerobe. 2008;14:166–171.
Axelsson LT, Chung TC, Dobrogosz WJ, Lindgren SE. Production of a broad spectrum antimicrobial substance by Lactobacillus reuteri. Microbial Ecol Health Dis. 1989;2:131–136.
Talarico TL, Axelsson LT, Novotny J, Fiuzat M, Dobrogosz WJ. Utilization of glycerol as a hydrogen acceptor by Lactobacillus reuteri: purification of 1,3-propanediol: NAD oxidoreductase. Appl Environ Microbiol. 1990;56:943–948.
Das NK, Schwartz AJ, Barthel Get al. Microbial metabolite signaling is required for systemic iron homeostasis. Cell Metab. 2019.
Manoppo J, Tasiringan H, Wahani A, Umboh A, Mantik M. The role of Lactobacillus reuteri DSM 17938 for the absorption of iron preparations in children with iron deficiency anemia. Korean J Pediatr. 2019;62:173–178.
Rodwell AW. The histidine decarboxylase of a species of Lactobacillus; apparent dispensability of pyridoxal phosphate as coenzyme. J Gen Microbiol. 1953;8:233–237.
Rossi F, Gardini F, Rizzotti L, La Gioia F, Tabanelli G, Torriani S. Quantitative analysis of histidine decarboxylase gene (hdcA) transcription and histamine production by Streptococcus thermophilus PRI60 under conditions relevant to cheese making. Appl Environ Microbiol. 2011;77:2817–2822.
Hemarajata P, Gao C, Pflughoeft KJ, et al. Lactobacillus reuteri-specific immunoregulatory gene rsiR modulates histamine production and immunomodulation by Lactobacillus reuteri. J Bacteriol. 2013;195:5567–5576.
Thomas CM, Hong T, van Pijkeren JP, et al. Histamine derived from probiotic Lactobacillus reuteri suppresses TNF via modulation of PKA and ERK signaling. PloS one. 2012;7:e31951.
Pessione E, Mazzoli R, Giuffrida MG, et al. A proteomic approach to studying biogenic amine producing lactic acid bacteria. Proteomics. 2005;5:687–698.
Lucas PM, Claisse O, Lonvaud-Funel A. High frequency of histamine-producing bacteria in the enological environment and instability of the histidine decarboxylase production phenotype. Appl Environ Microbiol. 2008;74:811–817.
Izquierdo Canas PM, Gomez Alonso S, Ruiz Perez P, Sesena Prieto S, Garcia Romero E, Palop Herreros ML. Biogenic amine production by Oenococcus oeni isolates from malolactic fermentation of Tempranillo wine. J Food Prot. 2009;72:907–910.
Komatsuzaki N, Shima J, Kawamotoa S, Momosed H, Kimurab T. Production of y-aminobutyric acid (GABA) by Lactobacillus paracasei isolated from traditional fermented foods. Food Microbiol. 2005;22:497–504.
Siragusa S, De Angelis M, Di Cagno R, Rizzello CG, Coda R, Gobbetti M. Synthesis of gamma-aminobutyric acid by lactic acid bacteria isolated from a variety of Italian cheeses. Appl Environ Microbiol. 2007;73:7283–7290.
Pokusaeva K, Johnson C, Luk B, et al. GABA-producing Bifidobacterium dentium modulates visceral sensitivity in the intestine. Neurogastroenterol Motil. 2016;. https://doi.org/10.1111/nmo.12904.
Cohen SS. A Guide to the Polyamines. Oxford: Oxford University Press; 1997.
Shah P, Swiatlo E. A multifaceted role for polyamines in bacterial pathogens. Mol Microbiol. 2008;68:4–16.
Noack J, Kleessen B, Proll J, Dongowski G, Blaut M. Dietary guar gum and pectin stimulate intestinal microbial polyamine synthesis in rats. J Nutr. 1998;128:1385–1391.
Aragozzini F, Ferrari A, Pacini N, Gualandris R. Indole-3-lactic acid as a tryptophan metabolite produced by Bifidobacterium spp. Appl Environ Microbiol. 1979;38:544–546.
Keszthelyi D, Troost FJ, Masclee AA. Understanding the role of tryptophan and serotonin metabolism in gastrointestinal function. Neurogastroenterol Motil. 2009;21:1239–1249.
Smith EA, Macfarlane GT. Formation of phenolic and indolic compounds by anaerobic bacteria in the human large intestine. Microb Ecol. 1997;33:180–188.
Bansal T, Alaniz RC, Wood TK, Jayaraman A. The bacterial signal indole increases epithelial-cell tight-junction resistance and attenuates indicators of inflammation. Proc Natl Acad Sci USA. 2010;107:228–233.
Ruhlmann A, Kukla D, Schwager P, Bartels K, Huber R. Structure of the complex formed by bovine trypsin and bovine pancreatic trypsin inhibitor. Crystal structure determination and stereochemistry of the contact region. J Mol Biol. 1973;77:417–436.
Potempa J, Korzus E, Travis J. The serpin superfamily of proteinase inhibitors: structure, function, and regulation. J Biol Chem. 1994;269:15957–15960.
Turroni F, Foroni E, Motherway MOC, et al. Characterization of the serpin-encoding gene of Bifidobacterium breve 210B. Appl Environ Microbiol. 2010;76:3206–3219.
Schell MA, Karmirantzou M, Snel B, et al. The genome sequence of Bifidobacterium longum reflects its adaptation to the human gastrointestinal tract. Proc Natl Acad Sci USA. 2002;99:14422–14427.
Ivanov D, Emonet C, Foata F, et al. A serpin from the gut bacterium Bifidobacterium longum inhibits eukaryotic elastase-like serine proteases. J Biol Chem. 2006;281:17246–17252.
Haandrikman AJ, Kok J, Laan H, et al. Identification of a gene required for maturation of an extracellular lactococcal serine proteinase. J Bacteriol. 1989;171:2789–2794.
Haandrikman AJ, Kok J, Venema G. Lactococcal proteinase maturation protein PrtM is a lipoprotein. J Bacteriol. 1991;173:4517–4525.
Holck A, Axelsson L, Birkeland SE, Aukrust T, Blom H. Purification and amino acid sequence of sakacin A, a bacteriocin from Lactobacillus sake Lb706. J Gen Microbiol. 1992;138:2715–2720.
Hoermannsperger G, Clavel T, Hoffmann M, et al. Post-translational inhibition of IP-10 secretion in IEC by probiotic bacteria: impact on chronic inflammation. PloS one. 2009;4:e4365.
von Schillde MA, Hormannsperger G, Weiher M, et al. Lactocepin secreted by Lactobacillus exerts anti-inflammatory effects by selectively degrading proinflammatory chemokines. Cell Host Microbe. 2012;11:387–396.
Furusawa Y, Obata Y, Fukuda S, et al. Commensal microbe-derived butyrate induces the differentiation of colonic regulatory T cells. Nature. 2013;504:446–450.
Singh N, Gurav A, Sivaprakasam S, et al. Activation of Gpr109a, receptor for niacin and the commensal metabolite butyrate, suppresses colonic inflammation and carcinogenesis. Immunity. 2014;40:128–139.
Belenguer A, Duncan SH, Calder AG, et al. Two routes of metabolic cross-feeding between Bifidobacterium adolescentis and butyrate-producing anaerobes from the human gut. Appl Environ Microbiol. 2006;72:3593–3599.
Louis P, Duncan SH, McCrae SI, Millar J, Jackson MS, Flint HJ. Restricted distribution of the butyrate kinase pathway among butyrate-producing bacteria from the human colon. J Bacteriol. 2004;186:2099–2106.
Macfarlane GT, Macfarlane S. Bacteria, colonic fermentation, and gastrointestinal health. J AOAC Int. 2012;95:50–60.
Rios-Covian D, Ruas-Madiedo P, Margolles A, Gueimonde M, de Los Reyes-Gavilan CG, Salazar N. Intestinal short chain fatty acids and their link with diet and human health. Front Microbiol. 2016;7:185.
Cummings JH, Pomare EW, Branch WJ, Naylor CP, Macfarlane GT. Short chain fatty acids in human large intestine, portal, hepatic and venous blood. Gut. 1987;28:1221–1227.
Annison G, Illman RJ, Topping DL. Acetylated, propionylated or butyrylated starches raise large bowel short-chain fatty acids preferentially when fed to rats. J Nutr. 2003;133:3523–3528.
Gao Z, Yin J, Zhang J, et al. Butyrate improves insulin sensitivity and increases energy expenditure in mice. Diabetes. 2009;58:1509–1517.
Yanase H, Takebe K, Nio-Kobayashi J, Takahashi-Iwanaga H, Iwanaga T. Cellular expression of a sodium-dependent monocarboxylate transporter (Slc5a8) and the MCT family in the mouse kidney. Histochem Cell Biol. 2008;130:957–966.
Miyauchi S, Gopal E, Babu E, et al. Sodium-coupled electrogenic transport of pyroglutamate (5-oxoproline) via SLC5A8, a monocarboxylate transporter. Biochim Biophys Acta. 2010;1798:1164–1171.
Halestrap AP, Wilson MC. The monocarboxylate transporter family–role and regulation. IUBMB Life. 2012;64:109–119.
Karaki S, Mitsui R, Hayashi H, et al. Short-chain fatty acid receptor, GPR43, is expressed by enteroendocrine cells and mucosal mast cells in rat intestine. Cell Tissue Res. 2006;324:353–360.
Sleeth ML, Thompson EL, Ford HE, Zac-Varghese SE, Frost G. Free fatty acid receptor 2 and nutrient sensing: a proposed role for fibre, fermentable carbohydrates and short-chain fatty acids in appetite regulation. Nutr Res Rev. 2010;23:135–145.
Eberle JA, Widmayer P, Breer H. Receptors for short-chain fatty acids in brush cells at the “gastric groove”. Front Physiol. 2014;5:152.
Tazoe H, Otomo Y, Kaji I, Tanaka R, Karaki SI, Kuwahara A. Roles of short-chain fatty acids receptors, GPR41 and GPR43 on colonic functions. J Physiol Pharmacol. 2008;59(Suppl 2):251–262.
Nohr MK, Pedersen MH, Gille A, et al. GPR41/FFAR3 and GPR43/FFAR2 as cosensors for short-chain fatty acids in enteroendocrine cells vs FFAR3 in enteric neurons and FFAR2 in enteric leukocytes. Endocrinology. 2013;154:3552–3564.
Sina C, Gavrilova O, Forster M, et al. G protein-coupled receptor 43 is essential for neutrophil recruitment during intestinal inflammation. J Immunol. 2009;183:7514–7522.
Brown AJ, Goldsworthy SM, Barnes AA, et al. The orphan G protein-coupled receptors GPR41 and GPR43 are activated by propionate and other short chain carboxylic acids. J Biol Chem. 2003;278:11312–11319.
Voltolini C, Battersby S, Etherington SL, Petraglia F, Norman JE, Jabbour HN. A novel antiinflammatory role for the short-chain fatty acids in human labor. Endocrinology. 2012;153:395–403.
Shapiro H, Thaiss CA, Levy M, Elinav E. The cross talk between microbiota and the immune system: metabolites take center stage. Curr Opin Immunol. 2014;30:54–62.
Devillard E, McIntosh FM, Duncan SH, Wallace RJ. Metabolism of linoleic acid by human gut bacteria: different routes for biosynthesis of conjugated linoleic acid. J Bacteriol. 2007;189:2566–2570.
McIntosh FM, Shingfield KJ, Devillard E, Russell WR, Wallace RJ. Mechanism of conjugated linoleic acid and vaccenic acid formation in human faecal suspensions and pure cultures of intestinal bacteria. Microbiology. 2009;155:285–294.
Gorissen L, Raes K, Weckx S, et al. Production of conjugated linoleic acid and conjugated linolenic acid isomers by Bifidobacterium species. Appl Microbiol Biotechnol. 2010;87:2257–2266.
Gudbrandsen OA, Rodriguez E, Wergedahl H, et al. Trans-10, cis-12-conjugated linoleic acid reduces the hepatic triacylglycerol content and the leptin mRNA level in adipose tissue in obese Zucker fa/fa rats. Br J Nutr. 2009;102:803–815.
Toomey S, Harhen B, Roche HM, Fitzgerald D, Belton O. Profound resolution of early atherosclerosis with conjugated linoleic acid. Atherosclerosis. 2006;187:40–49.
Said HM, Mohammed ZM. Intestinal absorption of water-soluble vitamins: an update. Curr Opin Gastroenterol. 2006;22:140–146.
Ichihashi T, Takagishi Y, Uchida K, Yamada H. Colonic absorption of menaquinone-4 and menaquinone-9 in rats. J Nutr. 1992;122:506–512.
Hill MJ. Intestinal flora and endogenous vitamin synthesis. Eur J Cancer Prev. 1997;6(Suppl 1):S43–S45.
Gill SR, Pop M, Deboy RT, et al. Metagenomic analysis of the human distal gut microbiome. Science. 2006;312:1355–1359.
Bhaskaram P. Micronutrient malnutrition, infection, and immunity: an overview. Nutr Rev. 2002;60:S40–S45.
Cheng CH, Chang SJ, Lee BJ, Lin KL, Huang YC. Vitamin B6 supplementation increases immune responses in critically ill patients. Eur J Clin Nutr. 2006;60:1207–1213.
Meydani SN, Meydani M, Blumberg JB, et al. Vitamin E supplementation and in vivo immune response in healthy elderly subjects: a randomized controlled trial. JAMA. 1997;277:1380–1386.
Tamura J, Kubota K, Murakami H, et al. Immunomodulation by vitamin B12: augmentation of CD8+ T lymphocytes and natural killer (NK) cell activity in vitamin B12-deficient patients by methyl-B12 treatment. Clin Exp Immunol. 1999;116:28–32.
Said HM. Recent advances in transport of water-soluble vitamins in organs of the digestive system: a focus on the colon and the pancreas. Am J Physiol Gastrointest Liver Physiol. 2013;305:G601–G610.
Magnusdottir S, Ravcheev D, de Crecy-Lagard V, Thiele I. Systematic genome assessment of B-vitamin biosynthesis suggests co-operation among gut microbes. Front Genet. 2015;6:148.
LeBlanc JG, Milani C, de Giori GS, Sesma F, van Sinderen D, Ventura M. Bacteria as vitamin suppliers to their host: a gut microbiota perspective. Curr Opin Biotechnol. 2013;24:160–168.
Engevik MA, Morra CN, Roth D, et al. Microbial metabolic capacity for intestinal folate production and modulation of host folate receptors. Front Microbiol. 2019;10:2305.
Thomas CM, Saulnier DM, Spinler JK, et al. FolC2-mediated folate metabolism contributes to suppression of inflammation by probiotic Lactobacillus reuteri. Microbiologyopen. 2016;5:802–818.
Spinler JK, Sontakke A, Hollister EB, et al. From prediction to function using evolutionary genomics: human-specific ecotypes of Lactobacillus reuteri have diverse probiotic functions. Genome Biol Evol. 2014;6:1772–1789.
Olsen I, Amano A. Outer membrane vesicles–offensive weapons or good Samaritans? J Oral Microbiol. 2015;7:27468.
Gurung M, Moon DC, Choi CW, et al. Staphylococcus aureus produces membrane-derived vesicles that induce host cell death. PloS one. 2011;6:e27958.
Berleman J, Auer M. The role of bacterial outer membrane vesicles for intra- and interspecies delivery. Environ Microbiol. 2013;15:347–354.
Furuta N, Takeuchi H, Amano A. Entry of Porphyromonas gingivalis outer membrane vesicles into epithelial cells causes cellular functional impairment. Infect Immun. 2009;77:4761–4770.
Mazmanian SK, Liu CH, Tzianabos AO, Kasper DL. An immunomodulatory molecule of symbiotic bacteria directs maturation of the host immune system. Cell. 2005;122:107–118.
Lee YK, Mazmanian SK. Has the microbiota played a critical role in the evolution of the adaptive immune system? Science. 2010;330:1768–1773.
Shen Y, Giardino Torchia ML, Lawson GW, Karp CL, Ashwell JD, Mazmanian SK. Outer membrane vesicles of a human commensal mediate immune regulation and disease protection. Cell Host Microbe. 2012;12:509–520.
Mazmanian SK, Round JL, Kasper DL. A microbial symbiosis factor prevents intestinal inflammatory disease. Nature. 2008;453:620–625.
Lee YK, Menezes JS, Umesaki Y, Mazmanian SK. Proinflammatory T-cell responses to gut microbiota promote experimental autoimmune encephalomyelitis. Proc Natl Acad Sci USA. 2011;108(Suppl 1):4615–4622.
Ochoa-Reparaz J, Mielcarz DW, Ditrio LE, et al. Central nervous system demyelinating disease protection by the human commensal Bacteroides fragilis depends on polysaccharide A expression. J Immunol. 2010;185:4101–4108.
Hsiao EY, McBride SW, Hsien S, et al. Microbiota modulate behavioral and physiological abnormalities associated with neurodevelopmental disorders. Cell. 2013;155:1451–1463.
Funding
This study was supported by the NIH T32 Grant 5T32DK007664-28 awarded to WR, NIH U01CA170930 Grant awarded to JV, the NLM Training Program in Biomedical Informatics and Data Science T15LM007093 (SCD) awarded to JV, and the Digestive Diseases Center which is funded by NIH/NIDDK P30 DK56338-06A2 Grant awarded to JV.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
JV receives unrestricted research support from BioGaia AB, a Swedish probiotics company. JV serves on the scientific advisory board of Seed, a USA-based probiotics/prebiotics company. JV serves on the scientific advisory board of Biomica, an Israeli informatics enterprise, and on the scientific advisory board of Plexus Worldwide, a USA-based nutrition company.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ruan, W., Engevik, M.A., Spinler, J.K. et al. Healthy Human Gastrointestinal Microbiome: Composition and Function After a Decade of Exploration. Dig Dis Sci 65, 695–705 (2020). https://doi.org/10.1007/s10620-020-06118-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-020-06118-4