
Abstract
Background
Methotrexate is widely used as a chemotherapeutic agent for leukemia and other malignancies. The efficacy of this drug is often limited by mucositis and intestinal injury, which are the major causes of morbidity in children and adults.
Aim
The present study investigates whether melatonin, a powerful antioxidant, could have a protective effect.
Method
Rats were pretreated with melatonin (20 and 40 mg/kg body weight) daily 1 h before methotrexate (7 mg/kg body weight) administration for three consecutive days. After the final dose of methotrexate, the rats were sacrificed and the small intestine was used for light microscopy and biochemical assays. Intestinal homogenates were used for assay of oxidative stress parameters malondialdehyde and protein carbonyl content, and myeloperoxidase activity, a marker of neutrophil infiltration as well as for the activities of the antioxidant enzymes.
Result
Pretreatment with melatonin had a dose-dependent protective effect on methotrexate (MTX)-induced alterations in small intestinal morphology. Morphology was saved to some extent with 20 mg melatonin pretreatment and near normal morphology was achieved with 40 mg melatonin pretreatment. Biochemically, pretreatment with melatonin significantly attenuated MTX-induced oxidative stress (P < 0.01 for MDA, P < 0.001 for protein carbonyl content) and restored the activities of the antioxidant enzymes (glutathione reductase P < 0.05, superoxide dismutase P < 0.01).
Conclusion
The results of the present study demonstrate that supplementation by exogenous melatonin significantly reduces MTX-induced small intestinal damage, indicating that it may be beneficial in ameliorating MTX-induced enteritis in humans.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Methotrexate (MTX) is used widely as chemotherapeutic agent in the treatment of malignancies and various inflammatory diseases, such as psoriasis, rheumatoid arthritis, and inflammatory bowel disease [1]. However, the usage of this drug is often limited by severe side effects and toxic sequelae. One of the major toxic effects of MTX is intestinal injury and mucositis. The small intestinal damage induced by MTX treatment results in malabsorption and diarrhea disturbing the cancer chemotherapy of patients [2, 3].
Reactive oxygen species (ROS) is reported to play an important role in the pathogenesis of MTX-induced intestinal damage [4–8]. Miyazono et al. [4] have reported that increased oxidative stress and MPO activity (marker of neutrophil infiltration/inflammation) contribute to MTX-induced small intestinal damage. They have also shown that the ROS production precedes an increase in myeloperoxidase activity, suggesting neutrophil infiltration. MTX administration has been shown to increase cytosolic peroxide and decrease cellular levels of the anti-oxidant glutathione [5]. Huang et al. [6] demonstrated that MTX-induced intestinal injury is ROS-dependent. Maeda et al. [7] have shown that MTX-induced ROS generation and lipid peroxidation is responsible for enhanced paracellular permeability of the small intestine. In addition, we have previously demonstrated an increase of MDA and protein carbonyl content, the measures of oxidative damage to lipids and proteins, respectively, and myeloperoxidase (MPO) activity in the small intestine of methotrexate (MTX)-treated rats [8]. Studies have shown that the administration of antioxidants such as N-acetyl cysteine [9], vitamin A [10], and garlic extract [11], and most recently lipoic acid [12] prevent MTX-induced damage in animal models.
Melatonin [MT] has been shown to have free radical scavenging actions at both physiologic and pharmacologic concentrations. A number of studies have shown that melatonin is significantly better than the classic antioxidants in resisting free radical-induced molecular destruction. In vivo studies have shown that melatonin was more effective than vitamin E [13], vitamin C [14], and β-carotene [15], and superior to garlic oil [16]. In addition, several evidences suggest that the gut mucosa barrier tissue is a target for melatonin’s protective effects [17–22]. Melatonin has been shown to be gastroprotective and its action has been attributed to scavenging of free radicals and to its ability to attenuate lipid membrane peroxidation, neutrophil-induced infiltration, and cytotoxicity caused by mucosal irritants [23–25]. Evidence exists for de novo melatonin synthesis and high tissue melatonin levels in the gut [21, 22]. Melatonin levels in the gut have been shown to be independent of pineal production, since in rats pinealectomy had no influence on gut melatonin concentrations [18]. Interestingly, at any time of the day or night, the gut contains at least 400 times more melatonin than the pineal gland, once again emphasizing the functional importance of melatonin in the gut [26]. Studies have shown that melatonin is synthesized by gut enterochromaffin cells, where it acts in a paracrine fashion by binding to MT2 receptors in the gut tissue as an antioxidant/anti-inflammatory agent [27]. The major function of locally produced MT in GIT is to help it in coping with the stressors such as oxidants and inflammatory agents and various irritants present in the digested food [28–30].
The above-mentioned findings prompted us to study whether melatonin pretreatment protects against MTX-induced small intestinal injury. In the present study, we have demonstrated that melatonin pretreatment attenuates MTX-induced oxidative stress and small intestinal damage in a dose-dependent manner, indicating that it may be beneficial in ameliorating MTX-induced enteritis in humans.
Methods
Animal Treatment
Dosage and route of administration of methotrexate were determined from those described in the literature as causing consistent intestinal injury in normal rats [29]. After administration of methotrexate, the rats present with histological evidence of drug-induced small intestinal enteropathy and villus atrophy as seen in humans [31]. The dose of melatonin was decided based on a recent study by Ucar et al. [32]. The study was approved by the institution’s animal ethics committee (IAEC).
Adult male Wistar rats (200–225 g) were divided into six groups and treated as follows.
-
Group I The rats in this group (n = 6) received the vehicle alone intraperitoneally for 3 days.
-
Group II The rats in this group (n = 6) received 20 mg of melatonin/kg body weight intraperitoneally for 3 days.
-
Group III The rats in this group (n = 6) received 40 mg of melatonin/kg body weight intraperitoneally for 3 days.
-
Group IV The rats in this group (n = 8) received three consecutive daily intraperitoneal injections of methotrexate at the dose 7 mg/kg body weight.
-
Group V The rats in this group (n = 8) received 20 mg of melatonin/kg body weight 1 h prior to MTX administration intraperitoneally for 3 consecutive days.
-
Group VI The rats in this group (n = 8) received 40 mg of melatonin/kg body weight 1 h prior to MTX administration intraperitoneally for 3 consecutive days.
The rats were sacrificed 24 h after the final dose of methotrexate/vehicle.
Tissue Procurement
Rats were weighed, anesthetized with halothane, and then killed by cervical dislocation. The entire length of the small intestine was removed and flushed with cold phosphate-buffered saline and weighed. The small intestine was divided into duodenum, jejunum, and ileum, and used for biochemical analysis as well as for histological assessment of injury.
Histology (Light Microscopy)
For light microscopic studies, a portion of the tissue was fixed in 10 % buffered formaldehyde and paraffin embedded. Four-micron serial sections were cut and stained with haematoxylin and eosin.
Biochemical Assays
The mucosa was scraped off from the remaining part of the small intestine using a glass slide, weighed, homogenized in appropriate buffers, and used for the biochemical assays including malondialdehyde level, protein carbonyl content, protein content, and myeloperoxidase activity, and for the activities of antioxidant enzymes, superoxide dismutase, glutathione peroxidase, glutathione reductase, gluathione S transferase, and catalase by methods as described in detail earlier [33].
Plasma Melatonin Levels
Plasma melatonin level was measured by ELISA kit (RE54021) purchased from IBL International, Hamburg, Germany.
Results
Effect of Pretreatment of Melatonin on MTX-induced Light Microscopic Changes in the Small Intestine
Light microscopic examination of the parts of small intestine in vehicle-treated rats showed normal morphology with sharp villi, long crypts, intact lining epithelium with normal mucus-secreting cells, normal vasculature, and normal cellularity lamina propria (Fig. 1a–c). The administration of 40 mg melatonin alone caused slight alteration in mucosal morphology especially in the jejunum. The tips of the villi were mildly blunted but the crypts were generally normal (Fig. 1d–f).

Histology of the duodenum, jejunum, and ileum of control (a–c) ×40. The small intestine showed normal morphology with sharp villi, long crypts, and intact lining epithelium with normal mucus-secreting cells, normal vasculature, and normal lamina propria. Histology of duodenum, jejunum, and ileum of rats treated with 40 mg/kg body wt. melatonin alone (d–f), magnification ×40. The crypts were normal but the villi were slightly blunted
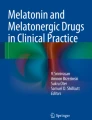
The administration of MTX alone caused damage to the architecture of the small intestine (Fig. 2a–c). The villi were distorted and blunted in the duodenum (Fig. 2a), atrophied and focally absent in the jejunum (Fig. 2b), and aborted, flattened, and fused in the ileum (Fig. 2c). The crypt abscesses were found in all the three segments of the small intestine, suggesting an inflammatory response. The mucosal thickness was reduced and was accompanied by decreased villus/crypt ratio. There was acute transmural inflammatory infiltrate in the mucosa, submucosa and the muscularis layers.

Effect of MTX and melatonin (40 mg/kg) pretreatment on the small intestine of rat ×40. a–c Duodenum, jejunum, and ileum of MTX-treated rats, respectively. The villi were shortened in the duodenum (a), distorted in the jejunum (b), and aborted, flattened, blunted, and fused in the ileum (c). d–f Duodenum, jejunum, and ileum of melatonin (40 mg/kg)-pretreated rats, respectively. Black arrow the villi, white arrow the crypt abscess
Pretreatment with 20 mg/kg melatonin did show some recovery from MTX–induced small intestinal damage (images not shown).
Pretreatment with 40 mg/kg melatonin before the administration of MTX almost restored the morphology of the small intestine. The damage to the mucosa and the severity of inflammatory response was less as compared to the MTX-treated rats. There was less damage to the villi and less crypt abscess in the small intestine of melatonin-pretreated rats. The villi/crypt ratio was greater and the inflammatory infiltrate of the mucosa and muscularis propria was less as compared to the MTX-treated rat. The order of recovery with 40 mg/kg melatonin pretreatment was jejunum > duodenum > ileum (Fig. 2d–f).
In conclusion, pretreatment with 40 mg/kg melatonin significantly protects the small intestine from the deleterious effects of MTX.
Effect of Exogenous Melatonin on Plasma Melatonin Levels in Rats (Table 1)
Basal levels of MT in plasma of untreated rats were high. The administration of MTX drastically decreased the basal MT levels. The administration of exogenous MT alone resulted in a threefold increase in plasma MT levels. The plasma level of MT in MTX + MT-treated rats was significantly higher than that of MTX-treated rats and lower than that of rats treated with MT alone.
Effect of Melatonin Pretreatment on MTX-induced Changes in Parameters of Oxidative Stress
MTX treatment resulted in increased oxidative stress as indicated by elevated malondialdehyde level and protein carbonyl content in the small intestine. It also resulted in significant decrease in the activities of the antioxidant enzymes, superoxide dismutase, glutathione reductase, catalase, and glutathione S transferase. A significant increase in MPO activity, marker of neutrophil infiltration, was observed in the small intestine of MTX-treated rats.
Pretreatment with 40 mg/kg melatonin completely attenuated MTX-induced elevation in the levels of MDA and protein carbonyl content in the small intestine (Figs. 3, 4), confirming the antioxidant role of MT.

Malondialdehyde levels in the small intestine of control and experimental rats with melatonin (20 and 40 mg) treatment, MTX treatment, and melatonin pretreatment . Data represent mean ± SD, n = 6 in each group, *P < 0.01 as compared with the control group; # P < 0.01 as compared with the MTX group

Protein carbonyl content in the small intestine of control and experimental rats with melatonin (20 and 40 mg) treatment, MTX treatment and melatonin pretreatment. Data represent mean ± SD, n = 6 in each group, *P < 0.01 as compared with the control group; # P < 0.01 as compared with the MTX group
Pretreatment with melatonin restored the activities of many antioxidant enzymes. Melatonin at 40 mg/kg completely restored the activity of superoxide dismutase (Fig. 5). Melatonin pretreatment partially but significantly restored the activity of glutathione reductase in a dose-dependent manner (Fig. 6). Pretreatment with 20 mg/kg body wt. melatonin significantly attenuated MTX-induced elevation in the activity of GPO, but the 40 mg dose had no effect (Fig. 7). However, melatonin pretreatment had no significant effect on MTX-induced alterations in the activities of catalase and glutathione S transferase (Figs. 8, 9).

Superoxide dismutase activity in the small intestine of control and experimental rats with melatonin (20 and 40 mg) treatment, MTX treatment and melatonin pretreatment. Data represent mean ± SD, n = 6 in each group, *P < 0.05 as compared with the control group; # P < 0.01 as compared with the MTX group; $ P < 0.05 as compared to the melatonin groups

Glutathione reductase activity in the small intestine of control and experimental rats with melatonin (20 and 40 mg) treatment, MTX treatment and melatonin pretreatment. Data represent mean ± SD, n = 6 in each group, *P < 0.01 as compared with the control group; # P < 0.05 as compared with the MTX group. $ P < 0.05 as compared with the melatonin group

Glutathione peroxidase activity in the small intestine of control and experimental rats with melatonin (20 and 40 mg) treatment, MTX treatment and melatonin pretreatment. Data represent mean ± SD, n = 6 in each group, *P < 0.05 as compared with the control group; # P < 0.05 as compared with the MTX group

Catalase activity in the activity in the small intestine of control and experimental rats with melatonin (20 and 40 mg) treatment, MTX treatment and melatonin pretreatment. Data represent mean ± SD, n = 6 in each group, *P < 0.05 as compared with the control group

Glutathione S transferase activity in the small intestine of control and experimental rats with melatonin (20 and 40 mg) treatment, MTX treatment and melatonin pretreatment. Data represent mean ± SD, n = 6 in each group, *P < 0.05 as compared to the control group; $ P < 0.05 as compared with the 40 mg melatonin group; # P < 0.05 as compared with both melatonin groups
Surprisingly, melatonin pretreatment had no effect on MTX-induced increased myeloperoxidase activity (Fig. 10).

Myeloperoxidase activity in the small intestine of control and experimental rats with melatonin (20 and 40 mg) treatment, MTX treatment and melatonin pretreatment. Data represent mean ± SD, n = 6 in each group, *P < 0.01 as compared with the control and melatonin groups
The administration of melatonin alone (20 mg or 40 mg/kg body wt.) increased the activities of the antioxidant enzymes, and decreased MDA levels in the small intestine as compared with control, but the results were not statistically significant.
Discussion
Methotrexate, a structural analogue of folic acid, is widely used as a chemotherapeutic agent for cancer treatment. It is also used in the treatment of various inflammatory diseases, such as psoriasis, rheumatoid arthritis, and inflammatory bowel disease [1]. Mucositis, intestinal injury, diarrhea, and malabsorption are serious side effects and major causes of MTX-related morbidity in children and adults. The damage to the gastrointestinal (GI) epithelium after MTX-chemotherapy includes villus shortening and fusion, epithelial atrophy, crypt loss, inflammatory infiltrate in the lamina propria, goblet cell depletion, and loss of mucosal integrity [2, 3]. Accordingly, in the present study, most of these features were observed in the small intestine of MTX-treated rats.
Although, pretreatment with 20 mg/kg melatonin did show some recovery from MTX-induced small intestinal damage, 40 mg/kg body wt. melatonin showed almost complete recovery from damage. The villi/crypt ratio was greater and the inflammatory infiltrate of the mucosa and muscularis propria was less as compared to the MTX-treated rat.
In agreement with results reported by us [8] and others [4–7], MTX treatment resulted in increased oxidative stress in the small intestine as evidenced by elevated MDA levels and protein carbonyl content. There were decreased activities of important antioxidant enzymes as well as increases in MPO activity, a marker of neutrophil infiltration. All these studies provide evidence for the important role for ROS in MTX-induced small intestinal damage.
In the present study, the protective effect of MT on MTX-induced small intestinal damage involved attenuation of oxidative stress. MT pretreatment attenuated MTX-induced increased MDA level and protein carbonyl content and restored the activities of important antioxidant enzymes such as superoxide dismutase and glutathione reductase. In addition, melatonin pretreatment ameliorated MTX-induced small intestinal damage in a dose-dependent manner. This finding suggests that melatonin protects against MTX-induced small intestinal damage by acting as an antioxidant. Melatonin is a versatile antioxidant and acts in different ways. It is a major scavenger of free radicals [33, 34], and it also supports several intracellular enzymatic antioxidant enzymes, including SOD and glutathione peroxidase (GPO) [35]. Melatonin has been shown to influence both enzyme activity and cellular mRNA levels for SOD and GPO under physiological conditions and during elevated oxidative stress [35]. Melatonin preserves or even increases the content of GSH in tissues. Melatonin has been shown to induce the activity of γ-glutamylcysteine synthetase, thereby stimulating the production of glutathione (GSH) [36]. Accordingly, Jahovic et al. [31] have shown that MT pretreatment reverses MTX-induced depletion of GSH in the intestine, liver, and kidney of rats. Melatonin has many advantages over the other antioxidants. One advantage is that melatonin has a sparing effect on GSH as it sacrifices itself and does not participate in redox cycling after scavenging free radicals, as do other antioxidants such as vitamins E and C by consuming GSH. Therefore, melatonin is classified as a suicidal or terminal antioxidant [37]. Another advantage of melatonin is that it also stabilizes lipid membranes and defends them from peroxidation, particularly due to its high lipophilicity and easy entrance into the cells to protect their subcellular compartments [38]. Unlike other antioxidants it is believed to lack prooxidant activity [39]. Its lack of toxicity and the ease with which melatonin crosses morpho-physiological barriers and enters subcellular compartments are essential features of this antioxidant. Thus, melatonin appears to be superior to other cellular antioxidants.
It is important to mention that the gastrointestinal tract of vertebrate species is a rich source of extrapineal melatonin. The concentration of melatonin in the gastrointestinal tissues exceeds blood levels by 10–100 times, and there is at least 400 times more melatonin in the gastrointestinal tract than in the pineal gland. The gastrointestinal tract contributes significantly to circulating concentrations of melatonin, especially during the daytime, and melatonin may serve as an endocrine, paracrine, or autocrine hormone influencing the regeneration and function of epithelium, enhancing the immune system of the gut, and reducing the tone of gastrointestinal muscles [40, 41]. There is strong evidence that GIT mucosa, particularly that of duodenal cluster unit (stomach, duodenum and hepato-biliary system), exhibits high biosynthetic activity for MT [26, 27]. Studies have shown that GIT is capable of synthesising MT from its precursor, tryptophan (Trp). Oral Trp administration has been shown to increase the circulating levels of MT, particularly in the portal vein, and this was unaffected by prior pinealectomy, but immensely reduced by a partial ligation of the portal vein [42]. In another study, it has been demonstrated that following Trp administration (orally, 50–200 mg/kg), the GIT mucosa, the liver, and the portal blood show several fold increases in MT content as compared to control rats. These studies demonstrate the capacity of the GIT not only to synthesise MT from Trp but also to secrete it into the circulation [20]. We propose that pretreatment withTrptryptophan instead of melatonin could have similar protective effects on MTX-induced oxidative stress and small intestinal damage (although we could not carry out trp pretreatment studies).
Melatonin receptors have been identified in different parts of the gut, suggesting its role in gut physiology. The main receptor in the GIT for melatonin is the MT2 receptor [27]. The major function of locally produced MT in GIT is to help it cope with the stressors such as oxidants and inflammatory agents and various irritants present in the digested food [28–30].
As mentioned earlier, studies have shown that melatonin is synthesized by gut enterochromaffin cells, where it acts in a paracrine fashion by binding to MT2 receptors in the gut tissue as an antioxidant/anti-inflammatory agent and gets absorbed through mesenteric circulation, to be passed on through the hepatic portal circulation to the liver, where it gets recycled through bile or catabolized and excreted through the kidneys [28–30, 40, 41]. Several recent reports indicating an anti-inflammatory/antioxidant role for melatonin, as well as data linking extra-pineal melatonin imbalance to gut pathophysiology, have been reported [43, 44]. These studies prove the antioxidant role for melatonin under physiological conditions.
In an earlier study, we have shown that MTX administration results in increased neutrophil infiltration as well as increased activity of MPO in the small intestine of rats [8]. This finding is in agreement with those reported earlier [4, 45–47]. MPO is released by activated neutrophils, and is a biomarker for inflammation. MPO, an enzyme linked to both inflammation and oxidative stress, catalyzes the production of hypochlorous acid and a range of other highly reactive species, which, by killing pathogens, play a protective role in the innate immune response.
Melatonin is reported to possess anti-inflammatory properties [48]. Galijasevic et al. [49] identified melatonin as a potent inhibitor of MPO. They showed that, at physiological and supraphysiological concentrations, melatonin interferes with the catalytic activity of MPO by multiple pathways that includes switching the activity of MPO from peroxidation to catalase-like activity and conversion of MPO to an inactive form. Other than inhibition of MPO, melatonin may also reduce the activity of MPO by two other mechanisms. First, it is a potent scavenger of reactive oxygen species and may thereby limit the production of hydrogen peroxide, the co-substrate of MPO [33]. Second, the anti-inflammatory properties of melatonin may reduce infiltration by MPO-secreting leukocytes.
In the present study, however, the protective effect of melatonin on MTX-induced small intestinal damage was mediated by attenuation of oxidative stress and not MPO activity. One possible explanation for this observation is that in in vivo conditions, MT administration scavenges hydrogen peroxide, the co-substrate for MPO, thereby resulting in decreased activity of MPO. However, in ex vivo conditions, this cannot be demonstrated, as the substrate (H2O2) is provided in the incubation medium. The decrease in MPO activity in response to MT treatment despite the provision of the substrate H2O2 as reported in other studies may be due to the direct inactivation of the enzyme by MT as suggested by Galijasevic et al. [49].
In our study, although the administration of melatonin had no significant inhibitory effect on MPO activity, it attenuated MTX-induced crypt abscess formation in the small intestine. This could be explained based on the fact that the inhibition of MPO activity is not the only mechanism by which melatonin ameliorates inflammation, it can also act by blocking transcriptional factors (NFkB) and TNF-α [41, 50]. In addition, studies have shown that COX-2 and iNOS, the mediators of inflammation, are molecular targets for melatonin and its metabolites [51].
There have been studies that show that melatonin may not exert its anti-inflammatory effect by inhibiting neutrophil infiltration. Exogenous melatonin has been shown to preserve renal functional status following I/R-induced injury by increasing glutathione and reducing lipid peroxidation, without any apparent effect on neutrophil infiltration [52]. Alarcon et al. [53] have shown that pretreatment with melatonin inhibits indomethacin-induced gastric ulceration and was not associated with a reduction in neutrophil infiltration. These authors have suggested that the protection afforded by melatonin against indomethacin-induced gastric injury may involve mechanisms other than inhibition of neutrophil infiltration.
Melatonin has been shown to prevent ulcerations of gastrointestinal mucosa by an antioxidant action, reduction of secretion of hydrochloric acid, stimulation of the immune system, fostering epithelial regeneration, and increasing microcirculation [40, 54, 55].
Melatonin is proven to be non-toxic to humans and animals when administered in both physiological and pharmacological amounts [39, 56]. Melatonin is easily synthesized in a pharmacologically pure form and is inexpensive and affordable. In addition, as melatonin is an endogenous antioxidant, the chances of it producing side effects may be less than the exogenous antioxidants.
Beneficial antioxidant effects of melatonin have been recently shown in clinical settings for several chronic diseases, including patients with rheumatoid arthritis [57], elderly patients with primary essential hypertension [58], and females with infertility [59].
Thus, supplementation with melatonin as an adjuvant therapy may be promising in alleviating the gastrointestinal side effects of methotrexate. However, it should be borne in mind that pharmacological and not physiological doses of melatonin protect against oxidative stress and organ injury. Melatonin plays an important role in the regulation of various body functions including circadian rhythms, blood pressure, seasonal reproduction, and immunity [60]. In addition, recent studies have demonstrated that melatonin can act as a prooxidant at high concentrations [61], although earlier studies have reported that melatonin in pharmacological doses is non-toxic to humans [56]. Therefore, before administering melatonin to humans, the side effects of long-term intake of melatonin need to be verified.
References
da Fonseca MA, Casamassimo P. Old drugs, new uses. Pediatr Dent. 2011;33:67–74. (review).
Maiguma T, Hayashi Y, Ueshima S, Kaji H, Egawa T, Chayama K. Relationship between oral mucositis and high-dose methotrexate therapy in pediatric acute lymphoblastic leukemia. Int J Clin Pharmacol Ther. 2008;46:584–590.
Ishaq M, Muhammad JS, Hameed K, Mirza AI. Leflunomide or methotrexate? Comparison of clinical efficacy and safety in low socio-economic rheumatoid arthritis patients. Mod Rheumatol. 2011;21:375–380.
Miyazono Y, Gao F, Horie T. Oxidative stress contributes to methotrexate-induced small intestinal toxicity in rats. Scand J Gastroenterol. 2004;39:1119–1127.
Phillips DC, Woollard KJ, Griffiths HR. The anti-inflammatory actions of methotrexate are critically dependent upon the production of reactive oxygen species. Br J Pharmacol. 2003;138:501–511.
Huang CC, Hsu PC, Hung YC, Liao YF, Liu CC, Hour CT. Ornithine decarboxylase prevents methotrexate-induced apoptosis by reducing intracellular reactive oxygen species production. Apoptosis. 2005;10:895–907.
Maeda T, Miyazono Y, Ito K, Hamada K, Sekine S, Horie T. Oxidative stress and enhanced paracellular permeability in the small intestine of methotrexate-treated rats. Cancer Chemother Pharmacol. 2010;65:1117–1123.
Kolli VK, Abraham P, Isaac B. Alteration in antioxidant defense mechanisms in the small intestines of methotrexate treated rat may contribute to its gastrointestinal toxicity. Cancer Therapy. 2007;5:501–510.
Ciralik H, Bulbuloglu E, Cetinkaya A, Kurutas EB, Celik M, Polat A. Effects of N-acetylcysteine on methotrexate-induced small intestinal damage in rats. Mt Sinai J Med. 2006;73:1086–1092.
Yuncu M, Eralp A, Koruk M, Sari I, Bagci C, Inaloz S. Effect of vitamin A against methotrexate-induced damage to the small intestine in rats. Med Princ Pract. 2004;13:346–352.
Yüncü M, Eralp A, Celik A. Effect of aged garlic extract against methotrexate-induced damage to the small intestine in rats. Phytother Res. 2006;20:504–510.
Somi MH, Hajipour B, Abad GD, et al. Protective role of lipoic acid on methotrexate-induced intestinal damage in rabbit model. Indian J Gastroenterol. 2011;30:38–40.
Baydas G, Canatan H, Turkoglu A. Comparative analysis of the protective effects of melatonin and vitamin E on streptozocin-induced diabetes mellitus. J Pineal Res. 2002;32:225–230.
Gultekin F, Delibas N, Yasar S, Kilinc I. In vivo changes in antioxidant systems and protective role of melatonin and a combination of vitamin C and vitamin E on oxidative damage in erythrocytes induced by chlorpyrifos-ethyl in rats. Arch Toxicol. 2001;75:88–96.
Hsu C, Han B, Liu M, Yeh C, Casida JE. Phosphine-induced oxidative damage in rats: attenuation by melatonin. Free Radic Biol Med. 2000;28:636–642.
Anwar MM, Meki AR. Oxidative stress in streptozotocin-induced diabetic rats: effects of garlic oil and melatonin. Comp Biochem Physiol A: Mol Integr Physiol. 2003;135:539–547.
Reiter RJ, Tan DX, Mayo JC. Neurally-mediated and neurally-independent beneficial actions of melatonin in the gastrointestinal tract. J Physio Pharm. 2003;54:113–125.
Sewerynek E, Reiter RJ, Melchiorri D. Oxidative damage in the liver induced by ischemia-reperfusion: protection by melatonin. Hepatogastroenterology. 1996;43:898–905.
Messner M, Huether G, Lorf T. Presence of melatonin in the human hepatobiliary-gastrointestinal tract. Life Sci. 2001;69:543–551.
Konturek SJ, Konturek PC, Brzozowska I. Localization and biological activities of melatonin in intact and diseased gastrointestinal tract (GIT). J Physiol Pharmacol. 2007;58:381–405.
Huether G. The contribution of extrapineal sites of melatonin synthesis to circulating melatonin levels in higher vertebrates. Experientia. 1993;49:665–670.
Stefulj J, Hörtner M, Ghosh M. Gene expression of the key enzymes of melatonin synthesis in extrapineal tissues of the rat. J Pineal Res. 2001;30:243–247.
Bubenik GA, Pang SF, Cockshut JR. Circadian variation of portal, arterial and venous blood levels of melatonin in pigs and its relationship to food intake and sleep. J Pineal Res. 2000;28:9–15.
Reiter RJ, Tan DX. What constitutes a physiological concentration of melatonin? J Pineal Res. 2003;34:79–80.
Tan DX, Manchester LC, Reiter RJ, et al. High physiological levels in the bile of mammals. Life Sci. 1999;65:2523–2529.
Kvetnoy IM, Ingel IE, Kvetnaia TV, et al. Gastrointestinal melatonin: cellular identification and biological role. Neuro Endocrinol Lett. 2002;23:121–132.
Lee PPN, Pang SF. Melatonin and its receptors in the gastrointestinal tract. Biol Signals. 1993;2:181–193.
Pandi-Perumal SR, Srinivasan V, Maestroni GJM, Cardinali DP, Poeggeler B, Hardeland R. Melatonin nature is most versatile biological signal? FEBS J. 2006;273:2813–2838.
Tan DX, Manchester LC, Reiter RJ. A novel melatonin metabolite, cyclic 3-hydroxymelatonin: a biomarker of in vivo hydroxyl radical generation. Biochem Biophys Res Commun. 1998;253:614–620.
Hirata F, Hayaishi O, Tokuyama T, Seno S. In vitro and in vivo formation of two new metabolites of melatonin. J Biol Chem. 1974;249:1311–1313.
Jahovic N, Cevik H, Sehirli AO. Melatonin prevents methotrexate induced hepatorenal oxidative injury in rats. J Pineal Res. 2003;34:282–287.
Ucar M, Korkmaz A, Reiter RJ. Melatonin alleviates lung damage induced by the chemical warfare agent nitrogen mustard. Toxicol Lett. 2007;173:124–131.
Reiter RJ, Tan DX, Maldonado MD. Melatonin as an antioxidant: physiology versus pharmacology. J Pineal Res. 2005;39:215–216.
Reiter RJ, Tan DX, Terron MP, Flores LJ, Czarnocki Z. Melatonin and its metabolites: new findings regarding their production and their radical scavenging actions. Acta Biochim Pol. 2007;54:1–9.
Rodriguez C. Regulation of antioxidant enzymes: a significant role for melatonin. J Pineal Res. 2004;36:1–9.
Winiarska K, Fraczyk T, Malinska D, Drozak J, Bryla J. Melatonin attenuates diabetes induced oxidative stress in rabbits. J Pineal Res. 2006;40:168–176.
Tan DX. Chemical and physical properties and potential mechanisms: melatonin as a broad spectrum antioxidant and free radical scavenger. Curr Top Med Chem. 2002;2:181–197.
Costa EJX, Lopes RH, Lamy-Freund MT. Solubility of pure bilayers to melatonin. J Pineal Res. 1995;19:123–126.
Seabra ML, Bignotto M, Pinto LR Jr, Tufik S. Randomized, double-blind clinical trial, controlled with placebo, of the toxicology of chronic melatonin treatment. J Pineal Res. 2000;29:193–200.
Aydin M, Canpolat S, Kuloğlu T, Yasar A, Colakoglu N, Kelestimur H. Effects of pinealectomy and exogenous melatonin on ghrelin and peptide YY in gastrointestinal system and neuropeptide Y in hypothalamic arcuate nucleus: immunohistochemical studies in male rats. Regul Pept. 2008;146:197–203.
Reiter RJ. Melatonin: clinical relevance. Best Pract Res Clin Endocrinol Metab. 2003;17:273–285.
Huether G, Poegeller G, Reimer R, George A. Effect of tryptophan administration on circulating melatonin levels in chicks and rats: evidence for stimulation of melatonin synthesis and release in the gastrointestinal tract. Life Sci. 1992;51:945–953.
Sener G, Jahovic N, Tosun O, Atasoy BM, Yegen BC. Melatonin ameliorates ionizing radiation—induced oxidative organ damage in rats. Life Sci. 2003;74:563–572.
Al-Ghoul WM, Abu-Shaqra S, Park BG, Fazal N. Melatonin plays a protective role in postburn rodent gut pathophysiology. Int J Biol Sci. 2010;6:282–293.
Gao F, Ueda S, Horie T. Effect of a synthetic analog of prostaglandin E1 on the intestinal mucosa of methotrexate-treated rats. Anticancer Res. 2001;21:1913–1917.
Sener G, Ekşioğlu-Demiralp E, Cetiner M, Ercan F, Yeğen BC. Beta-glucan ameliorates methotrexate-induced oxidative organ injury via its antioxidant and immunomodulatory effects. Eur J Pharmacol. 2006;542:170–178.
Sener G, Ekşioğlu-Demiralp E, Cetiner M, et al. L-Carnitine ameliorates methotrexate-induced oxidative organ injury and inhibits leukocyte death. Cell Biol Toxicol. 2006;22:47–60.
Konturek SJ, Konturek PC, Brzozowski T. Melatonin in gastroprotection against stress-induced acute gastric lesions and in healing of chronic gastric ulcers. J Physiol Pharmacol. 2006;57:51–66. (review).
Galijasevic S, Abdulhamid I, Abu-Soud HM. Melatonin is a potent inhibitor for myeloperoxidase. Biochemistry. 2008;47:2668–2677.
Li JH. Melatonin reduces inflammatory injury through inhibiting NF-kappaB activation in rats with colitis. Mediators Inflamm. 2005;2005:185–193.
Mayo JC, Sainz RM, Tan DX, et al. Anti-inflammatory actions of melatonin and its metabolites, N1-acetyl-N2-formyl-5-methoxy-kynuramine (AFMK) and N1-acetyl-5-methoxykynuramine (AMK), in macrophages. J Neuroimmunol. 2005;165:139–149.
Rodríguez-Reynoso S, Leal C, Portilla-de Buen E, Castillo JC, Ramos-Solano F. Melatonin ameliorates renal ischemia/reperfusion injury. J Surg Res. 2004;116:242–247.
Alarcón de la Lastra C, Motilva V, Martín MJ, et al. Protective effect of melatonin on indomethacin-induced gastric injury in rats. J Pineal Res. 1999;26:101–107.
Cuzzocrea S, Mazzon E, Serraino I, Lepore V, Terranova ML, Ciccolo A. Melatonin reduces dinitrobenzene sulfonic acid-induced colitis. J Pineal Res. 2001;30:1–12.
Konturek PC, Konturek SJ, Brzozowski T, et al. Gastroprotective activity of melatonin and its precursor, l-tryptophan, against stress-induced and ischaemia-induced lesions is mediated by scavenge of oxygen radicals. Scand J Gastroenterol. 1997;32:433–438.
Reiter RJ. Oxidative processes and antioxidative defense mechanisms in the aging brain. FASEB J. 1995;9:526–533.
Forrest CM, Mackay GM, Stoy N, Stone TW, Darlington LG. Inflammatory status and kynurenine metabolism in rheumatoid arthritis treated with melatonin. Br J Clin Pharmacol. 2007;64:517–526.
Kedziora-Kornatowska K. Antioxidative effects of melatonin administration in elderly primary essential hypertension patients. J Pineal Res. 2008;45:312–317.
Tamura H. Oxidative stress impairs oocyte quality and melatonin protects oocytes from free radical damage and improves fertilization rate. J Pineal Res. 2008;44:280–287.
Brzezinski A. Melatonin in humans. N Engl J Med. 1997;336:186–195.
Kadoma Y, Fujisawa S. Radical-scavenging activity of melatonin, either alone or in combination with vitamin E, ascorbate or 2-mercaptoethanol as co-antioxidants, using the induction period method. In Vivo. 2011;25:49–53.
Acknowledgment
The authors acknowledge the Council for Scientific and Industrial Research (CSIR), New Delhi for the financial support for the study. Mr. Viswa Kalyan Kolli is a senior research fellow on the present study.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kolli, V.K., Abraham, P., Isaac, B. et al. Preclinical Efficacy of Melatonin to Reduce Methotrexate-Induced Oxidative Stress and Small Intestinal Damage in Rats. Dig Dis Sci 58, 959–969 (2013). https://doi.org/10.1007/s10620-012-2437-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-012-2437-4