
Abstract
Purpose Music has been utilized as a therapeutic tool during colonoscopy, but various randomized controlled trials (RCTs) have been inconsistent. We conducted a meta-analysis to analyze the effect of music on patients undergoing colonoscopy. Patients and Methods Multiple medical databases were searched (12/06). Only RCTs on adult subjects that compared music versus no music during colonoscopy were included. Meta-analysis was analyzed for total procedure time, dose of sedative medications (midazolam and mepiridine), and patients’ pain scores, experience, and willingness to repeat the same procedure in the future. Results Eight studies (N = 712) met the inclusion criteria. Patients’ overall experience scores (P < 0.01) were significantly improved with music. No significant differences were noted for patients’ pain scores (P = 0.09), mean doses of midazolam (P = 0.10), mean doses of meperidine (P = 0.23), procedure times (P = 0.06), and willingness to repeat the same procedure in future (P = 0.10). Conclusions Music improves patients’ overall experience with colonoscopy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Colonoscopy can be a stressful but important procedure for patients throughout the world as a screening, diagnostic, and therapeutic tool. The stress seems to be attributed to an increased amount of anxiety and discomfort before and during the procedure, leading to patient refusal and elevated medication administration [1]. Anxiety is an important predictor of patient cooperation during gastrointestinal endoscopy [2].
In an effort to decrease stress and anxiety, various stress-reducing medical modalities have been tried, including music. Therapeutic uses of music have been utilized in many disciplines of medicine, including cardiology, radiology, pulmonology, and gastroenterology. Music therapy has promoted relaxation responses, triggered positive associations, and diverted attention from anxiety during pain-invoking experiences [3]. The use of music has been used to decrease anxiety levels in patients in a variety of scenarios, such as those admitted to the coronary intensive care units, undergoing magnetic resonance imaging, and undergoing bronchoscopy [4–6]. In gastroenterology, music has been hypothesized to act as an anxiolytic for stressful procedures; however, published studies have exhibited differing outcomes.
Music played during flexible sigmoidoscopies revealed improved satisfaction of patients and decreased mean arterial blood pressure and heart rate [7, 8]. In other procedures, including esophagogastroduodenoscopy and colonoscopy, relaxing music was shown to improve patient tolerance and attitudes toward overall feelings about the procedure, although the effects of music were thought to be marginal [9]. Some studies have demonstrated that music during colonoscopy results in decreased doses of sedative medications [10, 11]. The use of relaxing music during colonoscopies has been shown to reduce state-trait anxiety inventory test scores [12, 13]; however, a similar study revealed no significant difference between music and non-music groups [14]. Furthermore, when music was played during esophagogastroduodenoscopy and colonoscopy, no significant differences were noted compared to controls in respect to tolerance of examination, pain sensation, and perception of the endoscopy room ambiance; although a majority of patients expressed a preference for music during future endoscopy [15].
Randomized controlled trials (RCTs) on the subject of music during colonoscopy have shown varying results in many regards. Patients’ anxiety, pain, experience, and willingness to have a repeat procedure have varied remarkably between studies with music therapy. From the endoscopists’ perspective, time to the cecum, total time of colonoscopy, and sedative medication requirements have also been inconsistent.
We performed a meta-analysis to evaluate the effect of music during colonoscopy on patients’ pain, satisfaction, sedative medication requirements, and willingness to repeat exam.
Methods
Study Selection Criteria
Randomized controlled trials (RCTs) using music during colonoscopy were selected. Each study was assigned a Jadad score to access the quality of the study [16].
Data Collection and Extraction
Articles were searched in Medline, Old Medline, Cochrane Central Register of Controlled Trials and Database of Systematic Reviews, DARE, OVID Healthstar & Journals, Cumulative Index for Nursing & Allied Health Literature, and Pubmed (from 1966 to 2006) as well as abstracts from major national GI meetings (Digestive Disease Week and American College of Gastroenterology National Meeting from 2001 to 2006) were searched (search date December 2006). The search terms used were music, colonoscopy, randomized, relaxing music, and music during colonoscopy. Only RCTs on adult subjects (≥18 years old) that compared music versus no music during colonoscopy were included. Standard forms were utilized by two independent reviewers in extracting the data, with differences being resolved by mutual agreement. Length of procedure, sedative medication requirements (meperidine and midazolam), and patients’ experience, pain, and willingness to repeat the same procedure were identified and extracted from the randomized trials. If data was not identified within the manuscript, corresponding authors were contacted for additional information or clarification.
Statistical Methods
Meta-analysis for the effect of music on patients undergoing colonoscopy was analyzed by calculating pooled estimates of total procedure time, dose of sedative medications (midazolam and mepiridine), and patients’ pain scores, experience, and willingness to repeat the same procedure in the future. Separate analyses were performed for each main outcome by using odds ratio (OR), weighted mean difference (WMD), and standardized mean difference (SMD). Heterogeneity was assessed by calculating the I2 measure of inconsistency. A random effects model was utilized to calculate the summary estimate. Significance was indicated by P-value <0.05. Publication bias was assessed by funnel plots. RevMan 4.2 was utilized for statistical analysis of the data.
Results
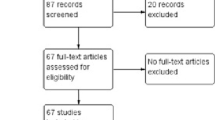
The initial search identified 107 articles (music and colonoscopy) (Fig. 1). Of these articles, 14 relevant articles were selected and reviewed by two independent authors. Eight randomized controlled trials (N = 712) met the inclusion criteria and were selected for this study. Data was extracted from these eight studies. All included studies were published as full-text articles in peer-reviewed journals. Table 1 shows the details and Jadad score for the selected studies (5, excellent quality; 0, poor quality). All randomized trials were published from 2002 to 2006. Studies were performed worldwide, including the USA (two), Spain, Germany, India, China, Japan, and Turkey. Gender was approximately equal among the studies.

Article identification and selection algorithm
Patients’ overall experience scores were improved with music (SMD −0.65, 95% CI: −1.01 to −0.28, P < 0.01) (Fig. 2). In respect to sedative medication requirements, no statistically significant differences between music and no music groups were noted for patients’ pain scores (SMD −0.46, 95% CI: −0.98–0.07, P = 0.09) (Fig. 3), mean doses of midazolam (WMD −0.55, 95% CI: −1.21–0.10, P = 0.10) (Fig. 4), and mean doses of mepiridine (WMD −5.27, 95% CI: −13.96–3.41, P = 0.23) (Fig. 5). Music was associated with a trend, though not statistically significant, toward shorter procedure times (WMD −2.32 min, 95% CI: −4.76–0.13, P = 0.06) (Fig. 6). The music groups did not demonstrate a significant increase in willingness to have a repeat procedure in the future (OR 3.89, 95% CI: 0.76–19.97, P = 0.10) (Fig. 7).

Forrest plot showing standard mean difference with random effect model for patients’ experience with music versus no music during colonoscopy

Forrest plot showing standard mean difference with random effect model for patients’ pain reduction with music versus no music during colonoscopy

Forrest plot showing weighted mean difference with random effect model for midazolam dose reduction with music versus no music during colonoscopy

Forrest plot showing weighted mean difference with random effect model for mepiridine dose reduction with music versus no music during colonoscopy

Forrest plot showing weighted mean difference with random effect model for total procedure time with music versus no music during colonoscopy

Forrest plot showing odds ratio with random effect model for patients’ willingness to repeat same procedure with music versus no music during colonoscopy
Publication bias was evaluated by funnel plot. No significant publication bias was identified (Fig. 8).

Funnel plot showing no significant publication bias
Discussion
Colonoscopy is a stressful procedure for many patients. Stress reducers of any kind may be beneficial in decreasing intra-procedural doses of sedative medications as well as for increasing patients’ willingness to undergo the procedure, which, in turn, may promote more patients to undergo further screening or surveillance colonoscopies. History has shown that music may be a simple non-invasive stress reducer for stressful events and procedures.
Music has been shown to be beneficial for patients undergoing a variety of medical experiences and procedures, including stays in cardiac intensive-care units, radiology procedures, and gastrointestinal endoscopy [4–6]. Several studies have evaluated music as an adjunct relaxation therapy during various endoscopic procedures, including flexible proctosigmoidoscopy [7, 8, 17], colonoscopy [10–12, 14, 18–21], and a mix of EGD and colonoscopy [9, 13, 15]. Of these studies, music seems to be the most effective in reducing procedure-related anxiety and improving overall experience [7, 8, 10, 12, 13, 15, 17, 18, 20, 21]. Music may also decrease heart rates and blood pressure values in patients undergoing lower GI endoscopic procedures [8, 14]. However, in regards to various parameters, including anxiety, the beneficial effects of music during colonoscopy have not been consistent among studies.
Three studies have demonstrated that music during colonoscopy has reduced the need for sedative medications [10, 14, 18]; however, other studies have found no significant differences [11, 15, 20, 21]. Similar results have been found in regards to patients’ pain levels during colonoscopy. One study revealed a decrease in the amount of patients’ pain levels with the addition of music [21]; however, four other studies revealed no significant differences between the music and non-music groups [10, 15, 18, 20]. One study showed a significant decrease in overall procedure time [11], but six studies differed with no significant procedure time reduction with music during colonoscopy [10, 12, 14, 18–20].
This meta-analysis study demonstrates that music played during colonoscopy significantly improves patients’ experience during colonoscopy. This effect is likely due to music’s role in patient relaxation during the stressful procedure of colonoscopy. Music during colonoscopy was also associated with a trend, though not significant, toward shorter procedure times. The addition of music to colonoscopy did not demonstrate a significant decrease in patients’ pain levels, amount of sedative medications, or an increase in willingness to repeat a colonoscopy in the future.
This study had a few strengths. First, it included only randomized clinical trials, limiting observational and selection bias. Second, an extensive search was performed including seven databases and major GI meeting abstracts. Third, for data not easily identified in manuscripts, corresponding authors were contacted and missing data was obtained for analysis. Fourth, the trials were performed throughout the world, including both western and eastern hemispheres, and consisted of many different cultures.
However, this study also had a few weaknesses. First, the quality of the RCTs included in this study, although good, did lack in certain aspects. The music utilized in the included studies varied from relaxing classical music to patient-directed selections. The timing of the music being played also varied among studies as well. Music was played in the pre-operative area just prior to the procedure or only during the procedure. A more consistent timing and music selection may have altered the results, possibly impacting those results which showed a positive trend but were not statistically significant. Also, a majority of the studies were not blinded to the endoscopist. To minimize this aspect, endoscopist satisfaction was eliminated from the meta-analysis. Total procedure time and possibly medication administration were the only endoscopist-driven variables. Second, the studies included were heterogeneous. The most likely reason for this was the vast differences among the findings for each of the studies. Although the study designs were adequate, the protocols were not equivalent. Variations in music and delivery of music differed among studies. The amounts of required sedative medications, procedure times, willingness to repeat colonoscopy, and pain scores all differed significantly based upon populations studied. This meta-analysis included many different cultures and endoscopists from around the world, which may influence the variables leading to increased heterogeneity. Due to the heterogeneity, a random effects model was utilized for data analysis, expanding the confidence interval in an effort to more easily detect a difference, if one exists. Third, four relevant studies were not included in this meta-analysis. Three studies [9, 13, 22] examining music therapy with both EGD and colonoscopy were not included due to the inability to extract the requested data regarding the effects of music during colonoscopy only and one large study [15] was not included due to lack of randomization.
In conclusion, this meta-analysis demonstrates that music played during colonoscopy improves patients’ overall experience but does not alter other parameters, such as sedative pain medication requirements, procedure times, patients’ pain, and patients’ willingness to repeat the same procedure in the future. Since patients’ experience is improved with the addition of music to the colonoscopy, it is reasonable to offer this non-invasive modality to endoscopy laboratories.
References
Petravage J, Swedberg J (1988) Patient response to sigmoidoscopy—recommendations via mailed reminders. J Fam Pract 27:387–389
Mahajan RJ, Johnson JC, Marshall JB (1997) Predictors of patient cooperation during gastrointestinal endoscopy. J Clin Gastroenterol 24:220–223. doi:10.1097/00004836-199706000-00007
Cook JD (1981) The therapeutic use of music: a literature review. Nurs Forum 20:252–266. doi:10.1111/j.1744-6198.1981.tb00754.x
Guzzetta CE (1989) Effects of relaxation and music therapy on patients in a coronary care unit with presumptive acute myocardial infarction. Heart Lung 18:609–616
Slifer KJ, Penn-Jones K, Cataldo MF, Conner RT, Zerhouni EA (1991) Music enhances patients’ comfort during MR imaging [letter]. Am J Roentgenol 156:403
Dubois JM, Bartter T, Pratter MR (1995) Music improves patient comfort level during outpatient bronchoscopy. Chest 108:129–130. doi:10.1378/chest.108.1.129
Chlan L, Evans D, Greenleaf M, Walker J (2000) Effects of a single music therapy intervention on anxiety, discomfort, satisfaction, and compliance with screening guidelines in outpatients undergoing flexible sigmoidoscopy. Gastroenterol Nurs 23:148–156. doi:10.1097/00001610–200007000-00003
Palakanis KC, DeNobile JW, Sweeney WB, Blankenship CL (1994) Effect of music therapy on state anxiety in patients undergoing flexible sigmoidoscopy. Dis Colon Rectum 37:478–481. doi:10.1007/BF02076195
Bampton P, Draper B (1997) Effect of relaxation music on patient tolerance of gastrointestinal endoscopic procedures. J Clin Gastroenterol 25:343–345. doi:10.1097/00004836-199707000-00010
Lee DW, Chan KW, Poon CM, Ko CW, Chan KH, Sin KS, Sze TS, Chan ACW (2002) Relaxation music decreases the dose of patient-controlled sedation during colonoscopy: a prospective randomized controlled trial. Gastrointest Endosc 55:33–36. doi:10.1067/mge.2002.120387
Schiemann U, Gross M, Reuter R, Kellner H (2002) Improved procedure of colonoscopy under accompanying music therapy. Eur J Med Res 7:131–134
Lopez-Cepero Andrada JM, Amaya Vidal A, Castro Aguilar-Tablada T, Garcia Reina I, Silva L, Ruiz Guinaldo A, De la Rosa JL, Herrero Cibaja I, Ferre Alamo A, Benitez Roldan A (2004) Anxiety during the performance of colonoscopies: modification using music therapy. Eur J Gastroenterol Hepatol 16:1381–1386. doi:10.1097/00042737-200412000-00024
Hayes A, Buffum M, Lanier E, Rodahl E, Sasso C (2003) A music intervention to reduce anxiety prior to gastrointestinal procedures. Gastroenterol Nurs 26:145–149. doi:10.1097/00001610-200307000-00002
Smolen D, Topp R, Singer L (2002) The effect of self-selected music during colonoscopy on anxiety, heart rate, and blood pressure. Appl Nurs Res 15:126–136. doi:10.1053/apnr.2002.34140
Binek J, Sagmeister M, Borovicka J, Knierim M, Magdeburg B, Meyenberger C (2003) Perception of gastrointestinal endoscopy by patients and examiners with and without background music. Digestion 68:5–8. doi:10.1159/000073219
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ (1996) Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 17:1–12. doi:10.1016/0197-2456(95)00134-4
Lembo T, Fitzgerald L, Matin K, Woo K, Mayer EA, Naliboff BD (1998) Audio and visual stimulation reduces patient discomfort during screening flexible sigmoidoscopy. Am J Gastroenterol 93:1113–1116. doi:10.1111/j.1572-0241.1998.00339.x
Harikumar R, Raj M, Paul A, Harish K, Kumar KS, Sandesh K, Asharaf S, Thomas V (2006) Listening to music decreases need for sedative medication during colonoscopy: a randomized, controlled trial. Indian J Gastroenterol 25:3–5
Uedo N, Ishikawa H, Morimoto K, Ishihara R, Narahara H, Akedo I, Ioka T, Kaji I, Fukuda S (2004) Reduction in salivary cortisol level by music therapy during colonoscopic examination. Hepatogastroenterology 51:451–453
Bechtold ML, Perez RA, Puli SR, Marshall JB (2006) Effect of music on patients undergoing outpatient colonoscopy. World J Gastroenterol 12:7309–7312
Ovayolu N, Ucan O, Pehlivan S, Pehlivan Y, Buyukhatipoglu H, Savas MC, Gulsen MT (2006) Listening to Turkish classical music decreases patients’ anxiety, pain, dissatisfaction and the dose of sedative and analgesic drugs during colonoscopy: a prospective randomized controlled trial. World J Gastroenterol 12:7532–7536
Salmore RG, Nelson JP (2000) The effect of preprocedure teaching, relaxation instruction, and music on anxiety as measured by blood pressures in an outpatient gastrointestinal endoscopy laboratory. Gastroenterol Nurs 23:102–110. doi:10.1097/00001610-200005000-00003
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bechtold, M.L., Puli, S.R., Othman, M.O. et al. Effect of Music on Patients Undergoing Colonoscopy: A Meta-Analysis of Randomized Controlled Trials. Dig Dis Sci 54, 19–24 (2009). https://doi.org/10.1007/s10620-008-0312-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-008-0312-0