
Abstract
Sleep disturbances are commonly reported by patients who suffer from gastroesophageal reflux disease (GERD) but it is uncertain if GERD plays a role in patients with sleep disorders of undetermined origin. The prevalence of GERD in patients with sleep disorders of unknown etiology is uncertain; the aim of this study was to determine this prevalence. Three hundred eighty-five consecutive patients reporting to an outpatient clinic for evaluation of sleep disorders were assessed for their sleepiness in relation to reflux symptom intensity. Reflux symptoms that met the survey criteria for a diagnosis of GERD were present in 45 of the 385 subjects (12.8%). These subjects did not have a diagnosis of GERD and were not being treated. Multiple regression analysis showed that excessive sleepiness was associated with intensity of GERD symptoms. Patients with GERD had significantly higher Epworth sleep scores than patients without GERD (12.8 vs. 10.6; p=0.007), indicating more daytime sleepiness. We conclude that unrecognized and untreated GERD are present in many patients presenting with sleep disorders. Patients with GERD had significantly greater sleepiness. Further studies of the impact of GERD treatment in this population are necessary.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Symptoms of gastroesophageal reflux disease (GERD) occurring once a week are present in 14%–20% of the population and daily symptoms are reported by 7% [1]. In a large telephone survey, 13% of respondents with symptoms of gastroesophageal reflux reported nocturnal symptoms only and 65% reported both daytime and nocturnal symptoms [2]. Seventy-five percent of respondents with nocturnal symptoms reported that GERD symptoms affected their sleep [2]. Undiagnosed sleep disturbances are reported in at least 2%–4% of middle-aged adults and it has been suggested that GERD may contribute to daytime somnolence, but direct proof of this is lacking [3]. Patients with nocturnal acid reflux have been shown to have an increased number of arousals from sleep [4]. Repeated arousal has been shown to fragment sleep and to result in daytime somnolence. The aim of our study was to determine the prevalence of reflux symptoms in a cohort of patients with sleep disturbances severe enough to warrant investigation with polysomnography and to determine if patients with symptoms of gastroesophageal reflux had poorer sleep and consequently excessive daytime sleepiness compared to those without these symptoms.

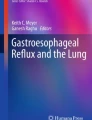
Questions from the Reflux Disease Questionnaire used to determine if the subject has GERD symptoms
Methods
Three hundred eighty-five consecutive patients referred to an outpatient sleep disorders clinic for the evaluation of previously uninvestigated sleep disorders were studied. Subjects were excluded from the study if they carried any specific diagnosis of a sleep disturbance from an earlier examination or if they were undergoing studies to monitor therapy instituted for a sleep disturbance. Demographic data were collected at the baseline visit, along with information on alcohol, medication, and tobacco use. Two validated questionnaires were administered to all patients: the Epworth sleep questionnaire and the Reflux Disease Questionnaire (RDQ). The Epworth Sleepiness Scale is a validated instrument used for measurement of the general level of daytime sleepiness. It measures the sleep propensity in various life situations and consists of eight self-reported questions [5]. Each question has a score ranging from 0 to 3. A value of 5.9±2.2 represents the norm in the community [6, 7]. Possible scores range from 0 (the least sleepy) to 24 (the most sleepy). An Epworth sleepiness scale score of 10 is indicative of significant sleepiness and is a threshold for referral for sleep evaluation [8]. The Epworth Sleepiness Scale is considered to be the most discriminating test for measurement of excessive daytime sleepiness. The RDQ is a validated symptom questionnaire of 12 questions which is designed to identify individuals with symptoms of gastroesophageal reflux. A score ≥8 strongly suggests a diagnosis of GERD [9]. This is calculated by adding the values for the four questions shown in Fig 1. The instrument is sensitive to change in symptoms. It has been validated in different populations and languages and was designed as a diagnostic tool for GERD [10–12].
Statistics
All data were analyzed using SPSS for Windows (Release 11.0.5; SPSS Inc., Chicago, IL). Chi-square and t-tests were used to compare subjects with and without GERD symptoms by demographic and related characteristics. A multiple linear regression model was constructed using a backward elimination technique. The continuous variables evaluated were age (years), body mass index (BMI), and RDQ score, and the dichotomous variables were gender, acid suppression, alcohol use, and smoking. All the variables listed above were entered together in the first step of the procedure and removed one at a time, until only variables significant at P<0.10 remained. The variables significant at P<0.05 were then entered into the final model.
The protocol was approved by the institutional review board at Aurora Sinai Medical Center and patients gave informed consent.
GERD symptoms
Symptoms of gastroesophageal reflux were present in 45 subjects (12.8%) based on an RDQ score ≥8. The mean Epworth score in patients with GERD symptoms was significantly higher than in those without GERD symptoms (n=340). Of the 45 patients, 16 were already receiving acid-suppressive therapy. Twenty-nine were not diagnosed with GERD and were not taking any specific treatment directed at GERD. Symptoms of GERD were therefore present in a total of 45 of the 385 patients, of whom 29 (7.5%) were not receiving treatment. The prevalence of symptomatic reflux disease was 11.7%.
Of the 340 patients without GERD symptoms by the RDQ questionnaire, 27 were taking a proton pump inhibitor (PPI) and/or H2 blocker, with relief of their symptoms. These 27 individuals had a mean RDQ score of 2.11 (well below the threshold for a diagnosis of GERD). Medication use was as follows: single daily dose of PPI (n=19), H2 blocker BID or QD (n=7), and one or a combination of PPI and H2 blocker.
Daytime sleepiness measurement
Table 2 reports the differences between subjects with and those without symptoms of GERD. Subjects with GERD symptoms had significantly higher daytime sleepiness scores compared to those without symptoms. There were no differences in gender, BMI, smoking, or alcohol use between the two groups.
Multiple regression
The only variables significant at the P<0.05 level were the RDQ score, BMI, and age. The RDQ score was significantly and positively associated with the Epworth Sleepiness Scale and BMI. Age was negatively associated with Epworth scale. The adjusted R 2 was 0.054, indicating that the model accounts for only about 5% of the variation in the sleepiness scale (Table 3).
Results
Three hundred eighty-five subjects participated in the study. Table 1 reports the characteristics of the study population.
Discussion
The interplay between gastroesophageal reflux and sleep has largely been studied in patients with an established diagnosis of GERD and in healthy volunteers. In healthy individuals, acid perfused into the distal esophagus is more likely to migrate into the proximal esophagus during sleep than in the waking state and acid clearance times are longer in the midesophagus and proximal esophagus during sleep compared with the waking state [13]. Experimental studies have shown that brief arousals from sleep reduce daytime alertness the following day by fragmenting sleep [14, 15]. In an earlier study of patients undergoing polysomnography for possible sleep apnea, we showed that gastroesophageal reflux was associated with an increased rate of arousals, decreased durations spent in the deeper stages of sleep, and poorer sleep-related quality of life [16]. A recent study demonstrated that patients with GERD and sleep disturbances had an increased rate of arousals from sleep and that acid inhibitory therapy with omeprazole decreased the rate of arousals from sleep [4]. Our study adds to this information by demonstrating that unrecognized GERD is frequently found in patients presenting for sleep evaluations and that greater daytime sleepiness is found in patients with GERD symptoms. In keeping with other studies, our multivariate analysis showed that sleep disturbance was associated with increasing age and with an increase in BMI [17, 18].
In keeping with other cross-sectional studies, our study has several limitations. It does not establish a causal relationship between reflux and sleep disturbance but this relationship has been demonstrated before. It does, however, demonstrate that a substantial number of patients presenting to sleep laboratories have unrecognized GERD. Further study is necessary to determine if the treatment of these patients improves or resolves their sleep disorder. Advantages of our study design include the evaluation of consecutive patients, the use of validated instruments, and the use of a community-based sample which provides a more accurate representation of real-life conditions. A limitation of the use of the RDQ is that it does not specifically assess nocturnal symptoms; but many nocturnal reflux events are unrecognized and may not be recalled by the subject [19]. Recognizing and treating GERD in patients presenting with sleep disturbances may be a useful therapeutic intervention and deserves further study.
References
Locke GR, III, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ, III (1997) Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology 112(5):1448–1456
Shaker R, Castell DO, Schoenfeld PS, Spechler SJ (2003) Nighttime heartburn is an under-appreciated clinical problem that impacts sleep and daytime function: the results of a Gallup survey conducted on behalf of the American Gastroenterological Association. Am J Gastroenterol 98(7):1487–1493
Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S (1993) The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med 328(17):1230–1235
Dimarino AJ Jr, Banwait KS, Eschinger E, Greenberg A, Dimarino M, Doghramji K, Cohen S (2005) The effect of gastro-oesophageal reflux and omeprazole on key sleep parameters. Aliment Pharmacol Ther 22(4):325–329
Johns MW (1991) A new method for measuring daytime sleepiness: the Epworth Sleepiness Scale. Sleep 14(6):540–545
Johns MW (1992) Reliability and factor analysis of the Epworth Sleepiness Scale. Sleep 15(4):376–381
Johns MW (2000) Sensitivity and specificity of the multiple sleep latency test (MSLT), the maintenance of wakefulness test and the Epworth Sleepiness Scale: failure of the MSLT as a gold standard. J Sleep Res 9(1):5–11
Johns MW (1994) Sleepiness in different situations measured by the Epworth Sleepiness Scale. Sleep 17(8):703–710
Long ME, Shaw MJ, Adlis S, et al. (2003) Self-reported use and benefit of OTC H2RA in the community. Gastroenterology 124 (Suppl 1):A619
Chinese GERD Study Group (2004) Value of reflux diagnostic questionnaire in the diagnosis of gastroesophageal reflux disease. Chin J Dig Dis 5(2):51–55
Nocon M, Kulig M, Leodolter A, Malfertheiner P, Willich SN (2005) Validation of the Reflux Disease Questionnaire for a German population. Eur J Gastroenterol Hepatol 17(2):229–233
Shaw MJ, Talley NJ, Beebe TJ, et al. (2001) Initial validation of a diagnostic questionnaire for gastroesophageal reflux disease. Am J Gastroenterol 96(1):52–57
Orr WC, Elsenbruch S, Harnish MJ, Johnson LF (2000) Proximal migration of esophageal acid perfusions during waking and sleep. Am J Gastroenterol 95(1):37–42
Bonnet MH (1989) The effect of sleep fragmentation on sleep and performance in younger and older subjects. Neurobiol Aging 10(1):21–25
Bonnet MH (1989) Infrequent periodic sleep disruption: effects on sleep, performance and mood. Physiol Behav 45(5):1049–1055
Guda N, Partington S, Vakil N (2004) Symptomatic gastro-oesophageal reflux, arousals and sleep quality in patients undergoing polysomnography for possible obstructive sleep apnoea. Aliment Pharmacol Ther 20(10):1153–1159
Vorona RD, Winn MP, Babineau TW, Eng BP, Feldman HR, Ware JC (2005) Overweight and obese patients in a primary care population report less sleep than patients with a normal body mass index. Arch Intern Med 165(1):25–30
Gander PH, Marshall NS, Harris R, Reid P (2005) The Epworth Sleepiness Scale: influence of age, ethnicity, and socioeconomic deprivation. Epworth Sleepiness scores of adults in New Zealand. Sleep 28(2):249–253
Orr WC, Johnson LF (1998) Responses to different levels of esophageal acidification during waking and sleep. Dig Dis Sci 43(2):241–245
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Guda, N., Partington, S., Shaw, M.J. et al. Unrecognized GERD Symptoms Are Associated with Excessive Daytime Sleepiness in Patients Undergoing Sleep Studies. Dig Dis Sci 52, 2873–2876 (2007). https://doi.org/10.1007/s10620-007-9768-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-007-9768-6