
Abstract
Purpose of Review
Gastroesophageal reflux disease is one of the most common conditions encountered by primary care physicians, gastroenterologists, foregut surgeons and otolaryngologists. While approximately 50% of patients experience nocturnal reflux symptoms, the relationship between gastroesophageal reflux disease and sleep is often overlooked. The aim of this review is to provide an update on the current understanding of this relationship and its clinical implications. Recent studies pertaining to the association between GERD and sleep with focus on sleep disturbances, obstructive sleep apnea, extraesophageal manifestations of GERD and treatment are discussed.
Recent Findings
There is a close relationship between GERD and sleep disturbances, but the nature of this relationship remains to be elucidated. Similarly, new data supports the association between GERD and obstructive sleep apnea, but whether this association is independent of confounding risk factors remains unresolved. Extraesophageal manifestations due to nocturnal GERD are primarily respiratory and can be explained by microaspiration and vagally-induced bronchospasm. Treatment of nocturnal GERD, both pharmacologically and surgically, improves sleep quality. Conversely, pharmacologic treatment of sleep disorders can improve nocturnal GERD symptoms.
Summary
There is a bi-directional relationship between GERD and sleep. GERD is associated with various sleep disturbances. Sleep deficiency can exacerbate GERD. There is an association between extraesophageal manifestations and nocturnal GERD. Treatment directed towards GERD can improve sleep experience, and treatment directed to improve sleep can improve GERD symptoms.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastroesophageal reflux disease (GERD) is a chronic disorder which develops when the reflux of stomach contents into the esophagus causes troublesome symptoms or complications [34]. Typical GERD symptoms include heartburn and regurgitation. Atypical and extra-esophageal symptoms may occur due to gastroesophageal reflux into the larynx, pharynx, oral cavity and pulmonary system [53]. GERD is a very common condition, affecting 18–28% of the US adult population [10]. An estimated 13% of the world’s population [15] and 20% of the US population experience GERD symptoms at least once per month [70]. GERD also exerts a large burden on the healthcare system, costing an estimated $10 billion annually in the US [63].
Good sleep hygiene is a key component to general health and quality of life [55•]. Yet, 35% of Americans do not achieve the recommended 7–9 h of sleep per night [75]. In fact, many sleep no more than 5–6 h per night and thus fall under the category of being sleep deprived. The average amount of time people sleep has declined by 2 h in the past century [45].
Both the duration and quality of sleep are important. Interruption of sleep quality occurs due to sleep fragmentation from nighttime arousals or awakenings [69]. Sleep deficiency can lead to numerous health-related disorders such as impaired cognition, anxiety and depression, obesity, dementia, diabetes mellitus, reduced immune response, cardiovascular disease, motor vehicle, work related, and at-home accidents, poor quality of life, and increase in all-cause mortality [69]. Severe daytime sleepiness occurs in approximately 20% of the US population [75]. Some authors have also recently noted the importance of a proper alignment of the sleep/wake cycle with the circadian cycle of the body in achieving healthy sleep [55•]. The circadian rhythm is primarily represented physiologically in changes of body temperature and secretion of melatonin. As these properties of the circadian cycle also have an effect on gastrointestinal physiology, the authors suggest that for optimal sleep and gut-related health, sleep/wake times and meal times should match the circadian cycle as closely as possible [55•].
The Association between GERD and Sleep Disturbances
The association between GERD and sleep disturbances has been known in the literature for a long time [27, 53], especially in terms of the overlap between GERD symptoms and reported sleep disorders [47] (Table 1). Prior studies have shown that patients with nocturnal GERD symptoms are 50% more likely to experience sleep disturbances than those with daytime only GERD symptoms [47]. In a large cross-sectional study, patients with self-reported nighttime awakenings and waking up tired at least eight times per month were nearly twice as likely to have heartburn and regurgitation compared to patients with less than eight sleep awakenings per month [8].
A recent small study that surveyed patients with a variety of gastrointestinal disorders at a tertiary care GI clinic offered further support for this association [3]. The authors found that of the 29 patients with GERD, 60% had self-reported poor sleep, as compared with 38% of the healthy controls, 37% clinical insomnia (18% in healthy controls), and 32% took a medication for sleep at least once per week (15% in healthy controls).
Other recent studies have provided further support for the association between GERD and sleep disturbances. One large cross-sectional study investigated the association between various gastrointestinal symptoms and sleep disturbances [26]. The authors found an odds ratio of 1.48 for the association between the symptom of acid regurgitation and sleep disturbances. Another similar study found that patients with sleep disturbances were more likely to experience severe GERD symptoms and had a higher prevalence of non-erosive reflux disease (OR 1.88, p < 0.004) than patients who did not report sleep disturbance when presenting for their health checkups [41].
Other studies have demonstrated that the association between GERD and sleep disturbances is a global phenomenon and affects both genders. An Australian community-based study, in which 1612 men completed a GERD symptom questionnaire, found a significant positive correlation between severity of GERD symptoms and self-reported poor quality of sleep (OR, 1.8; 95% CI, 1.2–2.9) [52]. A similar Japanese study found that the rate of sleep disturbances was approximately 36% among GERD patients, compared to 15% in controls (P < 0.001), and that sleep duration was significantly shorter in patients with erosive esophagitis [51]. The patients with symptomatic GERD also had a higher assessment of sleep disturbances on the Athens Insomnia Score (AIS), which includes several parameters of sleep including overall quality of sleep (mean score 0.73 ± 0.67 on 4-point scale vs. 0.47 ± 0.60 in patients without GERD, P < 0.01), and total sleep duration (mean score 0.70 ± 0.64 on 4-point scale vs. 0.47 ± 0.58 in patients without GERD). A Swedish study that followed a large group of women over 10 years found that those with persistent nocturnal GERD symptoms have significantly higher prevalence of daytime sleepiness than those without nocturnal GERD symptoms [23]. This finding offered further support to a prior survey study of over 15,000 patients that showed a strong association between nocturnal heartburn and snoring, daytime sleepiness, and insomnia [17]. This study also noted that benzodiazepines, which are commonly used to improve insomnia, are strongly associated with nocturnal heartburn, presumably due to their effect on lower esophageal sphincter basal pressure, transient lower esophageal sphincter relaxation rate and gastric motility.
Bidirectional Relationship
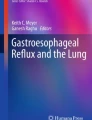
It has been proposed that GERD and sleep demonstrate a bidirectional relationship, where GERD can lead to sleep deficiency and in turn sleep deficiency by itself can lead to GERD, resulting in a vicious cycle (Fig. 1) [66••]. GERD has been shown to result in sleep fragmentation due to conscious awakenings that can be associated with reflux symptoms, or more commonly due to multiple amnestic arousals [61]. In contrast, sleep deficiency can lead to increase in esophageal hypersensitivity and esophageal acid exposure, both acutely and chronically, in GERD patients [55•, 61].

The bi-directional relationship between GERD and sleep efficiency (Adapted from Shibli et al, Nocturnal gastroesophageal reflux disease (GERD) and sleep: an important relationship that is commonly overlooked. J Clin Gastroenterol)
The theory that sleep deprivation leads to increased esophageal hypersensitivity was bolstered by a 2016 study in which patients with sleep deficiency exhibited a heightened sensitivity to capsaicin infusion into the esophagus [78]. Another small study showed that self-reported poor sleep was correlated with a higher number of supine reflux events and longer duration of reflux events on ambulatory pH monitoring [9]. The same study also demonstrated that subjects were more likely to wake up during acid reflux events as detected on pH monitoring than during a time of normal esophageal pH. Furthermore, in a small subset who underwent polysomnography concomitantly with pH monitoring, 76% of detected acid reflux events were followed by a disruption of sleep, most commonly awakening for 30 s, or less frequently moving from a deeper to a lighter phase of sleep. An additional 14% had a reflux event immediately after awakening from a deep sleep. In another study, in which patients underwent simultaneous pH testing and actigraphy, the authors found that more than half of all nighttime awakenings were associated with reflux events [58]. However, in contrast to the prior study, they also noted that in almost all cases of awakenings associated with reflux events, the awakening occurred before the reflux event. While both of these studies suggested a causal relationship between GERD and sleep disturbances, the former study implies that the primary relationship is that GERD causes sleep disturbances, while the latter study implies the opposite.
In a recently published study, simultaneous pH-impedance testing and in-lab polysomnography were performed on a small number of patients to determine the temporal relationship between nocturnal reflux events and arousal from sleep [65••]. Overall, 96% of the detected reflux events occurred immediately after a brief arousal, but only 20% of all reflux events had an arousal that occurred afterward. The authors hypothesized that increase in transient lower esophageal sphincter relaxations that occur after awakenings likely explain the increase in reflux events after awakening. Furthermore, the authors observed that patients who had nocturnal reflux events during their study had no difference in sleep duration, efficiency, architecture, or awakenings compared to patients who did not have nocturnal reflux events. This study was supportive of the theory that it is primarily disturbed sleep which triggers worsening of GERD symptoms, rather than a bi-directional relationship.
In addition to possibly inducing immediate nocturnal reflux, interruption of sleep has recently been shown to increase esophageal acid exposure the next day. In a recent randomized controlled, cross-over study, patients with GERD and healthy controls were randomized to sleep deprivation (3 h) or good sleep (7–8 h), and after a washout period crossed over to the other arm. Patients with GERD demonstrated more than threefold higher esophageal acid exposure time after sleep deprivation as compared to normal sleep [77]. Furthermore, nearly half of healthy controls developed an abnormal esophageal acid exposure time after sleep deprivation while all had normal esophageal acid exposure time after normal sleep. The authors hypothesized that this finding may in part be due to increase in ghrelin and decrease in leptin blood levels that occur after sleep deprivation, leading to increase in craving and thus food consumption [62]. This study takes the bi-directional model one step further by demonstrating that the effects of poor sleep on GERD are not limited to esophageal hypersensitivity but also affect the basic underlying mechanisms of gastroesophageal reflux. Alterations in normal sleep of GERD patients contribute to an increase in severity of GERD by increasing overall acid exposure and reducing the esophageal thresholds for symptom perception. The studies support symptomatic effect but have not yet substantiated a mucosal effect.
GERD and OSA
Obstructive sleep apnea (OSA) is the most common breathing-related sleep disorder [79]. It is characterized by repetitive upper airway collapse leading to recurrent obstructive apnea, hypopnea, or nocturnal arousal related to respiratory effort. The relationship between OSA and GERD remains to be elucidated. Some studies suggested a causal relationship, while others proposed that the apparent relationship is due to common risk factors, such as obesity, rather than a causal effect of GERD on OSA or vice versa [36, 40, 48, 57, 80].
Despite difficulties in establishing causation between GERD and OSA, recent studies have continued to find an association between the two disorders. A recent meta-analysis found that OSA is associated with GERD, with an OR of 1.75 (95% CI 1.18–2.59) [76]. Another recent study using a reflux symptom questionnaire and video laryngoscopy found that more than 64% of patients with laryngopharyngeal reflux had OSA [5]. In fact, Erdem et al. [13] showed that OSA is even more strongly associated with laryngopharyngeal reflux (LPR) than GERD. Another recent study found that higher scores on a reflux questionnaire could be predictive of OSA in patients undergoing polysomnography [72]. Lastly, Gilani et al. [20] demonstrated that GERD is independently associated with OSA with OR 2.13 (95% CI 1.17–3.88) even after adjusting for possible confounding factors including age, gender, ethnicity, obesity, asthma, other pulmonary diseases, sinonasal and laryngopharyngeal disorders.
Whether severity of GERD correlates with severity of OSA also remains unknown. A recently published study has failed to show a correlation between severity of OSA with severity of GERD or laryngopharyngeal reflux, nor any correlation between timing of disordered breathing events and reflux episodes [13]. On the other hand, several recent studies demonstrated that GERD is associated with more severe phenotypes of OSA, and vice versa. One study showed that patients with more severe sleep apnea were more likely to have reflux, and that obesity was a positive predictor of reflux in patients with OSA [5]. Similarly, another study found that sleep indices related to OSA were more severely abnormal in patients with erosive esophagitis compared to those with GERD symptoms but a normal upper endoscopy [37]. Conversely, the presence of OSA has been associated with more severe phenotypes of GERD as well. A study showed that patients with OSA are three times more likely to have Barrett’s esophagus than patients without OSA [22]. This association increased with worsening severity of OSA. However, a recent retrospective study showed that even patients with polysomnography-proven severe OSA were no more likely to have GERD symptoms based on a questionnaire than those without OSA [33]. The study was unable to demonstrate that daytime sleepiness and mood symptoms were associated with GERD. In summary, there is clear association between GERD and OSA, but the exact underlying mechanisms that explain this association remain to be determined.
Recent studies have also demonstrated that treatment of GERD and OSA is mutually beneficial. One study demonstrated that continuous positive airway pressure (CPAP) treatment for OSA significantly decreased the prevalence of nocturnal GERD symptoms [71]. A total of 79 patients with OSA and nocturnal heartburn were treated with CPAP. The post-treatment mean Epworth sleepiness scale (ESS) score decreased by 43% (from 12.05 to 6.95, p = 0.0001) and the mean heartburn score decreased by 62% (from 3.69 to 1.38, p = 0.0001). Another recent study showed that CPAP effectively treats LPR in addition to GERD [74]. Li et al. recently published a meta-analysis of 10 studies that showed CPAP is effective in reducing esophageal acid exposure time, duration of longest reflux event, number of reflux events, and DeMeester score in patients with OSA [42]. The aforementioned studies support the findings of prior research [36].
Extraesophageal Manifestations
Nocturnal GERD has been demonstrated to be more commonly associated with extra-esophageal manifestations of GERD than daytime GERD [16, 21, 53]. However, the exact mechanism for this relationship remains to be elucidated. In a recent prospective study, Emilsson et al. [11] showed that nocturnal GERD is associated with both asthma-like respiratory symptoms such as shortness of breath, wheezing, chest tightness, and nocturnal cough, as well as bronchitis-like symptoms such as productive cough. Importantly, the authors documented both inflammatory and neurogenic serum biomarkers which were present at higher levels in patients with nocturnal GERD. These results suggested that both microaspiration of gastric contents causing inflammation and irritation, and reflux-induced vagal reflex leading to bronchoconstriction play an important role in symptom generation. The same study also determined a strong association between nocturnal GERD and snoring. In a subsequent similar study using data from a large, international cross-sectional study surveying randomly selected patients from the general population, the same investigators showed that patients with both snoring and nocturnal GERD had a greater association with both asthma-like and bronchitis-like respiratory symptoms than either nocturnal GERD or snoring alone [12]. In this study, snoring, but not nocturnal GERD, was associated with a gradual decline in pulmonary function.
GERD Treatment
Presently, treatment of nocturnal GERD and its associated sleep disturbances includes lifestyle modifications, pharmacologic therapy, endoscopic and surgical interventions, as well as complementary and alternative therapies (Table 2). As proposed in Fig. 2, therapeutic interventions that improve GERD can reduce sleep deficiency and those that improve sleep can reduce GERD severity. It is yet to be determined if combined treatment, for both sleep and GERD, can provide a better outcome than any of these therapeutic approaches alone [66••].

The effect of GERD or sleep treatment on the bidirectional relationship between GERD and sleep deficiency
Lifestyle modifications that have been proven to reduce nocturnal GERD include elevation of the head of bed, weight loss [31], avoidance of the right lateral decubitus position [24], and avoidance of eating meals 3 h prior to bedtime [14]. Avoidance of symptom-triggering foods such as coffee, chocolate, carbonated beverages, fatty and greasy foods, and alcohol are also commonly recommended [66••], though evidence to support the efficacy of specific food-avoidance in nocturnal GERD is scant [50].
Recent developments in lifestyle modification for nocturnal GERD includes the MedCline Reflux System, a positional medical device that maintains patients in the left lateral decubitus position by using a curved body pillow. In one study using this positional system, the authors demonstrated that nocturnal GERD Symptom Severity and Impact Questionnaire (N-GSSIQ) scores significantly improved by 68% (P < 0.001), and Health-Related Quality of Life questionnaire (GERD-HRQL) scores improved by 44% (P < 0.001) [2]. The authors also found an 87% decrease in esophageal acid exposure time.
In patients whose nocturnal symptoms are not controlled by lifestyle modifications alone, pharmacotherapy should be considered. When symptoms are mild and intermittent and not associated with esophageal mucosal injury, antacids [73] and histamine-2 receptor antagonists (H2RAs) [59] can be effective at reducing symptoms. Otherwise, proton pump inhibitors (PPIs) remain the mainstay of pharmacologic therapy for GERD. PPI treatment alone or in combination with H2RA at bedtime have been shown to reduce nocturnal reflux symptoms and improve sleep disturbances [6, 30, 59, 64]. Recent studies have also supported use of antacids and H2RAs for breakthrough symptoms in patients already taking PPIs. Gaviscon is an antacid that also includes alginate, which can form a raft on top of the acid pocket, a layer of acid in the proximal stomach purported to form on top of a recently ingested meal [49]. It can be presumed that symptoms related to the acid pocket are most likely to occur when the patient is in the recumbent position as is most common in nocturnal GERD. In one study that was open label and uncontrolled, the addition of alginate to PPI therapy led to subjective improvement in reflux symptoms by at least one point on a 5-point Likert scale in 72% of patients [49]. The improvement was even more pronounced in patients with higher severity of baseline symptoms. The authors also noted improvement in sleep disturbances based on GERD-Q questionnaire scores. Another recent study supported the value of combination of PPI with H2RA in GERD patients with sleep disturbances. The authors demonstrated that 4 weeks of combined H2RA with PPI was more effective than either drug alone in increasing total sleep time and duration of stages 3 and 4 of sleep, while decreasing nighttime awakenings and the apnea/hypopnea index [43].
Baclofen, a GABA (B) agonist, which reduces the rate of transient LES relaxations, was found to reduce the number of reflux events, improve total sleep time (440.8 vs 386.9 min) and improve sleep efficiency (91.7% vs 80.5%) compared to placebo in one study [54]. The authors recommended baclofen as an adjunctive therapy to PPIs in patients with residual nocturnal symptoms.
When patients do not respond to PPI therapy in combination with antacids or H2RAs, Potassium-competitive acid blockers (P-CABs) are a promising novel therapy. These are acid secretion suppressants with rapid onset and sustained action. These medications have rapid heartburn relief effect, faster healing of erosive esophagitis and better control of nighttime acid secretion than PPIs [67]. Vonoprazan, a potent P-CAB, was compared with lansoprazole in a randomized, double-blind, controlled trial that included 32 patients with erosive esophagitis. Clinical outcomes included relief of day and nighttime heartburn. By the end of a seven-day treatment period, nearly 70% of the patients receiving vonaprazan had complete relief of nocturnal heartburn, compared to only 10% in the lansoprazole group (P < 0.01) [56••].
Patients with symptoms refractory to all pharmacologic therapy, or patients who prefer to avoid medications often consider antireflux procedures, which can be endoscopic or surgical. Thus far, endoscopic therapies have not reported their effects on nocturnal GERD symptoms or sleep disturbances [18, 60].
Surgical therapy includes various degrees of fundoplication and magnetic sphincter augmentation. Nissen fundoplication has been shown to be effective at reducing nocturnal GERD symptoms [7]. Studies have also demonstrated that anti-reflux surgery improves subjective sleep parameters. One small study found that Nissen fundoplication improved the proportion of nights that a patient is in deep sleep, and patient-reported quality of sleep, but without a large change in objective sleep parameters [7]. Recently, several questionnaire studies demonstrated a trend towards less sleeplessness among patients who underwent anti-reflux surgery [29, 39]. One recently published small study was the first to compare recumbent reflux before and after fundoplication using impedance-pH testing. The study documented a marked reduction in recumbent reflux events after surgery [25•]. Interestingly, the authors found that most of the recumbent reflux events in the subgroup of patients with complications of reflux disease, were non-acidic. The authors also demonstrated that 42% of the patients with self-reported sleep disturbances prior to surgical fundoplication were found to have abnormal nighttime reflux. The majority of these patients noted improvement in their sleep experience after surgery.
Lastly, the LINX ™ device (magnetic sphincter augmentation technology) for endoscopic antireflux treatment has been determined to be as effective as laparoscopic fundoplication in preventing daytime and nighttime GERD symptoms [1, 81•]. In a recent meta-analysis, one study assessed the effect of LINX on sleep disturbances and found that prior to the procedure 65% of the patients had a history of perceived nocturnal awakenings due to heartburn, compared to 4% 4 weeks after the procedure (P < 0.001) [81•].
Patients who do not respond to traditional therapies or who prefer the approach of complementary and alternative medicine may find benefit from Rikkunshito, a traditional Japanese medicine used in the treatment of functional upper gastrointestinal disorders. In animal models, this therapy was found to have a protective effect on esophageal mucosa [46]. In a recent open-label uncontrolled study, patients with GERD symptoms refractory to PPI were given 6–8 weeks treatment with Rikkunshito in addition to PPI. The authors demonstrated that the patients had a small but significant improvement in dissatisfaction due interrupted sleep (2.81–2.64 on a 5-point visual analog scale, P = 0.035) [35]. The authors did not find a significant improvement in dissatisfaction due to difficulty falling asleep in the patients who received Rikkunshito.
Sleep Treatment
Another approach to the management of nocturnal GERD is to improve patients’ sleep experience. Based on the bidirectional model between sleep and GERD (Fig. 1), interruption of the connecting arm between poor sleep and GERD severity, may improve both GERD and sleep.
In one study, zolpidem reduced GERD-related nighttime awakenings, but unfortunately it prolonged the duration of nocturnal acid reflux events, potentially increasing the risk of GERD complications [19]. Melatonin, commonly used for insomnia, is also thought to be an effective treatment for GERD. In one study, patients with GERD were found to have lower serum levels of melatonin than the general population [38], raising the possibility that it might be used as a therapeutic modality for GERD. Melatonin has also been shown to have a protective effect against esophageal mucosal injury [4], including potentially preventing progression of Barrett’s esophagus to adenocarcinoma of the esophagus [44]. Previous randomized controlled trials have demonstrated that melatonin is an effective treatment that reduces nocturnal heartburn and regurgitation when used in combination with a supplement containing tryptophan, vitamin B6, vitamin B12, methionine and betaine [68], as monotherapy, and in combination with omeprazole [32]. In addition to symptom improvement, 8 weeks of treatment with melatonin led to an increase in LES resting pressure from 10.0 mmHg (SD 1.58) to 20.2 mmHg (SD1.56) (P < 0.05) and an increase in the average pH at 5 cm above the gastroesophageal junction over a 24 h period from 2.3 (SD 0.36) to 6.7 (SD 0.65) (P < 0.05). Recently, this mechanism of treatment has been extended to ramelteon, a melatonin receptor agonist [28]. After undergoing an upper endoscopy 16 patients were randomized to 8 weeks of ramelteon 8 mg at bedtime vs. placebo. The ramelteon group experienced a significant decrease in GERD symptoms that was most pronounced in nighttime heartburn (42% decrease in symptoms compared to 78% increase in the placebo group, P < 0.05) based on the GERD symptom assessment scale. As expected, ramelteon also significantly improved several parameters of sleep quality on actigraphy testing, including sleep efficiency and sleep latency.
Conclusions
Nocturnal GERD symptoms and its associated sleep disorders are both common and significantly impact quality of life. In addition, there is an association between GERD and OSA but the nature of this relationship remains to be elucidated. Moreover, evidence is conflicting as to whether GERD and sleep disturbances causally linked to each other in a bi-directional manner or if it is primarily sleep disturbances that drive nocturnal GERD. Regardless, poor sleep quality is associated with increase in esophageal hypersensitivity and overall acid exposure. Extraesophageal manifestations of GERD are partly driven by nighttime gastroesophageal reflux. Treatment of GERD improves sleep quality and treatment of sleep disorders can improve GERD. In addition to medical therapy, surgical interventions have been shown to improve nocturnal GERD and sleep disturbances.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Aiolfi A, Asti E, Bernardi D, et al. Early results of magnetic sphincter augmentation versus fundoplication for gastroesophageal reflux disease: systematic review and meta-analysis. Int J Surg. 2018;52:82–8. https://doi.org/10.1016/j.ijsu.2018.02.041.
Allampati S, Lopez R, Thota PN, Ray M, Birgisson S, Gabbard SL. Use of a positional therapy device significantly improves nocturnal gastroesophageal reflux symptoms. Dis Esophagus. 2017;30(3):1–7. https://doi.org/10.1111/dote.12495.
Ballou S, Alhassan E, Hon E, et al. Sleep disturbances are commonly reported among patients presenting to a gastroenterology clinic. Dig Dis Sci. 2018;63(11):2983–91. https://doi.org/10.1007/s10620-018-5237-7.
Brzozowska I, Strzalka M, Drozdowicz D, Konturek SJ, Brzozowski T. Mechanisms of esophageal protection, gastroprotection and ulcer healing by melatonin. implications for the therapeutic use of melatonin in gastroesophageal reflux disease (GERD) and peptic ulcer disease. Curr Pharm Des. 2014;20(30):4807–15. https://doi.org/10.2174/1381612819666131119110258.
Caparroz FA, de Milena ATC, Regina CG, et al. Clinical and polysomnographic predictors of laryngopharyngeal reflux in obstructive sleep apnea syndrome. Braz J Otorhinolaryngol. 2019;85(4):408–15. https://doi.org/10.1016/j.bjorl.2018.03.007.
Chand N, Johnson DA, Tabangin M, Ware JC. Sleep dysfunction in patients with gastro-oesophageal reflux disease: prevalence and response to GERD therapy, a pilot study. Aliment Pharmacol Ther. 2004;20(9):969–74. https://doi.org/10.1111/j.1365-2036.2004.02213.x.
Cohen JA, Arain A, Harris PA, et al. Surgical trial investigating nocturnal gastroesophageal reflux and sleep (STINGERS). Surg Endosc. 2003;17(3):394–400. https://doi.org/10.1007/s00464-002-8912-9.
Cremonini F, Camilleri M, Zinsmeister AR, Herrick LM, Beebe T, Talley NJ. Sleep disturbances are linked to both upper and lower gastrointestinal symptoms in the general population. Neurogastroenterol Motil. 2009;21(2):128–35. https://doi.org/10.1111/j.1365-2982.2008.01181.x.
Dickman R, Green C, Fass SS, et al. Relationships between sleep quality and pH monitoring findings in persons with gastroesophageal reflux disease. J Clin Sleep Med. 2007;3(5):505–13.
El-Serag HB, Sweet S, Winchester CC, Dent J. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2014;63(6):871–80. https://doi.org/10.1136/gutjnl-2012-304269.
Emilsson ÖI, Benediktsdóttir B, Ólafsson Í, et al. Respiratory symptoms, sleep-disordered breathing and biomarkers in nocturnal gastroesophageal reflux. Respir Res. 2016;17(1):115. https://doi.org/10.1186/s12931-016-0431-7.
Emilsson ÖI, Hägg SA, Lindberg E, et al. Snoring and nocturnal reflux: association with lung function decline and respiratory symptoms. ERJ Open Research. 2019;5(2) https://doi.org/10.1183/23120541.00010-2019.
Erdem D, Yılmaz YF, Özcan M, Titiz A, Özlügedik S, Ünal A. Correlation of sleep-disordered breathing and laryngopharyngeal reflux: a two-channel triple-sensor pHmetry catheter study. Eur Arch Otorhinolaryngol. 2018;275(10):2585–92. https://doi.org/10.1007/s00405-018-5107-0.
Esmaillzadeh A, Keshteli AH, Feizi A, Zaribaf F, Feinle-Bisset C, Adibi P. Patterns of diet-related practices and prevalence of gastro-esophageal reflux disease. Neurogastroenterol Motil. 2013;25(10):831–e638. https://doi.org/10.1111/nmo.12192.
Eusebi LH, Ratnakumaran R, Yuan Y, Solaymani-Dodaran M, Bazzoli F, Ford AC. Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: a meta-analysis. Gut. 2018;67(3):430–40. https://doi.org/10.1136/gutjnl-2016-313589.
Fass R. The relationship between gastroesophageal reflux disease and sleep. Curr Gastroenterol Rep. 2009;11(3):202–8. https://doi.org/10.1007/s11894-009-0032-4.
Fass R, Quan SF, O’Connor GT, Ervin A, Iber C. Predictors of heartburn during sleep in a large prospective cohort study. Chest. 2005;127(5):1658–66. https://doi.org/10.1378/chest.127.5.1658.
Fass R, Cahn F, Scotti DJ, Gregory DA. Systematic review and meta-analysis of controlled and prospective cohort efficacy studies of endoscopic radiofrequency for treatment of gastroesophageal reflux disease. Surg Endosc. 2017;31(12):4865–82. https://doi.org/10.1007/s00464-017-5431-2.
Gagliardi GS, Shah AP, Goldstein M, et al. Effect of zolpidem on the sleep arousal response to nocturnal esophageal acid exposure. Clin Gastroenterol Hepatol. 2009;7(9):948–52. https://doi.org/10.1016/j.cgh.2009.04.026.
Gilani S, Quan SF, Pynnonen MA, Shin JJ. Obstructive sleep apnea and gastroesophageal reflux: a multivariate population-level analysis. Otolaryngol Head Neck Surg. 2016;154(2):390–5. https://doi.org/10.1177/0194599815621557.
Gislason T, Janson C, Vermeire P, et al. Respiratory symptoms and nocturnal gastroesophageal reflux: a population-based study of young adults in three European countries. Chest. 2002;121(1):158–63. https://doi.org/10.1378/chest.121.1.158.
Hadi YB, Khan AA, Naqvi SFZ, Kupec JT. Independent association of obstructive sleep apnea with Barrett’s esophagus. J Gastroenterol Hepatol. 2020;35(3):408–11. https://doi.org/10.1111/jgh.14779.
Hägg SA, Emilsson ÖI, Franklin K, Janson C, Lindberg E. Nocturnal gastroesophageal reflux increases the risk of daytime sleepiness in women. Sleep Med. 2019;53:94–100. https://doi.org/10.1016/j.sleep.2018.08.036.
van Herwaarden MA, Katzka DA, Smout AJ, Samsom M, Gideon M, Castell DO. Effect of different recumbent positions on postprandial gastroesophageal reflux in normal subjects. Am J Gastroenterol. 2000;95(10):2731–6. https://doi.org/10.1111/j.1572-0241.2000.03180.x.
Hoshino M, Omura N, Yano F, et al. The evaluation of recumbent reflux by multichannel intraluminal impedance pH testing for patients with gastroesophageal reflux disease and sleep disturbance. Esophagus. 2020;17(3):348–54. https://doi.org/10.1007/s10388-020-00717-w. A study that reports the effect of anti-reflux surgery on nocturnal GERD.
Hyun MK, Baek Y, Lee S. Association between digestive symptoms and sleep disturbance: a cross-sectional community-based study. BMC Gastroenterol. 2019;19(1):34. https://doi.org/10.1186/s12876-019-0945-9.
Jansson C, Nordenstedt H, Wallander M-A, et al. A population-based study showing an association between gastroesophageal reflux disease and sleep problems. Clin Gastroenterol Hepatol. 2009;7(9):960–5. https://doi.org/10.1016/j.cgh.2009.03.007.
Jha LK, Fass R, Gadam R, et al. The effect of ramelteon on heartburn symptoms of patients with gastroesophageal reflux disease and chronic insomnia: a pilot study. J Clin Gastroenterol. 2016;50(2):e19–24. https://doi.org/10.1097/MCG.0000000000000322.
Johannessen R, Petersen H, Olberg P, Johnsen G, Fjøsne U, Kleveland PM. Airway symptoms and sleeping difficulties in operated and non-operated patients with gastroesophageal reflux disease. Scand J Gastroenterol. 2012;47(7):762–9. https://doi.org/10.3109/00365521.2012.683041.
Johnson DA, Orr WC, Crawley JA, et al. Effect of esomeprazole on nighttime heartburn and sleep quality in patients with GERD: a randomized, placebo-controlled trial. Am J Gastroenterol. 2005;100(9):1914–22. https://doi.org/10.1111/j.1572-0241.2005.00285.x.
Kaltenbach T, Crockett S, Gerson LB. Are lifestyle measures effective in patients with gastroesophageal reflux disease? An evidence-based approach. Arch Intern Med. 2006;166(9):965–71. https://doi.org/10.1001/archinte.166.9.965.
Kandil TS, Mousa AA, El-Gendy AA, Abbas AM. The potential therapeutic effect of melatonin in gastro-esophageal reflux disease. BMC Gastroenterol. 2010;10:7. https://doi.org/10.1186/1471-230X-10-7.
Kang HH, Lim C-H, Oh JH, Cho M-J, Lee SH. The influence of gastroesophageal reflux disease on daytime sleepiness and depressive symptom in patients with obstructive sleep apnea. J Neurogastroenterol Motil. 2020; https://doi.org/10.5056/jnm20071.
Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol. 2013;108(3):308–28; quiz 329. https://doi.org/10.1038/ajg.2012.444.
Kawai T, Hirayama Y, Oguchi A, et al. Effects of rikkunshito on quality of life in patients with gastroesophageal reflux disease refractory to proton pump inhibitor therapy. J Clin Biochem Nutr. 2017;60(2):143–5. https://doi.org/10.3164/jcbn.16-77.
Kerr P, Shoenut JP, Millar T, Buckle P, Kryger MH. Nasal CPAP reduces gastroesophageal reflux in obstructive sleep apnea syndrome. Chest. 1992;101(6):1539–44. https://doi.org/10.1378/chest.101.6.1539.
Kim Y, Lee YJ, Park JS, et al. Associations between obstructive sleep apnea severity and endoscopically proven gastroesophageal reflux disease. Sleep Breath. 2018;22(1):85–90. https://doi.org/10.1007/s11325-017-1533-2.
Klupińska G, Wiśniewska-Jarosińska M, Harasiuk A, et al. Nocturnal secretion of melatonin in patients with upper digestive tract disorders. J Physiol Pharmacol. 2006;57(Suppl 5):41–50.
Kumar A, Raja K, Kumar S, Quasimuddin N, Rizwan A. Quality of life in gastroesophageal reflux disease three months after laparoscopic Nissen’s fundoplication. Cureus. 2020;12(9):e10674. https://doi.org/10.7759/cureus.10674.
Kuribayashi S, Kusano M, Kawamura O, et al. Mechanism of gastroesophageal reflux in patients with obstructive sleep apnea syndrome. Neurogastroenterol Motil. 2010;22(6):611–e172. https://doi.org/10.1111/j.1365-2982.2010.01485.x.
Lei W-Y, Chang W-C, Wong M-W, et al. Sleep disturbance and its association with gastrointestinal symptoms/diseases and psychological comorbidity. Digestion. 2019;99(3):205–12. https://doi.org/10.1159/000490941.
Li C, Wu Z-H, Pan X-L, Yuan K. Effect of continuous positive airway pressure on gastroesophageal reflux in patients with obstructive sleep apnea: a meta-analysis. Sleep Breath. 2020; https://doi.org/10.1007/s11325-020-02224-9.
Liu C. Clinical efficacy of proton pump inhibitor combined with ranitidine in the treatment of throat reflux. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2020;34(8):710–2;718. https://doi.org/10.13201/j.issn.2096-7993.2020.08.008.
Majka J, Wierdak M, Brzozowska I, et al. Melatonin in prevention of the sequence from reflux esophagitis to Barrett’s esophagus and esophageal adenocarcinoma: experimental and clinical perspectives. Int J Mol Sci. 2018;19(7):2033. https://doi.org/10.3390/ijms19072033.
Martin SE, Wraith PK, Deary IJ, Douglas NJ. The effect of nonvisible sleep fragmentation on daytime function. Am J Respir Crit Care Med. 1997;155(5):1596–601. https://doi.org/10.1164/ajrccm.155.5.9154863.
Miwa H, Koseki J, Oshima T, et al. Rikkunshito, a traditional Japanese medicine, may relieve abdominal symptoms in rats with experimental esophagitis by improving the barrier function of epithelial cells in esophageal mucosa. J Gastroenterol. 2010;45(5):478–87. https://doi.org/10.1007/s00535-009-0180-1.
Mody R, Bolge SC, Kannan H, Fass R. Effects of gastroesophageal reflux disease on sleep and outcomes. Clin Gastroenterol Hepatol. 2009;7(9):953–9. https://doi.org/10.1016/j.cgh.2009.04.005.
Morse CA, Quan SF, Mays MZ, Green C, Stephen G, Fass R. Is there a relationship between obstructive sleep apnea and gastroesophageal reflux disease? Clin Gastroenterol Hepatol. 2004;2(9):761–8. https://doi.org/10.1016/s1542-3565(04)00347-7.
Müller M, Labenz G, Borkenstein D-P, Labenz J, Studiengruppe LOPA. Alginate on demand as add-on for patients with gastro-oesophageal reflux disease and insufficient PPI effect. Dtsch Med Wochenschr. 2019;144(4)):e30–5. https://doi.org/10.1055/a-0736-5959.
Newberry C, Lynch K. The role of diet in the development and management of gastroesophageal reflux disease: why we feel the burn. J Thorac Dis. 2019;11(Suppl 12):S1594–601. https://doi.org/10.21037/jtd.2019.06.42.
Okuyama M, Takaishi O, Nakahara K, et al. Associations among gastroesophageal reflux disease, psychological stress, and sleep disturbances in Japanese adults. Scand J Gastroenterol. 2017;52(1):44–9. https://doi.org/10.1080/00365521.2016.1224383.
On ZX, Grant J, Shi Z, et al. The association between gastroesophageal reflux disease with sleep quality, depression, and anxiety in a cohort study of Australian men. J Gastroenterol Hepatol. 2017;32(6):1170–1177. doi: https://doi.org/10.1111/jgh.13650
Orr WC. Gastrointestinal functioning during sleep: a new horizon in sleep medicine. Sleep Med Rev. 2001;5(2):91–101. https://doi.org/10.1053/smrv.2000.0149.
Orr WC, Goodrich S, Wright S, Shepherd K, Mellow M. The effect of baclofen on nocturnal gastroesophageal reflux and measures of sleep quality: a randomized, cross-over trial. Neurogastroenterol Motil. 2012;24(6):553–9, e253. https://doi.org/10.1111/j.1365-2982.2012.01900.x.
Orr WC, Fass R, Sundaram SS, Scheimann AO. The effect of sleep on gastrointestinal functioning in common digestive diseases. Lancet Gastroenterol Hepatol. 2020;5(6):616–24. https://doi.org/10.1016/S2468-1253(19)30412-1. Updated review of the physiologic relationship between sleep and GERD.
Oshima T, Arai E, Taki M, et al. Randomised clinical trial: vonoprazan versus lansoprazole for the initial relief of heartburn in patients with erosive oesophagitis. Aliment Pharmacol Ther. 2019;49(2):140–6. https://doi.org/10.1111/apt.15062. First randomized controlled trial to show the efficacy of P-CABs in nocturnal GERD.
Penzel T, Becker HF, Brandenburg U, Labunski T, Pankow W, Peter JH. Arousal in patients with gastro-oesophageal reflux and sleep apnoea. Eur Respir J. 1999;14(6):1266–70. https://doi.org/10.1183/09031936.99.14612669.
Poh CH, Allen L, Gasiorowska A, et al. Conscious awakenings are commonly associated with acid reflux events in patients with gastroesophageal reflux disease. Clin Gastroenterol Hepatol. 2010;8(10):851–7. https://doi.org/10.1016/j.cgh.2010.05.022.
Rackoff A, Agrawal A, Hila A, Mainie I, Tutuian R, Castell DO. Histamine-2 receptor antagonists at night improve gastroesophageal reflux disease symptoms for patients on proton pump inhibitor therapy. Dis Esophagus. 2005;18(6):370–3. https://doi.org/10.1111/j.1442-2050.2005.00518.x.
Richter JE, Kumar A, Lipka S, Miladinovic B, Velanovich V. Efficacy of laparoscopic Nissen fundoplication vs transoral incisionless fundoplication or proton pump inhibitors in patients with gastroesophageal reflux disease: a systematic review and network meta-analysis. Gastroenterology. 2018;154(5):1298–1308.e7. https://doi.org/10.1053/j.gastro.2017.12.021.
Schey R, Dickman R, Parthasarathy S, et al. Sleep deprivation is hyperalgesic in patients with gastroesophageal reflux disease. Gastroenterology. 2007;133(6):1787–95. https://doi.org/10.1053/j.gastro.2007.09.039.
Schmid SM, Hallschmid M, Jauch-Chara K, Born J, Schultes B. A single night of sleep deprivation increases ghrelin levels and feelings of hunger in normal-weight healthy men. J Sleep Res. 2008;17(3):331–4. https://doi.org/10.1111/j.1365-2869.2008.00662.x.
Shaheen NJ, Hansen RA, Morgan DR, et al. The burden of gastrointestinal and liver diseases, 2006. Am J Gastroenterol. 2006;101(9):2128–38. https://doi.org/10.1111/j.1572-0241.2006.00723.x.
Shaker R, Castell DO, Schoenfeld PS, Spechler SJ. Nighttime heartburn is an under-appreciated clinical problem that impacts sleep and daytime function: the results of a Gallup survey conducted on behalf of the American Gastroenterological Association. Am J Gastroenterol. 2003;98(7):1487–93. https://doi.org/10.1111/j.1572-0241.2003.07531.x.
Shepherd K, Ockelford J, Ganasan V, Holloway R, Hillman D, Eastwood P. Temporal relationship between night-time gastroesophageal reflux events and arousals from sleep. Am J Gastroenterol. 2020;115(5):697–705. https://doi.org/10.14309/ajg.0000000000000627. A study reporting that nocturnal awakenings due to primary sleep disorder induce nocturnal reflux, and not vice versa.
Shibli F, Skeans J, Yamasaki T, Fass R. Nocturnal gastroesophageal reflux disease (GERD) and sleep: an important relationship that is commonly overlooked. J Clin Gastroenterol. 2020a;54(8):663–74. https://doi.org/10.1097/MCG.0000000000001382. Most comprehensive and updated review of GERD and sleep.
Shibli F, Kitayama Y, Fass R. Novel therapies for gastroesophageal reflux disease: beyond proton pump inhibitors. Curr Gastroenterol Rep. 2020b;22(4):16. https://doi.org/10.1007/s11894-020-0753-y.
de Souza Pereira R. Regression of gastroesophageal reflux disease symptoms using dietary supplementation with melatonin, vitamins and aminoacids: comparison with omeprazole. J Pineal Res. 2006;41(3):195–200. https://doi.org/10.1111/j.1600-079X.2006.00359.x.
St-Onge M-P, Grandner MA, Brown D, et al. Sleep duration and quality: impact on lifestyle behaviors and cardiometabolic health: a scientific statement from the American Heart Association. Circulation. 2016;134(18):e367–86. https://doi.org/10.1161/CIR.0000000000000444.
Tack J, Becher A, Mulligan C, Johnson DA. Systematic review: the burden of disruptive gastro-oesophageal reflux disease on health-related quality of life. Aliment Pharmacol Ther. 2012;35(11):1257–66. https://doi.org/10.1111/j.1365-2036.2012.05086.x.
Tamanna S, Campbell D, Warren R, Ullah MI. Effect of CPAP therapy on symptoms of nocturnal gastroesophageal reflux among patients with obstructive sleep apnea. J Clin Sleep Med. 2016;12(9):1257–61. https://doi.org/10.5664/jcsm.6126.
Teklu M, Gouveia CJ, Yalamanchili A, et al. Predicting obstructive sleep apnea status with the reflux symptom index in a sleep study population. Laryngoscope. 2020;130(12):E952–7. https://doi.org/10.1002/lary.28592.
Tran T, Lowry AM, El-Serag HB. Meta-analysis: the efficacy of over-the-counter gastro-oesophageal reflux disease therapies. Aliment Pharmacol Ther. 2007;25(2):143–53. https://doi.org/10.1111/j.1365-2036.2006.03135.x.
Wang L, Han H, Wang G, et al. Relationship between reflux diseases and obstructive sleep apnea together with continuous positive airway pressure treatment efficiency analysis. Sleep Med. 2020;75:151–5. https://doi.org/10.1016/j.sleep.2020.07.024.
Wilson JF. Is sleep the new vital sign? Ann Intern Med. 2005;142(10):877–80. https://doi.org/10.7326/0003-4819-142-10-200505170-00026.
Wu Z-H, Yang X-P, Niu X, Xiao X-Y, Chen X. The relationship between obstructive sleep apnea hypopnea syndrome and gastroesophageal reflux disease: a meta-analysis. Sleep Breath. 2019;23(2):389–97. https://doi.org/10.1007/s11325-018-1691-x.
Yamasaki T, Quan SF, Fass R. The effect of sleep deficiency on esophageal acid exposure of healthy controls and patients with gastroesophageal reflux disease. Neurogastroenterol Motil. 2019;31(12):e13705. https://doi.org/10.1111/nmo.13705.
Yi C-H, Lei W-Y, Hung J-S, Liu T-T, Orr WC, Chen C-L. Sleep disturbance and enhanced esophageal capsaicin sensitivity in patients with gastroesophageal reflux disease. J Gastroenterol Hepatol. 2016;31(12):1940–5. https://doi.org/10.1111/jgh.13428.
Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328(17):1230–5. https://doi.org/10.1056/NEJM199304293281704.
Young T, Skatrud J, Peppard PE. Risk factors for obstructive sleep apnea in adults. JAMA. 2004;291(16):2013–6. https://doi.org/10.1001/jama.291.16.2013.
Zadeh J, Andreoni A, Treitl D, Ben-David K. Spotlight on the Linx™ reflux management system for the treatment of gastroesophageal reflux disease: evidence and research. Med Devices (Auckl). 2018;11:291–300. https://doi.org/10.2147/MDER.S113679. A study reporting the effect of the LINX procedure on sleep.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Esophagus
Rights and permissions
About this article

Cite this article
Kurin, M., Shibli, F., Kitayama, Y. et al. Sorting out the Relationship between Gastroesophageal Reflux Disease and Sleep. Curr Gastroenterol Rep 23, 15 (2021). https://doi.org/10.1007/s11894-021-00815-4
Accepted:
Published:
DOI: https://doi.org/10.1007/s11894-021-00815-4