
Abstract
Youth anxiety disorders are highly prevalent and are associated with considerable school impairment. Despite the identification of well-supported strategies for treating youth anxiety, research has yet to evaluate the differential effects of these treatments on anxiety-related school impairment. The present study leveraged data from the Child/Adolescent Anxiety Multimodal Study to examine differential treatment effects of CBT, sertraline, and their combination (COMB), relative to placebo (PBO), on anxiety-related school impairment among youth (N = 488). Latent growth modeling revealed that all three active treatments demonstrated superiority over PBO in reducing anxiety-related school impairment over time, with COMB showing the most robust effects. According to parent report, medication strategies may have stronger effects on anxiety-related school impairment among males than among females. Results were discrepant across parents and youth. Findings are discussed in terms of clinical implications for anxious youth and the need for continued research to examine treatment effects on anxiety-related school impairment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anxiety disorders affect up to 1/3rd of U.S. youth by the time they reach young adulthood [1] and when left untreated these disorders are associated with considerable psychological and functional impairments [2,3,4]. These disorders predict a range of current and future mental health problems [5,6,7,8,9,10] and can lead to long-term impairments across multiple domains [11,12,13,14,15]. Importantly, anxiety-related disruptions in school functioning can lead to poorer educational attainment, lower wages, welfare dependency, and lower quality of life [16, 17]. Accordingly, effective treatment that adequately attends to school-related impairments is critical for improving the long-term functioning of youth with anxiety and school impairment.
The past few decades have witnessed tremendous advances in the treatment of youth anxiety. Across numerous randomized trials, cognitive-behavioral therapy (CBT) and selective serotonin reuptake inhibitors (SSRIs) have each been found to be effective in reducing anxiety, and their combination has been found to be particularly effective [18, 19]. Moreover, these treatments have been shown to improve many impairments associated with anxiety, including family burdens, sleep problems, substance use, and overall life interference [4, 18, 20,21,22].
Few studies have examined the effects of youth anxiety treatment specifically on school-related impairment. This is particularly concerning given that youth anxiety disorders are associated with considerable school-related impairments including academic (e.g., difficulty attending and paying attention in class, taking tests, presenting in front of the class) and social (e.g., reading aloud, joining conversations, asking for help, engaging with others) impairments [12, 13, 15, 23]. Youth anxiety often manifests in school settings and is commonly identified by school-based personnel [12]. The content of youth anxiety commonly pertains to school settings [24, 25] and it is commonly these school-related impairments—rather than symptoms and diagnoses—that prompt adults to bring children into treatment.
Researchers have begun to address the effects of anxiety treatment on school impairment. Wood [26] examined the impact of CBT for youth anxiety on school performance in a small sample and found treatment-related anxiety decreases to be associated with school performance increases. In another study, Nail and colleagues [27] assessed youth anxiety treatment effects on academic impairment in a large sample and found positive treatment response was associated with improved academic functioning. Youth in this study received CBT, sertraline (SRT), or combination treatment (CBT + SRT), yet analyses were pooled across all treated youth. Previous studies have not examined school impairment effects within each treatment type, nor have analyses compared school impairment outcomes between these supported three treatments. To date, research has yet to evaluate whether CBT, SSRIs, or their combination, yield differential effects on anxiety-related school impairment. Moreover, research has not evaluated the rate at which school-related impairments improve across treatment. Traditional two-wave, pre-versus-post analytic designs are limited as they are unable to address differential shapes of change across treatments [28] Although recent years have increasingly focused on trajectories of change in youth anxiety treatment [20, 28, 29], much remains to be learned about dynamic processes that unfold across youth anxiety treatment with regard to school-related outcomes.
The present study leveraged data from the Child/Adolescent Anxiety Multimodal Study (CAMS =) [19] to examine differential changes in school impairment across CBT, SRT, and their combination, in the treatment of youth anxiety. The CAMS trial offers a rare opportunity to examine differential outcomes in anxiety-related school impairment across leading evidence-based youth anxiety treatments (and pill placebo) in the context of a single randomized trial. Latent growth modeling examined change trajectories in anxiety-related school impairment across treatments based on both parent and youth reports. Consistent with the primary and secondary outcomes of the CAMS trial focused on anxiety symptoms [18, 19] it was hypothesized school impairment would decrease over time across all three active treatments, and that combination treatment would have a significantly greater effect on school impairment than either of the monotherapies. Further we explored age moderation effects given the large CAMS age range (7–17 years), and gender effects given that males and females tend to experience differing impairment levels associated with anxiety, with males experiencing less anxiety symptoms and generally less functional impairment [30, 31]. However, data on gender differences related to school impairment have been mixed [32, 33]; therefore, no directional hypotheses regarding gender were made.
Methods
Participants
Participants were 488 youth (ages 7–17 years; M = 11.16, SD = 2.81; 49.6% female) participating in the CAMS trial who met DSM-IV-TR criteria for at least one of the following anxiety disorders: separation anxiety disorder, generalized anxiety disorder and/or social anxiety disorder. Participants were recruited from six study sites. Exclusion criteria were major depressive disorder, bipolar disorder, pervasive developmental disorder, and schizophrenia/schizoaffective disorder. Participant demographic data are presented in Table 1. Additional CAMS participant information can be found elsewhere [19, 34, 35].
Procedures
Study procedures were approved by institutional review boards at each of the six study sites and by the National Institute of Mental Health Data Safety and Monitoring Board. Informed consent and assent were obtained prior to baseline assessment. Baseline evaluations included parent- and youth-report questionnaires, and assessments not included in the present analysis. After baseline evaluation, participants were randomly assigned to one of four 12-week treatment conditions: (1) CBT, (2) medication (i.e., sertraline; SRT), (3) combination of CBT and SRT (i.e., COMB), or (4) placebo drug (i.e., PBO). Participants were assigned to CBT, SRT, COMB, and PBO conditions in a 2:2:2:1 ratio.
Data for the present analysis were drawn from parent- and youth-reports collected at baseline, and weeks 4, 8, and 12 (posttreatment). Follow-up data were not included given the contamination across conditions and differing individual treatment courses inherent in the CAMS design during the posttreatment follow-up interval. Procedural and dosage details regarding CBT, SRT, COMB, and PBO in the CAMS trial, as well as training and treatment fidelity data, can be found elsewhere [19, 34].
Measures
The Child Anxiety Impact Scale (CAIS) [33] is a parent- and youth-report measure that assesses anxiety-related psychosocial impairment. The two parallel forms ask how much anxiety has gotten in the way of completing various activities. Items scored on a 4-point Likert-style scale (0 = “not at all” to 3 = “very much”). For present purposes, we were only interested in the CAIS School impairment subscale, which includes 10 items (e.g. How much does anxiety interfere with “getting good grades?,” “concentrating on work?,” “doing homework?,” “taking tests or exams?”). CAIS School impairment scores range from 0 to 30. The CAIS has demonstrated strong internal reliability, construct validity, convergent validity, and divergent validity [33].
Analytic Strategy
Latent growth models (estimated in Mplus v.7.2) [36] examined change in anxiety-related school impairment (i.e., CAIS School scores) over the course of treatment via random slope, and differences in anxiety-related school impairment at posttreatment via random intercept. The time variable was centered at week 12 to assess posttreatment school impairment differences. CAIS school impairment scores at baseline, and weeks 4, 6, and 12 were included in the model, with weeks since randomization as the growth variable, and age, gender, study site, race, ethnicity, and income as covariates. Treatment groups were dummy coded to observe potential differences between conditions.
First, an intercept-only model was conducted with both equal and freely estimated residual variances to compare later models with their corresponding null model [37]. Models were compared using likelihood ratio tests; significant Chi square tests indicate that the more complicated model better fits the data. Model statistics—including root mean square error of approximation (RMSEA) and standardized root mean square residual (SRMR) in conjunction with a comparative fit index (CFI) using the null model—assessed model fit. RMSEA and SRMR < 0.08 indicates adequate fit and < 0.05 indicates good fit. CFI > 0.90 indicates adequate fit and > 0.95 indicates good fit. The final model was built by testing both linear and quadratic models against the intercept-only null model to determine the best model fit. Covariates were entered first, with the predictor of interest (treatment group) entered next. Next, moderation/product terms for age and gender were entered. Maximum likelihood estimation addressed missing data in latent growth curve models under the assumption that missing data were missing at random. Additionally, a missing values analysis was conducted and variables related to missingness were included in models. Parent-report and child-report models were computed separately.
Results
Table 2 presents raw means of the CAIS school impairment scale across time points, broken down by treatment condition and by informant.
Parent Report
A linear model with freely estimated residual variances provided good fit for the parent-report CAIS school impairment data (CFI = 0.96, RMSEA = 0.04, SRMR = 0.02) and was determined to best fit the data. Latent growth analyses demonstrated that across participants there was significant and negative linear change in parent-reported, anxiety-related school impairment over time (b = − 1.90, p < 0.001). When treatment group was added to the model, parent-report data indicated that at posttreatment, youth in the COMB group (b = − 5.47, p < 0.001), the SRT group (b = − 4.97, p < 0.001) and the CBT group (b = − 2.51, p < 0.05) all showed significantly less anxiety-related school impairment than youth in the PBO group. Although youth in all active treatments showed less posttreatment school impairment than youth in PBO, CBT-treated youth nonetheless showed significantly greater posttreatment school impairment than SRT-treated youth (b = 2.45, p < 0.05) and than COMB-treated youth (b = 2.95, p < 0.01).
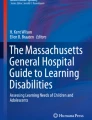
Additionally, treatment condition significantly predicted rate of change in anxiety-related school impairment over the course of treatment (see Fig. 1). Specifically, relative to youth receiving PBO, youth receiving COMB, (b = − 1.877, p < 0.01), SRT (b = − 1.36, p < 0.01), and CBT (b = − 1.20, p < 0.05) each showed significantly steeper decreases in parent-reported school impairment across the course of treatment. Anxiety-related school impairment decreased 3.08 points every 4 weeks among COMB-treated youth, decreased 2.67 points among SRT-treated youth, decreased 2.51 points among CBT-treated youth, and decreased 1.31 points among PBO-treated youth. There were no differences between the active treatment conditions regarding the rate of change in anxiety-related school impairment overtime.

Parent-report CAIS School Impairment scores, by condition, across 12 weeks of treatment for youth anxiety. Note: COMB Combination of sertraline (SRT) and cognitive-behavioral therapy (CBT), PBO medication management with placebo, week 0 baseline, week 12 post-treatment
Interaction terms for gender and age were added to the parent-report model, however, only gender displayed significant interaction effects. Therefore, the final model only included gender as a moderator. Gender significantly moderated the posttreatment difference between the treatment groups (see Fig. 2). The difference between PBO and SRT at posttreatment was moderated by gender (b = 3.851, p < 0.05), with males showing a larger SRT effect (relative to PBO) on anxiety-related school impairment than females. The difference between PBO and COMB groups at posttreatment was also moderated by gender (b = 3.284, p < 0.05), with males showing a larger COMB effect (relative to PBO) on anxiety-related school impairment than females. Gender also moderated differences in the rate of change between conditions, with gender patterns for SRT (b = 1.857, p < 0.05), COMB (b = 1.354, p < 0.05), and CBT (b = 1.274, p < 0.05) response each significantly different from the gender pattern for PBO response. Specifically, whereas females showed a steeper decrease than males in school impairment across PBO treatment, males showed a steeper decline than females in school impairment across SRT treatment (see Fig. 3). Males and females showed more comparable declines in school impairment across COMB and CBT treatment (see Fig. 3). There were no gender effects on the differences in rate of change across the active treatments.

Parent-report CAIS School Impairment scores at post-treatment, by gender

Parent-report CAIS School Impairment scores, by condition, by gender across 12 weeks of treatment for child anxiety
Youth Report
As with the parent-report data, a linear model with freely estimated residual variances provided good-to-fair fit for the youth-report data (CFI = 0.86, RMSEA = 0.04, SRMR = 0.03) and was determined to best fit youth-report CAIS School impairment data across time.
Latent growth analyses of youth-report CAIS school impairment scale found that across participants there was significant and negative change in anxiety-related school impairment over time (b = − 1.29, p < 0.001). By posttreatment, COMB-treated youth reported significantly lower anxiety-related school impairment relative to PBO-treated youth (b = − 1.52, p < 0.05). There were no significant posttreatment differences in youth-reported school impairment across the active treatments. Further, there were no significant differences in the rate of change in youth-reported school impairment over time between the four treatment groups, nor did age or gender moderate effects.
Discussion
Although previous work has documented that CBT, SSRI, and their combination, have beneficial effects on youth anxiety-related problems [18, 19] (the present study is the first to examine differential effects of these treatment strategies on anxiety-related school impairment. In this analysis, all three active treatments demonstrated superiority over PBO with regard to anxiety-related school impairment, and COMB showed the most robust effects. Specifically, both parent- and youth-reports found significantly lower posttreatment anxiety-related school impairment among COMB-treated youth compared to PBO-treated youth. According to parent-report, SRT and CBT also showed significantly lower school impairment at posttreatment than PBO, and all three active treatments showed steeper decreases in anxiety-related school impairment over the course of treatment than PBO youth. Of note, despite CBT superiority over PBO, CBT-treated youth still demonstrated more school impairment at posttreatment than youth treated with either of the medication strategies. Given the scope of school-related problems associated with youth anxiety [11], these findings provide support for the role of three active treatment strategies for reducing anxiety-related school impairment, with particularly robust support for combining SSRI and CBT.
According to parent-report, CBT was somewhat less effective than the active medication strategies for reducing anxiety-related school impairment. Importantly, however, CBT did show significant superiority over PBO, and youth reports suggested SRT alone, in the absence of concomitant CBT, was insufficient for reducing anxiety-related school impairment. Given the preferences of many families to avoid medication treatment in managing child anxiety [38, 39] and some unfavorable side effects associated with SSRIs [40, 41], the present findings support CBT as a valuable first treatment option for many anxious youth with school impairment when families or providers prefer to avoid pharmacologic options. In addition, the present findings suggest that when taking a pharmacologic approach, youth perceive the impact on school impairment to be insufficient unless CBT is additionally incorporated into a combined treatment regimen.
Consistent with previous studies, results were somewhat discrepant across parent- and youth-reports [12, 19, 42, 43]. Although parents and youth both agreed on the relative superiority of COMB over PBO on anxiety-related school impairment, only parents reported that SRT-alone and CBT-alone also outperformed PBO. Further, according to parents, all three active treatments were associated with more rapid decreases than PBO in anxiety-related school impairment, whereas children did not perceive such differences. In contrast with the parent-report data, youth-report data revealed minimal differences in the effect of treatment type on reducing anxiety-related school impairment. One possible explanation of such cross-informant discrepancies is that youth can be reluctant disclosers and commonly underreport anxiety and anxiety improvements [42]. The fewer findings based on youth report is consistent with previous youth anxiety trials [18, 44]. That said, given the needs for youth engagement, compliance, and adherence in the treatment of youth anxiety, providers will do well to continue to solicit input directly from treated youth regarding their anxiety-related impairments and the clinical targets of greatest relevance to them. The presently observed parent-youth discrepancies may also reflect the possibility that some parent perceptions of the differential effects of various treatment strategies are somewhat inflated.
Importantly, treatment in the CAMS trial was delivered in office-based settings. An increasing body of literature is supporting the role of school-based mental health treatment [45]. Providing services within schools has the potential to maximize treatment reach, improve ecological validity, and overcome disparities in care by providing services in children’s natural environments [46]. When anxious youth are showing anxiety-related school impairments, it may be advantageous for school-based providers to deliver the CBT aspects of treatment, as they may be more familiar with the specifics of a child’s school-related impairments and the school setting in which impairment is occurring. Indeed, researchers have found clinicians and school personnel can effectively deliver CBT for youth social anxiety [47, 48]. However, other studies have suggested that CBT yields no better outcomes than usual care delivered by school personnel in inner city schools [49], and there is some evidence school-based mental health care is more effective for externalizing than for internalizing problems [45]. Continued research is needed to examine the extent to which school-based treatment strategies can have an important role in the management of anxiety-related school impairment.
The present results suggest that school-related impairment among males may respond better to medication strategies than among females. Specifically, based on parent-reports males showed greater decrease in anxiety-related school impairment by posttreatment when they received SRT or COMB than females. Additionally, PBO-treated females showed a significantly steeper reduction in school impairment than males, whereas SRT-treated males showed a significantly steeper reduction in anxiety-related school impairment than females. While there are known gender-related differences in the prevalence and experience of anxiety, there has been little support to suggest that treatment responses associated with anxiety or anxiety-related school impairment varies by gender [12, 19, 26]. Perhaps, academic impairment types may be differentially represented among males and females. For example, males may have more attention-related impairment (e.g., concentrating on schoolwork), whereas females may have more social impairment (e.g., difficulty engaging with peers, presenting in front of class). That said, there is some evidence suggesting males may respond better to SSRIs than females [50], however many studies do not find SSRI gender effects. Continued studies are needed to assess gender differences across treatment strategies in the management of anxiety-related school-impairment.
Several study limitations warrant comment. First, we relied only on parent and youth perceptions of school impairment, and did not have access to objective measures (e.g., grades, attendance) or teacher reports. Incorporating such objective and/or teacher-report data would have provided more comprehensive information, although such data likely could not speak to whether such school impairment was anxiety-related. Second, given the contamination across conditions and differing individual treatment courses in the CAMS design during the posttreatment follow-up interval (e.g., after week 12 PBO-treated youth given choice of active treatments, non-responders referred for additional services, responders given maintenance sessions), the present analysis only evaluated acute outcomes. Long-term outcomes are critical to informing which treatment strategies are associated with maintained gains in anxiety-related school impairment. It remains unclear whether medication effects endure after medication discontinuation, or whether CBT-treated youth maintain gains due to skill acquisition. CAMS follow-up analyses have suggested that many acute treatment gains may dissipate with time [51,52,53]. Booster treatment may be required for some youth to maintain improvements in anxiety-related school impairment. Third, CAMS included mostly Caucasian and middle-to-high SES youth, limiting the generalizability of results to minority or economically disadvantaged families. Moreover, the sample only included youth meeting inclusion/exclusion criteria and had GAD, SOP and/or SAD, further limiting the generalizability of results. Lastly, the CAMS design cannot rule out the possibility that superior COMB effects are simply due to additive effects associated with additional time spent with providers.
Despite limitations this study holds important clinical implications for anxious youth suffering from anxiety-related school impairment. While the effects of treatment on youth anxiety symptoms have been well-studied, this is the first study to assess the differential effects of evidence-based treatment strategies on anxiety-related school impairment. The combination of sertraline and CBT yielded the most robust effects for reducing anxiety-related school impairments. There was also some support for the utility of sertraline or CBT as monotherapies in the management of anxiety-related school-impairment. Given the extent to which youth anxiety is associated with school impairment [11, 12] continued research is needed to identify which treatment options are most likely to benefit which youth with what forms of anxiety-related school impairments. Further, mediation analyses will be critical to elucidate the mechanisms through which various treatment strategies effect anxiety-related school impairment.
Summary
Youth anxiety disorders are highly prevalent and associated with considerable school impairment. Results from the present study indicated that three evidence-based treatments for anxiety—i.e., Cognitive Behavior Therapy (CBT), sertraline (SRT), and their combination (COMB)—demonstrated superiority over placebo (PBO) in reducing anxiety-related school impairment, with COMB showing the most robust effects. According to parent reports, anxious youth receiving SRT and CBT also showed significantly lower school impairment at posttreatment than PBO, and all three active treatments showed steeper decreases in anxiety-related school impairment over the course of treatment than PBO youth. According to youth report, only COMB treatment predicted significantly lower school impairment at posttreatment. In contrast to parent reports, youth reports revealed no significant posttreatment differences in school impairment across the active treatments and no significant differences in the rate of change in youth-reported school impairment over time among the four treatment groups. According to parent-report, medication strategies (i.e., SRT, COMB) may have stronger effects on anxiety-related school impairment among males than among females, however no gender effects were found by youth-report. These results underscore the need to further examine treatment effects on anxiety-related school impairments that can have long-lasting impacts on youth development. Continued research is needed to understand for whom certain anxiety treatments are most helpful in reducing associated functional impairments such as anxiety-related school impairment.
References
Merikangas KR, He JP, Burstein M, Swanson SA, Avenevoli S, Cui L et al (2010) Lifetime prevalence of mental disorders in US adolescents: results from the National Comorbidity Survey Replication-Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry 49:980–989. https://doi.org/10.1016/j.jaac.2010.05.017
Comer JS, Blanc C, Grant B, Hasin D, Liu SM, Turner JB, Olfson M (2011) Health-related quality of life across the anxiety disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry 72:43–50. https://doi.org/10.4088/jcp.09m05094blu
Comer JS, Olfson M (2010) The epidemiology of anxiety disorders. In: Simpson HB, Schneier F, Neria Y, Lewis-Fernandez R (eds) Anxiety disorders. Theory, research, and clinical perspectives. Cambridge University Press, New York, pp 6–19. https://doi.org/10.1017/cbo9780511777578.004
Lyneham HJ, Sburlati ES, Abbott MJ, Rapee RM, Hudson JL, Tolin DF et al (2013) Psychometric properties of the Child Anxiety Life Interference Scale (CALIS). J Anxiety Disord 27:711–719. https://doi.org/10.1016/j.janxdis.2013.09.008
Bittner A, Egger HL, Erkanli A, Costello EJ, Foley DL, Angold A (2007) What do childhood anxiety disorders predict? J Child Psychol Psychiatry 48:1174–1183. https://doi.org/10.1111/j.1469-7610.2007.01812.x
Cornacchio D, Crum KI, Coxe S, Pincus DB, Comer JS (2016) Irritability and severity of anxious symptomatology among youth with anxiety disorders. J Am Acad Child Adolesc Psychiatry 55:54–61. https://doi.org/10.1016/j.jaac.2015.10.007
Cummings CM, Caporino NE, Kendall PC (2014) Comorbidity of anxiety and depression in children and adolescents: 20 years after. Psychol Bull 140:816–845. https://doi.org/10.1037/a0034733
Duperrouzel J, Hawes S, Lopez-Quintero C, Pacheco-Colon I, Comer JS, Gonzalez R (2017) The relationships between adolescent cannabis use and anxiety: a parallel process analysis. Addict Behav 78:107–113. https://doi.org/10.1016/j.addbeh.2017.11.005
Poznanski B, Cornacchio D, Coxe S, Pincus DB, McMakin DL, Comer JS (2018) The link between anxiety severity and irritability among anxious youth: evaluating the mediating role of sleep problems. Child Psychiatry Hum Dev 49:352–359. https://doi.org/10.1007/s10578-017-0769-1
Wu P, Goodwin R, Comer JS, Hoven C, Cohen P (2010) The relationship between anxiety disorders and substance use among adolescents in the community: specificity and gender differences. J Youth Adolesc 39:177–188. https://doi.org/10.1007/s10964-008-9385-5
Copeland WE, Angold A, Shanahan L, Costello EJ (2014) Longitudinal patterns of anxiety from childhood to adulthood: the great smoky mountains study. J Am Acad Child Adolesc Psychiatry 53:21–33. https://doi.org/10.1016/j.jaac.2013.09.017
Green JG, Comer JS, Donaldson AR, Elkins RM, Nadeau MS, Reid G, Pincus D (2017) School functioning and use of school-based accommodations by treatment-seeking anxious children. J Emot Behav Disord 25:220–232. https://doi.org/10.1177/1063426616664328
Mychailyszyn MP, Mendez JL, Kendall PC (2010) School functioning in youth with and without anxiety disorders: comparisons by diagnosis and comorbidity. Sch Psychol Rev 39:106–121
Swan AJ, Kendall PC (2016) Fear and missing out: youth anxiety and functional outcomes. Clin Psychol Sci Pract 23:417–435. https://doi.org/10.1111/cpsp.12169
Woodward LJ, Fergusson DM (2001) Life course outcomes of young people with anxiety disorders in adolescence. J Am Acad Child Adolesc Psychiatry 40:1086–1093. https://doi.org/10.1097/00004583-200109000-00018
Kessler RC, Foster CL, Saunders WB, Stang PE (1995) Social consequences of psychiatric disorders, I: educational attainment. Am J Psychiatry 152:1026–1032. https://doi.org/10.1176/ajp.152.7.1026
Kessler RC, Greenberg PE (2002) The economic burden of anxiety and stress disorders. Neuropsychopharmacology 67:981–992
Albano AM, Comer JS, Compton SN, Piacentini J, Kendall PC, Birmaher B et al (2018) Secondary outcomes from the child/adolescent anxiety multimodal study: Implications for clinical practice. Evid Based Pract Child Adolesc Ment Health 3:30–41. https://doi.org/10.1037/e583972013-001
Walkup JT, Albano AM, Piacentini J, Birmaher B, Compton SN, Sherrill JT et al (2008) Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety. N Engl J Med 359:2753–2766. https://doi.org/10.1056/NEJMoa0804633.Cognitive
Kendall PC, Safford S, Flannery-Schroeder E, Web A (2004) Child anxiety treatment: outcomes in adolescence and impact on substance use and depression at 7.4-year follow-up. J Consult Clin Psychol 72:276–287. https://doi.org/10.1037/0022-006x.72.2.276
Peris TS, Compton SN, Kendall PC, Birmaher B, Sherrill J, March J et al (2015) Trajectories of change in youth anxiety during cognitive-behavior therapy. J Consult Clin Psychol 83:239–252. https://doi.org/10.1037/a0038402
Peterman JS, Carper MM, Elkins RM, Comer JS, Pincus DB, Kendall PC (2016) The effects of cognitive behavioral therapy for youth anxiety on sleep problems. J Anxiety Disord 37:78–88. https://doi.org/10.1016/j.janxdis.2015.11.006
Beidel DC, Turner SM, Morris TL (1999) Psychopathology of childhood social phobia. J Am Acad Child Adolesc Psychiatry 38:643–650. https://doi.org/10.1097/00004583-199906000-00010
Silverman WK, La Greca AM, Wasserstein S (1995) What do children worry about? Worries and their relation to anxiety. Child Dev 66:671–686. https://doi.org/10.1111/j.1467-8624.1995.tb00897.x
Weems CF, Silverman WK, La Greca AM (2000) What do youth referred for anxiety problems worry about? Worry and its relation to anxiety and anxiety disorders in children and adolescents. J Abnorm Child Psychol 28:63–72. https://doi.org/10.1023/a:1005122101885
Wood J (2006) Effect of anxiety reduction on children’s school performance and social adjustment. Dev Psychol 42:345–349. https://doi.org/10.1037/0012-1649.42.2.345
Nail JE, Cristofferson J, Ginsburg GS, Drake K, Kendall PC, McCracken JT et al (2015) Academic impairment and impact of treatments among youth with anxiety disorders. Child Youth Care Forum 44:327–342. https://doi.org/10.1007/s10566-014-9290-x
Gallo KP, Cooper-Vince CE, Hardway C, Pincus DB, Comer JS (2014) Trajectories of change across outcomes in intensive treatment for adolescent panic disorder and agoraphobia. J Clin Child Adolesc Psychol 43:742–750. https://doi.org/10.1080/15374416.2013.794701
Chu BC, Skriner LC, Zandberg LJ (2013) Shape of change in cognitive behavioral therapy for youth anxiety: symptom trajectory and predictors of change. J Consult Clin Psychol 81:573–587. https://doi.org/10.1037/a0033390
Craske MG (1999) Anxiety disorders: psychological approaches to theory and treatment. Westview Press, Boulder
McLean CP, Asnaani A, Litz BT, Hofmann SG (2011) Gender differences in anxiety disorders: prevalence, course of illness, comorbidity and burden of illness. J Psychiatr Res 45:1027–1035. https://doi.org/10.1016/j.jpsychires.2011.03.006
Derdikman-Eiron R, Indredavik MS, Bakken IJ, Bratberg GH, Hjemdal O, Colton M (2012) Gender differences in psychosocial functioning of adolescents with symptoms of anxiety and depression: longitudinal finding from the Nord-Trondelag Health Study. Soc Psychiatry Psychiatr Epidemiol 47:1855–1863. https://doi.org/10.1007/s00127-012-0492-y
Langley AK, Bergman R, McCracken J, Piacentini JC (2004) Impairment in childhood anxiety disorders: preliminary examination of the Child Anxiety Impact Scale-Parent Version. J Child Adolesc Psychopharmacol 14:105–114. https://doi.org/10.1089/104454604773840544
Compton SN, Walkup JT, Albano AM, Piacentini JC, Birmaher B, Sherrill JT et al (2010) Child/Adolescent Anxiety Multimodal Study (CAMS): rationale, design, and methods. Child Adolesc Psychiatry Ment Health 4:1–15. https://doi.org/10.1186/1753-2000-4-1
Kendall PC, Compton SN, Walkup JT, Birmaher B, Albano AM, Sherrill J et al (2010) Clinical characteristics of anxiety disordered youth. J Anxiety Disord 24:360–365. https://doi.org/10.1016/j.janxdis.2010.01.009
Muthén LK, Muthén BO (1998–2015) Mplus User’s Guide. Seventh Edn. Muthén & Muthén, Los Angeles
Widaman KF, Ferrer E, Conger RD (2010) Factorial invariance within longitudinal structural equation models: measuring the same construct across time. Child Dev Perspect 4:10–18. https://doi.org/10.1111/j.1750-8606.2009.00110.x
Brown AM, Deacon BJ, Abramowitz JS, Dammann J, Whiteside SP (2007) Parents’ perceptions of pharmacological and cognitive-behavioral treatments for childhood anxiety disorders. Behav Res Ther 45:819–828. https://doi.org/10.1016/j.brat.2006.04.010
Prins MA, Verhaak PF, Bensing JM, van der Meer K (2008) Health beliefs and perceived need for mental health care of anxiety and depression—the patients’ perspective explored. Clin Psychol Rev 28:1038–1058. https://doi.org/10.1016/j.cpr.2008.02.009
Jick H, Kaye JA, Jick SS (2004) Antidepressants and the risk of suicidal behaviors. JAMA 292:338–343. https://doi.org/10.1001/jama.292.3.338
Rynn M, Walkup JT, Compton SN, Sakolsky DJ, Sherrill JT, Shen S et al (2015) Child/Adolescent anxiety multimodal study: evaluating safety. J Am Acad Child Adolesc Psychiatry 54:180–190. https://doi.org/10.1016/j.jaac.2014.12.015
Comer JS, Kendall PC (2004) A symptom-level examination of parent-child agreement in the diagnosis of anxious youths. J Am Acad Child Adolesc Psychiatry 43:878–886. https://doi.org/10.1097/01.chi.0000125092.35109.c5
De Los Reyes A, Kazdin AE (2005) Informant discrepancies in the assessment of childhood psychopathology: a critical review, theoretical framework, and recommendations for further study. Psychol Bull 131:483. https://doi.org/10.1037/0033-2909.131.4.483
Kendall PC, Hudson JL, Gosch E, Flannery-Schroeder E, Suveg C (2008) Cognitive-behavioral therapy for anxiety disordered youth: a randomized clinical trial evaluating child and family modalities. J Consult Clin Psychol 76:282–297. https://doi.org/10.1037/0022-006x.76.2.282
Sanchez AL, Cornacchio D, Poznanski B, Golik AM, Chou T, Comer JS (2018) The effectiveness of school-based mental health services for elementary-aged children: a meta-analysis. J Am Acad Child Adolesc Psychiatry 57:153–165. https://doi.org/10.1016/j.jaac.2017.11.022
Atkins MS, Cappella E, Shernoff ES, Mehta TG, Gustafson EL (2017) Schooling and children’s mental health: realigning resources to reduce disparities and advance public health. Annu Rev Clin Psychol 13:123–147. https://doi.org/10.1146/annurev-clinpsy-032816-045234
Ginsburg GS, Drake KL (2002) School-based treatment for anxious African-American adolescents: a controlled pilot study. J Am Acad Child Adolesc Psychiatry 41:768–775. https://doi.org/10.1097/00004583-200207000-00007
Ginsburg GS, Becker KD, Drazdowski TK, Tein JY (2012) Treating anxiety disorders in inner city schools: results from a pilot randomized controlled trial comparing CBT and usual care. Child Youth Care Forum 41:1–19. https://doi.org/10.1007/s10566-011-9156-4
Masia Warner C, Colognori D, Brice C, Herzig K, Mufson L, Lynch C et al (2016) Can school counselors deliver cognitive-behavioral treatment for social anxiety effectively? A randomized controlled trial. J Child Psychol Psychiatry 57:1229–1238. https://doi.org/10.1111/jcpp.12550
Simon NM, Zalta AK, Worthington Iii JJ, Hoge EA, Christian KM, Stevens JC et al (2006) Preliminary support for gender differences in response to fluoxetine for generalized anxiety disorder. Depress Anxiety 23:373–376. https://doi.org/10.1002/da.20184
Ginsburg GS, Kendall PC, Sakolsky D, Compton SN, Piacentini J, Albano AM et al (2011) Remission after acute treatment in children and adolescents with anxiety disorders: findings from the CAMS. J Consult Clin Psychol 79:806. https://doi.org/10.1037/a0025933
Ginsburg GS, Becker-Haimes EM, Keeton C, Kendall PC, Iyengar S, Sakolsky D et al (2018) Results from the Child/Adolescent Anxiety Extended Long-Term Study (CAMELS): primary anxiety outcomes. J Am Acad Child Adolesc Psychiatry 57:471. https://doi.org/10.1016/j.jaac.2018.03.017
Piacentini J, Bennett S, Compton S, Kendall PC, Birmaher B, Albano AM et al (2014) 24- and 36-week outcomes for the Child/Adolescent Anxiety Multimodal Study (CAMS). J Am Acad Child Adolesc Psychiatry 53:297–310. https://doi.org/10.1016/j.jaac.2013.11.010
Funding
This research was supported by NIMH Grants U01 MH64088, U01 MH064003, U01 MH63747, U01 MH64003, U01 MH64092, U01 MH64107, U01 MH064089, and K23 MH090247. Sertraline and matching placebo were supplied free of charge by Pfizer.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Ms. Sanchez reports nothing to disclose. Dr. Comer reports Grant Support from NIMH, NICHD, NSF, PCORI, the Charles H. Hood Foundation, the Andrew Kukes Foundation for Social Anxiety, and the International Obsessive–Compulsive Disorder Foundation, as well as personal fees from Oxford University Press and Worth Publishing/Macmillan Learning. Dr. Albano reports royalties from Oxford University Press and has received honorarium from American Psychological Association. Dr. Piacentini reports grant support from NIMH, Tourette Association of America, TLC Foundation for BFRBs, Pettit Family Foundation, and Pfizer Pharmaceuticals. He reports royalties from Guilford Press and Oxford University Press and has received honorarium and travel support from the Tourette Association of America, and the International OCD Foundation. Dr. Compton reports research support from NIMH and has served as a consultant to Shire Pharmaceuticals. He has received honoraria from the Nordic Long-Term Obsessive–Compulsive Disorder (OCD)-Treatment Study Research Group and Journal of Consulting and Clinical Psychology (JCCP). He has provided expert testimony at Duke Forensic Group. Dr. Walkup reports grant support from the Hartwell Foundation and the Tourette Syndrome Association. He has served on the advisory board and speaker’s bureau of the Tourette Syndrome Association. He reports royalties from Guilford Press and Oxford University Press and has received honorarium and travel support from the Tourette Syndrome Association. He is an unpaid member of the Scientific Advisory Board of the Trichotillomania Learning Center, the Scientific Council of the Anxiety and Depression Association of America, and a Scientific Advisor to the American Foundation of Suicide Prevention. Dr. Ginsburg reports research support from NIMH and DOE. Dr. Rynn research support from NIMH, personal fees from Oxford University Press, and royalties from UpToDate. Dr. Birmaher reports grant support from NIMH and personal fees from Random House, Inc., Lippincott Williams and Wilkins, and UpToDate. Dr. Kendall reports grant support from NIMH and NICHD, as well as personal fees from Oxford University Press, Guilford Press, Ericsson, and Workbook Publishing. Dr. Kendall receives royalties from the sales of materials related to the treatment of anxiety in youth, such as the materials used in the CAMS report.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sanchez, A.L., Comer, J.S., Coxe, S. et al. The Effects of Youth Anxiety Treatment on School Impairment: Differential Outcomes Across CBT, Sertraline, and their Combination. Child Psychiatry Hum Dev 50, 940–949 (2019). https://doi.org/10.1007/s10578-019-00896-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10578-019-00896-3