
Abstract
Approximately 3 million child and adolescent cases are investigated for maltreatment each year, and 75% of those cases are categorized as neglect. Parentification, a form of neglect, has emerged as an important clinical topic and focus of empirical research. Similar to the research base on neglect, the accumulated literature point toward a significant positive relation between parentification and pernicious outcomes, although nascent literature also has found a link between parentification and resiliency and select competencies. The purpose of the current study was two-fold: (a) To explore the extent to which parentification mediates the relation between parenting behaviors and depressive symptoms and well-being (as measured by negative and positive affect) in a sample of early adolescents (i.e., ages 11–14)? And, (b) to what extent does gender moderate the proposed mediation model? We found in our sample (N = 314) parentification mediated the association between parenting behaviors and depressive symptoms (negative affect) and partially mediated the relation between parenting behaviors and well-being (positive affect). In addition, gender partially moderated select mediation models. These findings may be useful in the conceptualization of cross-sectional and longitudinal studies focused on family systems and parenting interventions in families where parentification has occurred.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
According to the most recent report by the U.S. Department of Health and Human Services (HHS 2014) National Center on Child Abuse and Neglect, National Child Abuse and Neglect Data System, approximately 3 million child and adolescent cases are investigated for maltreatment each year, and 75% of those cases are categorized as neglect. The American Humane Association (2013) described child neglect as occurring when a parent or caregiver fails to provide basic physical, emotional, educational, or medical care. The negative sequelae evidenced from neglect are far reaching. For example, children, adolescents, and emerging adults who have experienced neglect are 3 times more likely to be diagnosed with depression and to report suicide behaviors than those who have not experienced neglect (Sfoggia et al. 2008).
With both maltreatment and neglect steadily increasing over the last decade (HHS 2014), parentification, a form of neglect (Garber 2011), has emerged as an important clinical topic and area of empirical research (Schimmenti and Bifulco 2015; Tomeny et al. 2016). Garber (2011) discussed—in the law practice literature—how parentification can be a form of neglect, cautioning family court litigators to be aware of this often overlooked aspect of neglect. Parentification refers to the reversal of roles between the parent and child whereby a child is held accountable for a parent’s or other family member’s ability to function at the expense of the adolescent’s own needs (Hooper 2007a; Hooper et al. 2013). Like other forms of neglect, parentification—a family systems process—is correlated with diverse negative outcomes and, less frequently investigated, positive outcomes. For example, some family systems scholars have considered the extent to which and when the parentification process is perceived to be fair or beneficial in understanding bimodal outcomes (Chase 1999; East 2010; Jurkovic 1997; Hooper et al. 2011; Tompkins 2007). Given the role reversal present with parentification, boundaries between and around the family system and subsystems (parent and sibling) are often poor or blurred, which allow parentification to emerge and be maintained (Kerig 2014).
The parentification process can be observed in roles, responsibilities, and relationships whereby parents or caregivers abdicate their parental role for diverse reasons. The commonly reported antecedents include parents’ or caregivers’ experiences related to substance use, chronic physical health conditions, depressive disorders, divorce, and personality and characterological disturbances (Hooper et al. 2011). Jurkovic (1997) outlined two types of parentification (i.e., emotional parentification and instrumental parentification), which are the most common roles and responsibilities discussed and evaluated in the literature. Emotional parentification occurs when family members depend on the parentified child for emotional support and assistance, or when the parentified child must regulate affectivity for parents or other family members (Jurkovic 1997; Mika et al. 1987). Instrumental parentification is often related to behavioral tasks like cleaning, caring for siblings, providing medical care, managing medications, cooking (Jurkovic 1997), and, more recently examined, language brokering (Arellano et al. 2018; Kam 2011). These family systems processes (i.e., emotional and instrumental parentification) are most often directed toward parents and siblings, although they can involve other family members as well. Given their ubiquity, researchers have focused on the current or aftereffects of emotional and instrumental parentification based on to whom the parentified behavior is directed (e.g., parent vs. sibling, Hooper et al. 2012; Peris et al. 2008; Tomeny et al. 2016). Hooper et al. (2011) asserted that engaging in instrumental and emotional parentification with a sibling may portend less deleterious outcomes as compared to engaging in instrumental and emotional parentification with a parent.
The parallels between the construct and process of parentification and those of neglect are clear (Garber 2011). For example, what is often observed in both cases includes but is not limited to: (a) inappropriate attachment formation, (b) the parent’s lack of competence in providing a developmentally appropriate environment, (c) the parent’s abdication of adult roles and responsibilities to the child, and (d) deprivation of affection, emotional support, and psychological and physical care (Hooper 2007a). The aftereffects of child maltreatment, neglect, and parentification are often—but not always—long lasting and seen from cradle to grave.
Bronfenbrenner (1986) proposed in his bioecological theory that various adult relationships, behaviors, systems (familial, school, environmental, and ecological), and social factors influence one’s development, especially during early adolescence, when individuals experience substantive developmental changes (Cole et al. 2008). With the onset of puberty, early adolescence is an especially vulnerable group. For example, Crone and Dahl (2012) provided a comprehensive overview of how the period of early adolescent development influences overall functioning, including biological changes associated with hormones and puberty, cognitive changes such as onset of abstract thinking and problem-solving abilities, and social-affective changes like emotional regulation and interpersonal skills. The contexts or systems in which these individual changes take place is important (i.e., individuals in their environment). Examining antecedents, predictors, and outcomes associated with parentification in early adolescence is paramount given the vulnerability to the development of depressive symptoms often seen in this age group (Holder and Blaustein 2014). Weinberger et al. (2018) discussed the significant upsurge in rates of depression among adolescents. Specifically, they found depression increased from 8.7% in 2005 to 12.7% in 2015 among adolescents. During early adolescence, rates of major depressive episodes nearly triple from 4 to 11% (National Institute of Mental Health 2012) and suicide is the second leading cause of death among early adolescents (Centers for Disease Control and Prevention 2015). In addition, empirical research has underscored the significant negative association between age, maltreatment (or neglect, of which parentification can be a part), and depression later in adulthood (Kaplow and Widom 2007). These findings support exploring the combined effects of parentification on bimodal outcomes (negative and positive affect; Dejonckheere et al. 2018).
Studies that take a balanced approach to clarify bimodal outcomes are important (see Hooper et al. 2012), although clarifying the link between parentification and depression and depressive symptoms may be particularly beneficial among early adolescents. Consonant with examinations focused on depressive symptomatology and well-being, Clark and Watson (1991) described how differential outcomes (positive and negative affect) might be evidenced. Their tripartite model posited that depression is a combination of high negative affect and low positive affect; this model has been empirically supported with early adolescent populations (Lambert et al. 2004). The National Institute of Mental Health’s (n.d.) Research Domain Criteria applied Clark and Watson’s tripartite model to conceptualize depression. Therefore, by measuring affect, researchers can draw conclusions about correlates and predictors of depressive symptoms and consider how some constructs mediate and moderate positive and negative affect. Clark and Watson’s (1991) model has relevance to the study of parentification and bimodal outcomes (as measured by positive and negative affect).
With regard to the link between parentification and depression, one theme that has been identified throughout family systems, child development, and health literature as a critical contributor to early adolescent outcomes is parenting behaviors (Johnson and Greenberg 2013). Parenting behaviors have long been linked with outcomes as diverse as academic achievement, intrapersonal and interpersonal factors, and depression (Peris et al. 2008). Bronfenbrenner’s (1986) bioecological theory has been used to undergird research involving family systems constructs and processes, as well as to buttress the study of parenting behaviors (Bronfenbrenner 1986; Bronfenbrenner and Morris 2006). Parenting behavior—which is an active ingredient in parentification—can serve as a predictor of depression and well-being for family members, including early adolescents.
The extent to which there is a significant and positive relation between parenting behavior and parentification is intuitive. This association has long been studied in the empirical literature base and also discussed in the theoretical and clinical literature (Peris et al. 2008; Tompkins 2007). Specifically, three themes regarding parenting behaviors relevant to parentification appear in the literature: (a) parents’ use of punishment (Peris et al. 2008), (b) positive parenting and parental involvement (Peris et al. 2008; Tompkins 2007), and (c) parental monitoring and supervision (Tompkins 2007). In a study composed of a small, racially diverse sample of 43 female adolescents between the ages of 9 and 16 (42% African American, 44% Latina, 14% European American) whose mothers were diagnosed with HIV, Tompkins (2007) investigated whether parentification is related to select parenting behaviors. In addition, the Tompkins study explored whether outcomes were more beneficial or burdensome for the adolescent-participants. Tompkins (2007) found that parentified youth reported more parental involvement and positive parenting (as reported by the parent) due to the pair’s increased emotional closeness as a result of the parent’s medical illness (Tompkins 2007). She asserted that this pattern was especially prevalent for those who were parentified due to the parent’s HIV condition, compared with those who were parentified for other reasons (e.g., alcoholism). Similarly, Peris et al. (2008) followed 300 adolescents for a year and found that higher rates of parentification were associated with parenting behavior indicative of low warmth (i.e., low levels of positive parenting) and perceived threat (i.e., corporal punishment). With the exception of these studies (Peris et al. 2008; Tompkins 2007), no studies have investigated the relation between parenting behavior and parentification among early adolescent participants, although a clear link exists between parenting behavior and various elements of early adolescents’ psychosocial outcomes, such as internalizing and externalizing behavior (Peris et al. 2008), depression (Wimsatt et al. 2013), and positive and negative affect (Davidov and Grusec 2006; Johnson and Greenberg 2013). In early adolescence, research has demonstrated that corporal punishment is positively related to depression (Wimsatt et al. 2013) and to negative affect (Burton and Pössel 2017). Further, inconsistent discipline is positively related to negative affect (Burton and Pössel 2017); parental involvement is positively related to positive affect (Burton and Pössel 2017); and poor monitoring and supervision is negatively related to positive affect (Johnson and Greenberg 2013).
A growing body of literature has investigated how cultural variables explain the relation between parentification and depressive symptoms (Hooper et al. 2011). In particular, gender has been identified as being related to parentification, parenting behaviors, and depression (Burnett et al. 2006; Byng-Hall 2008; Diaz et al. 2007; Hooper et al. 2011). The existing research regarding gender differences, perceptions of parenting behavior, and depressive symptoms has been mixed. Carlson (2006) reported no significant gender differences for parental involvement across select domains of negative affect and internalizing behaviors, and Mazefsky and Farrell (2005) found that males reported higher rates of poor parental monitoring and parental supervision and inconsistent discipline than did females. Some researchers have contended that females and males respond differently to parental corporal punishment, with males demonstrating increased externalizing symptoms and behaviors, whereas females demonstrate increased internalizing symptoms and behaviors (Jang 2007). These findings underscore that most studies focus on gender differences among externalizing behaviors (Carlson 2006; Gryczkowski et al. 2010), with a minimal focus on internalizing behaviors.
Gender has relevance for parentification, but the accumulated literature on this relation is mixed as well. Females often (but not always; e.g., Hooper et al. 2015) report higher frequencies of parentification and caregiving than males do (Burnett et al. 2006; Byng-Hall 2008). Thus, theoretically, females should be considered at a greater risk for negative outcomes associated with parentification than males (Jurkovic 1997), although one study found the inverse, in that male participants reported more experiences of parentification and worse outcomes than their female counterparts (Diaz et al. 2007). East (2010) asserted that these inconsistent findings may be attributed to the role of socialization. According to Bronfenbrenner’s (1986) bioecological theory, an individual’s social environment can dictate the development of that individual’s expression of gender identity. Patterns evidenced in Westernized ecologies show females have higher rates of morbidity, while males have higher rates of mortality (Case and Paxson 2005). It could be that females are encouraged to serve as caretakers, a core role of parentification, through seeking help and disclosing health concerns for both self and others, resulting in increased morbidity rates. On the other hand, males—in some cultures—are discouraged from demonstrating caretaking behaviors, such as seeking help or reporting health concerns, given that caretaking behavior may be perceived as shameful and a sign of femininity (Case and Paxson 2005). The secrecy around the experience of parentification—similar to child neglect—may result in fewer disclosures to others and thus higher mortality rates for men (Case and Paxson 2005). Socialization of gender roles and perceptions about "appropriate" gendered ways of being might explain why females take on more caretaking responsibilities and how they are encouraged to process and disclose psychopathology, whereas males are often socialized to underreport caretaking roles and responsibilities that characterize parentification (East 2010).
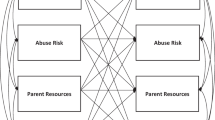
Given the extant literature base and the dearth of research focused on early adolescence (i.e., ages of 11 through 14), the current study explores the relation between parenting behavior and well-being and depressive symptomatology, as measured by positive affect and negative affect, as well as the extent to which parentification (i.e., as measured by parent-focused parentification, sibling-focused parentification, and perceived benefits of parentification) mediates this relation. Because the literature on gender differences is mixed, we tested a moderated mediation analysis (see Fig. 1), with gender hypothesized to moderate the mediation effect of parentification on the association between parenting behavior and adolescents’ negative and positive affect. Taken together, two research questions informed the current study: (a) To what extent does parentification mediate the relation between parenting behaviors and well-being and depressive symptoms in early adolescents? And (b) to what extent does gender moderate the mediation model?

Moderated mediation hypothesized model. X predictor variable, Y outcome variable, M mediator variable, W moderator variable
Method
Participants
Early adolescents from five middle schools located in three school districts in the southern United States were recruited. Three of the middle schools were public schools and two were Catholic or parochial private schools. Four schools were located in an urban area and one public school was located in a rural region. Between grades 6 through 8707 students were invited to participate, with 335 early adolescent-participants receiving parental consent to continue with the study, for a participation rate of 47.38%. No incentives were provided, nor did the study include any exclusion criteria for participation. Of the 335 adolescents participating in the first wave of data collection, 21 (6%) were excluded from the current study because they did not have complete data on all target variables. For the final study sample, participants were 314 early adolescents, with 50.6% (n = 159) females and 49.4% (n = 155) males. The participants were aged 11 years (15.3%, n = 48), 12 years (31.2%, n = 98), 13 years (32.5%, n = 102), 14 years (20.1%, n = 63) or 15 years (1.0%, n = 3). The participant self-report current grade levels as follows: 6th grade (36.0%, n = 113), 7th grade (24.2%, n = 76), or 8th grade (39.8%, n = 125). The racial and ethnic composition of the sample was 2.2% (n = 7) Asian or Pacific Islander, 9.9% (n = 31) Black American, 1.9% (n = 6) Hispanic, 1.0% (n = 3) Native American or Alaska Native, 77.7% (n = 244) White American, and 7.3% (n = 23) Two or more races.
Procedure
Once we gained approval from both the university’s and the school districts’ institutional review boards, we contacted middle school principals in the corresponding districts by email and invited them to participate in the study. We distributed parental consent forms to students in five schools two to three weeks preceding data collection. Those students who returned their parental consent forms participated in two waves of data collection. The current study was delimited to wave 1 data. The data collection took place during the regular school day and took approximately 45 min. Each school determined during which school periods the data collection took place. The adolescents participated in groups, and although teachers were present, they did not participate in data collection procedures. Instead research staff members distributed the paper-and-pencil assents and surveys and answered all questions.
Measures
Alabama Parenting Questionnaire (APQ)
We measured parenting behaviors by the Alabama Parenting Questionnaire (APQ; Frick 1991), which served as a predictor variable in the current study. The APQ comprises 42 items grouped into five subscales: corporal punishment (3 items, e.g., “Your parents hit you with a belt, switch, or other object as a punishment”), inconsistent discipline (6 items, e.g., “Your parent threatens to punish you and then does not do it”), parental involvement (10 items, e.g., “You have a friendly talk with your parent”), poor monitoring/supervision (10 items, e.g., “You fail to leave a note or let your parent know where you are going”), and positive parenting (6 items, e.g., “Your parent tells you that you are doing a good job”). Although the APQ contains an additional seven items that measure disciplinary techniques that do not qualify as corporal punishment, our analyses did not include these items. On a Likert-type 5-point scale (1 = never to 5 = always), participants indicate their agreement with each item based on the caretaker with whom they spend the most time. Each parenting behavior is calculated by summing the items, with lower scores suggesting lower frequency of a parenting behavior. See Table 1 for the APQ’s internal consistencies in the current study.
Parentification Inventory (PI)
We measured parentification by administering the Parentification Inventory (Hooper 2009), which served as a mediator in the current study. The PI evaluates the extent to which children carry out caregiver roles and obligations for which adults are generally responsible and assesses to what extent the parentification roles and responsibilities are perceived to be beneficial. The 22-item PI has three subscales: parent-focused parentification (12 items, e.g., “I often help solve problems between my parent(s)”), sibling-focused parentification (7 items, e.g., “I am the primary person who disciplines my siblings”), and perceived benefits of parentification (3 items, e.g., “I feel like our family is a team and work well together”). Participants self-report the extent to which they experience each statement on a Likert-type 5-point scale (1 = never true and 5 = always true), with higher scores indicating higher perceived levels of parentification or benefits of parentification. Each subscale is summed and averaged to create scores for parent-focused parentification, sibling-focused parentification, and perceived benefits of parentification that range between one and five. The internal consistencies for the PI subscales in the current study are reported in Table 1.
Positive and Negative Affect Schedule for Children (PANAS-C)
We measured depressive symptoms and well-being via the Positive and Negative Affect Schedule for Children (Laurent et al. 1999). The PANAS-C scores served as the outcome or dependent variable in the current study. The PANAS-C comprises 30 items that measure positive and negative affect, which serve as its two subscales: positive affect (15 items, e.g., “cheerful,” “energetic,” and “proud”) and negative affect (15 items, e.g., “sad,” “ashamed,” and “upset”). Student-participants self-reported their responses on a Likert-style 5-point scale (1 = very slightly or not at all to 5 = extremely). The positive affect and negative affect subscale scores are calculated by summing the 15 items in each subscale. Internal consistencies for the PANAS-C in the current study are reported in Table 1.
Data Analyses
First, we computed descriptive statistics for each of the study variables, followed by bivariate correlations. Second, we computed two sets of linear regression models using both the PANAS-C positive affect and the PANAS-C negative affect subscale scores separately as the dependent variables, with parenting behaviors as the independent variables in separate models (as measured by the APQ involvement, APQ positive parenting, APQ poor monitoring/supervision, APQ inconsistent discipline, APQ corporal punishment). For each significant association, we conducted a simple mediation analysis using all three parentification subscale scores collectively (as measured by parent-focused parentification, sibling-focused parentification, and perceived benefits of parentification) as the mediators. Last, we conducted a moderated mediation analysis by adding gender to each of the significant mediation models. The moderated mediation model is presented in Fig. 1. Grade was included as the only covariate in all regression and mediation models. All mediation analyses were conducted using the PROCESS macro (Hayes 2013) in SPSS Version 24.0. Descriptive statistics and regression analyses used the same version of SPSS.
Results
Bivariate Relations between Parenting Behavior and Adolescent Positive Affect and Negative Affect
Descriptive statistics for all study variables along with their bivariate correlations appear in Table 1. To determine the direct associations among the five parenting behaviors (APQ involvement, APQ positive parenting, APQ poor monitoring/supervision, APQ inconsistent discipline, APQ corporal punishment) and well-being and depressive symptoms (i.e., PANAS-C positive and negative affect), we computed simple linear regression models. Parameter estimates appear in Table 2.
Positive affect
Both APQ parental involvement and APQ positive parenting were significantly and positively related to well-being (positive affect). Greater APQ parental involvement and higher levels of APQ positive parenting were related to higher levels of well-being. The other three parenting behaviors—APQ poor monitoring/supervision, APQ inconsistent discipline, and APQ corporal punishment—were not significantly related to well-being (positive affect). The grade level of the adolescent was a significant covariate with a negative relationship in all five regression models, all p’s < 0.008, indicating the older the adolescent, the lower the positive affect scores.
Negative affect
In contrast, all five parenting behaviors measured by the APQ were significantly related to depressive symptoms (negative affect). Both APQ parental involvement and APQ positive parenting were negatively associated with depressive symptoms, indicating that higher levels of both APQ parental involvement and APQ positive parenting related to less signs of depressive symptoms (negative affect). However, APQ poor parental monitoring/supervision, APQ inconsistent discipline, and APQ corporal punishment were all positively related to depressive symptoms (negative affect), indicating that higher levels of APQ poor monitoring/supervision, more APQ inconsistent discipline, and higher levels of APQ corporal punishment were all associated with more indications of depressive symptoms (negative affect). The grade level of the adolescent was not a significant covariate in any of the simple regression models involving negative affect.
Mediating Effects of Parentification
Positive affect
The simple mediation analysis considered only those significant direct relations noted previously in the simple regression models (APQ parental involvement and APQ positive parenting) to determine whether a significant mediation effect was present by simultaneously adding all three PI subscales (parent-focused parentification, sibling-focused parentification, and perceived benefits of parentification) as possible mediators to each individual model. The direct and indirect effects for well-being (positive affect) appear in Table 3, with the mediation results displayed in Fig. 2. The PI perceived benefits of parentification subscale score was a significant partial mediator for both APQ parental involvement and APQ positive parenting, mediating 46 and 59% of the two positive direct effects, respectively. As seen in Fig. 2, adolescents with higher levels of either APQ parental involvement or APQ positive parenting reported higher levels of perceived benefits of parentification, which in turn was related to significantly greater levels of well-being (positive affect). Higher levels of perceived benefits of parentification bolstered the significant positive relation between well-being (positive affect) and both APQ parental involvement and APQ positive parenting. The grade level of the adolescent was also a significant covariate in the mediation model such that the higher the grade level, the lower the positive affect.

Significant simple mediation results for positive PANAS-C. *p < 0.05. cIndicates grade was a significant covariate at α = 0.05
Negative affect
The simple mediation results for depressive symptoms (negative affect) appear in Table 4, with the mediation results displayed in Fig. 3. Significant mediation effects were found in all five parenting behaviors. Both parent-focused parentification and the perceived benefits of parentification fully mediated the relations between depressive symptoms (negative affect) and the three parenting behaviors of APQ parental involvement, APQ positive parenting, and APQ poor monitoring/supervision. APQ inconsistent discipline was partially mediated, with parent-focused parentification mediating 11% of the direct effect between APQ inconsistent discipline and depressive symptoms (negative affect), while perceived benefits of parentification mediated 26%. APQ corporal punishment was also partially mediated, with perceived benefits of parentification mediating 33% of the direct effect between APQ corporal punishment and depressive symptoms (negative affect). Grade was a significant covariate in some of the subsets of relationships present in the mediation analyses. The grade of the adolescent was a significant covariate in all five of the mediation models, such that older adolescents were more likely to report lower levels of sibling-focused parentification. Additionally, grade level was a significant covariate in three of the five models (APQ poor monitoring/supervision, APQ inconsistent discipline, and APQ corporal punishment) such that adolescents in higher grades reported lower levels of parent-focused parentification.

Significant simple mediation results for negative PANAS-C. *p < 0.05. cIndicates grade was a significant covariate at α = 0.05
As seen in Fig. 3, four parenting measures—APQ parental involvement, APQ positive parenting, APQ poor monitoring/supervision, and APQ inconsistent discipline—were all significantly and positively related to parent-focused parentification, indicating that greater APQ parental involvement, greater APQ positive parenting, higher levels of APQ poor monitoring/supervision, and higher levels of APQ inconsistent discipline all relate to higher levels of parent-focused parentification. In turn, for each of these four measures, higher levels of parent-focused parentification result in higher levels of negative affect.
Looking at the mediating effects of parent-focused parentification, higher levels of APQ parental involvement and APQ positive parenting were shown to be directly related to reduced levels of depressive symptoms (negative affect). However, high levels of both parenting behaviors were related to increased levels of parent-focused parentification, which in turn was related to increased levels of depressive symptoms (negative affect). The mediating effect of parent-focused parentification altered the direction of the relationship between both APQ parental involvement and APQ positive parenting with depressive symptoms (negative affect). In contrast, parent-focused parentification magnified the relationship between APQ poor monitoring/supervision and APQ inconsistent discipline with depressive symptoms (negative affect). While the direct relationship showed higher levels of these two parenting behaviors resulting in greater depressive symptoms (negative affect), parent-focused parentification magnified this negative relation, meaning that higher levels of both parenting behaviors were related to increased levels of parent-focused parentification, which in turn was related to increased levels of negative affect.
As shown in Fig. 3, all five APQ subscale scores (i.e., APQ involvement, APQ positive parenting, APQ poor monitoring/supervision, APQ inconsistent discipline, APQ corporal punishment) were significantly related to the perceived benefits of parentification as measured by the PI. APQ parental involvement and APQ positive parenting were positively related, whereas APQ poor monitoring/supervision, APQ inconsistent discipline, and APQ corporal punishment were negatively related. That is, higher levels of APQ parental involvement and APQ positive parenting and lower levels of APQ poor monitoring/supervision, APQ inconsistent discipline, and APQ corporal punishment were significantly related to a greater level of perceived benefits of parentification. In each model, a greater level of perceived benefits of parentification was then negatively related to negative affect, indicating the greater the level of benefits of parentification, the lower the report of depressive symptoms (negative affect). In looking at the mediating effects of the perceived benefits of parentification, this subscale score bolstered the positive relation between negative affect and the three parenting measures of APQ poor monitoring/supervision, APQ inconsistent discipline, and APQ corporal punishment, while also bolstering the negative relation between depressive symptoms (negative affect) and the two parenting measures of APQ parental involvement and APQ positive parenting.
Moderating Effects of Gender
Last, we tested moderated mediation effects (see Fig. 1) to determine whether gender differences within the indirect effects existed for any significant mediation effects. Results for well-being (positive affect) are shown in Table 5, while results for depressive symptoms (negative affect) appear in Table 6. Only two significant gender differences within the indirect effects appeared within the moderated mediation analyses; these are displayed in Fig. 4, separated by gender. Both significant gender effects occur in models of negative affect. The conditional mediation effect was significantly stronger for females with regard to the perceived benefits of parentification for the relation between depressive symptoms (negative affect) and both APQ parental involvement and APQ corporal punishment. In both models, the grade level of the adolescents was a significant covariate, such that older adolescents experienced lower parent-focused parentification and lower sibling-focused parentification.

Significant moderated mediation results by gender. *p < 0.05. Boldfaced values indicate paths with significant gender differences. cIndicates grade was a significant covariate at α = 0.05
APQ parental involvement
As stated in the simple mediation results, APQ parental involvement was positively related to the perceived benefits of parentification, which in turn was negatively related to depressive symptoms (negative affect). The negative relation between the perceived benefits of parentification and negative affect was not significant for the males, yet significant for the females, indicating a stronger relationship for the females (see Fig. 4). These results suggest females are receiving a greater advantage (buffering effect) of the perceived benefits of parentification relative to their depressive symptoms (negative affect). If both genders had equal levels of perceived benefits of parentification, the females would have significantly lower depressive symptoms (negative affect) than their male counterparts.
APQ corporal punishment
Additionally, in the simple mediation results above, APQ corporal punishment was negatively related to the perceived benefits of parentification, which in turn was negatively related to depressive symptoms (negative affect). Separated by gender, males had a non-significant positive association between APQ corporal punishment and perceived benefit of parentification, while females had a significant negative association, indicating a stronger relationship for females as compared to males (See Fig. 4). These results suggest that females who experience APQ corporal punishment were negatively impacted (exacerbating effect), as compared to their male counterparts who were not significantly impacted. That is, females exhibited decreases in the perceived benefits of parentification, which correlated with greater levels of depressive symptoms (negative affect). The grade level was also a significant covariate in relation to negative affect, with older adolescents reporting higher levels of negative affect.
Discussion
The current study tested a moderated mediation analysis. Specifically, we explored the extent to which parentification mediates the relation between parenting behaviors and depressive symptoms and well-being (as measured by negative and positive affect) in a sample of early adolescents? And to what extent gender moderates the proposed mediation model? Several findings add to the literature base: (a) all five parenting behaviors were related to depressive symptoms; (b) perceived benefits of parentification mediated the association between all five parenting behaviors and depressive symptoms; (c) the impact of perceived benefits of parentification on the association between select parenting behaviors and depressive symptoms varied based on gender; and (d) no significant findings related to sibling-focused parentification emerged in the study.
First, regarding direct effects, several findings were consonant with the early adolescent literature base. Parental involvement and positive parenting are related with positive affect (Burton and Pössel 2017) and negatively related with negative affect; and poor monitoring/supervision, inconsistent discipline, and corporal punishment are positively related with depressive symptoms (Wimsatt et al. 2013). Noteworthy is the finding that all five parenting behaviors are related to depressive symptoms in the current study. This becomes of even greater importance when considering early adolescents’ rates of major depressive episodes are nearly three times greater than during childhood (National Institute of Mental Health 2012). These findings provide one example of the bimodal influence of parenting behaviors on depressive symptoms and well-being, something new to the early adolescent literature base. Without separating depressive symptoms into bimodal constructs (see Dejonckheere et al. 2018), researchers and clinicians may miss important findings on the relation among these variables. Also, consonant with Bronfenbrenner’s (1986) bioecological theory, the findings support the notion that parents are critical to adolescents’ microsystem, and thus have the most direct and significant impact on a range of psychosocial outcomes, such as internalizing and externalizing behavior (Peris et al. 2008), depression, and affect (Davidov and Grusec 2006; Johnson and Greenberg 2013).
Second, perceived benefits of parentification mediated the relations between well-being and parental involvement and positive parenting, as well as the relations between depressive symptoms and parental involvement and positive parenting. Moreover, when respondents reported lower levels of perceived benefits of parentification, they manifested a higher risk for experiencing depressive symptoms. The literature has often regarded parentification as a negative, adverse, or even traumatic childhood experience with severe and deleterious long-term outcomes (Cicchetti 2004; Hooper 2007b; Kubiak 2005), although, a growing body of research has attempted to clarify to what extent parentification is beneficial and, if so, through which pathways (Hooper et al. 2008; Stein et al. 2007; Tompkins 2007)? Toward this end, researchers have found that early adolescents may perceive parentification as a means to foster competencies for adulthood (Stein et al. 2007; Tompkins 2007) and strengthen emotional bonds among family members who may have been thrust into parentification due to serious medical conditions (Tompkins 2007). As the perceived benefits of parentification were found to have a significant indirect effect on both depressive symptoms and well-being in the current study, this construct might be similar to the construct of perceived fairness, that is, the extent to which parentified individuals perceive the parentification process as fair (see Jankowski et al. 2013). For example, Jankowski et al. (2013) found that fairness, or lack thereof, serves as a mediator between parentification and depressive symptoms. Those who considered the parentification experience to be beneficial might also view it as fair and vice versa. However, much of this literature is focused on young children (Stein et al. 2007; Tompkins 2007), adolescents (Stein et al. 2007; Tompkins 2007), and young adults (Hooper et al. 2008; Jankowski et al. 2013). Additional literature focused on early adolescents is needed.
Third, consonant with Bronfenbrenner’s (1986) tenets about the macrosystem, which recognizes socialization as a cultural factor influencing potential gender differences, we found that perceived benefits of parentification serves as a strong protective factor for females in the association between parental involvement and depression symptoms; whereas corporal punishment serves as a stronger predictor for females reporting lower levels of perceived benefits of parentification, thereby placing them at a higher risk for depression. Theoretically, we anticipated these findings; yet prior research specific to parenting behavior and gender differences has been mixed. In particular, studies have indicated that parental involvement in early adolescence is perceived as slightly more significant for males than females (Carlson 2006; Gryczkowski et al. 2010), but those studies measured externalizing behaviors. Thus, future studies should examine to what extent parental involvement serves as a protective factor differentially for males and females, depending on internalizing versus externalizing behavior. Our finding related to corporal punishment is congruent with past literature asserting that many males respond to corporal punishment through externalized symptoms and behaviors, while many females respond in internalized symptoms and behaviors (Jang 2007). While the current findings add to the mixed literature on parentification and gender in adolescents, the current study had a more complex focus: that is, the extent to which gender is implicated in a model focused on parentification as a mediator. With relevance to the positive aspects of parentification, previous research has relied on measures that did not include the construct of perceived benefits of parentification and were not composed of early adolescent samples (Burnett et al. 2006; Diaz et al. 2007; Kuperminc et al. 2009; Tompkins 2007). Consequently, our findings that gender matters in understanding the relations among these variables and in early adolescence are unique. Future studies should examine how perceived benefits of parentification may impact the relation between parenting behavior and depressive symptoms and well-being in other age groups, as well as in more racially, ethnically, and culturally diverse populations.
Fourth, although the study yielded diverse findings related to parent-focused parentification and perceived benefits of parentification, we had no significant findings related to sibling-focused parentification. This outcome was unexpected, given nascent research about sibling-focused parentification and mental health outcomes in adulthood (Tomeny et al. 2016), although many studies have not reported on outcomes uniquely focused on sibling-focused parentification (Hooper et al. 2012; Peris et al. 2008). Moreover, this finding was unexpected because we anticipated that sibling-focused parentification would serve as a significant mediator and thus lessen deleterious outcomes, including high levels of depression symptoms, given that sibling-focused parentification was negatively associated with psychosocial maladjustment in a previous study (see Fitzgerald et al. 2008). Our findings may be explained by the fact that siblings are sometimes viewed as friends, and therefore caring for them is perceived as more fulfilling, rewarding, and self-efficacious (Fitzgerald et al. 2008). Based on the current study’s findings, we propose that sibling-focused parentification may be adaptive in early adolescence. Future research should attempt to disentangle the differential effects of sibling-focused parentification compared to parent-focused parentification and examine whether to whom parentification is directed makes distinct contributions to diverse outcomes.
Strengths and Limitations
Given the influence of socialization on gender roles (East 2010), especially in relation to parentification (Burnett et al. 2006; Byng-Hall 2008; Diaz et al. 2007; Jurkovic 1997) and depressive symptomatology (Case and Paxson 2005), a significant strength of this study is its examination of gender as a moderator. In order to encourage empirical research consistent with the recent multicultural guidelines proffered by the American Psychological Association (APA 2017), future studies ought to include other moderators, such as race or ethnicity (East 2010; Hooper et al. 2011; Hooper and Blaustein 2014) and socio-economic and immigration status of the family, which have been identified as contributing to parentification (Arellano et al. 2018; Burton 2007; Hooper et al. 2011, 2018).
Although our study did not find that sibling-focused parentification mediated the relations between parent behaviors and well-being and depressive symptoms, we recommend that future studies continue to explore this construct. Additionally, the lack of information related to the sibling subsystem serves as a limitation of the study. Our findings are only representative of a broad sample, and since we did not collect information regarding age differences between siblings, sibling constellation, number of siblings, or sibling genders, we could not analyze within-group differences of those who experience sibling-focused parentification. It could be that individuals with diverse expectations of sibling-focused parentification may be affected in unique ways.
As with any individual study, several aspects of the research serve as limitations: (a) lack of an experimental design, (b) lack of longitudinal design, and (c) sole use of adolescent self-report measures. Without an experimental design, causal conclusions cannot be drawn. Further, although a longitudinal research design can provide more clarity regarding the direction of the relations among the variables, this is not possible with the cross-sectional design used in the current study. In addition, exclusively relying on self-report measures may result in inflated associations. That is, the respondent’s affect may impact their perceptions of the construct being measured, and thus the results should be interpreted cautiously. One way to mitigate these concerns in the future would be to have multiple informants, including parent-report measures, to increase quality of interpretability. An additional future consideration is the inclusion of observational data, often considered the gold standard (Douglas 2009), provided that the time and monetary resources are available to support such a labor-intensive method.
Another limitation is that of the family structure of the sample were unknown to the researchers. The number of siblings and the number of parents living in the home could have relevance on the parentification scales. Future research ought to consider using these as additional moderators in the analyses. A final limitation to the current study is that 75% of the sample identified as White American, with the remaining 25% representing Asian or Pacific Islanders, Black Americans, Latinx, Native American or Alaska Natives, and other races and ethnicities. Accordingly, although females and males were nearly equally represented, the generalizability of the outcomes is limited regarding individuals who identify with diverse racial and ethnic backgrounds. Thus, future studies should recruit a more racially and ethnically diverse sample and explore additional cultural factors as potential moderators (APA 2017; East 2010; Hooper et al. 2011).
References
American Humane Association. (2013). Child neglect. https://www.childwelfare.gov/pubPDFs/chronic_neglect.pdf
American Psychological Association. (2017). Multicultural guidelines: an ecological approach to context, identity, and intersectionality. http://preview.apa.org/about/policy/multicultural-guidelines.pdf
Arellano, B., Mier-Chairez, J., Tomek, S., & Hooper, L. M. (2018). Parentification and language brokering: an exploratory study of the similarities and differences in their relations to continuous and dichotomous mental health outcomes. Journal of Mental Health Counseling.
Bronfenbrenner, U. (1986). Ecology of the family as a context for human development: research perspectives. Developmental Psychology, 22, 723–742. https://doi.org/10.1037/0012-1649.22.6.723.
Bronfenbrenner, U, Morris, P. A, Damon, W., & Lerne, R. M. (2006). The bio-ecological model of human development. In Damon. W, Lerne. R. M, (eds.) Handbook of child psychology: theoretical models of human development. 6th. (pp. 793–828). Hoboken, NJ: Wiley.
Burnett, G., Jones, R. A., Bliwise, N. G., & Ross, L. T. (2006). Family unpredictability, parental alcoholism, and the development of parentification. American Journal of Family Therapy, 34, 181–189. https://doi.org/10.1080/019261800550437.
Burton, L. (2007). Childhood adultification in economically disadvantaged families: A conceptual model. Family Relations, 56, 329–345. https://doi.org/10.1111/j.1741-3729.2007.00463.x.
Burton, S. M., & Pössel, P. (2017). The adolescent blues: An investigation of the temporal directionality between parenting behavior and early adolescents’ affect.
Byng‐Hall, J. (2008). The significance of children fulfilling parental roles: Implications for family therapy. Journal of Family Therapy, 30, 147–162. https://doi.org/10.1111/j.1467-6427.2008.00423.x.
Carlson, M. J. (2006). Family structure, father involvement, and adolescent behavioral outcomes. Journal of Marriage and Family, 68, 137–154. https://doi.org/10.1111/j.1741-3737.2006.00239.x.
CaseA., & PaxsonC. (2005). Sex differences in morbidity and mortality. Demography, 42, 189–214. https://doi.org/10.1353/dem.2005.0011.
Centers for Disease Control and Prevention. (2015). Leading causes of death reports, national and regional, 1999-2014. https://www.cdc.gov/injury/wisqars/leading_causes_death.html.
Chase, N. D. (1999). Burdened children: Theory, research, and treatment of parentification. Thousand Oaks, CA: Sage.
Cicchetti, D. (2004). An odyssey of discovery: lessons learned through three decades of research on child maltreatment.American Psychologist, 59, 731–741. https://doi.org/10.1037/0003-066X.59.8.731.
Clark, L. A., & Watson, D. (1991). Tripartite model of anxiety and depression: psychometric evidence and taxonomic implications. Journal of Abnormal Psychology, 100, 316–336. https://doi.org/10.1037/0021-843X.100.3.316.
Cole, D. A., Ciesla, J. A., Dallaire, D. H, JacquezF. M., Pineda, A. Q., LaGrange, B., & Felton, J. W. (2008). Emergence of attributional style and its relation to depressive symptoms. Journal of Abnormal Psychology, 117, 16–31.https://doi.org/10.1037/0021-843X.117.1.16.
Crone, E. A., & Dahl, R. E. (2012). Understanding adolescence as a period of social–affective engagementand goal flexibility. Nature Reviews Neuroscience, 13, 636–650.
Davidov, M., & Grusec, J. E. (2006). Untangling the links of parental responsiveness to distress and warmth to child outcomes. Child Development, 77, 44–58.https://doi.org/10.1111/j.1467-8624.2006.00855.x.
Dejonckheere, E., Mestdagh, M., Houben, M., Erbas, Y., PeM.., Koval, P., & Kuppens, P. (2018). The bipolarity of affect and depressive symptoms. Journal of Personality and Social Psychology, 114, 323–341.https://doi.org/10.1037/pspp0000186.
Diaz, N., Siskowski, C., & Connors, L. (2007). Latino young caregivers in the United States: who are they and what are the academic implications of this role?. Child Youth Care Forum, 36, 131–140. https://doi.org/10.1007/s10566-007-9040-4.
Douglas, K. (2009). Sharpening our focus in measuring classroom instruction. Educational Researcher, 38, 518–521. https://doi.org/10.3102/0013189X09350881.
East, P. L. (2010). Children's provision of family caregiving: benefits or burden. Child Development Perspectives, 4, 55–61. https://doi.org/10.1111/cdep.2010.4.issue-1.
Fitzgerald, M. M., Schneider, R. A., Salstrom, S., Zinzow, H. M., Jackson, J., & Fossel, R. V. (2008). Child sexual abuse, early family risk, and childhood parentification: pathways to current psychosocial adjustment. Journal of Family Psychology, 22, 320–324. https://doi.org/10.1037/0893-3200.22.2.320.
Frick, P. J. (1991). The alabama parenting questionnaire. https://cyfar.org/sites/default/files/PsychometricsFiles/Parenting%20Questionnaire-Alabama%20(parents%20of%20children%206-18)_0.pdf
Garber, B. D. (2011). Parental alienation and the dynamics of the enmeshed parent–child dyad:Adultification, parentification, and infantilization. Family Court Review, 49, 322–335.
Gryczkowski, M. R., Jordan, S. S., & Mercer, S. H. (2010). Differential relations between mother's and father's parenting practices and child externalizing behavior. Journal of Child and Family Studies, 19, 539–546. https://doi.org/10.1007/s10826-009-9326-2.
Hayes, A. F (2013). An introduction to mediation, moderation, and conditional process analysis: a regression-based approach. New York, NY: Guilford.
Holder, M. K., & Blaustein, J. D. (2014). Puberty and adolescence as a time of vulnerability to stressors that alter neurobehavioral processes. Frontiers in Neuroendocrinology, 35, 89–110. https://doi.org/10.1016/j.yfrne.2013.10.004.
Hooper, L. M. (2007a). The application of attachment theory and family systems theory to the phenomena of parentification. The Family Journal, 15, 217–223.https://doi.org/10.1177/1066480707301290.
Hooper, L. (2007b). Expanding the discussion regarding parentification and its varied outcomes: implications for mental health research and practice. Journal of Mental Health Counseling, 29, 322–337. https://doi.org/10.17744/mehc.29.4.48511m0tk22054j5.
Hooper, L.M. (2009). Parentification inventory [measurement instrument]. http://guru.louisville.edu/parentification/uploads/1/8/9/9/18990327/parentification-inventory-2009-website.pdf
Hooper, L. M., DeCoster, J., White, N., & Voltz, M. L. (2011). Characterizing the magnitude of the relation between self-reported childhood parentification and adult psychopathology: a meta-analysis. Journal of Clinical Psychology, 67, 1028–1043. https://doi.org/10.1002/jclp.20807.
Hooper, L. M., Doehler, K., Jankowski, P. J., & Tomek, S. E. (2012). Patterns of self-reported alcohol use, depressive symptoms, and body mass index in a family sample: the buffering effects of parentification. The Family Journal, 20, 164–178. https://doi.org/10.1177/1066480711435320.
Hooper, L. M, L'Abate, L., Sweeney, L. G., Gianesini, G., & Jankowski, P. J. (2013). Models of psychopathology: generational processes and relational roles. New York, NY: Springer.
Hooper, L. M., Marotta, S. A., & Lanthier, R. P. (2008). Predictors of growth and distress following childhood parentification: a retrospective exploratory study.Journal of Child and Family Studies, 17, 693–705. https://doi.org/10.1007/s10826-007-9184-8.
Hooper, L. M., Tomek, S., Bond, J. M., & Reif, M. S. (2015). Race/ethnicity, gender, parentification, and psychological functioning: comparisons among a nationwide university sample. The Family Journal, 23, 33–48. https://doi.org/10.1177/1066480714547187.
Jang, S. (2007). Gender differences in strain, negative emotions, and coping behaviors: a general strain theory approach. Justice Quarterly, 24, 523–553. https://doi.org/10.1080/07418820701485486.
Jankowski, P. J., Hooper, L. M., Sandage, S. J., & Hannah, N. J. (2013). Parentification and mental health symptoms: mediator effects of perceived unfairness and differentiation of self. Journal of Family Therapy, 35, 43–65. https://doi.org/10.1111/j.1467-6427.2011.00574.x.
Johnson, L. E., & Greenberg, M. T. (2013). Parenting and early adolescent internalizing: The importance ofteasing apart anxiety and depressive symptoms. Journal of Early Adolescence, 33, 201–226.
Jurkovic, G. J (1997). Lost childhoods: the plight of the parentified child. New York, NY: Routledge.
Kam, J. A. (2011). The effects of language brokering frequency and feelings on Mexican-heritage youth’smental health and risky behaviors. Journal of Communication, 61, 455–475. https://doi.org/10.1111/j.1460-2466.2011.01552.x.
Kaplow, J. B., & Widom, C. S. (2007). Age of onset of child maltreatment predicts long-term mental health outcomes. Journal of Abnormal Psychology, 116, 176–187. https://doi.org/10.1037/0021-843X.116.1.176.
Kerig, P. K (2014). Implications of parent-child boundary dissolution for developmental psychopathology: "Who is the parent and who is the child?". New York, NY: Routledge.
Kubiak, S. P. (2005). Trauma and cumulative adversity in women of a disadvantaged social location. American Journal of Orthopsychiatry, 75, 451–465. https://doi.org/10.1037/0002-9432.75.4.451.
Kuperminc, G. P., Jurkovic, G. J., & Casey, S. (2009). Relations of filial responsibility to the personal and social adjustment of Latino adolescents from immigrant families. Journal of Family Psychology, 23, 14–22. https://doi.org/10.1037/a0014064.
Lambert, S. F., McCreary, B. T., Joiner, T. E., Schmidt, N. B., & Lalongo, N. S. (2004). Structure of anxiety and depression in urban youth: an examination of the tripartite model. Journal of Consulting and Clinical Psychology, 72, 904–908. https://doi.org/10.1037/0022-006X.72.5.904.
Laurent, J., Catanzaro, S. J., Joiner, T. E., Rudolph, K. D., PotterK. I.., Lambert, S., & Gathright, T. (1999). A measure of positive and negative affect for children: scale development and preliminary validation. Psychological Assessment, 11, 326–338. https://doi.org/10.1037/1040-3590.11.3.326.
Mazefsky, C. A., & Farrell, A. D. (2005). The role of witnessing violence, peer provocation, family support, and parenting practices in the aggressive behavior of rural adolescents. Journal of Child and Family Studies, 14, 71–85. https://doi.org/10.1007/s10826-005-1115-y.
Mika, P., Bergner, R. M., & Baum, M. C. (1987). The development of a scale for the assessment of parentification. Family Therapy, 14, 229–236.
National Institute of Mental Health. (n.d.). Research domain criteria. http://www.nimh.nih.gov/research-priorities/rdoc/index.shtml
National Institute of Mental Health. (2012). Major depression among adolescents. http://www.nimh.nih.gov/health/statistics/prevalence/major-depression-among-adolescents.shtml
Peris, T. S., Goeke-Morey, M. C., Cummings, E. M., & Emery, R. E. (2008). Marital conflict and support seeking by parents in adolescence: empirical support for the parentification construct.Journal of Family Psychology, 22, 633–642. https://doi.org/10.1037/a0012792.
Schimmenti, A., & Bifulco, A. (2015). Linking lack of care in childhood to anxiety disorders in emerging adulthood: the role of attachment styles.Child and Adolescent Mental Health, 20, 41–48. https://doi.org/10.1111/camh.12051.
Sfoggia, A., Pacheco, M. A., & Grassi-Oliveira, R. (2008). History of childhood abuse and neglect and suicidal behavior at hospital admission.Crisis, 29, 154–158. https://doi.org/10.1027/0227-5910.29.3.154.
Stein, J. A., Rotheram-Borus, M. J., & Lester, P. (2007). Impact of parentification on long-term outcomes among children of parents with HIV/AIDS.Family Process, 46, 317–333. https://doi.org/10.1111/j.1545-5300.2007.00214.x.
Tomeny, T.S., Barry, T.D., & Fair, E.C. (2016). Parentification of adult siblings of individuals with autism spectrum disorder: distress, sibling relationship attitudes, and the role of social support. Journal of Intellectual & Developmental Disability. https://doi.org/10.3109/13668250.2016.1248376
Tompkins, T. L. (2007). Parentification and maternal HIV infection: beneficial role or pathological burden. Journal of Child and Family Studies, 16, 113–123. https://doi.org/10.1007/s10826-006-9072-7.
U.S. Department of Health and Human Services (HHS), National Center on Child Abuse and Neglect, National Child Abuse and Neglect Data System. (2014). Child maltreatment 2014: Reports from the states to the National Center on Child Abuse and Neglect. Washington, DC: U.S. Government Printing Office.
Weinberger, A. H., Gbedemah, M., Martinez, A. M., Nash, D., Galea, S., & Goodwin, R. D. (2018). Trends in depression prevalence in the USA from 2005 to 2015: widening disparities in vulnerable groups.Psychological Medicine, 48, 1308–1315. https://doi.org/10.1017/S0033291717002781.
Wimsatt, A. R., Fite, P. J., Grassetti, S. N., & Rathert, J. L. (2013). Positive communication moderates therelationship between corporal punishment and child depressive symptoms. Child and Adolescent Mental Health, 18, 225–230. https://doi.org/10.1111/j.1475-3588.2012.00682.x.
Author Contributions
S.B.: collaborated on the study design, writing of the study, and editing of the final paper. L.M.H.: designed the study, assisted with the data analyses and results, and wrote the paper. S.T.: analyzed the data, wrote the results, and aided in the writing and editing of the final paper. B.C.: organized the data collection and aided in the writing and editing of the final paper. A.W.: collaborated in the writing and editing of the final paper. P.P.: collaborated on the design of the study and in the writing and editing of the final paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The Institutional Review Board at the University of Louisville approved this study.
Informed Consent
Informed consent was obtained from all participants of the study.
Rights and permissions
About this article

Cite this article
Burton, S., Hooper, L.M., Tomek, S. et al. The Mediating Effects of Parentification on the Relation Between Parenting Behavior and Well-Being and Depressive Symptoms in Early Adolescents. J Child Fam Stud 27, 4044–4059 (2018). https://doi.org/10.1007/s10826-018-1215-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-018-1215-0