
Abstract
Background
Childhood internalizing and externalizing problems are closely related and often co-occur. Directional models have been employed to test how these problems are related, while few studies have tested a third variables model.
Objective
This study investigates whether internalizing and externalizing problems are reciprocally or unidirectionally related, whether these relations can be explained by third variables, and how these relations are associated with onset and stability.
Methods
A community sample of 1,434 children aged 5.08 (SD = 1.25) and their mothers participated in two 1-year interval data waves. Internalizing and externalizing problems were examined with the Strengths and Difficulties Questionnaire.
Results
Using latent cross-lagged modeling, externalizing problems were found not be related to subsequent internalizing problems, or vice versa. These results were also found when controlling for inadequate parenting, parenting stress, maternal health and social preference. When taking problem level into account, externalizing problems were related to stability of clinical level internalizing problems, even when controlling for third variables inadequate parenting, parenting stress, maternal mental health and social preference.
Conclusions
Strong autoregressive paths for internalizing and externalizing problems were found. Internalizing and externalizing problems do not seem to influence each other over time in the community sample. When investigating relations among internalizing and externalizing problems, it seems to be important to take problem level into account.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Internalizing and externalizing problems represent the two major psychopathologies of early childhood, are closely related and tend to co-occur (Achenbach et al. 1991; Lilienfeld 2003; Oland and Shaw 2005). Although research has begun to unravel how and why these problems are associated, it remains unclear whether third variables may explain the relations between internalizing and externalizing problems. As such, it is deemed important to simultaneously examine a directional model and a third variable model of childhood psychopathology (cf. Lee and Bukowski 2012; Mathiesen et al. 2009). Therefore, the current study investigated whether internalizing and externalizing problems are reciprocally or unidirectionally related over time. Further, it tested whether relations between internalizing and externalizing problems might be explained by third variables.
The interrelatedness of internalizing and externalizing problems in childhood and adolescence has largely been studied from a directional model perspective. Studies starting from this perspective have addressed whether internalizing problems precede externalizing problems (Bittner et al. 2007; Ialongo et al. 1996; Last et al. 1996; Ritakallio et al. 2008; Vitaro et al. 2000), which is in line with the acting out hypothesis that depressive symptoms lead to acting out behaviors (Glaser 1967), or the hypothesis that anxiety underlies aggression (Granic 2012). Others studies have applied the failure model which suggests that conduct problems lead to failures in social situations that in turn lead to anxiety and depression (Patterson and Capaldi 1990), and indeed found externalizing problems to precede internalizing problems (Boylan et al. 2007, 2012; Burke et al. 2005; Copeland et al. 2009; Hoglund and Leadbeater 2004; Lahey et al. 2002; Speltz et al. 1999). Finally, studies have addressed whether change in one cluster of problems is associated with changes in the other and act as risk factor to the other (Gilliom and Shaw 2004; Keiley et al. 2000; Lee and Bukowski 2012; Mesman et al. 2001). While these studies provide evidence for direct relations between internalizing and externalizing problems, there are also studies examining the role of third variables in explaining this relationship (Fergusson et al. 1996; Weiss et al. 1998). Third variables may act as latent or indirectly observed tendencies to develop a disorder (Krueger and Markon 2006). Consequently, third variables could be described as those factors that are related to multiple disorders, such as to internalizing and externalizing problems, and are hypothesized to underlie both problems.
As stated by many researchers, studies on co-variation of disorders are highly complex and subject to problems on various levels (heterogeneity of terminology concerning ‘comorbidity’, sampling or referral bias, informant bias, variability in diagnostic and analytic procedures, taxonomic problems and symptom overlap (Angold et al. 1999; Krueger and Markon 2006). Although recently there is increasing evidence that covariation of disorders is more than a conceptual artifact or methodological nuisance (cf. Lee and Bukowski 2012; Mathiesen et al. 2009),developmental pathways are far from being completely unraveled. This study adds to the plethora of research in various ways. First, most studies have focused on either the directional or the third variables model, and have not evaluated these models simultaneously. Second, few studies have studied multiple third variables and corrected for spurious relations. This study focuses on several contextual third variables known to be related internalizing and externalizing problems. Third, this study employs rigorous modeling techniques such as cross-lagged modeling. Fourth, we focus on young children where relations between internalizing and externalizing may be different than for older children or adolescents.
According to transactional ecological models of psychopathology, the interplay between biological, psychological and social systems contributes to the development of internalizing and externalizing problems (Bronfenbrenner and Evans 2000; Cicchetti and Toth 1998). Specifically, factors from social systems such as parents and peers may underlie both internalizing and externalizing problems as they are proximal to the child and hypothesized to exert great influence during early childhood (Cicchetti and Toth 1998; Ford et al. 2007). As such, the covariation among internalizing and externalizing problems may be in part explained by common factors in the social system wherein the child is developing. Indeed, inadequate parenting, parenting stress and maternal mental health have been strongly linked to internalizing and externalizing problems (e.g., Arnold et al. 1993; Barry et al. 2005; Beardslee et al. 1998; Gross et al. 2008; Prinzie et al. 2003; Rodriguez 2011). Furthermore, children disliked by their peers, indicated by low social preference, have often been reported as showing more internalizing and externalizing problems than their peers who are not disliked (e.g., Gooren et al. 2011; Laird et al. 2001). Thus, inadequate parenting, parenting stress, maternal mental health and low social preference are hypothesized to act as third variables, thereby explaining a possible spurious relation between internalizing and externalizing problems.
Some empirical evidence supports the premises that third variables partially explain the relations between internalizing and externalizing problems (Gjone and Stevenson 1997; Kessler et al. 2011). The following two studies show how third variables explain relations between in- and externalizing problems. In a sample of children followed from 18 months to 4.5 years, internalizing and externalizing problems were moderately related. Yet, when controlling for family stress, partner support and child emotionality, this relation became substantially weaker (Mathiesen et al. 2009). Similarly, in boys aged 10–13, but not girls, reciprocal effects of externalizing and internalizing problems over time became smaller when including parental violence to the model (Lee and Bukowski 2012). However, other studies do not support that third variables explain these results. In contrast, these studies show that relations hold while controlling for these variables (Bornstein et al. 2010; Burt and Roisman 2010; Mesman et al. 2001). First, in a study that followed preschoolers through adolescence, predictive paths from externalizing problems to internalizing problems were found, and these were not altered by the inclusion of the third variable social problems (Mesman et al. 2001). Second, a study following preschoolers through adolescence found externalizing problems to impact academic competence which in turn impacted internalizing problems. These associations held while controlling for gender, socioeconomic status, early caregiving and cognitive ability (Burt and Roisman 2010). Third, children followed from early childhood to adolescence were found to have more problems when their social competence was lower at preschool, when controlling for intelligence, maternal education and social desirability (Bornstein et al. 2010). Clearly, more research is needed in order to examine how internalizing and externalizing problems are related over time. These studies have not been conducted in early childhood, where effects of common environmental influences on co-occurring internalizing and externalizing problems were found to be greatest (Gjone and Stevenson 1997). Further, two of these studies employed latent growth curve modeling, a person-centered approach (Lee and Bukowski 2012; Mathiesen et al. 2009). Although person-centered analyses are important, variable-centered analyses are advised when investigating associations between variables, and when investigating the relative contribution that a predictor variable (e.g., externalizing problems) makes to an outcome (e.g., internalizing problems) (Laursen and Hoff 2006). Also, the risk factors included in these studies did not take parenting into account, which is known to be an important factor in the development of child psychopathology (e.g., Dishion and Patterson 2006). Finally, the former studies did not emphasize whether the two problem clusters predict each other’s onset or stability, nor whether the third variables impact onset or stability specifically. It seems essential to establish which third variables impact onset versus stability. As such, it would be possible to distinguish between factors that set the stage for problem behavior versus factors that affect symptoms when the problem behavior is already present.
In sum, the purpose of the present longitudinal study is to test both a directional and third variables model of internalizing and externalizing problems in early childhood in a large sample. First, we examined whether parent-reported internalizing and externalizing problems are related reciprocally or unidirectionally. We expected that externalizing problems are strongly related to subsequent internalizing problems, and vice versa. Second, we identified third variables that are related to internalizing and externalizing problems over time. Specifically, we simultaneously examined the associations of inadequate parenting, parenting stress, maternal mental health, and social preference with both internalizing and externalizing problems, while controlling for the other problem cluster. It is expected that, parenting stress, inadequate parenting, maternal mental health, and social preference act as third variables for both internalizing and externalizing problems. Further, we investigated whether internalizing and externalizing problems are related to each others’ onset and stability and to what extent third variables contribute to these associations. It is expected that internalizing problems are related to stability in externalizing problems, and vice versa. Furthermore, all third variables are expected to be related to onset and stability of internalizing and externalizing problems.
Method
Sample and Procedure
Mothers of children aged 4–7 from 29 primary schools throughout the Netherlands were recruited for the Dutch “Child in Sight (Kind in Zicht)” study, of whom 1,339 mothers filled in questionnaires for their children (M age = 5.08, SD = 1.25, 50.1 % boys) in the first assessment (T1). In a subsequent assessment 1 year later (T2) the participation rate was 67 %, with 95 parents who did not participate in the baseline assessment. Due to use of Structural Equation Modeling, wherein missing cases are accounted for, our final number of participants is 1,434. At baseline, mothers had a mean age of 36.61 (SD = 4.41), the majority were of Dutch origin (92.4 %) and were part of a two-parent household (89.1 %). Most mothers, 44.6 %, were highly educated with a college or university degree, 37.8 % finished vocational education and 13.7 % finished a low level of Dutch secondary school, 3.9 % finished a different form of education. A logistic regression analysis showed that families who completed two waves (n = 817) did not differ from the dropouts (n = 522) in child age, sex, maternal educational level, internalizing, and externalizing problems.
We used data of two annual waves of Kind in Zicht, a large cohort study of Dutch children aged 4–7 at baseline which was approved by the committee on ethics. Schools were randomly selected from the population of elementary schools in the Netherlands. Schools in the larger provinces, Noord-Holland, Zuid-Holland, Noord-Brabant and Gelderland and the four largest cities, Amsterdam, Rotterdam, The Hague and Utrecht, were oversampled. In total, 440 schools were selected. Principals of these schools first received a letter inviting them to participate in the study and subsequently, were asked for participation by phone, which led to participation of 29 schools (6.6 %), containing 2,558 children in two kindergarten classes, Grade 1 and 2. Schools received €1,000 for their participation. Teachers handed out information and consent letters to parents. In total, 110 classrooms participated in the baseline assessment. Class sizes varied from 7 to 36 children. Sociometry interviews were conducted by trained interviewers from January until March 2010 in the schools, outside of the classroom. Passive consent of 2,360 (92.3 %) parents was obtained. Only mothers were allowed to participate in the study, as a mother is the primary caregiver in most families (Renk et al. 2003). In both waves mothers completed questionnaires either digitally or by paper and pencil.
Measures
Internalizing and Externalizing Problems
The Dutch parent version of a screening questionnaire for psychopathology, the Strengths and Difficulties Questionnaire was used at both waves to assess internalizing and externalizing problems (SDQ; van Widenfelt et al. 2003). The SDQ has been shown reliable and valid for use in a community sample (see for a review Stone et al. 2010). The subscale emotional symptoms (e.g., many worries, often seems worried) was used to measure internalizing problems. The conduct problems scale (e.g., often lies or cheats) was used to measure externalizing problems. Each scale contains five items and parents rated their child’s behavior on a 3-point scale ranging from 0 (not true) to 2 (certainly true). The scoring procedures used in this study are available online at www.sdqinfo.com. As scale distributions of the SDQ are skewed, alternative indicators of reliability based on Structural Equation Modeling—known as Jöreskog rho or McDonalds Omega H , were used to assess reliability (Jöreskog 1971; McDonald 1978, 1999; Revelle and Zinbarg 2009; Stone et al. 2013a). Omega (ωh) values were .79 and .80 at T1 and T2 for the emotional symptoms scale, and .71 and .75 at T1 and T2 and for the conduct problems scale.
Inadequate Parenting
The Parenting Scale was used at the first wave and asks parents to rate 30 short parenting situations on a 7-point scale (Arnold et al. 1993). Sample items include “When I want my child to stop doing something I firmly tell my child to stop/I coax or beg my child to stop” and “When I’m upset or under stress I am picky and on my child’s back/I am no more picky than usual”. Inadequate parenting behavior is divided across three subscales: permissiveness, restrictiveness, and verbosity. All the items sum up to the total score, which was used in the current study. The higher the score, the more inadequate the parenting behavior is. Psychometric properties are adequate (Arnold et al. 1993). Cronbach’s alpha was .78 for the total score.
Parenting Stress
At the first wave, mothers rated the frequency of daily hassles with their child over the past 6 months (Parenting Daily Hassles: PDH; Crnic and Greenberg 1990). The questionnaire consists of 20 events of which the parent has to rate how often (seldom, sometimes, often, constantly) they occur. Sample items include “Continually cleaning up messes of food and toys” and “The kids demand that you entertain them or play with them”. Psychometric properties of the PDH have been found adequate (Crnic and Greenberg 1990; Rispens et al. 1996). Cronbach’s alpha was .77.
Mental Health
The degree of mental health of the mothers during the past 4 weeks was measured at the first wave with a short version of the General Health Questionnaire (GHQ; Hardy et al. 1999). Mothers rated their mental health via 12 questions (e.g., did you lose confidence in yourself? did you feel able to make decisions?) on a 4-point scale. The summed items yield a total score, with higher scores indicating diminished mental health. Research into reliability and validity indicates that the GHQ has adequate psychometric properties (Koeter and Ormel 1991). Cronbach’s alpha was .89.
Social Preference
During individual interviews, children were shown a photograph of their classmates. A trained research assistant pointed out a child on the photograph and asked the child whether (s)he knew who this child was, ensuring familiarity, and was then asked whether (s)he liked, disliked the child or thought neutral of him/her (cf. Coie et al. 1982; Otten et al. 2009). To increase comprehension and ease shy children, the child could respond verbally or by pointing to three fluffy smileys, with either a happy, sad or neutral expression. This procedure was repeated until the child gave a nomination about every child in the class. The order of asking questions about children in the photograph was counterbalanced, such that the interviewer started either at the upper left, upper right, lower left or lower right corner of the photograph. Unlimited nominations (like, dislike, neutral) were used, because these tend to spread more evenly among children in a class than limited nominations (i.e., fewer children receive a raw nomination score of zero). The total least-liked nomination was subtracted from the total most-liked nomination to obtain a measure of social preference. Social preference scores were then standardized within each classroom (cf. Coie et al. 1982).
Strategy for Analysis
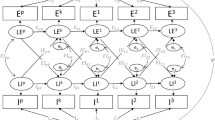
First, means, standard deviations and bivariate correlations of all study variables were calculated. Second, to evaluate the associations of internalizing and externalizing problems over time, we tested a latent cross-lagged path model while controlling for sex and age, and subsequently including the third variables inadequate parenting, parenting stress, maternal mental health and social preference in the model, using MPLUS version 5 (Muthén and Muthén 1998–2007; see Fig. 1 for the conceptual model). Internalizing and externalizing problems are latent variables measured by five items each. The items have 3-points response scales and are mostly very positively skewed. For this type of items (denoted as ordered categorical in Mplus) we used the Weighted Least Square estimator with Mean- and Variance-adjusted Chi square test statistic (WLSMV). Asparouhov and Muthén (2010) have investigated the consistency of the WLS(MV)-estimator under various missing data assumptions and concluded that using all available pairwise information in the data produced unbiased and efficient estimates for the parameters to be estimated. As χ2 is known to be affected by sample size, and may become significant easily with large samples, a significant χ2 is not directly interpreted as indicative of poor fit (Schermelleh-Engel et al. 2003). For this reason we used the comparative fit index (CFI, critical value ≥.90) (Bentler and Bonett 1980), the Tucker Lewis Index (TLI, critical value ≥.90) (Bentler 1990) and the root mean squared estimate of approximation (RMSEA, critical value ≤.08) (Browne and Cudeck 1992), to establish model fit.

Conceptual model. Variable abbreviations include internalizing problems (INT), externalizing problems (EXT), inadequate parenting (IP), parenting stress (PS), mental health (MH), social preference (SP). Numbers after variable names refer to data waves
Third, we tested whether the model parameters differed for children with no internalizing (n = 1,243, score 0–3) or no externalizing problems at T1 (n = 1,200, score 0–2) (non-cases) and children with internalizing (n = 191, score 4–10) or externalizing problems (n = 234, score 3–10) in the clinical range (cases) at T1. Continuous internalizing and externalizing scores were classified into ‘non-cases’ and ‘cases’ scores based on the SDQ’s scoring procedures, at T1 and T2, such that approximately 90 % of children are classified as non-cases. Goodman (2001) examined the clinical validity of this scoring method extensively and found adequate clinical validity for the parent version of the SDQ. We tested four models with one including non-cases of internalizing problems at T1 and predicting onset of internalizing ‘caseness’ at T2 (e.g., predicting a score of 0 = no clinical level internalizing problems, versus 1 = clinical level internalizing problems present), and one including cases of internalizing problems at T1 and predicting stability in internalizing problems at T2. The third model includes non-cases of externalizing problems at T1 and predicts onset of externalizing problems at T2. The fourth model includes cases of externalizing problems at T1 and predicts stability in externalizing problems at T2. Because the use of latent constructs would lead to too many parameters to be estimated for the sample size that we had, we used observed variables for the onset and stability analyses. In all of these models again we controlled for sex and age, and the third variables were included to test whether third variables accounted for the variance in the possible association between internalizing and externalizing problems. Also, we controlled for concurrent associations between internalizing and externalizing problems at T2. As our dependent variable in the onset and stability analyses is categorical, we used the WLSMV-estimator.
As children are in the same classes, our data may be nested such that children from the same classes may share common behaviours (i.e., clustering). Therefore, we corrected for this in our analyses using the TYPE is COMPLEX command in Mplus.
Results
Descriptive Statistics
As expected, internalizing and externalizing problems were significantly related (Table 1). Further, internalizing problems at T1 were strongly correlated with internalizing problems at T2, indicating high stability of these problems. A similar association was found for externalizing problems, again indicating stability of these problems in young children. Internalizing problems at T1 were most strongly related to parenting stress at T1, and internalizing problems at T2 were most strongly related to parenting stress, and maternal mental health, while externalizing problems at T1 and T2 were most strongly associated with inadequate parenting, parenting stress and social preference. At both waves, more internalizing than externalizing problems were reported. Finally, on average, internalizing problems increased from T1 to T2, whereas externalizing problems decreased.
Model Findings
Fit statistics for the model investigating the relations between internalizing and externalizing problems were satisfactory [χ2(186) = 349.43, p < .001; CFI = .952; RMSEA = .028 (CI .023–.033); TLI = .941]. Standardized estimates are presented in Fig. 2 and factor loadings are presented in Fig. 3. Internalizing problems at T1 predicted subsequent internalizing problems, and externalizing problems at T1 predicted externalizing problems at T2. No cross-lagged associations were found. Sex was negatively associated with externalizing problems at T1 and T2. This means that mothers reported more externalizing problems for boys than for girls. Age was positively related to internalizing problems at T1, indicating that mothers reported more internalizing problems for older children.

Latent cross-lagged model without controlling for third variables. Variable abbreviations include inadequate parenting (IP), parenting stress (PS), mental health (MH), social preference (SP). Numbers after variable names refer to data waves. Only significant associations are presented here for clarity reasons

Presentation of factor loadings in the measurement model without controlling for third variables. Numbers after variable names refer to data waves
When including the third variables in the model, the fit statistics were satisfactory [χ2(250) = 452.65, p < .001; CFI = .944; RMSEA = .027 (CI .023–.031); TLI = .927]. Standardized estimates are presented in Fig. 4 and factor loadings are presented in Fig. 5. Internalizing problems at T2 were predicted by maternal general health, such that the more health related problems mothers experienced at T1 the more internalizing problems their children showed 1 year later. For externalizing problems, parenting stress was positively related to externalizing problems, which means that the more parenting stress mothers experienced at T1, the more externalizing problems their children had 1 year later. None of the other variables predicted internalizing and externalizing problems. No cross-lagged paths were found from internalizing to externalizing problems and vice versa. Sex was negatively associated with externalizing problems at T2. This means that mothers reported more externalizing problems for boys than for girls. Age was positively related to internalizing problems at T1, indicating that mothers reported more internalizing problems for older children.

Latent cross-lagged model, controlling for third variables. Variable abbreviations include inadequate parenting (IP), parenting stress (PS), mental health (MH), social preference (SP). Numbers after variable names refer to data waves. Only significant associations are presented here for clarity reasons

Presentation of factor loadings in the measurement model while controlling for third variables. Numbers after variable names refer to data waves
Furthermore, inadequate parenting and parenting stress were positively associated to externalizing problems concurrently, such that the more inadequate parenting and parenting stress were reported, the more externalizing problems. Also, social preference at T1 was negatively related to externalizing problems at T1. The lower the child’s social status, the more externalizing problems were reported. These relations were absent longitudinally. Parenting stress was related to internalizing problems concurrently, such that the more parenting stress was reported, the more internalizing problems children showed. Again, this relation was absent longitudinally.
Onset and Stability
The standardized estimates of the models for onset and stability are presented in Table 2. These models were saturated, therefore no fit statistics are given.Footnote 1 Externalizing problems of children at T1 were related to onset for children without clinical internalizing scores at T1 and to stability in internalizing problems at T2 for children with clinical internalizing scores at T1. When we controlled for third variables, the relation of externalizing problems with onset of clinical level internalizing problems disappeared. This means that externalizing problems are related to stability of already existing internalizing problems over time quite robustly, while this does not hold for onset of clinical level internalizing problems. Regarding third variables, maternal mental health was related to both onset and stability of clinical level internalizing problems. This indicates that the more mental health related problems mothers experienced, the more internalizing problems they reported at T2 for children who were rated as non-clinical in their internalizing problems at T1 and for children who were rated as clinical in their internalizing problems at T1. Inadequate parenting and parenting stress were related to internalizing problems at T2 for children who were rated as non-clinical in their internalizing problems at T1, but were not related to stability of internalizing problems at T2 for children who were already rated as having clinical internalizing problems at T1. This indicates that inadequate parenting and parenting stress were related to the onset of internalizing problems, but not on the stability of these problems over time.
Internalizing problems were related to onset of externalizing problems, but this relation disappeared when we controlled for third variables. Further, internalizing problems were not related to stability of clinical level externalizing problems. As for third variables, only parenting stress was related to the stability of clinical level externalizing problems. This indicates that the more parenting stress mothers experienced, the more externalizing problems they reported at T2 for children who were rated as clinical in their externalizing problems at T1.
Discussion
The current study investigated whether parent reported internalizing and externalizing problems are related unidirectionally or reciprocally in early childhood and whether third variables may explain these relations. Our longitudinal design and large sample size permitted us to test these questions using a rigorous analytical approach. Therefore, the results of this study add to the body of literature investigating relations among internalizing and externalizing problems. We found strong relative stability of internalizing and externalizing problems over time. Further, evidence for these problem clusters reciprocally influencing each other seemed to depend on severity of the problems. When problem level was not taken into account, externalizing problems were not related to subsequent internalizing problems. Internalizing problems did not have any relation with externalizing problems 1 year later in the total sample. Still, when classifying the internalizing and externalizing scores as clinical and non-clinical based on the norm cut-off we employed, externalizing problems at baseline were related to onset of internalizing problems 1 year later and to stability of already existing internalizing problems at baseline. The effects regarding stability, but not onset, remained strong when we controlled for third variables, indicating that externalizing problems are substantially related to existing clinical internalizing problems. Internalizing problems were related to onset of subsequent externalizing problems, but not to stability of externalizing problems. Moreover, this relation diminished when third variables were taken into account.
From these results, we may conclude that externalizing problems have a robust association with subsequent clinically elevated internalizing problems (i.e., the stability of these problems), even when controlling for third variables. As such, these results are partly in favor of a directional model and a third variables model (Fergusson et al. 1996; Patterson and Capaldi 1990; Weiss et al. 1998). Furthermore, these results also point out that we did not find evidence for the ‘acting out’ or ‘anxiety underlying aggression’ hypotheses from directional models in the current study as internalizing problems were not related to subsequent externalizing problems when controlling for third variables (Glaser 1967; Granic 2012).
According to one of the directional models (i.e., the failure model), conduct problems lead to failures in social situations that in turn lead to anxiety and depression (Patterson and Capaldi 1990). According to this model one would expect that externalizing problems at baseline predict ‘new cases’ of internalizing problems 1 year later (cf. Lahey et al. 2002). Our results only partly support this, as this relation became non-significant when including parent and peer factors. We did find that concurrent externalizing problems were related to subsequent clinically elevated internalizing problems for children already scoring in the 10 % highest range at baseline, even when controlling for inadequate parenting, parenting stress, maternal mental health and social preference. Conclusively, the present findings suggest that externalizing problems in early childhood may better be viewed as a strong maintaining factor in clinical internalizing problems and less likely to be a precipitating factor as the Patterson and Capaldi model would suggest (Lahey et al. 2002). As our study was the first to employ cross-lagged modeling with continuous and categorical variables, we contributed to the large body of literature by showing that the role of externalizing problems in the development of internalizing problems seems to depends on its severity.
Regarding the third variables model, when observing the stronger relations of externalizing with internalizing problems in the group with high internalizing levels at baseline, inclusion of third variables did not decrease this relation. On the other hand, results regarding onset do offer some support for the third variables model, in that relations of internalizing problems with onset of externalizing problems, and vice versa became weaker and nonsignificant when including third variables. These results thus partly support the third variables model (Fergusson et al. 1996; Weiss et al. 1998) and are partly in line with former studies, which also reported a decrease of reciprocal influences of internalizing and externalizing, although not a complete disappearance when including third variables (Lee and Bukowski 2012; Mathiesen et al. 2009). Furthermore, it should be noted that the third variables explained only a modest amount of variance in in- and externalizing problems. Possibly, relatively stable third variables such as genetic liability or temperament, could potentially account for the association of externalizing problems with elevated internalizing problems (Keiley et al. 2000; O’Connor et al. 1998).
Still, we did find that some of the included variables were specifically related to either internalizing or externalizing problems, and we were able to distinguish which variables are related to onset of problem behavior and which affect symptoms in children with elevated levels of problems at baseline. First, parenting stress was related to subsequent externalizing problems in the total sample and onset of clinical internalizing problems. These results are in line with studies showing strong concurrent links of parenting stress with internalizing problems (e.g., Rodriguez 2011), longitudinal effects of parenting stress on externalizing problems (e.g., Benzies et al. 2004), and highlight the salience of parenting stress (Deater-Deckard 2004). Parenting stress also was related to stability of clinical externalizing problems but not of clinical internalizing problems. This suggests that parenting stress might be a maintaining factor for clinical externalizing problems, which may be explained by the lack of consistent parenting associated with parenting stress (Pinderhughes et al. 2000).
Second, maternal mental health was related to subsequent internalizing problems in the total sample and onset and stability of clinically elevated internalizing problems. Possibly, maternal mental health can be seen as a broad-band specific feature (Weiss et al. 1998), which relates primarily to the broad-band concept of internalizing problems specifically but not to externalizing problems. However, this finding is in contradiction to studies that have reported a link between maternal mental health and externalizing problems (Fanti and Henrich 2010; Gross et al. 2008). Although these studies did not control for parenting stress and inadequate parenting which are known to be related to maternal mental health (Deater-Deckard 2004), more research is needed to draw conclusions regarding the role of maternal mental health in relation to internalizing and externalizing problems.
Third, social preference was related to externalizing problems concurrently, but not longitudinally and not to onset and stability of clinical externalizing problems. These results coincide with research indicating that peer rejection is related to externalizing problems (Keiley et al. 2000). Exclusion by peers is proposed to lead to, or increase acting out behaviors (Loeber and Keenan 1994; Van Lier and Koot 2010), although our analyses regarding onset and stability do not support this reasoning. The reverse might also be true; children who show externalizing problems may be particularly prone to become excluded (Hammen 2006; Panak and Garber 1992).
Fourth, inadequate parenting was not related to internalizing and externalizing problems in the total sample, although concurrent relations were present. Apparently, the effects of maternal mental health and parenting stress are stronger than those of inadequate parenting when simultaneously evaluated. Inadequate parenting was related to onset of internalizing problems, and marginally to onset of externalizing problems. As such, inadequate parenting may be a risk factor for onset of multiple problems. It is possible that parenting constructs that are more disturbing or intrusive in nature may relate more strongly to both problem clusters, such as harsh punishment and psychological control (Keiley et al. 2000; Rather et al. 2011, Stone et al. 2013b).
The present study is not without limitations. First, although our study was longitudinal, it included two time-points. With more assessment waves it is possible to examine whether internalizing and externalizing problems are related to each other over a longer course in childhood and adolescence. Also, this would enable more fine-grained analyses, such as the identification of trajectories of internalizing and externalizing problems or latent growth curves (Nagin 1999; Willett and Sayer 1994). It is possible that the observed relations between internalizing and externalizing problems differ dependent on its specific trajectory. For example, reciprocal influences of externalizing on internalizing problems may be stronger in children following an increasing internalizing and externalizing trajectory. In order to fully understand how and why internalizing and externalizing problems are related, it should also be investigated whether these relations hold when including common risk factors. Future studies should include three or more time points, enabling them to apply sensitive statistical techniques, such as growth curve modeling in order to test developmental change and to test several developmental paths (e.g., linear, quadratic). Second, although our study was comprehensive in its inclusion of risk factors, it is definitely not exhaustive. Inclusion of ontogenic factors, such as temperament or child personality, attachment and self-esteem would provide us with better understanding of developmental mechanisms of child psychopathology (Cichetti and Toth 1998; De Pauw and Mervielde 2010). In addition, we call for the need to include constructs that are theorized to relate specifically to internalizing problems, such as psychological control, as this remains an understudied area in childhood (Rubin and Mills 1991; Stone et al. 2013b). Third, because the mother is used as informant for all but one variable, some of the relations between child behavior and mother characteristics like maternal mental health, parenting stress and parenting style, may actually be a reflection of distress of the mother influencing her report of the child’s behavior than the actual child behavior, i.e., shared rater bias. For example, when parents experience mental health problems, they may feel more easily burdened by daily hassles and parenting tasks, as a result of which they may be more likely to report their child’s behavior as problematic. There are several studies revealing that maternal anxiety is related to higher child anxiety as reported by the mother compared to reports of the child itself (Frick et al. 1994; Manassis et al. 2009). Furthermore, there are also studies showing that parental stress is related to informant discrepancies between child and parents on both internalizing and externalizing behavior (De Los Reyes and Kazdin 2005).
Despite these limitations, the current study adds to literature by showing that both a directional model and third variables model may explain the interrelatedness between parent-reported internalizing and externalizing problems in young children. The interrelatedness between internalizing and externalizing problems seems to depend on severity of these problems, and researchers should do well to distinguish between onset and stability of both problem clusters in order to disentangle how internalizing and externalizing are related and what role is played by third variables.
Second, results from this study may have potential implications for intervention and prevention. There are numerous depression prevention programs for children and adolescents (Stice et al. 2009). To our best knowledge, none of these programs target co-morbid externalizing problems. This study suggests that externalizing problems are a maintaining factor in internalizing problems, even when controlling for various risk factors. Therefore, it may be important for future studies examining depression prevention and intervention programs, to include a group wherein co-morbid externalizing problems are targeted in addition to the regular prevention program, and a group wherein the regular prevention program is conducted. Also, if replicated, our results point to targeting third variables not as maintaining factors in internalizing problems but rather as risk factors in the onset of these problems. Therefore, in intervention programs, inadequate parenting, parenting stress and social preference should not be targeted as maintaining factors, though maternal mental health could be treated as a maintaining factor. This advice is in line with RCT’s which did not find an additive effect of focusing on parental guidance in treatment of internalizing problems (Bodden et al. 2008; Nauta et al. 2003). Moving to prevention strategies, inadequate parenting, parenting stress and maternal mental health could be targeted as risk factors for developing internalizing problems. Again, these findings are in line with studies on selective prevention which show that targeting children of parents with psychological problems can help to decrease and prevent internalizing problems in children (Horowitz et al. 2007).
Notes
We conducted multi-group modeling to check whether child age or sex moderated our results. We found no moderation effects. Details are available upon request at the first author.
References
Achenbach, T. M., Howell, C. T., Quay, H. C., & Conners, C. K. (1991). National survey of problems and competencies among four- to sixteen-year-olds: Parents’ reports for normative and clinical samples. Monographs of the Society for Research in Child Development, 56, 1–131.
Angold, A., Costello, E. J., & Erkanli, A. (1999). Comorbidity. Journal of Child Psychology and Psychiatry, 40, 57–87.
Arnold, D. S., O’Leary, S. G., Wolff, L. S., & Acker, M. M. (1993). The parenting scale: A measure of dysfunctional parenting in discipline situations. Psychological Assessment, 5, 137–144.
Asparouhav, T., & Muthén, B. (2010). Weighted least squares estimation with missing data. http://www.statmodel.com/download/GstrucMissingRevision.pdf
Barry, T. D., Dunlap, S. T., Cotten, S. J., Lochman, J. E., & Wells, K. C. (2005). The influence of maternal stress and distress on disruptive behavior problems in boys. Journal of the American Academy of Child and Adolescent Psychiatry, 44, 265–273.
Beardslee, W. R., Versage, E. M., & Gladstone, T. R. G. (1998). Children of affectively ill parents: A review of the past 10 years. Journal of the American Academy of Child and Adolescent Psychiatry, 37, 1134–1141.
Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107, 238–246.
Bentler, P. M., & Bonett, D. G. (1980). Significance tests and goodness of fit in the analysis of covariance structures. Psychological Bulletin, 88(3), 588–606.
Benzies, K. M., Harrison, M. J., & Magill-Evans, J. (2004). Parenting stress, marital quality, and child behavior problems at age 7 years. Public Health Nursing, 21, 111–121.
Bittner, A., Egger, H. L., Erkanli, A., Costello, J. E., Foley, D. L., & Angold, A. (2007). What do childhood anxiety disorders predict? Journal of Child Psychology and Psychiatry, 48, 1174–1183.
Bodden, D. H., Bögels, S. M., Nauta, M. H., De Haan, E., Ringrose, J., Appelboom, C., & Appelboom-Geerts, K. C. (2008). Child versus family cognitive-behavioral therapy in clinically anxious youth: An efficacy and partial effectiveness study. Journal of the American Academy of Child and Adolescent Psychiatry, 47(12), 1384–1394.
Bornstein, M. H., Hahn, C.-S., & Haynes, O. M. (2010). Social competence, externalizing, and internalizing behavioral adjustment from early childhood through early adolescence: Developmental cascades. Development and Psychopathology, 22, 717–735.
Boylan, K., Vaillancourt, T., Boyle, M., & Szatmari, P. (2007). Comorbidity of internalizing disorders in children with oppositional defiant disorder. European Child and Adolescent Psychiatry, 16, 484–494.
Boylan, K., Vaillancourt, T., & Szatmari, P. (2012). Linking oppositional behaviour trajectories to the development of depressive symptoms in childhood. Child Psychiatry and Human Development, 43, 484–497.
Bronfenbrenner, U., & Evans, G. W. (2000). Developmental science in the 21st century: Emerging theoretical models, research designs, and empirical findings. Social Development, 9, 115–125.
Browne, M. W., & Cudeck, R. (1992). Alternative ways of assessing model fit. Sociological Methods & Research, 21(2), 230–258.
Burke, J. D., Loeber, R., Lahey, B. B., & Rathouz, P. (2005). Developmental transitions among affective and behavioral disorders in adolescent boys. Journal of Child Psychology and Psychiatry, 46, 1200–1210.
Burt, K. B., & Roisman, G. I. (2010). Competence and psychopathology: Cascade effects in the NICHD Study of Early Child Care and Youth Development. Development and Psychopathology, 22, 557–567.
Cicchetti, D., & Toth, S. L. (1998). The development of depression in children and adolescents. American Psychologist, 53, 221–241.
Coie, J. D., Dodge, K. A., & Coppotelli, H. (1982). Dimensions and types of social status: A cross-age perspective. Developmental Psychology, 18, 557–570.
Copeland, W. E., Shanahan, L., Costello, E. J., & Angold, A. (2009). Childhood and adolescent psychiatric disorders as predictors of young adult disorders. Archives of General Psychiatry, 66, 764–772.
Crnic, K. A., & Greenberg, M. T. (1990). Minor parenting stresses with young children. Child Development, 61, 1628–1637.
De Los Reyes, A., & Kazdin, A. E. (2005). Informant discrepancies in the assessment of childhood psychopathology: A critical review, theoretical framework, and recommendations for further study. Psychological Bulletin, 131, 483–509.
De Pauw, S. S. W., & Mervielde, I. (2010). Temperament, personality and developmental psychopathology: A review based on the conceptual dimensions underlying childhood traits. Child Psychiatry and Human Development, 41, 313–329.
Deater-Deckard, K. (2004). Parenting stress. New Haven, CT: Yale University Press.
Dishion, T. J., & Patterson, G. R. (2006). The development and ecology of antisocial behavior in children and adolescents. In D. J. Cohen & D. Cicchetti (Eds.), Developmental psychopathology. Vol. 3: Risk, disorder, and adaptation (pp. 503–541). Hoboken, NJ: Wiley.
Fanti, K. A., & Henrich, C. C. (2010). Trajectories of pure and co-occurring internalizing and externalizing problems from age 2 to age 12: Findings from the National Institute of Child Health and Human Development Study of Early Child Care. Developmental Psychology, 46, 1159–1175.
Fergusson, D. M., Lynskey, M. T., & Horwood, L. J. (1996). Origins of comorbidity between conduct and affective disorders. Journal of the American Academy of Child and Adolescent Psychiatry, 35, 451–460.
Ford, T., Collishaw, S., Meltzer, H., & Goodman, R. (2007). A prospective study of childhood psychopathology: Independent predictors of change over three years. Social Psychiatry and Psychiatric Epidemiology, 42, 953–961.
Frick, P. J., Silverthorn, P., & Evans, C. (1994). Assessment of childhood anxiety using structured interviews: Patterns of agreement among informants and association with maternal anxiety. Psychological Assessment, 6, 372–379.
Gilliom, M., & Shaw, D. S. (2004). Codevelopment of externalizing and internalizing problems in early childhood. Development and Psychopathology, 16, 313–333.
Gjone, H., & Stevenson, J. (1997). The association between internalizing and externalizing behavior in childhood and early adolescence: Genetic or environmental common influences? Journal of Abnormal Child Psychology, 25, 277–286.
Glaser, K. (1967). Masked depression in children and adolescents. American Journal of Psychotherapy, 21, 565–574.
Goodman, R. (2001). Psychometric properties of the Strengths and Difficulties Questionnaire. Journal of the American Academy of Child and Adolescent Psychiatry, 40, 1337–1345.
Gooren, E. M. J. C., van Lier, P. A. C., Stegge, H., Terwogt, M. M., & Koot, H. M. (2011). The development of conduct problems and depressive symptoms in early elementary school children: The role of peer rejection. Journal of clinical and adolescent psychology, 40, 245–253.
Granic, I. (2012). Don’t worry, be angry: Anxiety, aggression and repair in parent–child relationships. Unpublished inaugural speech, Radboud University Nijmegen, The Netherlands.
Gross, H. E., Shaw, D. S., & Moilanen, K. L. (2008). Reciprocal associations between boys’ externalizing problems and mothers’ depressive symptoms. Journal of Abnormal Psychology, 36, 693–709.
Hammen, C. (2006). Stress generation in depression: Reflections on origins, research, and future directions. Journal of Clinical Psychology, 62, 1065–1082.
Hardy, G. E., Shapiro, D. A., Haynes, C. E., & Rick, J. K. (1999). Validation of the General Health Questionnaire using a sample of employees from the Health Care Services. Psychological Assessment, 11, 159–165.
Hoglund, W. L., & Leadbeater, B. J. (2004). The effects of family, school, and classroom ecologies on changes in children’s social competence and emotional and behavioral problems in first grade. Developmental Psychology, 40, 533–544.
Horowitz, J. L., Garber, J., Ciesla, J. A., Young, J. F., & Mufson, L. (2007). Prevention of depressive symptoms in adolescents: A randomized trial of cognitive-behavioral and interpersonal prevention programs. Journal of Consulting and Clinical Psychology, 75(5), 693.
Ialongo, N., Edelsohn, G., Werthamer-Larsson, L., Crockett, L., & Kellman, S. (1996). The course of aggression in first-grade children with and without comorbid anxious symptoms. Journal of Abnormal Child Psychology, 24, 445–456.
Jöreskog, K. G. (1971). Statistical analysis of sets of congeneric tests. Psychometrika, 36, 109–133.
Keiley, M. K., Bates, J. E., Dodge, K. A., & Pettit, G. S. (2000). A cross-domain growth analysis: Externalizing and internalizing behaviors during 8 years of childhood. Journal of Abnormal Child Psychology, 28, 161–179.
Kessler, R. C., Petukhova, M., & Zaslavsky, A. M. (2011). The role of latent internalizing and externalizing predisposition in accounting for the development of comorbidity among common mental disorders. Current Opinion in Psychiatry, 24, 307–312.
Koeter, M. W. J., & Ormel, J. (1991). General Health Questionnaire, Dutch version manual. Swets and Zeitlinger, Lisse
Krueger, R. F., & Markon, K. E. (2006). Reinterpreting comorbidity: A model-based approach to understanding and classifying psychopathology. Annual Review of Clinical Psychology, 2, 111–133.
Lahey, B. B., Loeber, R., Burke, J., Rathouz, P. J., & McBurnett, K. (2002). Waxing and waning in concert: Dynamic comorbidity of conduct disorder with other disruptive and emotional problems over 7 years among clinic-referred boys. Journal of Abnormal Psychology, 111, 556–567.
Laird, R. D., Jordan, K., Dodge, K. A., Pettit, G. S., & Bates, J. E. (2001). Peer rejection in childhood, involvement with antisocial peers in early adolescence, and the development of externalizing problems. Development and Psychopathology, 13, 337–354.
Last, C. G., Perrin, S., Hersen, M., & Kazdin, A. E. (1996). A prospective study of childhood anxiety disorders. Journal of the American Academy of Child and Adolescent Psychiatry, 35, 1502–1510.
Laursen, B. P., & Hoff, E. (2006). Person-centered and variable-centered approaches to longitudinal data. Merrill-Palmer Quarterly, 52, 377–389.
Lee, E. J., & Bukowski, W. M. (2012). Co-development of internalizing and externalizing problems behaviors: Causal direction and common vulnerability. Journal of Adolescence. doi:10.1016/j.adolescence.2011.10.008.
Lilienfeld, S. O. (2003). Comorbidity between and within childhood externalizing and internalizing disorders: Reflections and directions. Journal of Abnormal Child Psychology, 31, 285–291.
Loeber, R., & Keenan, K. (1994). Interaction between conduct disorder and its comorbid conditions: Effects of age and gender. Clinical Psychology Review, 14, 497–523.
Manassis, K., Tannock, R., & Monga, S. (2009). Anxious by maternal- versus self-report: Are they the same children? Journal of Canadian Academy of Child and Adolescent Psychiatry, 18, 103–109.
Mathiesen, K. S., Sanson, A., Stoolmiller, M., & Karevold, E. (2009). The nature and predictors of undercontrolled and internalizing problem trajectories across early childhood. Journal of Abnormal Child Psychology, 37, 209–222.
McDonald, R. P. (1978). Generalizability in factorable domains: “Domain validity and generalizability”. Educational and Psychological Measurement, 38, 75–79.
McDonald, R. P. (1999). Test theory: A unified treatment. Mahwah, NJ: Lawrence Erlbaum.
Mesman, J., Bongers, I. L., & Koot, H. M. (2001). Preschool developmental pathways to preadolescent internalizing and externalizing problems. Journal of Child Psychology and Psychiatry, 42, 679–690.
Muthén, L. K., & Muthén, B. O. (1998–2007). Mplus user’s guide (5th ed.). Los Angeles, CA: Muthén and Muthén.
Nagin, D. (1999). Analyzing developmental trajectories: A semi-parametric, group-based approach. Psychological Methods, 4, 139–157.
Nauta, M. H., Scholing, A., Emmelkamp, P. M., & Minderaa, R. B. (2003). Cognitive-behavioral therapy for children with anxiety disorders in a clinical setting: No additional effect of a cognitive parent training. Journal of the American Academy of Child and Adolescent Psychiatry, 42(11), 1270–1278.
O’Connor, T. C., McGuire, S., Reiss, D., Hetherington, E. M., & Plomin, R. (1998). Co-occurrence of depressive symptoms and antisocial behavior in adolescence: A common genetic liability. Journal of Abnormal Psychology, 107, 27–38.
Oland, A. J., & Shaw, D. S. (2005). Pure versus co-occurring externalizing and internalizing symptoms in children: The potential role of socio-developmental milestones. Clinical Child and Family Psychology Review, 8, 247–270.
Otten, R., Wanner, B., Vitaro, F., & Engels, R. C. (2009). Disruptiveness, peer experiences and adolescent smoking: A long-term longitudinal approach. Addiction, 104, 641–650.
Panak, W. F., & Garber, J. (1992). Role of aggression, rejection, and attributions in the prediction of depression in children. Development and Psychopathology, 4, 145–165.
Patterson, G. R., & Capaldi, D. M. (1990). A mediational model for boys’ depressed mood. In J. E. Rolf & A. S. Masten (Eds.), Risk and protective factors in the development of psychopathology (pp. 141–163). New York: Cambridge University Press.
Pinderhughes, E. E., Dodge, K. A., Bates, J. A., Pettit, G. S., & Zelli, A. (2000). Discipline responses: Influence of parents’ socioeconomic status, ethnicity, beliefs about parenting, stress, and cognitive–emotional processes. Journal of Family Psychology, 14, 380–400.
Prinzie, P., Onghena, P., Hellinckx, W., Grietens, H., Ghesquiere, P., & Colpin, H. (2003). The additive and interactive effects of parenting and children’s personality on externalizing behaviour. European Journal of Personality, 17, 95–117.
Rathert, J., Fite, P. J., & Gaertner, A. E. (2011). Associations between effortful control, psychological control and proactive and reactive aggression. Child Psychiatry and Human Development, 42, 609–621.
Renk, K., Roberts, R., Roddenberry, A., Luick, M., Hillhouse, S., Meehan, C., et al. (2003). Mothers, fathers, gender role, and time parents spend with their children. Sex Roles, 48, 305–315.
Revelle, W., & Zinbarg, R. E. (2009). Coefficients alpha, beta, omega, and the GLB: Comments on Sijtsma. Psychometrika, 74, 145–154.
Rispens, J., Hermanns, J. M. A., & Meeus, W. H. J. (1996). Opvoeden in Nederland. Assen: van Gorcum.
Ritakallio, M., Koivisto, A., von der Pahlen, B., Pelkonen, M., Marttunen, M., & Kaltiala-Heino, R. (2008). Continuity, comorbidity and longitudinal associations between depression and antisocial behavior in middle adolescence: a 2-year prospective follow-up study. Journal of Adolescence, 31, 355–370.
Rodriguez, C. (2011). Association between independent reports of maternal parenting stress and children’s internalizing symptomatology. Journal of Child and Family Studies, 20, 631–639.
Rubin, K. H., & Mills, R. S. L. (1991). Conceptualizing developmental pathways to internalizing disorders in childhood. Canadian Journal of Behavioural Science, 23, 300–317.
Schermelleh-Engel, K., Moosbrugger, H., & Müller, H. (2003). Evaluating the fit of structural equation models: Test of significance and descriptive goodness-of-fit measures. Methods of Psychological Research, 8, 23–74.
Speltz, M., McClellan, J., DeKleyn, M., & Jones, K. (1999). Preschool boys with oppositional defiant disorder: Clinical presentation and diagnostic change. Journal of the American Academy of Child and Adolescent Psychiatry, 38, 838–845.
Stice, E., Shaw, H., Bohon, C., Marti, C. N., & Rohde, P. (2009). A meta-analytic review of depression prevention programs for children and adolescents: Factors that predict magnitude of intervention effects. Journal of Consulting and Clinical Psychology, 77, 486.
Stone, L. L., Otten, R., Engels, R. C. M. E., Vermulst, A. A., & Janssens, J. M. A. M. (2010). Psychometric properties of the parent and teacher versions of the Strengths and Difficulties Questionnaire for 4-to 12-year-olds: A review. Clinical Child and Family Psychology Review, 13, 254–274.
Stone, L. L., Otten, R., Ringlever, L., Hiemstra, M., Engels, R. C. M. E., Vermulst, A. A., & Janssens, J. M. A. M. (2013a). The parent version of the Strengths and Difficulties Questionnaire: Omega as an alternative to alpha and a test for measurement invariance. European Journal of Psychological Assessment, 29, 44–50.
Stone, L. L., Otten, R., Soenens, B., Kuntsche, E., & Engels, R. C. M. E. (2013b). Does parental psychological control relate to internalizing problems in early childhood? An examination using the Berkeley puppet interview. International Journal of Behavioral Development, 37, 309–318.
Van Lier, P., & Koot, H. M. (2010). Developmental cascades of peer relations and symptoms of externalizing and internalizing problems from kindergarten to fourth-grade elementary school. Development and Psychopathology, 22, 569–582.
van Widenfelt, B. M., Goedhart, A. W., Treffers, P. D. A., & Goodman, R. (2003). Dutch version of the Strengths and Difficulties Questionnaire (SDQ). European Child and Adolescent Psychiatry, 12, 281–289.
Vitaro, F., Brendgen, M., & Tremblay, R. (2000). Influence of deviant friends on delinquency: Searching for moderator variables. Journal of Abnormal Child Psychology, 28, 313–325.
Weiss, B., Süsser, K., & Catron, T. (1998). Common and specific features of childhood psychopathology. Journal of Abnormal Psychology, 107, 118–127.
Willett, J. B., & Sayer, A. G. (1994). Using covariance structure analysis to detect correlates and predictors of individual change over time. Psychological Bulletin, 116, 363–381.
Acknowledgments
This research was granted by the Dutch Organization for Health Research and Care Innovation (ZonMW: 80-82435-98-8026).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Stone, L.L., Otten, R., Engels, R.C.M.E. et al. Relations Between Internalizing and Externalizing Problems in Early Childhood. Child Youth Care Forum 44, 635–653 (2015). https://doi.org/10.1007/s10566-014-9296-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10566-014-9296-4