
Abstract
Purpose
Chronically elevated catecholamine levels activate cardiac β-adrenergic receptors, which play a vital role in the pathogenesis of heart failure. Evidence suggests that vasostatin-1 (VS-1) exerts anti-adrenergic effects on isolated and perfused hearts in vitro. Whether VS-1 ameliorates hypertrophy/remodeling by inducing the chronic activation of β-adrenergic receptors is unknown. The present study aims to test the efficacy of using VS-1 to treat the advanced hypertrophy/remodeling that result from chronic β-adrenergic receptor activation and to determine the cellular and molecular mechanisms that underlie this response.
Methods and Result
Rats were subjected to infusion with either isoprenaline (ISO, 5 mg/kg/d), ISO plus VS-1 (30 mg/kg/d) or placebo for 2 weeks. VS-1 suppressed chamber dilation, myocyte hypertrophy and fibrosis and improved in vivo heart function in the rats subjected to ISO infusion. VS-1 increased phosphorylated nitric oxide synthase levels and induced the activation of protein kinase G. VS-1 also deactivated multiple hypertrophy signaling pathways that were triggered by the chronic activation of β-adrenergic receptors, such as the phosphoinositide-3 kinase (PI3K)/Akt and Ca2+/calmodulin-dependent kinase (CaMK-II) pathways. Myocytes isolated from ISO + VS-1 hearts displayed higher Ca2+ transients, shorter Ca2+ decays, higher sarcoplasmic reticulum Ca2+ levels and higher L-type Ca2+ current densities than the ISO rat hearts. VS-1 treatment restored the protein expression of sarcoplasmic reticulum Ca2+ uptake ATPase, phospholamban and Cav1.2, indicating improved calcium handling.
Conclusions
Chronic VS-1 treatment inhibited the progression of hypertrophy, fibrosis, and chamber remodeling, and improved cardiac function in a rat model of ISO infusion. In addition, Ca2+ handling and its molecular modulation were also improved by VS-1. The beneficial effects of VS-1 on cardiac remodeling may be mediated by the enhanced activation of the eNOS-cGMP-PKG pathway.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronically elevated catecholamine (CA) levels have long been known harm the heart [1–3]. The heart initially develops cardiac hypertrophy when exposed to prolonged and excessive adrenergic stress [4, 5]. If left uncontrolled, this hypertrophy will develop into heart failure. To ensure sufficient cardiac output, the sympathetic nervous system (SNS) and renin-angiotensin-aldosterone system (RAAS) are activated and sustained [6]. A growing amount of evidence indicates that the sustained activation of the SNS and the associated excess activation of adrenergic signaling pathways by CAs, have adverse prognostic effects and accelerate progress toward heart failure [7]. These findings are of substantial clinical significance, and they provide theoretical support that anti-adrenergic therapies, including the use of β-adrenergic-blockers, remain the most effective drug treatments for heart failure.
Chromogranin A (CgA) is a major soluble protein that is co-stored in and co-released with CAs from secretory vesicles located in adrenal medulla chromaffin cells [8]. CgA gives rise to several bioactive peptides via a post-translational proteolytic processing mechanism. One of these peptides, vasostatin, is a novel cardiac modulator and a stabilizer of adrenergic tone, which contributes to cardio-circulatory homeostasis. Evidence has indicated that the N-terminal regions of human recombinant CGA1–78 (hr-CGA1–78, vasostatin-1, VS-1) and hrCGA1–113 (vasostatin-2, VS-2) exert cardiodepressive and anti-adrenergic effects on isolated and perfused hearts in eel, frog and rat [9–11]. VS-1 and VS-2 inhibit myocardial contractility (negative inotropism) and relaxation (negative lusitropism) in a concentration-dependent manner under both basal and adrenergically stimulated conditions. Studies have demonstrated that the anti-adrenergic effect that is induced by VS-1 is caused by the Ca2+-independent, PI3K-dependent endothelial release of NO and not on a direct interaction with cardiac cells. In addition, VS-1 also exerts a protective effect in ischemic hearts via an adenosine/nitric oxide signaling mechanism [12]. Four N-terminal CGA-derived peptides (CGA(4–113), CGA(1–124), CGA(1–135), and CGA(1–199)) that contain the vasostatin sequence have been characterized in rat hearts [13]. This strongly suggests that these fragments play roles in the autocrine/paracrine regulation of cardiac function. However, most studies have focused on the transient, anti-adrenergic effects of vasostatin on perfused hearts. Whether vasostatin protects the heart against chronic β-ARs overstimulation in vivo remains unknown.
In the present study, we tested the effects of VS-1 treatment in hearts subjected to chronic β-ARs activation. We show that VS-1 suppressed chamber, cellular, and molecular remodeling and improved cardiac function in the treated hearts. In addition, Ca2+ cycling and its molecular regulation were improved. A molecular signaling pathway analysis indicated that the beneficial effects of VS-1 on cardiac remodeling may be mediated via the enhanced activation of the eNOS-cGMP-PKG pathway.
Materials and Methods
Animal Models
All experimental procedures were performed according to the Guide for the Care and Use of Laboratory Animals that was published by the US National Institutes of Health (NIH Publication #85–23, revised 1996), and the protocol was approved by the Animal Care and use Committee of Renmin Hospital of Wuhan University, China.
Male Sprague-Dawley rats (Experimental Animal Center of the Medical College of Wuhan University) weighing 250–300 g each were randomly divided into three groups: a control group in which the rats received a volume of 0.9 % saline; an ISO group in which the rats received ISO (Sigma) alone (5 mg/kg/d, intraperitoneally [ip]); and an ISO + VS-1 (synthetized by Wuhan Moon Biosciences Co. Ltd., China) group in which the rats received ISO (5 mg/kg/d, ip) and VS-1 (30 mg/kg/d, ip). Drugs and saline were administered for 2 weeks (1/3 total doses every 8 h). VS-1 treatment was initiated 30 min prior to ISO administration. The human recombinant Ser-Thr-Ala CGA 1–78 (VS-1) peptide was produced and characterized as previously described [14].
Physiological Studies
We performed two-dimensional, guided M-mode echocardiography in anesthetized rats. Measurements were acquired using a sequoia C256 (Siemens) with a 15-MHz linear-array transducer. Intact heart hemodynamic analyses were performed as previously described [15]. A catheter was inserted into the right carotid artery and then advanced into the left ventricle (LV) to record LV systolic pressure and LV end-diastolic pressure (Biopac systems, Inc. MP150).
Histology
Hearts were fixed in 10 % formalin overnight, embedded in paraffin, sectioned to a thickness of 5 μm and stained with hematoxylin/eosin or Masson’s trichrome. Myocyte diameters and interstitial collagen fractions were determined using a digital image analysis (Adobe Photoshop 7.0, NIH image J), with the observer blinded to the tissue source. In four different hearts from each group, five separate fields were analyzed (a total of 50–70 cells per heart).
Quantitative PCR
mRNA expression was analyzed using real-time quantitative PCR as previously described [16]. Total RNA was extracted from cells, and 0.2 μg of RNA was analyzed. The following PCR primers were used in this study: rat atrial natriuretic peptide (ANP), 5′-GGGCTTCTTCCTCTTCCTG-3′ and 3′-CTGAGACGGGTTGACTTCC-5′; rat brain natriuretic peptide (BNP), 5′-CTCAAAGGACCAAGGCCCTACAA-3′ and 3′-AAACAACCTCAGCCCGTCACAG-5′; and rat β-myosin heavy chain (MHC), 5′-CAGTATGAGGAGGAGACAGAG-3′ and 3′-AGGAACACTTGGCATTGACAGC-5′. To adjust for equal loading, the results were normalized to the levels of glyceraldehyde-3phosphate dehydrogenase (GAPDH), which was amplified using the following primers: 5′-ACAGCAACAGGGTGGTGGAC-3′ and 3′-TTTGAGGGTGCAGCGAACTT-5′.
Western Blot Analysis
Protein was prepared from snap-frozen heart tissue as previously described [17]. Protein extracts were run on 4–12 % Bis-Tris NuPage gels, blotted onto nitrocellulose membranes, and probed using the following primary antibodies: eNOS, Ser1179-phospho-eNOS, PI3K, P-PI3K, Akt, Ser-473-phospho-Akt (Cell Signaling Technology), PKG, CaMK-II, Thr-286-phospho-CaMK-II, SERCA2a, PLB, p-PLB (phospho S16 + T17) and Cav1.2 (Abcam). The primary antibodies were visualized using horseradish peroxidase-conjugated secondary antibodies and enhanced using chemiluminescence (Pierce). Total protein levels (eNOS, PI3K, Akt, and CaMK-II) were assessed after stripping the same membranes and using them to detect phospho-proteins. The blots were quantified using NIH Image J software, and the ratios of phosphorylated/total protein levels were calculated and normalized to the control group results.
Myocyte Isolation
Rat ventricular myocytes were isolated as previously described [18]. Briefly, hearts were quickly excised and perfused at 37 °C on a Langendorff’s apparatus. After 5 min of perfusion with Ca2+-free Tyrode’s solution (NaCl, 130 mM; KCl, 5.4 mM; CaCl2, 1.8 mM; MgCl2, 2 mM; Na2HPO4, 0.3 mM; Hepes, 10 mM; and glucose, 10 mM; pH, 7.40 ± 0.05), the perfusate was switched to Tyrode’s solution containing type II collagen enzyme (Sigma) to digest connective tissues. After 15 min of digestion, single ventricular myocytes were isolated from dissected and triturated ventricles and stabilized in BSA containing Tyrode’s solution.
Systolic Ca2+ Transients and SR Ca2+ Content
Cardiomyocytes were incubated with Fluo-4 AM (10 μmol/L, Molecular Probes) for 25 min at room temperature. After the cells were stained, the cardiomyocytes were superfused for 25 min to allow the fluorescent dye to wash out and then de-esterified. The Fluo-4 was excited with the 460–480 nm line of an argon laser, and emission was collected at 500–550 nm (Leica Microsystems, Germany). Systolic Ca2+ transients were recorded under steady-state conditions and constant field stimulation (at 0.5, 1, or 2 HZ; 20 V). To assess SR Ca2+ content, we measured the amplitude of caffeine-induced Ca2+ transients. Two seconds after the stimulation was stopped under steady-state conditions, caffeine (10 μmol/L) was directly applied onto the cell, which led to immediate and complete SR Ca2+ release. The recorded Ca2+ transients were analyzed using Leica Microsystems software.
Measurement of ICa,L
Membrane currents were obtained and analyzed using an EPC-9 patch clamp amplifier (HEKA Electronik, Lambrecht, Germany). Single cardiac ventricular myocytes were placed in the experimental chamber and perfused with external solution (Tyrode’s solution) for 5 min at 2–3 ml/min. The measurements were acquired at RT. Glass microelectrodes were made using two-stage pulling with a resistance of 3.0–5.0 MΩ and filled with internal solution (120 mM CsCl, 1.0 mM CaCl2, 5.0 mM MgCl2, 5.0 mM Na2ATP, 11 mM EGTA, 10 mM HEPES and 11 mM glucose; adjusted to pH 7.2 with CsOH). The mean capacitance of the cells was 102.64 ± 32.68 pF, and the series resistances were <25 MΩ. ICa,L was recorded using a whole-cell patch clamp configuration.
Statistical Analysis
SPSS 19.0 for windows (SPSS Inc., Chicago, Illinois) was used for the statistical analyses. The data are presented as the mean ± S.E.M. Differences between groups were assessed using one-way analysis of variance followed by Tukey’s multiple comparisons test. When within-group variance differed substantially, a non-parametric Kruskal-Wallis test and Bonferroni correction was used.
Results
VS-1 Inhibits Hypertrophy, Remodeling and Fibrosis and Improves Cardiac Function
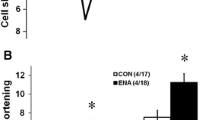
Chronic activation of β-ARs induced heart chamber dilation (LVESD: +26.17 %; LVEDD: +28.3 %; Fig. 1a) with reduced fractional shortening (−31.5 %; Fig. 1a). Both the chamber remodeling and the reduced FS were inhibited by treatment with VS-1 (Fig. 1a). VS-1 blocked 8.5 % of the increase in the HW/BW ratio that was observed in the ISO-infused rats (Fig. 1a). Chronic β-ARs activation also induced myocardial fibrosis and myocyte hypertrophy, and both were suppressed by VS-1 (by 46 % and 28 %, respectively; Fig. 1c).

Chronic VS-1 treatment suppresses progressive cardiac dilation, dysfunction, fibrosis and hypertrophy and improves cardiac systolic and diastolic function in hearts subjected to sustained β-ARs activation. a Representative echocardiographic data in CTL and ISO rats treated with or without VS-1; FS (%), LVEDD, LVESD, and PWT were analyzed using echocardiography, and HW/BW were measured in three groups (mean ± S.E.M.; n = 7). *, P < 0.001 versus the CTL group; #, P < 0.001 versus the ISO group; and §, P < 0.01 versus the ISO group. VS-1, vasostatin-1; AR, adrenergic receptor; CTL, control; ISO, isoprenaline; FS, fractional shortening; LVEDD, left ventricular end-diastole diameter; LVESD, left ventricular end-systole diameter; PWT, posterior-wall thickness; and HW/BW, heart weight/body weight. b In vivo cardiac systole function (dP/dtmax) and diastole function (dP/dtmn). *, P < 0.001 versus the CTL group; and #, P < 0.001 versus the ISO group. dP/dtmax, peak rate of pressure rise; and dP/dtmn, peak rate of pressure decline. c HE- and Masson’s-stained myocardium showing reduced interstitial fibrosis and myocyte hypertrophy following treatment with VS-1 (n = 5 for each). *, P < 0.001 versus the CTL group; #, P < 0.001 versus the ISO group. HE, hematoxylin and eosin
Figure 1b shows the results of our in vivo tests of cardiac function. Rats with sustained β-AR activation showed reduced contractility (dP/dtmax) and relaxation (dP/dtmn). Treatment with VS-1 increased contractility by 26 % and relaxation by 27 % (Fig. 1b).
Treatment with VS-1 Enhances eNOS-cGMP-PKG Pathway Activity and Blocks Fetal Gene Expression and PI3K/Akt Pathway Activity
The expression and activity of eNOS were suppressed in rat hearts that were subjected to chronic β-ARs activation (Fig. 3a). The activity of PKG-1α, a downstream effector of eNOS, was also inhibited by β-ARs activation (Fig. 3a). In hearts subjected to ISO infusion, treatment with VS-1 had no impact on the total expression level of eNOS (P = 0.717, Fig. 3a). However, VS-1 significantly increased the level of phosphorylated eNOS. In addition, chronic treatment with VS-1 restored a lower level of PKG-1α protein expression (Fig. 3a). These data suggest that treatment with VS-1 enhances eNOS-PKG pathway activity and suppresses the ISO infusion-induced re-expression of fetal genes, including ANP, BNP and β-MHC (Fig. 2).

Treatment with VS-1 prevents fetal gene re-expression. The expression levels of fetal ANP (a), BNP (b), and β-MHC (c) mRNAs were normalized to the level of GAPDH mRNA expression in whole heart isolates (n = 5 for each group). *, P < 0.001 versus the control group; #, P < 0.001 versus the ISO group; and &, P < 0.01 versus the ISO group. ANP, atrial natriuretic peptide; BNP, brain natriuretic peptide; MHC, myosin heavy chain
PI3K/Akt is a prominent signaling cascade that is stimulated by chronic β-AR activation. The hyperactivation of this pathway is associated with cardiac hypertrophy and remodeling. ISO infusion increased PI3K/Akt activity, as shown by the increased ratio of phosphorylated to total PI3K/AKT protein levels (Fig. 3b). VS-1 suppressed this response to nearly baseline levels (Fig. 3b).

Chronic VS-1 treatment enhances the activation of the eNOS-PKG pathway and prevents the expression of the hypertrophy signaling pathway. a Western blot analysis of eNOS and PKG-1α protein expression. The expression levels were normalized to GAPDH expression in whole heart isolates (n = 5 for each). *, P < 0.05 versus the control group; #, P < 0.05 versus the ISO group; eNOS,endothelial nitric oxide synthase; and PKG, protein kinase G. b Western blot analysis of PI3K/Akt protein expression (n = 5 for each). The PI3K/Akt summary results are shown as the ratio of phosphorylated (p) to total (t) protein. *, P < 0.01 versus the control group; §, P < 0.001 versus the ISO group; #, P < 0.01 versus the ISO group; and ★, P < 0.05 versus the ISO group. PI3K, phosphatidylinositol 3-kinase
VS-1 Improves Ca2+ Release and SR Ca2+ Content
To investigate the mechanism underlying Ca2+ handling, we isolated cardiomyocytes from animals in each of the three groups and measured epifluorescence (Fig. 4a). The cardiomyocytes were stimulated at 0.5, 1, 2 and 3 HZ, and systolic Ca2+ transients were recorded (Fig. 4b). When cells were stimulated at 0.5 HZ, the amplitudes of the systolic Ca2+ transients were 42 % lower in the ISO group than in the CTL group (47 % lower at 1 HZ, 49 % lower at 2 HZ and 49 % lower at 3 HZ; Fig. 3b). In addition, in response to 0.5 HZ stimulation, Ca2+ transient half-time decay was 32 % higher in the ISO group (Fig. 4c). Treatment with VS-1 alleviated the depressions in the amplitudes of systolic Ca2+ transients that were caused by stimulation with β-ARs (+30 % at 0.5 HZ, +33 % at 1 HZ, +40 % at 2 HZ, and +45 % at 3 HZ; Fig. 4c) and decreased the prolonged half-time decays of Ca2+ transients by 15 % when cells were stimulated at 0.5 HZ (Fig. 4c).

Chronic VS-1 treatment in hearts subjected to β-ARs activation improves isolated cardiomyocyte calcium handling. a Representative images of fluorescence ratios visualized with an intensity-defined pseudocolor gradient in three groups. b Example fluo-4 Ca2+ transients (∆F/F0) in response to 0.5 HZ electrical field stimulation in cardiomyocytes from three groups. c Summary data of Ca2+ transient amplitude and Ca2+ transient half-time of decay in response to o.5 HZ stimulation. Statistics of Ca2+ transient amplitude stimulation at 0.5, 1, 2 and 3 HZ (n ≥ 23 for each). *, P < 0.001 versus the control group; and #, P < 0.001 versus the ISO group. d Example traces of Ca2+ transients induced in response to the application of 10 mM caffeine. e Summary data for SR Ca2+ contents and release fractions (n ≥ 23 for each group). *, P < 0.001 versus the control; §, P < 0.001 versus the ISO group; and # P < 0.01 versus the ISO group. SR, sarcoplasmic-endoplasmic reticulum
Caffeine was applied to quantify SR Ca2+ content (Fig. 4d). We detected lower SR Ca2+ content in the ISO group, and 57 % lower caffeine-induced Ca2+ transients were detected in the ISO group than in the CTL group (Fig. 4e). In addition, the SR Ca2+ release fraction was also reduced by 24 % in the ISO group (Fig. 4e). Treatment with VS-1 resulted in 50 % higher SR Ca2+ content and increased the release fraction by 23 % (Fig. 4e).
VS-1 Reduces CaMK-II Pathway Activity and Restores Ca2+-Handling Proteins
As [Ca2+]i was elevated, CaMK-II, a factor that plays a vital role in cardiac remodeling, was chronically activated. We detected the expression levels and activity of CaMK-II in the present study. We found that both were increased in rat hearts that were subjected to β-ARs activation (Fig. 5a). In the ISO group, this enhanced level of activity in the CaMK-II pathway was suppressed by treatment with VS-1 (Fig. 5a).

In β-AR-stimulated hearts, chronic VS-1 treatment reduces CaMK-II expression and activity and restores calcium handling. a Western blot analysis of total CaMK-II and phosphorylated CaMK-II levels, with summary quantification (n = 5 each). *, P < 0.001 versus the control group; #, P < 0.001 versus the ISO group; and CaMK-II, Ca2+ and calmodulin-dependent protein kinase II. b SERCA2a, PLB, and Cav1.2 protein expression (western blot, left and summary data, right; n = 5 for each). *, P < 0.001 versus the control group; #, P < 0.001 versus the ISO group; &, P < 0.01 versus the ISO group; SERCA2a, sarcoplasmic-endoplasmic reticulum Ca2+ ATPase; and PLB, phospholamban
Because Ca2+ cycling was improved in VS-1 treated hearts, we examined the effects on sarcoplasmic reticulum handling proteins that could have been modified by the therapy. SERCA2a expression was 45 % lower after 3 weeks of ISO infusion (Fig. 5b). Levels of PLB, which combines with SERCA2a to induce an inhibitory effect on SERCA2a, were 107 % higher in the ISO group than in the CTL group (Fig. 5b). In addition, treatment with VS-1 decreased t-PLB and increased p-PLB expression, resulting in a higher p/t:PLB ratio (which reflects Ca2+ uptake) than was observed in the placebo-treated ISO group (Fig. 5b).
VS-1 Increases ICa,L and the Expression of Cav1.2
Figure 6a shows voltage-dependent ICa,L traces that were recorded in the CTL and ISO rats with or without VS-1 treatment. Peak ICa,L amplitudes were normalized by cell membrane capacitance and expressed as the peak ICa,L densities. Chronic β-ARs activation resulted in 41 % lower peak ICa,L densities (Fig. 6b) and 44 % lower Cav1.2 expression (Fig. 5b) than were observed in the CTL group. Treatment with VS-1 increased peak ICa,L densities by 1.3-fold (Fig. 6b) and Cav1.2 expression by 1.3-fold (Fig. 5b) over the results observed in the placebo-treated group.

Chronic VS-1 treatment prevents the β-ARs activation-induced suppression of ICa,L densities. a Examples of ICa,L recorded in the control, ISO and ISO + VS-1 groups. b Current-voltage (I-V) correlations for ICa,L and quantitative analysis of peak ICa,L densities in the three groups (n = 8 each). *, P < 0.001 versus the control group; and #, P < 0.05 versus the ISO group
Discussion
Chronically elevated CA levels result in the activation of cardiac β- ARs, which may play a major role in the pathogenesis of heart failure. Impaired myocardial structure and contractility have been observed in animals in which β-ARs are overactivated [19, 20]. Previous studies have suggested that VS-1 exerts an anti-adrenergic effect in isolated and perfused hearts. In the present study, we first showed that VS-1 played a protective role in rat hearts that were subjected to chronical β-ARs activation. Briefly, VS-1 suppressed chamber dilation, myocyte hypertrophy and fibrosis and improved in vivo heart functions in rats that were subjected to ISO infusion. Treatment with VS-1 increased phosphorylated nitric oxide synthase levels and activated protein kinase G. VS-1 also deactivated multiple hypertrophy signaling pathways that are normally triggered by chronic β-ARs activation, such as the PI3K/Akt [21] and CaMK-II pathways [22]. Ca2+ handling and its molecular modulation were also improved by treatment with VS-1.
The heart is viewed as an endocrine organ because a growing number of studies have demonstrated that cardiac cells possess the ability to synthesize and release many hormones, such as CAs [23] and natriuretic peptides (NPs) [24], which can function to regulate cardiovascular homeostasis under both normal and disease conditions [25]. The identification of Chromogranin-A (CgA) [26] and its derivative peptides [13] in the heart contribute to the notion that the heart is an endocrine organ. Among these peptides, VS-1 is one of the most well-studied, and it has been shown to be a novel cardiac modulator and stabilizer of adrenergic tone in cardio-circulatory homeostasis. It is worth noting that acute administration of VS-1 has been shown to have cardio-inhibitory effects under β-ARs stimulation conditions in previous studies. However, in the present study, chronic administration of VS-1 improved functions in hearts that were subjected to chronic β-ARs stimulation. The apparent paradox between the negative effects of acute exposure and positive effects of chronic exposure on contractility responses has some similarities with the effects of β-blockers. Acute administration of β-blockers is negatively inotropic, whereas chronic blockade in a stressed heart enhances contraction, likely by suppressing sustained catecholamine cytotoxicity [27].
Anti-Hypertrophy Is Effected via the eNOS-NO- PKG Pathway
Previous studies have shown that VS-1 exerts cardio-inhibitory effects via the eNOS-NO-PKG pathway under both basal and β-ARs stimulation conditions [9–11]. Similar to the results of previous studies, we found that VS-1 increased the levels of phosphorylated nitric oxide synthase and induced the activation of protein kinase G. Evidence suggests that eNOS-derived NO acts by elevating PKG and thereby exerts beneficial effects on cardiac remodeling. For example, mice that globally lack eNOS (eNOS−/−) develop greater cardiac hypertrophy and fibrosis and show more deterioration in cardiac functions following thoracic aorta coarctation (TAC) [28, 29]. Conversely, mice with cardiac-specific over-expression of eNOS showed improved left ventricular performance and reduced compensatory hypertrophy after myocardial infarction [30]. Thus, we hypothesized that the beneficial effects of VS-1 on cardiac remodeling are mediated by the enhancement of the eNOS-NO-PKG pathway.
Because no classical surface receptors of VS-1 have been documented, the cellular processes that lie upstream of the activation of eNOS by this peptide are not fully understood. Previous studies have shown that in endothelial cells, VS-1 acts as a cell-penetrating peptide by utilizing its cationic and amphipathic properties, binds to heparin sulfate proteoglycans (HSPGs) [31], and then activates eNOS phosphorylation (Ser1179) through a PI3K/Akt-dependent, endocytosis-coupled mechanism [10, 32].
In the present study, VS-1 suppressed the expression and activity of PI3K/Akt. These results appear to contradict the results of previous studies [8, 29], which have suggested that VS-1 does not act directly on cardiomyocytes but rather on endothelia cells. The increased expression and activity of PI3K/Akt reflected the acute effect of VS-1 on endothelia cells [10, 31, 32] that has been observed in previous studies. However, in our study, the samples contained various cell types but were mainly composed of myocardial cells. Consequently, the depressed expression and activity of PI3K/Akt that were observed in the present study reflected a chronic and indirect effect of VS-1 on myocardium and not its effect on endothelial cells. In addition, a growing amount of evidence suggests that sustained activation of the PI3K/Akt pathway is associated with the development of pathological cardiac hypertrophy [33–35]. Furthermore, chronic activation of the PI3K/Akt pathway is associated with TAC-inducing pressure-overload and was prevented by the phosphodiesterase-5 A (PDE5) inhibitor sildenafil, which increased cGMP synthesis [17, 36]. Consequently, we hypothesized that VS-1 suppressed the activation of PI3K/Akt that was stimulated by chronic ISO infusion, possibly by enhancing the eNOS-cGMP-PKG pathway and thereby exerting protective effects on the myocardium.
VS-1 Improves Ca2+ Handling and its Molecular Regulation
Calcium cycling in cardiomyocytes is crucial to both cardiac contraction and relaxation. Defective intracellular Ca2+ homeostasis is a central cause of contractile dysfunction and arrhythmias in failing myocardium and can result from pathological alterations in the expression and activity of structural proteins, ion channels, and enzymes. A growing amount of evidence suggests that the reduced expression and activity of SERCA2a and an increase in the inhibitory activity of PLB impairs uptake by the sarcoplasmic-endoplasmic reticulum (SR) in both animal models and human heart failure [37–39]. Defects in cytosolic Ca2+ removal result in increased diastolic [Ca]2+ i levels, and reduced SR Ca2+ content and systolic [Ca] 2+ i transients. In addition, elevated diastolic [Ca]2+ i causes a sustained activation of CaMK-II, which in turn causes additional damages to calcium cycling. In the present study, we found that chronic administration of VS-1 improved Ca2+ pump activity after ISO infusion by repairing SERCA2a expression and alleviating the increased inhibitory activity of PLB. Furthermore, the depressed systolic [Ca]2+ i transients and reduced SR Ca2+ content that were caused by ISO infusion were also significantly improved by treatment with VS-1. Finally, we found that VS-1 prevented the reduction of ICa,L that was caused by ISO administration, which might improve Ca2+ transients in cardiomyocytes.
cGMP-PKG-Dependent Modulation of the CaMK-II Pathway
Consistent with the results of previous studies [40], in the present study, we found that both the activity and expression of CaMK-II were increased by chronic stimulation with β-ARs. A growing amount of evidence suggests that CaMK-II regulates not only immediate cellular functions but also chronic processes, such as ventricular remodeling, that can lead to heart failure [41–43]. As shown in our study, the activity and expression of CaMK-II that were induced by chronic β-ARs stimulation were substantially suppressed by treatment with VS-1.
The inhibitory role of VS-1 on CaMK-II might be mediated by the enhancement of the eNOS-cGMP-PKG pathway. NO/cGMP have a substantial impact on intracellular calcium homeostasis. On the one hand, NO/cGMP strongly inhibit L-type Ca2+ channels [44, 45], which alleviates the intracellular calcium overload that is caused by the chronic infusion of ISO. On the other hand, evidence suggests that the cGMP-dependent pathway has an inhibitory effect on Na+/H+ exchange (NHE) [46–48]. NHE activity can, when [Na+]i is elevated, operate in reverse to extrude Na+ in exchange for the inflow of Ca2+, thereby leading to elevated [Ca2+]i. VS-1 increased the activity of the cGMP pathway and deactivated the CaMK-II pathway by decreasing the level of [Ca2+]i. Previous studies have come to similar conclusions. For example, sildenafil, which inhibits the cGMP-specific phosphodiesterase 5 A to increase [cGMP]i, inhibited the pressure overload-induced activity and expression of CaMK-II [49]. Further evidence supporting the notion that cGMP signals attenuate CaMK-II activation comes from pGC−/− mice, in which the observed hypertrophic phenotype was associated with the upregulation of CaMK-II expression, the increased autophosphosphorylation of CaMK-II and the phosphorylation of downstream targets of CaMK-II [50, 51].
Clinical Implications
Heart failure is a global problem with an estimated prevalence of 38 million patients. This number is increasing with the aging of the population. Despite the fact that some progress has been made in this field, the prognosis for heart failure is worse than that for most cancers. A growing amount of evidence suggests that chronic neurohumoral activation plays a vital role in the progression of heart failure. Strategies aimed at blocking neurohumoral activation exert cardio-protective effects to improve cardiac function. Previous studies have shown that VS-1 exerts anti-adrenergic effects in isolated and perfused hearts. In the present study, we showed that chronic administration of VS-1 stopped chamber, cellular, and molecular remodeling and improved calcium handling in rat hearts that were subjected to chronic β-ARs activation. These studies collectively suggest that VS-1 has the potential to become a new therapeutic drug for heart failure.
Conclusion
Chronic VS-1 treatment suppressed chamber dilation, myocyte hypertrophy and fibrosis and improved in vivo heart function in rats that were subjected to ISO infusion. Ca2+ cycling and its molecular modulation were also improved by VS-1. The beneficial effects of VS-1 on cardiac remodeling are dependent on the eNOS-cGMP-PKG pathway.
References
Samuels MA. The brain-heart connection. Circulation. 2007;116:77–84.
Goldspink DF, Burniston JG, Ellison GM, Clark WA, Tan LB. Catecholamine-induced apoptosis and necrosis in cardiac and skeletal myocytes of the rat in vivo: the same or separate death pathways? Exp Physiol. 2004;89:407–16.
Chien KR, Knowlton KU, Zhu H, Chien S. Regulation of cardiac gene expression during myocardial growth and hypertrophy: molecular studies of an adaptive physiologic response. FASEB J. 1991;5:3037–46.
Kitagawa, Y, Yamashita, D, Ito, H and Takaki, M. Reversible effects of isoproterenol-induced hypertrophy on in situ left vetricular function in rat hearts. Am J Physiol Heart Circ Physiol 2004;287:H277-HH85.
Zhang GX, Kimura S, Nishiyama A, Shokoji T, Rahman M, Yao L, et al. Cardiac oxidative stress in acute and chronic isoproterenol-infused rats. Cardiovasc Res. 2005;65:230–8.
Cohn JN, Levine TB, Olivari MT, Gaberg V, Lura D, Francis GS, et al. Plasma norepinephrine as a guide to prognosis in patients with chronic congestive heart failure. N Engl J Med. 1984;311:819–23.
Esler M, Kaye D, Lambert G, Esler D, Jennings G. Adrenergic nervous system in heart failure. Am J Cardiol. 1997;80:7 L–14 L.
Mahapatra NR. Catestatin is a novel endogenous peptide that regulates cardiac function and blood pressure. Cardiovasc Res. 2008;80:330–8.
Corti A, Mannarino C, Mazza R, Angelone T, Longhi R, Tota B, Chromogranin AN. Terminal fragments vasostatin-1 and the synthetic CGA 7-57 peptide act as cardiostatins on the isolated working frog heart. Gen Comp Endocrinol. 2004;136:217–24.
Gallo MP, Levi R, Ramella R, Brero A, Boero O, Tota B, et al. Endothelium-derived nitric oxide mediates the antiadrenergic effect of human vasostatin-1 in rat ventricular myocardium. Am J Physiol Heart Circ Physiol. 2007;292:2906–12.
Cerra MC, De Iuri L, Angelone T, Corti A, Tota B, Recombinant N. Terminal fragments of chromogranin-a modulate cardiac function of the Langendorff-perfused rat heart. Basic Res Cardiol. 2006;101:43–52.
Cappello S, Angelone T, Tota B, Pagliaro P, Penna C, Rastaldo R, et al. Human recombinant chromogranin A-derived vasostatin-1 mimics preconditioning via an adenosine/nitric oxide signaling mechanism. Am J Physiol Heart Circ Physiol. 2007;293:719–27.
Glattard E, Angelone T, Strub JM, Corti A, Aunis D, Tota B, et al. Characterization of natural vasostatin-containing peptides in rat heart. FEBS J. 2006;273:3311–21.
Corti A, Perez Sanchez L, Gasparri A, Curnis F, Longhi R, Branaazza A, et al. Production and structure characterization of recombinant chromograin a N-terminal fragment (vasostatin. Eur J Biochem. 1997;248:692–9.
Huang CX, Yuan MJ, Huang H, Wu G, Liu Y, SB Y, et al. Ghrelin inhibits post-infarct myocardial remodeling and improves cardiac function through anti-inflammation effect. Peptides. 2009;30:2286–91.
Yamamoto K, Dang QN, Kennedy SP, Osathanondh R, Kelly RA, Lee RT. Induction of tenascin-C in cardiac myocytes by mechanical deformation. J Biol Chem. 1999;274:21840–6.
Takinmoto E, Champion HC, Li M, Belardi D, Ren S, Rodriguez ER, et al. Chronic inhibition of cyclic GMP phosphodiesterase 5 A prevents and reverses cardiac hypertrophy. Nat Med. 2005;11:214–22.
Liu B, Ho HT, Velez-Cortes F, Lou Q, Valdivia CR, Knollmann BC, et al. Genetic ablation of ryanodine receptor 2 phosphorylation at Ser-2808 aggravates Ca(2+)-dependent cardiomyopathy by exacerbating diastolic Ca2+ release. J Physiol. 2014;592:1957–73.
Soltysinska E, Olesen SP, Osadchii OE. Myocardial structural, contractile, and electrophysiological changes in the Guinea-pig heart failure model induced by chronic sympathetic activation. Exp Physiol. 2011;96:647–63.
Osadchii OE. Cardiac hypertrophy induced by sustained beta-adrenoreceptor activation: pathophysiological aspects. Heart Fail Rev. 2007;12:66–86.
Naohiro Yano VI, Ting C. Zhao, Andy Tseng, James F. Padbury, and Yi-tang Tseng. A novel signaling pathway for beta-adrenergic receptor-mediated activation of phosphoinositide 3-kinase in H9c2 cardiomyocytes. Am J Physiol Heart Circ Physiol. 2007;293:H385–H93.
Grimm M, Brown JH. Beta-adrenergic receptor signaling in the heart: role of CaMKII. J Mol Cell Cardiol. 2010;48:322–30.
Lincoln T, Potter TC, Vallee L. Willman, David E. Wolfe. Synthesis, binding, release, and metabolism of norepinephrine in normal and transplanted dog hearts. Circ Res. 1965;16:468–81.
Bold AJd. Atrial natriuretic factor: A hormone produced by the heart. Science. 1985;230:767–70.
Tota B, Angelone T, Mazza R, Cerra M. The chromogranin A-derived vasostatins new players in the endocrine heart. Curr Med Chem. 2008;15:1444–51.
Pieroni, M, Corti, A, Tota, B, Curnis, F, Angelone, T, Colombo, B, Cerra, MC, Bellocci, F, Crea, F and Maseri, A. Myocardial production of chromogranin a in human heart a new regulator of cardiac function. Eur Heart J 2007;28:1117–1127.
Brodde OE. Beta-adrenoceptor blocker treatment and the cardiac beta-adrenoceptor-G-protein(s)-adenylyl cyclase system in chronic heart failure. Naunyn Schmiedeberg's Arch Pharmacol. 2007;374:361–72.
Buys ES, Raher MJ, Blake SL, Neilan TG, Graveline AR, Passeri JJ, et al. Cardiomyocyte-restricted restoration of nitric oxide synthase 3 attenuates left ventricular remodeling after chronic pressure overload. Am J Physiol Heart Circ Physiol. 2007;293:H620–H7.
Ichinose F, Bloch KD, JC W, Hataishi R, Aretz HT, Picard MH, et al. Pressure overload-induced LV hypertrophy and dysfunction in mice are exacerbated by congenital NOS3 deficiency. Am J Physiol Heart Circ Physiol. 2004;286:H1070–H5.
Janssens S, Pokreisz P, Schoonjans L, Pellens M, Vermeersch P, Tjwa M, et al. Cardiomyocyte-specific overexpression of nitric oxide synthase 3 improves left ventricular performance and reduces compensatory hypertrophy after myocardial infarction. Circ Res. 2004;94:1256–62.
Ramella R, Boero O, Alloatti G, Angelone T, Levi R, Gallo MP. Vasostatin 1 activates eNOS in endothelial cells through a proteoglycan-dependent mechanism. J Cell Biochem. 2010;110:70–9.
Cerra MC, Gallo MP, Angelone T, Quintieri AM, Pulera E, Filice E, et al. The homologous rat chromogranin A1-64 (rCGA1-64) modulates myocardial and coronary function in rat heart to counteract adrenergic stimulation indirectly via endothelium-derived nitric oxide. FASEB J. 2008;22:3992–4004.
Morisco C, Zebrowski D, Condorelli G, Tsichlis P, Vatner SF, Sadoshima J. The Akt-glycogen synthase kinase 3beta pathway regulates transcription of atrial natriuretic factor induced by beta-adrenergic receptor stimulation in cardiac myocytes. J Biol Chem. 2000;275:14466–75.
Condorelli G, Drusco A, Stassi G, Bellacosa A, Roncarati R, Iaccarino G, et al. Akt induces enhanced myocardial contractility and cell size in vivo in transgenic mice. Proc Natl Acad Sci U S A. 2002;99:12333–8.
Matsui T, Li L, JC W, Cook SA, Nagoshi T, Picard MH, et al. Phenotypic spectrum caused by transgenic overexpression of activated Akt in the heart. J Biol Chem. 2002;277:22896–901.
Hsu S, Nagayama T, Koitabashi N, Zhang M, Zhou L, Bedja D, et al. Phosphodiesterase 5 inhibition blocks pressure overload-induced cardiac hypertrophy independent of the calcineurin pathway. Cardiovasc Res. 2009;81:301–9.
Hasenfuss G, Reinecke H, Studer R, Meyer M, Pieske B, Holtz J, et al. Relation between myocardial function and expression of sarcoplasmic reticulum Ca2 + −ATPase in failing and nonfailing human myocardium. Circ Res. 1994;75:434–42.
Nicolaou P, Kranias EG. Role of PP1 in the regulation of Ca cycling in cardiac physiology and pathophysiology. Front Biosci. 2009;14:3571–85.
Schwinger RHG, Munch G, Bolck B, Karczewski P, Krause E-G, Erdmann E. Reduced Ca2 + −sensitivity of SERCA2a in failing human myocardium due to reduced serin-16 phospholamban phoshorylation. J Mol Cell Cardiol. 1999;31:479–91.
Chu G, Lester JW, Young KB, Luo W, Zhai J, Kranias EGA. Single site (Ser16) phosphorylation in phospholamban is sufficient in mediating its maximal cardiac responses to β-agonists. J Biol Chem. 2000;275:38938–43.
Bers D. Calcium cycling and signaling in cardiac myocytes. Annu Rev Physiol. 2008;70:23–49.
Ling H, Zhang T, Pereira L, Means CK, Cheng H, Gu Y, et al. Requirement for Ca2+/calmodulin-dependent kinase II in the transition from pressure overload-induced cardiac hypertrophy to heart failure in mice. J Clin Invest. 2009;119:1230–40.
Heineke J, Molkentin JD. Regulation of cardiac hypertrophy by intracellular signalling pathways. Nat Rev Mol Cell Biol. 2006;7:589–600.
Jiang LH, Gawler DJ, Hodson N, Milligan CJ, Pearson HA, Porter V, et al. Regulation of cloned cardiac L-type calcium channels by cGMP-dependent protein kinase. J Biol Chem. 2000;275:6135–43.
Schroder F, Single L. Type Ca2+ channel regulation by cGMP-dependent protein kinase type I in adult cardiomyocytes from PKG I transgenic mice. Cardiovasc Res. 2003;60:268–77.
Yeves AM, Garciarena CD, Nolly MB, Chiappe de Cingolani GE, Cingolani HE, Ennis IL. Decreased activity of the Na+/H+ exchanger by phosphodiesterase 5 A inhibition is attributed to an increase in protein phosphatase activity. Hypertension. 2010;56:690–5.
Kilic A, Velic A, De Windt LJ, Fabritz L, Voss M, Mitko D, et al. Enhanced activity of the myocardial Na+/H+ exchanger NHE-1 contributes to cardiac remodeling in atrial natriuretic peptide receptor-deficient mice. Circulation. 2005;112:2307–17.
Perez NG, Piaggio MR, Ennis IL, Garciarena CD, Morales C, Escudero EM, et al. Phosphodiesterase 5 A inhibition induces Na+/H+ exchanger blockade and protection against myocardial infarction. Hypertension. 2007;49:1095–103.
Nagayama T, Hsu S, Zhang M, Koitabashi N, Bedja D, Gabrielson KL, et al. Sildenafil stops progressive chamber, cellular, and molecular remodeling and improves calcium handling and function in hearts with pre-existing advanced hypertrophy caused by pressure overload. J Am Coll Cardiol. 2009;53:207–15.
Klaiber M, Kruse M, Völker K, Schröter J, Feil R, Freichel M, et al. Novel insights into the mechanisms mediating the local antihypertrophic effects of cardiac atrial natriuretic peptide: role of cGMP-dependent protein kinase and RGS2. Basic Res Cardiol. 2010;105:583–95.
Kilic A, Bubikat A, Gassner B, Baba HA, Kuhn M. Local actions of atrial natriuretic peptide counteract angiotensin II stimulated cardiac remodeling. Endocrinology. 2007;148:4162–9.
Acknowledgments
This work was supported by the Natural Science Foundation of Hubei Province, China (no. 2013CFA117) the Fundamental Research Funds for the Central Universities of China (no. 302274052), and Project of Wuhan Municipal Science and Technology (no.2014060101010033). The authors are grateful to the Wuhan University School of Basic Medical Science Medical Research Center for Structural biology for assisting in the performance of the experiments to test Ca2+ transients.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None
Additional information
Dandan Wang and Yinguang Shan contributed equally to this work.
Rights and permissions
About this article

Cite this article
Wang, D., Shan, Y., Huang, Y. et al. Vasostatin-1 Stops Structural Remodeling and Improves Calcium Handling via the eNOS-NO-PKG Pathway in Rat Hearts Subjected to Chronic β-Adrenergic Receptor Activation. Cardiovasc Drugs Ther 30, 455–464 (2016). https://doi.org/10.1007/s10557-016-6687-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10557-016-6687-9