
Abstract
Background
Animal studies showed that the use of metformin after myocardial infarction (MI) resulted in a protective effect on cardiac myocytes. In this study, we examined the effect of metformin in patients with diabetes mellitus (DM) on left ventricular ejection fraction (LVEF) and post-MI mortality.
Methods
We reviewed charts of patients with MI admitted to the UAMS medical center. Baseline characteristics and 12-month follow up data were collected. Patients were classified into three groups: Control group- no DM (n = 464), Metformin group- DM + MI (n = 88) and No-Metformin group- DM + MI (n = 168). First, we compared Metformin and No-Metformin groups to the Control group. Second, we performed propensity-score matching in patients with DM, and compared Metformin to No-Metformin groups.
Results
All-cause 30-day and 12-month mortality was significantly higher in the No-Metformin group compared to controls (13.5 vs 9.3 % p = 0.03 at 30 days, 23.7 vs 15.9 % p = 0.03 at 12 months). However, all-cause 30-day and 12-month mortality were similar in the Controls and Metformin group (9.3 vs 6.8 % p = 0.93 at 30 days, 15.9 vs 11.4 % p = 0.97 at 12 months). Mean LVEF on presentation (45 % in the three groups) and at follow up (47.84, 46.38 and 43.62 % in Control, Metformin, and No-Metformin groups, respectively) were not statistically different. There were no significant differences in regard to re-hospitalization, re-intervention, new stroke, CHF development, new MI, or identifiable arrhythmias. Metformin was an independent predictor of lower 30-day and 12-month all-cause mortality in patients with DM (HR 0.25, p = 0.02 and HR 0.32, p = 0.01, respectively). In the matched analysis, 30-day all-cause mortality was significantly higher in the No-Metformin compared to the Metformin group (21.1 vs 8.8 %, p = 0.05). However the difference in 12-month all-cause mortality did not reach statistical significance (24.6 vs 15.8 %, p = 0.15).
Conclusion
This proof-of-concept study shows that use of metformin in patients with DM is associated with lower 30-day all-cause mortality and tendency for a lower 12-month all-cause mortality following MI without discernible improvement in LVEF.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Coronary heart disease (CHD) continues to be the leading cause of mortality in the United States [1] with acute myocardial infarction (AMI) being the major and most dramatic presentation. If patients survive the initial insult, they are still at risk of developing left ventricular (LV) dysfunction [2]. Diabetes mellitus (DM) is strongly correlated with the development of CHD and its complications. Mortality in this population is predominately due to events such as AMI, cerebrovascular accidents and sudden death [3]. Multiple studies have demonstrated that effective glycemic control is associated with improved cardiovascular profile [4–6].
Metformin is a relatively inexpensive drug with a good safety profile that has been in use for the last 60 years. Metformin has shown prowess as the medication of choice for glycemic control in high-cardiovascular risk populations [3, 7, 8]. It is the only oral hypoglycemic agent that has been shown to reduce cardiovascular events and improve survival in patients with diabetes and significant cardiovascular risk factors [9–11]. The improvement in all-cause mortality correlates with improved LV function reported in animal models of heart failure following coronary occlusion or sustained hypertension [12–14]. Only one published study so far has demonstrated a beneficial effect of metformin on LV diastolic function as evident by improved isovolumetric LV relaxation times and longitudinal tissue velocities measured by tissue Doppler imaging in patients with DM [15]. It has been proposed that metformin may even be useful in patients without DM suffering from AMI by improving LV function. However, a recent study failed to show any benefit of chronic metformin therapy in patients without DM who underwent primary percutaneous coronary angioplasty (PCI) for ST segment elevation MI (STEMI) [16].
We designed this study to evaluate the effect of metformin use on LV ejection fraction (LVEF) and mortality in patients with AMI as compared to therapy with drugs other than metformin. We included a large number of patients with AMI but without DM as controls.
Methods
Study Population
Using data from University of Arkansas for Medical Sciences (UAMS) electronic medical records system, we identified patients who were admitted to the hospital between January 1, 2007 and December 31, 2011 with a primary diagnosis of AMI and those who developed AMI during admission. Each chart was reviewed by at least one of the authors, and the following information was collected: demographic data (age, sex, and race), past medical history [including prior CHD, heart failure with reduced ejection fraction (HFrEF, defined as history of LVEF less than 50 %), hypertension, cerebrovascular accident (CVA), DM and non-skin cancer], current smoker status, medications used on admission or at discharge, therapy [PCI, coronary artery bypass grafting (CABG), or medical therapy only], LVEF, blood sugar levels and creatinine at presentation, and presence of renal function impairment (defined as GFR less than 60 mL/min/1.73 m2)]. Follow-up information was collected for the 12 months following the index admission. Duration of follow up was based on the last physician note in each chart; if it was more than 1 year then follow up duration was considered 12 months. Follow-up data included first recurrent intervention, new AMI, new CVA, first re-hospitalization, arrhythmia (atrial fibrillation/flutter, ventricular tachycardia/fibrillation), development of heart failure (HF), and follow up LVEF. All-cause mortality was based on whether the patient was reported as deceased in his medical chart over the 12-month follow up period. The study was approved by the Institutional Review Board.
Acute Myocardial Infarction and Treatment
AMI was defined as: chest pain, shortness of breath, or other angina-equivalent symptoms in association with electrocardiographic (ECG) changes consistent with STEMI or non-STEMI (NSTEMI) in the setting of troponin-I elevation greater than 0.5 ng/mL within 24 h of onset of symptoms. STEMI was defined as ST-segment elevation of more than 1 mm in two contiguous leads or new left bundle branch block. NSTEMI was defined as dynamic T wave changes (flattening or inversion) and/or ST segment depression of more than 1 mm. Treatment regimens were classified as follows: medical therapy only, coronary intervention- PCI or CABG. The medical therapy group included patients who did not have any intervention or those who underwent diagnostic coronary angiography with no subsequent coronary intervention. The PCI group included patients who underwent balloon angioplasty and/or stent placement. The CABG group underwent coronary artery bypass grafting.
LVEF on Presentation and Follow-up
LVEF was obtained from echocardiogram, nuclear stress imaging, or LV angiogram reports at presentation and follow up. If LVEF was given in a range, the lower number of the range was used. For follow-up evaluation, LVEF was based on the first study reported after discharge from the index admission in the following 12 months.
Statistical Analysis
Patients were classified into three groups based on diabetes mellitus status and metformin use: first group included patients with no underlying diagnoses of diabetes and will be referred to as Control group. Second group included patients with diabetes mellitus that had metformin listed in their admission or discharge notes in the index admission and will be referred to as Metformin group. The last group included patients with diabetes mellitus and no reported use of metformin in index admission and will be referred to as No-Metformin group. Primary outcomes were LVEF on presentation and follow up, 30-day and 12-month all-cause mortality. Secondary outcomes were recurrent AMI, first re-hospitalization, coronary re-intervention, new CVA, arrhythmia and development of HF. A 12-month composite event rate was composed of 12-month all-cause mortality, new AMI, new arrhythmia and new stroke.
Descriptive statistics of patients’ baseline characteristics are presented. Categorical variables are reported as counts and percentages, differences were assessed with Chi-square test. Continuous variables are presented as means with one standard deviation, differences were compared with two-sample Student’s t test. LVEF on presentation and follow up were compared between the three groups using Univariate analysis. Kaplan-Meier analysis or Multivariable Cox regression analysis were used to compare 30-day all-cause mortality, 12-month all-cause mortality and secondary outcomes between the groups.
Data were analyzed in two ways. First we looked at the overall cohort comparing the Metformin and No-Metformin groups to the Control group. Second, we only looked at patients with DM, comparing the Metformin group directly to the No-Metformin group. In this step we used propensity-scores to generate two equal-sized groups. Propensity-score was computed by a logistic regression model using the following variables; age, sex, race, history of CHD, HFrEF , prior peripheral vascular disease (PVD), prior CVA, history of hypertension, prior non-skin cancer, current smoker status, aspirin use, beta blockers use, statin use, angiotensin converting enzyme inhibitors/angiotensin receptor blockers (ACEI/ARB) use, insulin use, sulfonylureas use, glitazones use, admission creatinine level, admission blood sugar more than 200 mg/dl, type of AMI and treatment received. One to one propensity–score nearest neighbor matching without replacement was applied with a caliber of 0.2 to balance for baseline confounders. A two sided p-value of equal to or less than 0.05 was considered significant. Analysis was performed using SPSS software, version 21.
Results
Study Population
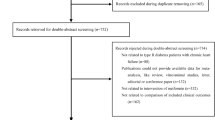
Based on the International Classification of Diseases (ICD-9) codes, we identified 1228 patients with AMI present in their hospitalization diagnoses list. On initial screening we excluded 423 patients who did not fulfill our criteria for AMI. Another 97 patients were excluded due to lack of LV function assessment in their index admission. The remaining 708 charts were manually reviewed and included in the study. Patients were divided into three groups based on diabetes status and metformin use during their index admission as mentioned above: Control group (no DM) (n = 464), Metformin group (with DM) (n = 88), and No-Metformin group (with DM) (n = 156). 82 % of the patients had complete 30-day follow up or died in the first month, and 69 % of the patients either had completed 12-month follow up or died.
In the Metformin group; average daily dose was 1220 mg; 10 patients were newly started on metformin. In the majority of the patients (88 %), metformin was held during the index admission but was restarted at discharge. Table 1 shows patients’ baseline characteristics. The Metformin group had generally similar cardiovascular profile compared to the controls, with the exception of higher incidence of hypertension and fewer current smokers. In addition, Metformin group had higher reported use of aspirin, statins and ACEI/ARB compared to controls. On the other hand, the No-Metformin group were somewhat older, had worse cardiovascular profile but few were current smokers, reported more aspirin, beta-blockers, statin and ACEI/ARB use, had worse kidney function and underwent less interventions compared to the controls. Insulin use was reported more in the No-Metformin group compared to the Metformin group.
Analysis of the Overall Cohort
Left Ventricular Function on Presentation and During Follow Up
Mean LVEF on presentation was around 45 % in the three groups. After controlling for demographics, co-morbidities and medication used, there were no significant differences in LVEF on presentation among the three groups. As expected, older age (p = 0.02), male-gender (p = 0.02), prior history of HFrEF (p < 0.01) and STEMI on presentation (p = 0.04) were associated with lower LVEF on presentation (Table 2a).
Follow up LVEF was available in 28 % of patients; in 128 patients in the Control group, 24 patients in the Metformin group, and 47 patients in the No-Metformin group. Mean follow-up duration for LVEF reassessment in the 3 groups was 4.5, 4.25 and 4.64 months, respectively (p = 0.89). Mean follow up LVEF was 47.84 % in the Control group, 46.38 % in Metformin group, and 43.62 % in No-Metformin group, however these differences were not significant. Nonetheless, male-gender (p = 0.01), history of HFrEF (<0.01) were associated with lower LVEF (Table 2b).
All-Cause Mortality
30-day all-cause mortality was 9.3 % in the Control group and 13.5 % in the No-Metformin group (HR 2.01, p = 0.03 vs. Control group). On the other hand, 30-day mortality was lower in the Metformin group (6.8 %) than that in the Control group but not significantly different (HR 0.96, p = 0.93).
Importantly, advancing age (HR 1.02 for each year increase, p = 0.03), higher admission creatinine (HR 1.15 per point increase, p = 0.01), history of non-skin cancer (HR 2.37, p = 0.009) and STEMI on presentation (HR 2.38, p = <0.01) were significantly associated with increased 30-day all-cause mortality. While, beta-blocker use (HR 0.32, p < 0.01), aspirin use (HR 0.39, p < 0.01), higher LVEF on presentation (HR 0.97 for each percent increase, p < 0.01), and PCI as treatment modality (HR 0.28, p < 0.01) all were associated with lower 30-day all-cause mortality regardless of the presence/absence of DM and or what therapy was used to treat DM (Table 3a).
12-month all-cause mortality was 15.9 % in Control group and 23.7 % in the No-metformin group (HR 1.63, p = 0.03 vs. Control group). However, 12-month all-cause mortality was not significantly different between Metformin group (11.4 %) and Control group (HR 0.97, p = 0.97).
Again, advancing age (HR 1.03 for each year increase, p < 0.01), non-skin cancer (HR 1.969, p < 0.01) and higher admission creatinine (HR 1.14 per point increase, p < 0.01) were associated with higher 12-month all-cause mortality. On the other hand, aspirin use (HR 0.46, p < 0.01), higher LVEF on presentation (HR 0.97 for each point increase, p < 0.01), treatment with PCI (HR 0.25, p < 0.01) and treatment with CABG (HR 0.09, p = 0.02) were associated with lower 12-month all-cause mortality regardless of the presence/absence of DM or what therapy was used to treat DM (Table 3b).
Secondary Outcomes
As shown in Table 4, there were no statistical differences between the three groups in regard to rate of re-hospitalization, repeat intervention, new stroke, development of HF or its exacerbation, new MI, identifiable arrhythmias or 12-month composite event rate (composed of 12-month all-cause mortality, new MI, new arrhythmia and new stroke over the 12-month follow up period) after adjusting for the same variables in Table 3.
Analysis of Patients with Diabetes Mellitus
Independent Predictors of Mortality
Table 5 shows independent predictors of mortality in patients with DM. Among different oral hypoglycemic agents and after adjusting for multiple variables (age, gender, race, CHD, PVD, history of CVA, hypertension, non-skin cancer, current smoker status, aspirin use, beta-blockers use, statin use, serum creatinine on presentation, type of AMI, treatment provided, LVEF on presentation and admission blood sugar), metformin use was the only one associated with lower 30-day all-cause mortality (HR 0.25, p = 0.02), and along with insulin use, was associated with lower 12-month all-cause mortality (HR 0.32 and 0.33, p = 0.01 and 0.02 respectively). Fig. 1 shows unadjusted Kaplan–Meier curves of 30-day and 12-Month all-cause mortality in the three groups.

Unadjusted Kaplan–Meier curves of 30-day and 12-Month all-cause mortality for each group. p-value calculated by log-rank test
Matching and Analysis of Primary and Secondary Outcomes
Propensity-score 1:1 matching was performed as described above. Two groups of 57 patients in Metformin and No-Metformin groups were generated. Average follow-up time in the matched Metformin and No-Metformin groups were 8.87 and 7.78 (p = 0.31) respectively. Table 6 shows patients’ baseline characteristics after matching.
Mean LVEF at presentation was not different between the two groups; 45.04 and 43.35 % in the Metformin and No-Metformin groups respectively (p = 0.52). Follow up LVEF was available in only 15 patients in of the Metformin group, and 14 patients in No-Metformin group. Mean LVEF at follow up was not also different between the matched two groups (p = 0.74).
Most importantly, 30-day all-cause mortality was significantly different between the Metformin and No-Metformin groups, 8.8 and 21.1 %, respectively (p = 0.05). Although, the 12-month all-cause mortality remained lower in the Metformin group compared to the No-Metformin group, 15.8 vs 24.6 % respectively, it did not reach statistical significance (p = 0.15), most likely a Type 2 error.
There were no significant differences between the two groups in regard to re-hospitalization, repeat intervention, new stroke, development of HF or its exacerbation, new MI, or identifiable arrhythmias over the 12-month follow up period. Although the 12-month composite event rate was lower in the Metformin group compared to No-Metformin group, 24.6 vs 33.3 % respectively, it was not statistically significant (p = 0.18), again most likely a Type 2 error. Figure 2 shows Kaplan–Meier curves of 30-day and 12-Month all-cause mortality and 12-month composite event rate for the matched two groups.

Kaplan–Meier curves of 30-day and 12-Month all-cause mortality and 12-month composite event rate (composed of 12-month all-cause mortality, new MI, new arrhythmia and new stroke) in patients with diabetes mellitus after matching. p-value calculated by log-rank test
Discussion
Metformin is a first-line oral agent for the treatment of patients with type II DM [11, 17, 18]. It is the only oral agent that has been shown to reduce cardiovascular mortality in patients with diabetes [9, 10, 19, 20]. Recent animal studies [12, 14, 21] have demonstrated a cardioprotective effect of metformin in non-diabetic rats subjected to coronary ligation. An observational human study suggested reduction in infarct size in patients with diabetes on metformin therapy undergoing PCI for STEMI [22]. All this information formed the basis of a recently reported study designed to look at the LVEF in non-diabetic patients with STEMI undergoing PCI treated with metformin [16]. No data on mortality, the most important end-point, was provided in either study.
Our study was designed to assess the effect of metformin therapy on LVEF and mortality following AMI. We observed that patients with diabetes not on metformin (No-Metformin group) had a significant 50 % increase in 30-day and 12-month all-cause mortality as compared with the Control group (without DM). On the other hand, patients with DM and treated with metformin (Metformin group) had 30-day and 12-month all-cause mortality comparable with the Control group. Metformin group patients also experienced a lower 30-day all-cause mortality and tendency for lower 12-month all-cause mortality when compared to patients with DM but not on metformin (No-Metformin group).
It may be assumed that the benefit of metformin in patients with AMI may be related to cardio-protection by this agent. However, we observed no significant differences in LVEF at presentation between the three groups of patients even after matching in the diabetic population. Further, we did not observe any significant differences in LVEF during follow-up. This suggests that the mortality benefit of metformin may be independent of improvement in LV function. It is also possible that echocardiography is not sensitive enough to detect subtle, but significant, tissue protective effect which may have a bearing on long-term mortality. The LVEF is the product of the initial injury to the heart which is highly dependent on atherosclerotic burden and the size of myocardium supplied by the affected vessels. Data on the effects of metformin on atherosclerotic burden are conflicting. Some studies have suggested reduction in carotid intima-media thickness, a surrogate marker for atherosclerosis, with metformin use [23, 24]. The more recent CAMERA trial did not provide evidence of such benefit [25].
Interpretation of data from follow up LVEF is severely limited as only 28 % of patients had reassessment of their LVEF in the 12-month follow up period. Nonetheless, our data on LVEF during follow-up are in agreement with the recently concluded prospective trial of metformin for STEMI in non-diabetic patients (GIPS-III), which also failed to show a salutary effect of this agent on LVEF [16]. It is noteworthy that the data from the GIPS-III trial have potential bias given that the patient population was limited to a lower risk group of patients without prior history of CHD or AMI. It is of note that Anderson et al. [15] showed improvement in LV relaxation pattern in diabetic patients on metformin as compared to non-metformin therapy. We did not have data on diastolic parameters in our study patients, but it is possible that an improvement in diastolic function may have contributed to some of the mortality benefit of metformin observed by us.
Not unexpectedly, both 30-day and 12-month all-cause mortality was significantly higher in No-Metformin group compared to the Control group. Further, both 30-day and 12-month all-cause mortality was comparable between Control group and Metformin group. In addition, metformin was the only oral hypoglycemic agent associated with lower all-cause mortality in patients with DM at 30 days. On the other hand, metformin and insulin therapy were associated with lower 12-month all-cause mortality.
In subgroup analysis of patients with diabetes, the Metformin group continued to show statistically significant lower 30-day all-cause mortality when compared to the No-Metformin group. Our findings are in concordance with the results of previously published studies that showed reduction in all-cause mortality with the use of metformin in patients with diabetes [3, 4, 26]. However, none of these studies assessed the benefit of metformin in patients with MI. Although there was no statistically significant difference in the rate of secondary outcomes when assessed individually, the metformin group had a clear tendency towards a lower composite event rate. One interesting finding was lower 12-month all-cause mortality with use of insulin in patients with DM. Data regarding insulin and mortality are conflicting. A recent retrospective study showed higher all-cause mortality with the use of exogenous insulin in patients with type 2 DM when compared to Metformin monotherapy [27]. On the other hand, in DIGAMI study, intensive insulin use in patients with MI was associated with reduction in long term mortality in patients with DM [28]. However, this finding was not reproduced in DIGAMI II study which also showed lower mortality with the use of metformin [29].
These observations collectively suggest a potent effect of metformin in terms of reduction in 30-day and 12-month all-cause mortality in patients with MI.
Based on animal work, it appears that metformin exerts its cardioprotective effect at the cellular level by affecting cardiac remodeling and preventing further oxidative injury to the cells [14, 30]. Rena et al. [17] reviewed the molecular mechanism of actions of metformin and suggested that metformin-induced activation of AMP-activated protein kinase may be important in enhanced expression of eNOS and PPARγ-coactivator-1α which are important regulators of mitochondrial biogenesis and function and play important role in the development of heart failure. This upregulated expression culminates in a multitude of effects including inhibition of protein synthesis, protection against free oxygen radicals, and reduction in DNA damage [31]. A recent study [32] found that metformin reduces genomic instability in diabetic rats, a phenomenon that may also play a role in the long-term cardioprotective effects of this drug.
Our study has several limitations. We examined a large population sample that received regular care at a tertiary care teaching hospital. We could not account for patients who were lost to follow up and may have received health care elsewhere. However, we think this would have affected all groups equally. We did not collect data regarding the methods used to assess LV function. We could not adjust for changes in medication usage, follow up visits, change in smoking status and family history of vascular disease between the groups which could potentially alter cardiovascular risk and mortality. We also did not differentiate between type 1 and type 2 DM, and did not have enough data regarding the duration of illness prior to the index admission. In addition we could not assess the duration of metformin use prior to the study or after the index admission and whether the patients in the No-metformin groups were started on metformin at some point following the index admission. We also recognize the presence of significance variation in group sizes and baseline characteristics which is inherent to this kind of retrospective study.
It is clear that patients with DM not using metformin had worse kidney function at baseline, and underwent less intervention compared to the other two groups and this, in part, can affect the increased mortality observed in this group. However, we adjusted for this variation in two ways; first, we included all the potential confounders in the statistical analysis module (Cox regression for time variables and Univariate analysis for continuous variables) when we analyzed the overall cohort. Second, we performed propensity score matching when we analyzed patients with DM. We did not have enough data on hemoglobin A1c values at the index admission and thus this measurement was not included in the analysis; however, we included the admission blood sugar values as a surrogate for diabetes control. Nonetheless, the possibility of other unknown confounders is still there, and any interpretation of the results should keep this in mind. Thus, we believe this study is a proof of concept that requires additional prospective studies to validate its findings. The initial inclusion criteria of the study was dependent on ICD-9 CM codes, which are subject to inherent bias. However, selection of patients based on ICD codes has been shown to be associated with 94 % sensitivity and 99 % specificity [33].
Even in a relatively small number of patients, we were able to observe that age, LVEF, presence of cancers or renal dysfunction, use of aspirin or beta-blockers, and coronary revascularization were significant predictors of outcome. The majority of patients in the metformin group were taken off the drug during index admission but were restarted at discharge, thus we believe that the data reported here actually likely reflects the long term effect of metformin.
Conclusion
The UK Prospective Diabetes Study (UKPDS) [19] demonstrated a major beneficial effect of metformin therapy on cardiovascular disease outcomes, with a 36 % relative risk reduction in all-cause mortality and a 39 % relative risk reduction in rates of AMI. The present study did not show any evidence of improvement in LVEF, yet there was an associated mortality benefit with metformin in patients with DM post-MI. This study in a relatively small number of patients should be considered a proof-of-concept of reduction in all-cause mortality with the use of metformin in patients with DM and MI.
References
Kochanek KD, Xu JQ, Murphy SL, Miniño AM, Kung HC. Deaths: final data for 2009. National vital statistics reports. 2011;60.
Jhund PS, McMurray JJ. Heart failure after acute myocardial infarction: a lost battle in the war on heart failure? Circulation. 2008;118(20):2019–21.
Roussel R, Travert F, Pasquet B, Wilson PW, Smith Jr SC, Goto S, et al. Metformin use and mortality among patients with diabetes and atherothrombosis. Arch Intern Med. 2010;170(21):1892–9.
UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet. 1998;352(9131):854–65.
Gæde P, Lund-Andersen H, Parving H, Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med. 2008;358(6):580–91.
Nathan DM, Cleary PA, Backlund JY, Genuth SM, Lachin JM, Orchard TJ, et al. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med. 2005;353(25):2643–53.
Eurich DT, Majumdar SR, McAlister FA, Tsuyuki RT, Johnson JA. Improved clinical outcomes associated with metformin in patients with diabetes and heart failure. Diabetes Care. 2005;28(10):2345–51.
Aguilar D, Chan W, Bozkurt B, Ramasubbu K, Deswal A. Metformin use and mortality in ambulatory patients with diabetes and heart failure. Circ Heart Fail. 2011;4(1):53–8.
Johnson JA, Majumdar SR, Simpson SH, Toth EL. Decreased mortality associated with the use of metformin compared with sulfonylurea monotherapy in type 2 diabetes. Diabetes Care. 2002;25(12):2244–8.
Hong J, Zhang Y, Lai S, Lv A, Su Q, Dong Y, et al. Effects of metformin versus glipizide on cardiovascular outcomes in patients with type 2 diabetes and coronary artery disease. Diabetes Care. 2013;36(5):1304–11.
Ali S, Fonseca V. Overview of metformin: special focus on metformin extended release. Expert Opin Pharmacother. 2012;13(12):1797–805.
Soraya H, Khorrami A, Garjani A, Maleki-Dizaji N, Garjani A. Acute treatment with metformin improves cardiac function following isoproterenol induced myocardial infarction in rats. Pharmacol Rep. 2012;64(6):1476–84.
Cittadini A, Napoli R, Monti MG, Rea D, Longobardi S, Netti PA, et al. Metformin prevents the development of chronic heart failure in the SHHF rat model. Diabetes. 2012;61(4):944–53.
Yin M, van der Horst IC, van Melle JP, Qian C, van Gilst WH, Sillje HH, et al. Metformin improves cardiac function in a nondiabetic rat model of post-MI heart failure. Am J Physiol Heart Circ Physiol. 2011;301(2):H459–68.
Andersson C, Sogaard P, Hoffmann S, Hansen PR, Vaag A, Major-Pedersen A, et al. Metformin is associated with improved left ventricular diastolic function measured by tissue Doppler imaging in patients with diabetes. Eur J Endocrinol. 2010;163(4):593–9.
Lexis CP, van der Horst IC, Lipsic E, Wieringa WG, de Boer RA, van den Heuvel AF, et al. Effect of metformin on left ventricular function after acute myocardial infarction in patients without diabetes: the GIPS-III randomized clinical trial. JAMA. 2014;311(15):1526–35.
Rena G, Pearson ER, Sakamoto K. Molecular mechanism of action of metformin: old or new insights? Diabetologia. 2013;56(9):1898–906.
Bosi E. Metformin–the gold standard in type 2 diabetes: what does the evidence tell us? Diabetes Obes Metab. 2009;11 Suppl 2:3–8.
King P, Peacock I, Donnelly R. The UK prospective diabetes study (UKPDS): clinical and therapeutic implications for type 2 diabetes. Br J Clin Pharmacol. 1999;48(5):643–8.
El Messaoudi S, Rongen GA, de Boer RA, Riksen NP. The cardioprotective effects of metformin. Curr Opin Lipidol. 2011;22(6):445–53.
Whittington HJ, Hall AR, McLaughlin CP, Hausenloy DJ, Yellon DM, Mocanu MM. Chronic metformin associated cardioprotection against infarction: not just a glucose lowering phenomenon. Cardiovasc Drugs Ther. 2013;27(1):5–16.
Lexis CP, Wieringa WG, Hiemstra B, van Deursen VM, Lipsic E, van der Harst P, et al. Chronic metformin treatment is associated with reduced myocardial infarct size in diabetic patients with ST-segment elevation myocardial infarction. Cardiovasc Drugs Ther. 2013.
Meaney E, Vela A, Samaniego V, Meaney A, Asbun J, Zempoalteca JC, et al. Metformin, arterial function, intima-media thickness and nitroxidation in metabolic syndrome: the mefisto study. Clin Exp Pharmacol Physiol. 2008;35(8):895–903.
Matsumoto K, Sera Y, Abe Y, Tominaga T, Yeki Y, Miyake S. Metformin attenuates progression of carotid arterial wall thickness in patients with type 2 diabetes. Diabetes Res Clin Pract. 2004;64(3):225–8.
Preiss D, Lloyd SM, Ford I, McMurray JJ, Holman RR, Welsh P, et al. Metformin for non-diabetic patients with coronary heart disease (the CAMERA study): a randomised controlled trial. Lancet Diab Endo. 2013.
Kao J, Tobis J, McClelland RL, Heaton MR, Davis BR, Holmes Jr DR, et al. Relation of metformin treatment to clinical events in diabetic patients undergoing percutaneous intervention. Am J Cardiol. 2004;93(11):1347–50.
Currie CJ, Poole CD, Evans M, Peters JR, Morgan CL. Mortality and other important diabetes-related outcomes with insulin vs other antihyperglycemic therapies in type 2 diabetes. J Clin Endocrinol Metab. 2013;98(2):668–77.
Malmberg K, Norhammar A, Wedel H, Ryden L. Glycometabolic state at admission: important risk marker of mortality in conventionally treated patients with diabetes mellitus and acute myocardial infarction: long-term results from the diabetes and insulin-glucose infusion in acute myocardial infarction (DIGAMI) study. Circulation. 1999;99(20):2626–32.
Mellbin LG, Malmberg K, Norhammar A, Wedel H, Ryden L. DIGAMI 2 investigators. Prognostic implications of glucose-lowering treatment in patients with acute myocardial infarction and diabetes: experiences from an extended follow-up of the diabetes mellitus insulin-glucose infusion in acute myocardial infarction (DIGAMI) 2 study. Diabetologia. 2011;54(6):1308–17.
Burla AK, Lobato NS, Fortes ZB, Oigman W, Neves MF. Cardiac fibrosis and vascular remodeling are attenuated by metformin in obese rats. Int J Cardiol. 2013;165(3):483–7.
Soraya H, Farajnia S, Khani S, Rameshrad M, Khorrami A, Banani A, et al. Short-term treatment with metformin suppresses toll like receptors (TLRs) activity in isoproterenol-induced myocardial infarction in rat: are AMPK and TLRs connected? Int Immunopharmacol. 2012;14(4):785–91.
Attia SM, Helal GK, Alhaider AA. Assessment of genomic instability in normal and diabetic rats treated with metformin. Chem Biol Interact. 2009;180(2):296–304.
Metcalfe A, Neudam A, Forde S, Liu M, Drosler S, Quan H, et al. Case definitions for acute myocardial infarction in administrative databases and their impact on in-hospital mortality rates. Health Serv Res. 2013;48(1):290–318.
Acknowledgments
None of the authors have reported conflict of interest. Funding was not required for this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Abualsuod, A., Rutland, J.J., Watts, T.E. et al. The Effect of Metformin Use on Left Ventricular Ejection Fraction and Mortality Post-Myocardial Infarction. Cardiovasc Drugs Ther 29, 265–275 (2015). https://doi.org/10.1007/s10557-015-6601-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10557-015-6601-x