
Abstract
Despite treatment advances, radioresistance and metastasis markedly impair the benefits of radiotherapy to patients with malignancies. Functioning as molecular switches, Rho guanosine triphosphatases (GTPases) have well-recognized roles in regulating various downstream signaling pathways in a wide range of cancers. In recent years, accumulating evidence indicates the involvement of Rho GTPases in cancer radiotherapeutic efficacy and metastasis, as well as radiation-induced metastasis. The functions of Rho GTPases in radiotherapeutic efficacy are divergent and context-dependent; thereby, a comprehensive integration of their roles and correlated mechanisms is urgently needed. This review integrates current evidence supporting the roles of Rho GTPases in mediating radiotherapeutic efficacy and the underlying mechanisms. In addition, their correlations with metastasis and radiation-induced metastasis are discussed. Under the prudent application of Rho GTPase inhibitors based on critical evaluations of biological contexts, targeting Rho GTPases can be a promising strategy in overcoming radioresistance and simultaneously reducing the metastatic potential of tumor cells.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
The Rho family of small guanosine triphosphatases (GTPases), which is one of the major branches of the Ras superfamily, consists of 8 subfamilies, among which the Rac (Rac1, Rac2, Rac3, RhoG), Rho (RhoA, RhoB, RhoC), and Cdc42 (Cdc42, RhoQ, RhoJ) subfamilies are best characterized [1, 2]. In recent decades, numerous studies on Rho GTPases have unveiled their critical roles in modulating the development of various diseases including cancer.
Functioning as molecular switches, Rho GTPases cycle between guanosine diphosphate (GDP)-bound state (inactive) and guanosine triphosphate (GTP)-bound state (active), and the GDP/GTP cycling is regulated mainly by three types of regulators: guanine nucleotide exchange factors (GEFs), GTPase-activating proteins (GAPs) and guanine nucleotide dissociation inhibitors (GDIs) [3]. GEFs catalyze GTP binding via removing the GDP from its binding site and therefore activate Rho GTPases for their interaction with various downstream effectors [2]. In contrast, GAPs accelerate the hydrolysis of GTP, converting the active state into the inactivate conformation [4, 5]. In addition, GDIs protect Rho GTPases from GDP dissociation and inhibit their activation by disturbing their interaction with GEFs [5].
Deregulations of Rho GTPase expression have been identified in different cancer types, indicating that they exert diverse effects to cancer development and progression (Table 1) [6]. Within tumor cells, Rho GTPases are involved in regulating a wide range of cellular events, such as actin cytoskeleton rearrangements, cell cycle progression, and repair to cellular damage [7,8,9]. Therefore, deregulations of Rho GTPases can alter the behavior of tumor cells, and the elucidation of how Rho GTPases participate in tumorigenesis and evasion to therapeutics is far-reaching in the development of anti-cancer treatment modalities.
In this review, the roles and underlying mechanisms of Rho GTPases in regulating radiotherapeutic efficacy and metastasis are investigated. Our review predominantly aims to integrate current findings on Rho GTPases referring to radioresistance and metastasis, and to provide insights into their correlations, which might inspire the development and application of novel strategies for cancer treatment.
2 Cancer radiotherapy and metastasis
2.1 Radiotherapy for cancer
For decades, radiotherapy has been a standard and effective treatment as monotherapy or in combination with surgery, chemotherapy, or targeted therapy for malignancies [10, 11]. The primarily used modalities of ionizing radiation (IR) include photon, electron, and particle radiations [12]. Photon radiation is most widely used in radiotherapy [13]. Electron radiation, which is beneficial in the treatment for superficial targets because of its highly centralized radiation doses and the sharp decline of doses with depth, is principally combined with other types of radiation in radiotherapy to improve dose distribution and therapeutic benefits [14, 15]. Compared to electron radiation, particle beam penetrates deeper with a rapid dose falloff, steeply depositing at the end of the particle range, and induces less damage to the outer surface [16]. Current research on radioresistance mainly focuses on photon (gamma) radiation.
The effect of IR on tumor cells is determined by various factors. At cellular levels, the lethal effect of IR on cancer cells is mainly achieved through the production of reactive oxygen species (ROS), also known as free radicals, and the induction of double-strand breaks (DSBs) of DNA [17]. If DSBs remain unrepaired, genome instability and cell death eventually occur [17, 18]. Therefore, cancer cells protect themselves from cellular damage by activating survival signals and pathways correlated with genome stability.
In clinical practice, the sensitivity of malignancies to IR determines the treatment responsiveness and efficacy. However, a large number of patients develop radioresistance, leading to impaired benefits and even treatment failure. Resistance to radiotherapy remains an enormous challenge and endeavors have been made to explore the underlying mechanisms.
2.2 Metastasis of cancer
Cancer metastasis indicates the spread of cells to locations distant from their original sites and the consequential adaptation to other tissues and environments [19]. The process of metastasis can be mainly divided into three steps including invasion, intravasation, and extravasation, and all of these steps involve cellular movements [20]. Actin cytoskeleton, which is required for cell motility, plays an important role in metastasis [21]. The rearrangement of actin cytoskeleton offers the structure and driving force essential for cell movements [21, 22]. A variety of molecules are involved in controlling the process of actin cytoskeleton rearrangement, among which Rho GTPases are notable for regulating this process [23].
Once the confined tumor metastasizes, it becomes nearly incurable by radiation due to dissemination, and radiotherapy for metastatic tumor can only represent an alternative for palliation with much fewer advantages compared to that for confined tumors [24,25,26]. In consequence, the majority of cancer deaths are caused by metastasis [27]. Based on the pernicious outcomes caused by cancer metastasis, the effectiveness of cancer therapy, including radiotherapy, largely depends on controlling the process of metastasis.
Unfortunately, researchers have identified that radiotherapy can promote the metastatic ability of tumor cells, which might counteract the benefits brought by radiotherapy. Therefore, the clarification of the complex regulatory pathways for radioresistance and metastasis is essential to inspire the development of novel strategies for optimizing therapeutic effects.
3 Rho GTPases in radiotherapy
Since Rho GTPases have established roles in tumorigenesis, recent studies emphasize on exploring the correlation between Rho GTPases and chemo- or radioresistance, aiming to provide evidence for improving treatment effectiveness by manipulating the activity and expression of Rho GTPases. Among the members of Rho GTPases, Rac1, RhoA, and RhoB are best characterized for their functions in radiotherapy (Table 2). Although Rho GTPases have been observed to be upregulated or hyper-activated in many tumor types, to date, it remains controversial whether Rho GTPases promote radioresistance in tumor cells.
3.1 Role of Rho GTPases in radiotherapy
3.1.1 Rac1 and radiotherapeutic efficacy
Rac1 is the best characterized member of Rac subfamily for its wide participation in tumorigenesis. The expression of Rac1 is generally upregulated in irradiated tumor cells compared to non-irradiated tumor cells or normal cells. For example, in comparison with parental cells, breast cancer cells under IR demonstrate an increase in Rac1 protein expression [33]. Rac1 is also upregulated in radioresistant head and neck squamous cell carcinoma (HNSCC) cells according to proteome-based data [50, 51]. Rac1 is not only upregulated but also hyper-activated in irradiated tumor cells. Under treatment with radiation, Rac1 activation levels and the binding of Rac1 with p21-activated kinases (PAKs) in non-small cell lung cancer (NSCLC) cells are dramatically increased, which indicates that radiation can activate Rac1 and induce the downstream pathways [31, 36]. In addition, marked activation of Rac1 is detected in IR-exposed breast cancer cells, cervical carcinoma cells, and breast cancer cells [29, 32, 33]. In human nasopharyngeal carcinoma cells, Rac1 is detected more abundantly in the active GTP-bound form and with translocation to cell membrane under the treatment with IR [38]. Intriguingly, the activation of Rac1 under radiotherapy can be regarded as a protective mechanism that increases radioresistance, or conversely the downstream signaling of IR-mediated apoptotic pathways which enhances radiation-induced cytotoxicity. The details of these discrepant effects are further discussed in our review.
Rac1 has been reported as a promoter of radioresistance in pancreatic cancer cells [30], glioma cells [34], HNSCC cells [31], cervical carcinoma cells [28, 32], and breast cancer cells [29, 33]. In pancreatic cancer cells, glioma cells, and HNSCC cells, the inhibition of Rac1 by inhibitors sensitizes cells to radiotherapy, indicating that Rac1 promotes radioresistance [30, 31, 34]. In addition, the dominant-negative form of Rac1 that is constitutively inactive, Rac1-N17, is used for investigation and it is demonstrated that cervical carcinoma cells and breast cancer cells with Rac1-N17 are more sensitive to radiotherapy, showing susceptibility to DNA damage, delayed DNA repair, and increased apoptosis [28, 29, 32, 33]. In contrast, reduced damage by DNA is detected in the dominant-positive Rac1-V12 clones of cervical carcinoma cells with higher Rac1 activation [32].
On the contrary, Rac1 has also been identified as an enhancer of radiosensitivity in nasopharyngeal carcinoma cells [38, 39] and NSCLC cells [36, 37]. In nasopharyngeal carcinoma cells, the enhanced activity of Rac1 is correlated with increased radiosensitivity [38, 39]. In addition, Rac1-N17 suppresses radiation-induced apoptosis in NSCLC cells [36]. The downregulation of GDI and subsequent Rac1 activation result in apoptosis and sensitization to radiotherapy in NSCLC cells [37]. When compared to the results from Skvortsov et al., it implies that pathways directly regulated by GDI and independent of Rac1 may exist, and these pathways can dominant the effect of Rac1 to radiotherapy in NSCLC cells [31, 37]. The use of different NSCLC cell lines also accounts for the discrepancies of the results [31, 36, 37].
Patient specimens are also used to validate the roles of Rac1 in radioresistance. Researchers identified that the expression of Rac1 is upregulated in radioresistant NSCLC patients [35]. Conversely, HNSCC patients with early response to chemo-radiotherapy are characterized by a lower expression of Rac1 in tumors [31]. Although the lack of clinical data or currently available database in terms of radiotherapy limits the amount of evidence, these data from patients more convincingly support the role of Rac1 in modulating radiotherapeutic efficacy and open new opportunities for future therapeutics.
3.1.2 RhoA and radiotherapeutic efficacy
RhoA is a canonical member of Rho subfamily that regulates cancer development and progression. Originally, RhoA was identified to be irrelevant to radioresistance [42]. However, later research reveals their correlations. The expression of RhoA in glioblastoma cells can be induced by IR exposure [41]. In addition, RhoA overexpression confers the sensitivity to radiation in glioblastoma cells, and therefore RhoA might be involved in the cytotoxic effects under radiotherapy [41]. Nevertheless, the majority of studies referring to RhoA and radioresistance show opposite results. In cervical carcinoma cells [52], melanoma cells [52], and glioblastoma cells [40], RhoA is identified to promote radioresistance. Cervical carcinoma cells utilize the upregulation of RhoA as a defense mechanism against DNA damage induced by radiation [52]. In cervical carcinoma cells and melanoma cells, the RhoA-V14 clones with constitutively activated RhoA demonstrate increased survival and proliferation under radiation compared to RhoA-N14 clones [52]. In contrast to RhoA activation, the inhibition of RhoA-mediated pathways overcomes the radioresistance of glioblastoma cells, indicating that RhoA promotes resistance to radiotherapy [40]. Compared to the radiosensitizing effect of RhoA identified by Mclaughlin et al., it might be contributed by the different glioblastoma cell lines used in the studies [40, 41].
3.1.3 RhoB and radiotherapeutic efficacy
RhoB is another member of Rho subfamily sharing over 85% similarity with RhoA in amino acid sequence identity, whereas RhoB possesses specific post-translational modification mechanisms and localizations, which are responsible for its distinct functions in regulating cellular events [53]. The role of RhoB in radioresistance can also be dualistic.
Ionizing radiation can alter the activation of RhoB. In glioma cells, the activation of RhoB is demonstrated to be enhanced after exposure to IR [45]. The activated RhoB further contributes to the alterations in radioresistance. For example, the resistance of cervical cancer cells [42], glioblastoma cells [45], colorectal cancer cells [46], and glioma cells [44] to radiotherapy is promoted by RhoB. The dominant-negative form of RhoB, RhoB-N19, induces sensitivity to radiation in cervical cancer cells [42]. The transfection with RhoB-N19 also reduces the survival of glioma cells under irradiation, indicating that RhoB can be targeted to produce the radiosensitizing effect [44]. In addition to in vivo studies, with the use of in vivo xenograft models of glioma cells, RhoB-N17 is identified to sensitize the tumor cells to irradiation [43]. RhoB overexpression is correlated with resistance to radiation, and the depletion of RhoB restores radiosensitivity in colorectal cancer cells and zebrafish models [46]. Patient specimens with clinical data are further utilized to validate the role of RhoB in the radioresistance of colorectal cancer patients. In colorectal cancer patients treated with radiotherapy, higher expression of RhoB contributes to advanced TNM stages, recurrence, and poorer survival [46].
In contrast, RhoB can protect neoplastically transformed mouse embryonic fibroblasts and leukemia cells from IR. RhoB is pivotal in the apoptotic response of neoplastically transformed mouse embryonic fibroblasts and xenograft models to radiotherapy, while targeting RhoB renders resistance to irradiation [48]. In addition, the downregulation of RhoB restores the growth and survival of leukemia cells and lung adenocarcinoma cells after irradiation [47, 49].
3.2 Mechanisms underlying the regulation of Rho GTPase-mediated radiotherapeutic efficacy
3.2.1 Mechanisms of Rac1 in regulating radiotherapeutic efficacy (Fig. 1)
Radiation-induced DSB is the major mechanism by which radiotherapy leads to cell death [54]. DSBs are predominantly repaired by the signaling pathways induced by ataxia-telangiectasia mutated (ATM)-associated protein kinases, which mainly include ATM and ataxia-telangiectasia and Rad3-related (ATR). ATM and ATR phosphorylate various downstream effectors for DSB repair, such as H2A histone family member X (H2AX), checkpoint kinase (Chk)1, and Chk2 [55]. Rac1 inhibition suppresses the activation of ATR and ATM signaling in breast cancer cells, indicating that Rac1 is involved in enhancing ATR and ATM levels to resist DSBs [29]. In pancreatic cancer cells, Rac1 plays a similar role as the promoter of radioresistance by activating ATR/Chk1 and ATM/Chk2 kinases, which involve in antagonizing radiation-induced apoptosis [30]. In human cervical carcinoma cells, the expression of pH2AX and pChk1 is significantly downregulated in dominant-negative Rac1-N17 clones, which indicates reduced DNA repair and increased apoptosis [32]. Moreover, Rac1 overexpression is correlated with enhanced activities of extracellular signal-regulated protein kinases 1 and 2 (ERK1/2) and nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB), and both of them lead to the expression of proteins against apoptosis, including myeloid cell leukemia-1 (Mcl-1), a B cell lymphoma 2 (Bcl-2) family member, and B cell lymphoma-extra large (Bcl-xL) in breast cancer cells [33]. The activation of ERK1/2 and NF-κB signaling has been widely recognized in cell survival and radioresistance [56, 57]. Cofilin (CFL)-1 is well-known as an actin cytoskeleton regulator, but it is also upregulated in irradiated glioma cells and contributes to the enhance DNA repair capacity [58, 59]. More specifically, in glioma cells, Rac1 promotes radioresistance through the activation of Rac1-Wiskott-Aldrich syndrome protein family member 2 (WAVE2)-actin-related proteins 2/3 (Arp2/3) signaling pathway, and the subsequent increase in CFL-1 [34].

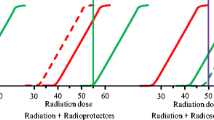
Rac1-mediated signaling pathways in regulating radiotherapeutic efficacy. Rac1 cycles between the inactive (GDP-bound) and active (GTP-bound) states. GEFs transform the inactive Rac1 into its active state, which further contributes to the activation of downstream effectors. Rac1 plays a dual role in regulating radioresistance via activating pro-apoptotic or anti-apoptotic signaling pathways depending on different biological contexts
The balance between DNA repair and cell cycle arrest also determines the survival of irradiated cells, because the arrest in cell cycle provides critical time for DNA repair prior to replication [60]. Inhibition of Rac1 abrogates the phosphorylation of ERK1/2 and mitogen-activated protein kinase kinase 1/2 (MEK1/2) and further attenuates the IR-induced cell cycle arrest in breast cancer cells, while this effect is not detected in normal mammary epithelial cells [29]. However, unlike that in breast cancer cells, the involvement of ERK1/2 is not detected in pancreatic cancer cells, indicating the diversity of Rac1-regulated pathways in different cell lines [29, 30].
Several studies have demonstrated an opposite role of Rac1 in regulating radioresistance, and the mechanisms are illustrated as follows. In response to stress signals including IR, apoptotic cell death occurs by the activation of Bcl-2-associated X (Bax) and Bcl-2 homologous antagonist killer (Bak), and p38 mitogen-activated protein kinase (MAPK) is also positively regulated in the induction of apoptosis [61]. It is shown that the expression of Rac1-N17 decreases p38 MAPK as well as Bak and Bax activation, and further inhibits apoptosis induced by radiotherapy in NSCLC cells [36, 62]. Compared to the Rac1-p38 MAPK-mediated radiosensitizing effects in NSCLC cells, in cervical carcinoma cells, Rac1 increases p38 MAPK activation, which further activates protein kinase B (PKB/Akt) and protects the cells from IR [28]. Therefore, the Rac1-p38 MAPK pathway can signal different downstream effectors, which lead to opposite responses to radiotherapy in different cell lines. In nasopharyngeal carcinoma cells, Rac1 activation induces nicotinamide adenine dinucleotide phosphate (NADPH)-mediated ROS generation, which further increases tumor susceptibility to radiotherapy [38]. Moreover, the Rac1-induced production of ROS also increases the activation of c-Jun N-terminal kinases (JNK) and activator protein 1 (AP1), which promotes the apoptosis of nasopharyngeal carcinoma cells [39].
3.2.2 Mechanisms of RhoA in regulating radiotherapeutic efficacy
Similar to Rac1, RhoA activation increases the levels of DNA damage repair via the activation of Chk1/Chk2 protein kinases and further phosphorylation of Chk1/Chk2 in cervical cancer cells [52]. In glioma cells, RhoA is related to the activation of Rho-associated protein kinase 2 (ROCK2) and CFL-1, which are essential for actin dynamics and promoting radioresistance [40]. The RhoA GEF, neuroepithelial cell transforming gene 1A (Net1A), is required for the activation of ATM and the further phosphorylation of H2AX, which repairs DNA damage induced by radiotherapy [63]. However, the Net1A-mediated signaling pathway is RhoA-independent, indicating that the GEFs of RhoA might also have essential roles in independently regulating radiotherapeutic efficacy [63]. In contrast, the mechanisms that RhoA suppresses radioresistance remain largely unclear.
3.2.3 Mechanisms of RhoB in regulating radiotherapeutic efficacy
With the use of clustered regularly interspaced short palindromic repeats (CRISPR), complete depletion of RhoB is achieved in colorectal cells, which allows a more convincible result on the role of RhoB in regulating radioresistance [46]. RhoB depletion enhances the resistance to radiotherapy via activating Akt and forkhead box protein M1 (FOXM1), which are vital in promoting cell survival [46]. The mechanisms by which RhoB regulates radioresistance also include the upregulation of hypoxia-inducible factor (HIF)-1α, which increases the ability of DNA repair and inhibits apoptosis [64, 65].
3.3 Other Rho GTPases in regulating radiotherapeutic efficacy
Rac2, which is a member of the Rac subfamily GTPases, also involves in the regulation of radiotherapeutic efficacy. The high expression of Rac2 contributes to the enhanced activity of NADPH oxidase, resulting in the generation of ROS under IR [66]. Rac2 also interacts with p38 MAPK and forms a negative feedback loop, which controls the activity of NADPH oxidase for the induction of DNA DSBs [66]. RhoC is a member of the Rho subfamily GTPases. RhoC overexpression confers the protection against radiotherapy for human cervical cancer cells, while RhoC inhibition leads to the sensitization of cells to irradiation [67]. In addition, RhoC activates ROCK2, which results in the increased expression of pH2AX and MRE11–RAD50–NBS1 (MRN) complex for DNA damage repair [67]. The roles and mechanisms of other Rho GTPases in regulating radioresistance remain largely unexplored. Therefore, they are not the focus of this commentary, and future studies should further investigate their involvement in radiotherapeutic resistance.
3.4 Other proposed mechanisms of Rho GTPases in regulating radiotherapeutic efficacy
As illustrated above, the mechanisms directly connecting Rho GTPases to radioresistance are identified by researchers. Except the currently unveiled molecular pathways, proposed mechanisms are also essential for the understanding of Rho GTPase-mediated radiotherapeutic efficacy, since Rho GTPases are involved in regulating a wide spectrum of cellular processes. Radioresistance can be affected by the existence of cancer stem cells (CSCs), and the response to radiation-induced oxidative stress and the alteration in metabolism. Emerging evidence has indicated their connections with Rho GTPases. The epigenetic regulation of Rho GTPases also contributes to their involvement in radioresistance.
3.4.1 Rho GTPases and cancer stem cells
The existence of CSCs and their status can determine the radiotherapeutic effects. CSCs are cancer cells possessing characteristics similar to normal stem cells, with the ability to generate tumors via self-renewal and differentiation into multiple cell types [68]. Their prompt activation of DNA repair pathway, enhanced ROS scavenging system, quiescence, and stemness are crucial to resist radiotherapy [69,70,71]. In addition, the microenvironment, more specifically the niche occupying hypoxic, perivascular, and invasive tumor areas, provides protection against radiation-induced damage [72, 73]. Hence, the failure to eradicate CSCs can contribute to the development of radioresistance. Rac1 promotes the expansion of liver CSCs [74]. In addition, Rac1 increases the frequency of hematopoietic cells in quiescent state and participates in leukemia initiation and maintenance [75]. Rac1 inhibition using shRNA or inhibitor decreases the expression of self-renewal transcription factor and prevents the acquisition of CSC states in gastric adenocarcinoma cells [76]. Yoon et al. identify that the inhibition of Rac1 suppresses the stemness of glioma stem cells and sensitizes the cells to radiation [77]. RhoA promotes stem cell phenotypes in gastric adenocarcinoma cells [78]. Moreover, Cdc42 enhances the activity of breast cancer stem cells and contributes to cell metastasis [79]. The Cdc42 signaling pathway is also involved in the tumorigenesis of cervical cancer by activating CSCs [80]. In conclusion, Rho GTPases are closely connected to CSCs and thereby enhance the resistance to radiotherapy.
3.4.2 Rho GTPases and radiation-induced oxidative stress response
Radiation-induced oxidative stress is mainly attributed to the production of ROS, and the response to radiation-induced oxidative stress affects cell survival under radiotherapy. As discussed above, Rac1 has been proved to increase radiosensitivity by increasing NADPH oxidase activity and ROS production in nasopharyngeal carcinoma cells [37, 38]. Other studies have also discovered the association of Rac1 and ROS, although there is no directly proved connection to radioresistance. Rac1 promotes ROS generation in pancreatic cancer cells, osteosarcoma cells, and hepatocellular carcinoma cells [81, 82]. For other members of Rho GTPases, very few reports have described their effects on simulating ROS production, and even one study suggests that Cdc42 is unable to stimulate ROS formation by NADPH oxidase [83]. In contrast, a number of studies identify that ROS directly or indirectly activates Rho GTPases, for example, RhoA and RhoB [84,85,86,87,88]. These studies suggest that interactions may exist between Rho GTPases and ROS, and further exploring the mechanisms can uncover the role of Rho GTPases on radiation-induced oxidative stress response and radioresistance.
3.4.3 Rho GTPases and cell metabolism
Deregulated metabolism is one of the hallmarks of tumor cells [89]. Aerobic glycolysis (the Warburg effect) is the best-known metabolic alteration of tumor cells [89]. Aerobic glycolysis provides survival advantages under resource limitation and is crucial for supporting cancer cells to evade apoptosis under stressful conditions [90]. Recent studies have identified that radioresistance is closely connected to aerobic glycolysis and the glycolytic enzymes within this process. For example, the AKT-mediated enhancement of aerobic glycolysis confers radioresistance to tumor cells [91]. In addition, the expression of glycolytic enzymes pyruvate kinase M2 isoform (PKM2) and hexokinase 2 (HK2) enhances aerobic glycolysis and induces radioresistance [92, 93]. Enhanced aerobic glycolysis provides nucleotide pools for DNA repair under irradiation [94, 95]. ROS production is also decreased by enhanced glycolysis due to the less reliance of cancer cells on mitochondrial oxidative phosphorylation [96]. The main product of aerobic glycolysis, lactic acid, inhibits the activation of immune cells [97]. Researchers have pointed out that Rho GTPases are associated with aerobic glycolysis. Rac1 activates AKT pathway and induces the expression of glycolytic enzymes [98, 99]. RhoA promotes glucose transporter translocation and stimulates aerobic glycolysis [100]. Therefore, targeting Rho GTPases and Rho GTPase-mediated altered metabolism is a feasible strategy for overcoming radioresistance.
3.4.4 Rho GTPases and epigenetic regulation
Epigenetic regulations contribute to the changes in the expression of Rho GTPases without alterations in DNA sequences, leading to the activation or inactivation of pathways involved in radioresistance [101]. DNA methylation, histone modification, and microRNA (miRNA) expression are the three main patterns of epigenetic regulations [102]. Rac1 promoter methylation is identified in glioblastoma cells and responsible for its transcription, while the removal of methylation represses Rac1 expression [103]. In contrast, Dopeso et al. find that the promoter hypermethylation of RhoA is not significantly correlated with RhoA expression variations in colorectal tumors [104]. Similar to RhoA, RhoB promoter methylation does not significantly regulate its expression in lung cancer cell lines [105]. There are by far no reports on the promoter methylation of Cdc42 in cancer cells. Interestingly, Cdc42 is reported to induce the methylation of the promoter of tumor suppressor genes in colorectal cancer cells [106]. The methylation status of Rho GTPase regulators also contributes to the activity of Rho GTPases. For example, the promoter region of Rac-GEF PREX1 is hypermethylated in luminal breast cancer, while hypomethylated in normal breast epithelium [107]. Hypermethylation of ARHGAP28 increases RhoA activity and promotes the metastasis of colon cancer cells [108]. Histone acetylation of Rho GTPase promoters can also regulate the expression of Rho GTPases. RhoB expression levels are upregulated under the histone acetylation of RhoB promoter in a wide spectrum of human cancer cells [109]. miRNAs are small, non-coding RNAs that target mRNAs for degradation or inhibition of translation [110]. miR-124 binds to the 3′-UTR of Rac1 and decreases the mRNA and protein expression of Rac1 in pancreatic cancer [111]. miR-31 inhibits the invasion and metastasis of gastric cancer by targeting RhoA [112]. miR-19a/19b targets RhoB and promotes the development of clear cell renal cell carcinoma [113]. miR-224 suppresses the migration of colorectal cancer cells by targeting Cdc42 [114]. The studies on Rho GTPases with methylation, histone acetylation, and miRNAs offer new insights into the epigenetic regulation of Rho GTPases, and novel drugs for mediating these epigenetic changes can be developed.
4 Rho GTPases and metastasis
Tumor metastasis is one of the hallmarks for cancer and contributes to the unfavorable prognosis of patients. The metastasis of tumor cells depends largely on cellular motility and involves invasion, intravasation, and extravasation. Throughout the process of metastasis, the formation and organization of actin cytoskeleton are the key components for cellular movements. The metastasis of cancer cells is largely dependent on cell migration, and the movement of tumor cells can be divided into two types, including individual and collective movement. Based on the majority of current studies, individual cell movement exhibits two behaviors, namely mesenchymal and amoeboid, which are interconvertible between each other.
Rho GTPases are deemed to be associated with metastasis due to their crucial roles in regulating actin structures. Rho GTPases are also critical in controlling the modes of tumor cell movements, and different subfamilies of Rho GTPases can exert diverse effects on certain movement types. For example, tumor cells utilize Rac-dependent mesenchymal movement in two-dimensional migration and resort to Rho-dependent amoeboid movement in three-dimensional migration [115, 116]. Rac1, Cdc42, and RhoA are the best characterized members of Rho GTPases in terms of metastasis. Herein, we mainly discuss the dominating pathways involved in modulating metastasis.
Epithelial-to-mesenchymal transition (EMT) is regarded as an important step of individual cell migration, by which tumor cells acquire mesenchymal mobility and are allowed to invade the surrounding tissues [117]. Rac1 activates its downstream effectors, WAVE and Arp2/3 complex, which bind to nucleating promoting factors and help produce the filament networks, namely lamellipodia, at the leading edge [118, 119]. Among the members of WAVE family proteins, WAVE2 is the most critical one in directing Rac1-regulated actin polymerization and lamellipodia formation [119, 120]. The downstream effector PAK, which is essential for kinase activation, is activated by Rac1 and contributes to EMT to enhance invasion and metastasis [121]. To be specific, the Rac1-PAK pathway modulates the phosphorylation of LIM kinase (LIMK), which further phosphorylates CFL and regulates actin dynamics as well as cell movement [122]. Rac1 also promotes EMT through simultaneously activating the MEK1/2 and Src signaling pathways [123]. The hallmarks of EMT include the loss of adhesion molecule E-cadherin and the increase of mesenchymal marker N-cadherin and vimentin. Signal transducer and activator of transcription 3 (STAT3) is identified to be involved in EMT by decreasing E-cadherin expression and increasing vimentin and N-cadherin expression [124]. By contrast, the EMT process can be disrupted by Rac1 inhibition which subsequently attenuates STAT3 phosphorylation, indicating the importance of Rac1-STAT3 pathway in metastasis [125]. The activation of Rac1 also enhances the MAPK pathway effectors ERK1/2 and JNK, which regulate cell metastasis [126, 127].
Tumor metastasis also involves the process of proteolysis, and matrix metallopeptidases (MMPs) are essential in this process for mediating extracellular matrix degradation and promoting the traverse through tissue barriers. Rac1 is identified to induce the expression of MMPs to promote metastasis [126]. In contrast, the disruption of Rac1-GTP significantly decreases MMP expression [125]. Through increasing the formation of lamellipodia, which provide the force of forward movement, and the production of MMPs for extracellular matrix degradation, Rac1 promotes the mesenchymal movement and metastasis of tumor cells.
Similar to Rac1, Cdc42 promotes mesenchymal cell movement by the formation of actin-rich protrusions, namely invadopodia, which provide focused regions for extracellular matrix (ECM) degradation by MMPs. Cdc42 regulates the expression of MMP9 expression, which contributes to the Cdc42-mediated ECM remodeling [128]. Cdc42 is also important for generating the actomyosin contractility, which is a hallmark of amoeboid tumor cell movement [129]. Under Cdc42 activation, myotonic dystrophy kinase-related Cdc42-binding kinase (MRCK) is activated and subsequently myosin light chain 2 (MLC2) is phosphorylated, which promotes actin contractility [130].
As illustrated above, Rac and Cdc42 induce the formation of membrane protrusions at the leading edge. In comparison, Rho stimulates tail retraction at the leading edge of migrating cells [131]. The amoeboid movement of tumor cells is associated with RhoA-mediated activation of ROCK, which is the best-characterized downstream effector of RhoA [132]. The activated ROCK stimulates actin cytoskeleton formation and generates the contractile force of actomyosin [132]. For the two ROCK isoforms ROCK1 and ROCK2, the expression of ROCK2 is higher in rounded cells, suggesting that ROCK2 is preferentially involved in amoeboid movement [133]. Moreover, ROCK phosphorylates downstream targets including LIMK and CFL, thereby inducing cellular contractility and actin polymerization [133, 134].
Overall, Rho GTPases have well-established roles in promoting cancer cell metastasis, and the overlapping pathways involved in controlling both radioresistance and metastasis indicate that interactions exist between the two processes.
5 Rho GTPases in radiation-induced metastasis
Radiotherapy prolongs the survival of patients suffering from cancer with restricting the size of primary tumors. However, an increasing number of studies have identified that radiotherapy can unexpectedly enhance cancer metastasis, leading to cancer progression and deaths.
One of the earliest studies that connect radiotherapy with metastasis was performed in rat glioma cells, in which the irradiation-induced metastasis can be further enhanced by the expression of dominant-negative Rac-N17 [135]. It seems counterintuitive that although Rac1 generally promotes metastasis, in glioma cells, Rac-N17 expression enhances radiation-induced metastasis, and this effect might be contributed by the simultaneous inhibition of Rac2 and Rac3, or can be cell type-dependent. By contrast, most of the later studies demonstrate the increased expression of Rho GTPases under radiotherapy, which promotes metastasis.
In radioresistant HNSCC cells, Rac1 is upregulated with enhanced migratory ability compared to radiosensitive cells [51]. Under IR exposure, the adhesion between tumor cells and endothelial cells is strengthened, which favors subsequent extravasation and metastasis, while the use of Rac1 inhibitors can reduce this adhesion [136]. In addition to the above in vitro studies, in mice model, total body radiation enhances the extravasation and lung metastasis of tumor cells [136]. Interestingly, the administration of lovastatin can suppress the radiation-enhanced metastasis, suggesting that the use of lipid-lowering drugs during radiotherapy might restrict cancer metastasis and benefit the patients [136].
Treatment with irradiation also enhances cell motility by activating RhoA and ROCK/MLC2 signaling pathways [137]. In irradiated glioblastoma cells, both Rac1 and RhoA are activated by phosphoinositide 3-kinases (PI3K), and subsequently ROCK activity is enhanced to induce the metastatic transformation of cells, suggesting that PI3K-mediated Rho signaling activation under irradiation is required for radiation-induced metastasis [138]. Osaki et al. extend the above results via RhoA-N19, which decreases the migration of cervical carcinoma cells following irradiation, and this effect is also observed in melanoma cells [52]. In addition, the carbon-ion irradiation of pancreatic carcinoma PANC-1 cells also promotes nitric oxide production, which activates the PI3K-Akt pathway [139]. The PI3K-Akt signaling pathway subsequently activates RhoA and promotes actomyosin contraction as well as cell invasion [139]. Intriguingly, Fujita et al. identify that in pancreatic carcinoma MIAPaCa-2 cells, carbon-ion irradiation inhibits the metastasis by degrading activated Rac1 and RhoA [139, 140].
Functioning as an important member in mediating radioresistance, RhoB also involves in radiation-induced metastasis. Zebrafish models provide robust, rapid, and inexpensive means to evaluate the metastatic potential of human cancer cells [141]. Complete RhoB depletion using CRISPR in zebrafish models impairs radiation-induced metastasis of colorectal cancer cells [46].
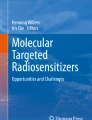
On the basis of these significant findings, Rho GTPases serve as essential mediators between irradiation and metastasis, contributing to the metastasis induced by radiotherapy. In consequence, radiotherapy should be performed with a better strategy, due to the evidence that radiotherapy promotes cell metastasis by altering the expression of Rho GTPases. For optimizing the therapeutic benefits of radiotherapy, inhibitors of Rho GTPases are promising to suppress radiation-induced metastasis, especially when radioresistance can simultaneously be decreased through interrupting Rho GTPase activity (Fig. 2).

Overview of the correlation among Rho GTPases, cancer radioresistance, and metastasis. Irradiation contributes to the activation of Rho GTPases. In general, Rho GTPases have a well-established role in promoting cell motility and serve as important mediators in radiation-induced metastasis. Rho GTPases can enhance or suppress radioresistance depending on different biological contexts, and therefore, inhibitors of Rho GTPases should be prudently used
6 Conclusions and future directions
Radiotherapy is a standard treatment for controlling tumor progression in a wide range of cancers. In spite of the advances in radiotherapy, the effectiveness and benefits of radiotherapy to patients are restricted by the development of radioresistance and metastasis. Regulations of radiotherapeutic resistance involve various signaling pathways, and Rho GTPases with their downstream effectors have been emerging as important regulators of radioresistance in recent years.
Our review highlights that contradictory results exist for the roles of Rho GTPases in regulating radioresistance. These variations can be contributed by several factors: (1) different methods interfering the expression of Rho GTPases such as siRNA, dominant-negative/positive mutants, and CRISPR; (2) different in vitro and in vivo models; (3) the types of irradiation; (4) the domination of downstream signaling pathways activated by Rho GTPases. Therefore, the effects of Rho GTPases can be biological context-dependent, and for those conditions where Rho GTPases promote radioresistance, inhibitors targeting Rho GTPases are promising in reversing the resistance to radiotherapy.
Unfortunately, an increasing number of studies demonstrate that radiotherapy increases the metastatic potential of malignancies. In light of the findings that irradiation activates Rho GTPases and activated Rho GTPases enhance cell motility, Rho GTPases serve as potent mediators between radiotherapy and metastasis. Intriguingly, although the role of Rho GTPases in radioresistance varies, the whelming majority of current studies linking radiotherapy with metastasis demonstrate that Rho GTPases are essentially utilized by cancer cells to both resist the cytotoxic effects of irradiation and evade radiotherapy by metastasizing from their original location. This phenomenon indicates that the use of Rho GTPase inhibitors might simultaneously suppress radioresistance and metastasis, which significantly restrains tumor progression and enhances therapeutic effects. However, for those conditions where radiosensitivity is enhanced by Rho GTPases, the benefits of inhibitors might be compromised. In consequence, Rho GTPase inhibitors must be prudently applied in clinical practice, and individualized treatment regimens with critical evaluations of therapeutic strategies should be performed.
Inhibitors of Rho GTPases have been developed as a critical strategy to target the activation of Rho GTPases both in vivo and in vitro [142]. However, none of these inhibitors can be applied in clinical practice. Current Rho GTPase inhibitors remain to be tested in clinical trials due to their low efficacy and potential deleterious effects. Rho GTPases are involved in various fundamental cellular processes in addition to tumorigenesis [143,144,145,146,147,148]. For example, Rho GTPases play critical roles in early embryogenesis and the development of organ systems in vivo, while the deletion of Rho GTPase leads to early embryonic death [143, 144]. Rho GTPases promote glucose uptake in adipose tissue, pancreas, and skeletal muscle, indicating that the inhibition of Rho GTPases may induce severe diabetes of patients [145,146,147]. Rho GTPases are involved in immune response including the development, activation, differentiation, and migration of lymphocytes, and therefore, Rho GTPase inhibition can unexpectedly disrupt immune response [148]. Future studies on Rho GTPase inhibitors should explore the strategy to optimize the efficacy of inhibition in cancers with minimizing the disruption of fundamental physiological processes.
Based on our review of the literature, current studies of Rho GTPases on radioresistance can be improved in the following aspects. To date, few studies have focused on the mechanisms by which other Rho GTPases, except Rac1, RhoA, and RhoB, regulate radioresistance. Future studies should explore the roles and the underlying mechanisms of these Rho GTPases, for example, the canonical member Cdc42, in mediating radioresistance. Moreover, most of the studies are limited to in vivo investigation; thereby, robust in vivo models can be established and applied for the study of Rho GTPase-regulated radioresistance. Furthermore, clinical data are required to confirm the role and evaluate the predictive value of Rho GTPases in radiotherapeutic efficacy.
In conclusion, the roles of Rho GTPases in radioresistance are highly dependent on biological contexts, while their roles in metastasis and radiation-induced metastasis are relatively more definite. Emerging studies on Rho GTPases provide exciting opportunities for improving the therapeutic effects of radiotherapy. The dissection of mechanisms leading to radioresistance and metastasis will facilitate the development and application of promising strategies for patient-specific treatment in clinical practice.
References
Goitre, L., Trapani, E., Trabalzini, L., & Retta, S. F. (2014). The Ras superfamily of small GTPases: the unlocked secrets. In Ras signaling (pp. 1–18). Springer.
Hodge, R. G., & Ridley, A. J. (2016). Regulating Rho GTPases and their regulators. Nature Reviews Molecular Cell Biology, 17(8), 496–510.
Cardama, G., Gonzalez, N., Maggio, J., Menna, P. L., & Gomez, D. (2017). Rho GTPases as therapeutic targets in cancer. International Journal of Oncology, 51(4), 1025–1034.
Ulu, A., & Frost, J. A. (2016). Regulation of RhoA activation and cytoskeletal organization by acetylation. Small GTPases, 7(2), 76–81.
Cherfils, J., & Zeghouf, M. (2013). Regulation of small gtpases by gefs, gaps, and gdis. Physiological Reviews, 93(1), 269–309.
Tang, Z., Li, C., Kang, B., Gao, G., Li, C., & Zhang, Z. (2017). GEPIA: a web server for cancer and normal gene expression profiling and interactive analyses. Nucleic Acids Research, 45(W1), W98–W102.
Woldu, S. L., Hutchinson, R. C., Krabbe, L.-M., Sanli, O., & Margulis, V. (2018). The Rho GTPase signalling pathway in urothelial carcinoma. Nature Reviews Urology, 15(2), 83–91.
Cho, H. J., Kim, J.-T., Baek, K. E., Kim, B.-Y., & Lee, H. G. (2019). Regulation of Rho GTPases by RhoGDIs in human cancers. Cells, 8(9), 1037.
Orgaz, J. L., Herraiz, C., & Sanz-Moreno, V. (2014). Rho GTPases modulate malignant transformation of tumor cells. Small GTPases, 5(4), e983867.
Bernier, J., Domenge, C., Ozsahin, M., Matuszewska, K., Lefèbvre, J.-L., Greiner, R. H., Giralt, J., Maingon, P., Rolland, F., Bolla, M., Cognetti, F., Bourhis, J., Kirkpatrick, A., van Glabbeke, M., & European Organization for Research and Treatment of Cancer Trial 22931. (2004). Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. New England Journal of Medicine, 350(19), 1945–1952.
Lievens, Y., Gospodarowicz, M., Grover, S., Jaffray, D., Rodin, D., Torode, J., Yap, M. L., Zubizarreta, E., & GIRO Steering and Advisory Committees. (2017). Global impact of radiotherapy in oncology: saving one million lives by 2035. Radiotherapy and Oncology, 125(2), 175–177.
Mihai, M., Spunei, M., & Malaescu, I. (2014). Comparison features for proton and heavy ion beams versus photon and electron beams. Romanian Reports in Physics, 66(1), 212–222.
Flejmer, A. M., Nyström, P. W., Dohlmar, F., Josefsson, D., & Dasu, A. (2015). Potential benefit of scanned proton beam versus photons as adjuvant radiation therapy in breast cancer. International Journal of Particle Therapy, 1(4), 845–855.
Hogstrom, K. R., & Almond, P. R. (2006). Review of electron beam therapy physics. Physics in Medicine & Biology, 51(13), R455–R489.
Salem, A., Mohamad, I., Dayyat, A., Kanaa’n, H., Sarhan, N., Roujob, I., Salem, A. F., Afifi, S., Jaradat, I., Mubiden, R., & Almousa, A. (2015). Combined photon-electron beams in the treatment of the supraclavicular lymph nodes in breast cancer: a novel technique that achieves adequate coverage while reducing lung dose. Medical Dosimetry, 40(3), 210–217.
Schulz-Ertner, D., & Tsujii, H. (2007). Particle radiation therapy using proton and heavier ion beams. Journal of Clinical Oncology, 25(8), 953–964.
Borrego-Soto, G., Ortiz-López, R., & Rojas-Martínez, A. (2015). Ionizing radiation-induced DNA injury and damage detection in patients with breast cancer. Genetics and Molecular Biology, 38(4), 420–432.
Mahaney, B. L., Meek, K., & Lees-Miller, S. P. (2009). Repair of ionizing radiation-induced DNA double-strand breaks by non-homologous end-joining. Biochemical Journal, 417(3), 639–650.
Valastyan, S., & Weinberg, R. A. (2011). Tumor metastasis: molecular insights and evolving paradigms. Cell, 147(2), 275–292.
Chiang, S. P., Cabrera, R. M., & Segall, J. E. (2016). Tumor cell intravasation. American Journal of Physiology-Cell Physiology, 311(1), C1–C14.
Izdebska, M., Zielińska, W., Grzanka, D., & Gagat, M. (2018). The role of actin dynamics and actin-binding proteins expression in epithelial-to-mesenchymal transition and its association with cancer progression and evaluation of possible therapeutic targets. BioMed Research International, 2018, 1–13.
Wang, W., Liu, Y., & Liao, K. (2011). Tyrosine phosphorylation of cortactin by the FAK-Src complex at focal adhesions regulates cell motility. BMC Cell Biology, 12(1), 49.
Sit, S.-T., & Manser, E. (2011). Rho GTPases and their role in organizing the actin cytoskeleton. Journal of Cell Science, 124(5), 679–683.
Stephens, S. J., Moravan, M. J., & Salama, J. K. (2018). Managing patients with oligometastatic non–small-cell lung cancer. Journal of Oncology Practice, 14(1), 23–31.
Ordoñez, R., Otero, A., Jerez, I., Medina, J. A., Lupiañez-Pérez, Y., & Gomez-Millan, J. (2019). Role of radiotherapy in the treatment of metastatic head and neck cancer. Oncotargets and Therapy, 12, 677–683.
Lutz, S. T., Jones, J., & Chow, E. (2014). Role of radiation therapy in palliative care of the patient with cancer. Journal of Clinical Oncology, 32(26), 2913–2919.
Dillekås, H., Rogers, M. S., & Straume, O. (2019). Are 90% of deaths from cancer caused by metastases? Cancer Medicine, 8(12), 5574–5576.
Kim, M.-J., Byun, J.-Y., Yun, C.-H., Park, I.-C., Lee, K.-H., & Lee, S.-J. (2008). c-Src-p38 mitogen-activated protein kinase signaling is required for Akt activation in response to ionizing radiation. Molecular Cancer Research, 6(12), 1872–1880.
Yan, Y., Greer, P. M., Cao, P. T., Kolb, R. H., & Cowan, K. H. (2012). RAC1 GTPase plays an important role in γ-irradiation induced G 2/M checkpoint activation. Breast Cancer Research, 14(2), R60.
Yan, Y., Hein, A. L., Etekpo, A., Burchett, K. M., Lin, C., Enke, C. A., Batra, S. K., Cowan, K. H., & Ouellette, M. M. (2014). Inhibition of RAC1 GTPase sensitizes pancreatic cancer cells to γ-irradiation. Oncotarget, 5(21), 10251–10270.
Skvortsov, S., Dudas, J., Eichberger, P., Witsch-Baumgartner, M., Loeffler-Ragg, J., Pritz, C., et al. (2014). Rac1 as a potential therapeutic target for chemo-radioresistant head and neck squamous cell carcinomas (HNSCC). British Journal of Cancer, 110(11), 2677–2687.
Espinha, G., Osaki, J. H., Magalhaes, Y. T., & Forti, F. L. (2015). Rac1 GTPase-deficient HeLa cells present reduced DNA repair, proliferation, and survival under UV or gamma irradiation. Molecular and Cellular Biochemistry, 404(1–2), 281–297.
Hein, A. L., Post, C. M., Sheinin, Y. M., Lakshmanan, I., Natarajan, A., Enke, C. A., Batra, S. K., Ouellette, M. M., & Yan, Y. (2016). RAC1 GTPase promotes the survival of breast cancer cells in response to hyper-fractionated radiation treatment. Oncogene, 35(49), 6319–6329.
Zhou, T., Wang, C. H., Yan, H., Zhang, R., Zhao, J. B., Qian, C. F., et al. (2016). Inhibition of the Rac1-WAVE2-Arp2/3 signaling pathway promotes radiosensitivity via downregulation of cofilin-1 in U251 human glioma cells. Molecular Medicine Reports, 13(5), 4414–4420.
Zhou, Y., Liao, Q., Han, Y., Chen, J., Liu, Z., Ling, H., Zhang, J., Yang, W., Oyang, L., Xia, L., Wang, L., Wang, H., Xue, L., Wang, H., & Hu, B. (2016). Rac1 overexpression is correlated with epithelial mesenchymal transition and predicts poor prognosis in non-small cell lung cancer. Journal of Cancer, 7(14), 2100–2109.
Choi, S.-Y., Kim, M.-J., Kang, C.-M., Bae, S., Cho, C.-K., Soh, J.-W., Kim, J. H., Kang, S., Chung, H. Y., Lee, Y. S., & Lee, S. J. (2006). Activation of Bak and Bax through c-abl-protein kinase Cδ-p38 MAPK signaling in response to ionizing radiation in human non-small cell lung cancer cells. Journal of Biological Chemistry, 281(11), 7049–7059.
Duan, W., Xu, Y., Dong, Y., Cao, L., Tong, J., & Zhou, X. (2013). Ectopic expression of miR-34a enhances radiosensitivity of non-small cell lung cancer cells, partly by suppressing the LyGDI signaling pathway. Journal of Radiation Research, 54(4), 611–619.
Wang, C., Pan, Z., Hou, H., Li, D., Mo, Y., Mo, C., & Li, J. (2016). The enhancement of radiation sensitivity in nasopharyngeal carcinoma cells via activation of the Rac1/NADPH signaling pathway. Radiation Research, 185(6), 638–646.
Su, Z., Li, Z., Wang, C., Tian, W., Lan, F., Liang, D., Li, J., Li, D., & Hou, H. (2019). A novel Rhein derivative: activation of Rac1/NADPH pathway enhances sensitivity of nasopharyngeal carcinoma cells to radiotherapy. Cellular Signalling, 54, 35–45.
Zhao, M., Chen, L., Xiao, Y., Xiao, H., & Liu, H. (2019). Impact on U251 glioma cell radiosensitivity and CFL1 level via inhibiting cell motility regulator ROCKII of RhoA-RockII-CFL1 pathway. American Society of Clinical Oncology, 37:15_suppl, e14630–e14630.
McLaughlin, N., Annabi, B., Bouzeghrane, M., Temme, A., Bahary, J.-P., Moumdjian, R., & Béliveau, R. (2006). The Survivin-mediated radioresistant phenotype of glioblastomas is regulated by RhoA and inhibited by the green tea polyphenol (−)-epigallocatechin-3-gallate. Brain Research, 1071(1), 1–9.
Ader, I., Toulas, C., Dalenc, F., Delmas, C., Bonnet, J., Cohen-Jonathan, E., & Favre, G. (2002). RhoB controls the 24 kDa FGF-2-induced radioresistance in HeLa cells by preventing post-mitotic cell death. Oncogene, 21(39), 5998–6006.
Ader, I., Delmas, C., Bonnet, J., Rochaix, P., Favre, G., Toulas, C., & Cohen-Jonathan-Moyal, E. (2003). Inhibition of Rho pathways induces radiosensitization and oxygenation in human glioblastoma xenografts. Oncogene, 22(55), 8861–8869.
Delmas, C., Heliez, C., Cohen-Jonathan, E., End, D., Bonnet, J., Favre, G., & Toulas, C. (2002). Farnesyltransferase inhibitor, R115777, reverses the resistance of human glioma cell lines to ionizing radiation. International Journal of Cancer, 100(1), 43–48.
Monferran, S., Skuli, N., Delmas, C., Favre, G., Bonnet, J., Cohen-Jonathan-Moyal, E., & Toulas, C. (2008). Alphavbeta3 and alphavbeta5 integrins control glioma cell response to ionising radiation through ILK and RhoB. International Journal of Cancer, 123(2), 357–364. https://doi.org/10.1002/ijc.23498.
Liu, N., Cui, W., Jiang, X., Zhang, Z., Gnosa, S., Ali, Z., et al. (2019). The critical role of dysregulated RhoB signaling pathway in radioresistance of colorectal cancer. International Journal of Radiation Oncology* Biology* Physics, 104(5), 1153–1164..
Luis-Ravelo, D., Antón, I., Zandueta, C., Valencia, K., Pajares, M.-J., Agorreta, J., Montuenga, L., Vicent, S., Wistuba, I. I., de Las Rivas, J., & Lecanda, F. (2014). RHOB influences lung adenocarcinoma metastasis and resistance in a host-sensitive manner. Molecular Oncology, 8(2), 196–206.
Liu, A.-x., Cerniglia, G. J., Bernhard, E. J., & Prendergast, G. C. (2001). RhoB is required to mediate apoptosis in neoplastically transformed cells after DNA damage. Proceedings of the National Academy of Sciences, 98(11), 6192–6197.
Kim, C.-H., Won, M., Choi, C.-H., Ahn, J., Kim, B.-K., Song, K.-B., Kang, C. M., & Chung, K. S. (2010). Increase of RhoB in γ-radiation-induced apoptosis is regulated by c-Jun N-terminal kinase in Jurkat T cells. Biochemical and Biophysical Research Communications, 391(2), 1182–1186.
Skvortsov, S., Debbage, P., Cho, W. C., Lukas, P., & Skvortsova, I. (2014). Putative biomarkers and therapeutic targets associated with radiation resistance. Expert Review of Proteomics, 11(2), 207–214.
Skvortsov, S., Jimenez, C. R., Knol, J. C., Eichberger, P., Schiestl, B., Debbage, P., Skvortsova, I., & Lukas, P. (2011). Radioresistant head and neck squamous cell carcinoma cells: intracellular signaling, putative biomarkers for tumor recurrences and possible therapeutic targets. Radiotherapy and Oncology, 101(1), 177–182.
Osaki, J. H., Espinha, G., Magalhaes, Y. T., & Forti, F. L. (2016). Modulation of RhoA GTPase activity sensitizes human cervix carcinoma cells to γ-radiation by attenuating DNA repair pathways. Oxidative Medicine and Cellular Longevity, 2016, 1–11.
Ju, J., & Gilkes, D. (2018). RhoB: team oncogene or team tumor suppressor? Genes, 9(2), 67.
Toulany, M. (2019). Targeting DNA double-strand break repair pathways to improve radiotherapy response. Genes (Basel), 10(1). https://doi.org/10.3390/genes10010025.
Lee, J., & Paull, T. T. (2007). Activation and regulation of ATM kinase activity in response to DNA double-strand breaks. Oncogene, 26(56), 7741–7748.
Marampon, F., Ciccarelli, C., & Zani, B. M. (2019). Biological rationale for targeting MEK/ERK pathways in anti-cancer therapy and to potentiate tumour responses to radiation. International Journal of Molecular Sciences, 20(10), 2530. https://doi.org/10.3390/ijms20102530.
Bai, M., Ma, X., Li, X., Wang, X., Mei, Q., Li, X., Wu, Z., & Han, W. (2015). The accomplices of NF-κB lead to radioresistance. Current Protein & Peptide Science, 16(4), 279–294. https://doi.org/10.2174/138920371604150429152328.
Yan, H., Yang, K., Xiao, H., Zou, Y. J., Zhang, W. B., & Liu, H. Y. (2012). Over-expression of cofilin-1 and phosphoglycerate kinase 1 in astrocytomas involved in pathogenesis of radioresistance. CNS Neuroscience & Therapeutics, 18(9), 729–736.
Leu, J.-D., Chiu, Y.-W., Lo, C.-C., Chiang, P.-H., Chiu, S.-J., Tsai, C.-H., Hwang, J. J., Chen, R. C., Gorbunova, V., & Lee, Y. J. (2013). Enhanced cellular radiosensitivity induced by cofilin-1 over-expression is associated with reduced DNA repair capacity. International Journal of Radiation Biology, 89(6), 433–444.
Ishikawa, K., Ishii, H., & Saito, T. (2006). DNA damage-dependent cell cycle checkpoints and genomic stability. DNA and Cell Biology, 25(7), 406–411.
Lu, Q., Insinna, C., Ott, C., Stauffer, J., Pintado, P. A., Rahajeng, J., Baxa, U., Walia, V., Cuenca, A., Hwang, Y. S., Daar, I. O., Lopes, S., Lippincott-Schwartz, J., Jackson, P. K., Caplan, S., & Westlake, C. J. (2015). Early steps in primary cilium assembly require EHD1/EHD3-dependent ciliary vesicle formation. Nature Cell Biology, 17(3), 228–240.
Van Laethem, A., Van Kelst, S., Lippens, S., Declercq, W., Vandenabeele, P., Janssens, S., et al. (2004). Activation of p38 MAPK is required for Bax translocation to mitochondria, cytochrome c release and apoptosis induced by UVB irradiation in human keratinocytes. FASEB Journal : Official Publication of the Federation of American Societies for Experimental Biology, 18(15), 1946–1948. https://doi.org/10.1096/fj.04-2285fje.
Oh, W., & Frost, J. A. (2014). Rho gtpase independent regulation of atm activation and cell survival by the rhogef net1a. Cell Cycle, 13(17), 2765–2772.
Skuli, N., Monferran, S., Delmas, C., Lajoie-Mazenc, I., Favre, G., Toulas, C., & Cohen-Jonathan-Moyal, E. (2006). Activation of RhoB by hypoxia controls hypoxia-inducible factor-1α stabilization through glycogen synthase kinase-3 in U87 glioblastoma cells. Cancer Research, 66(1), 482–489.
Xia, Y., Jiang, L., & Zhong, T. (2018). The role of HIF-1α in chemo-/radioresistant tumors. Oncotargets and Therapy, 11, 3003–3011.
Pei, H., Zhang, J., Nie, J., Ding, N., Hu, W., Hua, J., Hirayama, R., Furusawa, Y., Liu, C., Li, B., Hei, T. K., & Zhou, G. (2017). RAC2-P38 MAPK-dependent NADPH oxidase activity is associated with the resistance of quiescent cells to ionizing radiation. Cell Cycle, 16(1), 113–122.
Pranatharthi, A., Thomas, P., Udayashankar, A. H., Bhavani, C., Suresh, S. B., Krishna, S., et al. (2019). RhoC regulates radioresistance via crosstalk of ROCK2 with the DNA repair machinery in cervical cancer. Journal of Experimental & Clinical Cancer Research, 38(1), 1–24.
Moharil, R. B., Dive, A., Khandekar, S., & Bodhade, A. (2017). Cancer stem cells: an insight. Journal of Oral and Maxillofacial Pathology, 21(3), 463. https://doi.org/10.4103/jomfp.JOMFP_132_16.
Maugeri-Saccà, M., Bartucci, M., & De Maria, R. (2012). DNA damage repair pathways in cancer stem cells. Molecular Cancer Therapeutics, 11(8), 1627–1636. https://doi.org/10.1158/1535-7163.Mct-11-1040.
Ding, S., Li, C., Cheng, N., Cui, X., Xu, X., & Zhou, G. (2015). Redox regulation in cancer stem cells. Oxidative Medicine and Cellular Longevity, 2015, 750798–750711. https://doi.org/10.1155/2015/750798.
Chen, W., Dong, J., Haiech, J., Kilhoffer, M. C., & Zeniou, M. (2016). Cancer stem cell quiescence and plasticity as major challenges in cancer therapy. Stem Cells International, 2016, 1740936–1740916. https://doi.org/10.1155/2016/1740936.
Schulz, A., Meyer, F., Dubrovska, A., & Borgmann, K. (2019). Cancer stem cells and radioresistance: DNA repair and beyond. Cancers (Basel), 11(6). https://doi.org/10.3390/cancers11060862.
Krause, M., Dubrovska, A., Linge, A., & Baumann, M. (2017). Cancer stem cells: radioresistance, prediction of radiotherapy outcome and specific targets for combined treatments. Advanced Drug Delivery Reviews, 109, 63–73. https://doi.org/10.1016/j.addr.2016.02.002.
Jiang, Z. B., Ma, B. Q., Liu, S. G., Li, J., Yang, G. M., Hou, Y. B., Si, R. H., Gao, P., & Yan, H. T. (2019). miR-365 regulates liver cancer stem cells via RAC1 pathway. Molecular Carcinogenesis, 58(1), 55–65. https://doi.org/10.1002/mc.22906.
Chen, S., Li, H., Li, S., Yu, J., Wang, M., Xing, H., Tang, K., Tian, Z., Rao, Q., & Wang, J. (2016). Rac1 GTPase promotes interaction of hematopoietic stem/progenitor cell with niche and participates in leukemia initiation and maintenance in mouse. Stem Cells, 34(7), 1730–1741. https://doi.org/10.1002/stem.2348.
Yoon, C., Cho, S. J., Chang, K. K., Park, D. J., Ryeom, S. W., & Yoon, S. S. (2017). Role of Rac1 pathway in epithelial-to-mesenchymal transition and cancer stem-like cell phenotypes in gastric adenocarcinoma. Molecular Cancer Research, 15(8), 1106–1116. https://doi.org/10.1158/1541-7786.Mcr-17-0053.
Yoon, C. H., Hyun, K. H., Kim, R. K., Lee, H., Lim, E. J., Chung, H. Y., An, S., Park, M. J., Suh, Y., Kim, M. J., & Lee, S. J. (2011). The small GTPase Rac1 is involved in the maintenance of stemness and malignancies in glioma stem-like cells. FEBS Letters, 585(14), 2331–2338. https://doi.org/10.1016/j.febslet.2011.05.070.
Yoon, C., Cho, S. J., Aksoy, B. A., Park, D. J., Schultz, N., Ryeom, S. W., & Yoon, S. S. (2016). Chemotherapy resistance in diffuse-type gastric adenocarcinoma is mediated by RhoA activation in cancer stem-like cells. Clinical Cancer Research, 22(4), 971–983. https://doi.org/10.1158/1078-0432.Ccr-15-1356.
Nandy, S. B., Orozco, A., Lopez-Valdez, R., Roberts, R., Subramani, R., Arumugam, A., Dwivedi, A. K., Stewart, V., Prabhakar, G., Jones, S., & Lakshmanaswamy, R. (2017). Glucose insult elicits hyperactivation of cancer stem cells through miR-424-cdc42-prdm14 signalling axis. British Journal of Cancer, 117(11), 1665–1675. https://doi.org/10.1038/bjc.2017.335.
Dong, Z., Yu, C., Rezhiya, K., Gulijiahan, A., & Wang, X. (2019). Downregulation of miR-146a promotes tumorigenesis of cervical cancer stem cells via VEGF/CDC42/PAK1 signaling pathway. Artificial Cells, Nanomedicine, and Biotechnology, 47(1), 3711–3719. https://doi.org/10.1080/21691401.2019.1664560.
Binker, M. G., Binker-Cosen, A. A., Richards, D., Oliver, B., & Cosen-Binker, L. I. (2009). EGF promotes invasion by PANC-1 cells through Rac1/ROS-dependent secretion and activation of MMP-2. Biochemical and Biophysical Research Communications, 379(2), 445–450. https://doi.org/10.1016/j.bbrc.2008.12.080.
Kang, M. A., So, E. Y., Simons, A. L., Spitz, D. R., & Ouchi, T. (2012). DNA damage induces reactive oxygen species generation through the H2AX-Nox1/Rac1 pathway. Cell Death & Disease, 3(1), e249. https://doi.org/10.1038/cddis.2011.134.
Diebold, B. A., Fowler, B., Lu, J., Dinauer, M. C., & Bokoch, G. M. (2004). Antagonistic cross-talk between Rac and Cdc42 GTPases regulates generation of reactive oxygen species. The Journal of Biological Chemistry, 279(27), 28136–28142. https://doi.org/10.1074/jbc.M313891200.
Aghajanian, A., Wittchen, E. S., Campbell, S. L., & Burridge, K. (2009). Direct activation of RhoA by reactive oxygen species requires a redox-sensitive motif. PLoS One, 4(11), e8045. https://doi.org/10.1371/journal.pone.0008045.
Zhu, W., Ma, L., Yang, B., Zheng, Z., Chai, R., Liu, T., Liu, Z., Song, T., Li, F., & Li, G. (2016). Flavone inhibits migration through DLC1/RhoA pathway by decreasing ROS generation in breast cancer cells. In Vitro Cellular & Developmental Biology. Animal, 52(5), 589–597. https://doi.org/10.1007/s11626-016-0010-8.
MacKay, C. E., Shaifta, Y., Snetkov, V. V., Francois, A. A., Ward, J. P. T., & Knock, G. A. (2017). ROS-dependent activation of RhoA/Rho-kinase in pulmonary artery: role of Src-family kinases and ARHGEF1. Free Radical Biology & Medicine, 110, 316–331. https://doi.org/10.1016/j.freeradbiomed.2017.06.022.
Chung, K. S., Han, G., Kim, B. K., Kim, H. M., Yang, J. S., Ahn, J., Lee, K., Song, K. B., & Won, M. (2013). A novel antitumor piperazine alkyl compound causes apoptosis by inducing RhoB expression via ROS-mediated c-Abl/p38 MAPK signaling. Cancer Chemotherapy and Pharmacology, 72(6), 1315–1324. https://doi.org/10.1007/s00280-013-2310-y.
Pan, J., She, M., Xu, Z. X., Sun, L., & Yeung, S. C. (2005). Farnesyltransferase inhibitors induce DNA damage via reactive oxygen species in human cancer cells. Cancer Research, 65(9), 3671–3681. https://doi.org/10.1158/0008-5472.Can-04-2744.
Wu, W., & Zhao, S. (2013). Metabolic changes in cancer: beyond the Warburg effect. Acta Biochimica et Biophysica Sinica, 45(1), 18–26. https://doi.org/10.1093/abbs/gms104.
Sharma, A., Boise, L. H., & Shanmugam, M. (2019). Cancer metabolism and the evasion of apoptotic cell death. Cancers (Basel), 11(8). https://doi.org/10.3390/cancers11081144.
Shimura, T., Noma, N., Sano, Y., Ochiai, Y., Oikawa, T., Fukumoto, M., & Kunugita, N. (2014). AKT-mediated enhanced aerobic glycolysis causes acquired radioresistance by human tumor cells. Radiotherapy and Oncology, 112(2), 302–307. https://doi.org/10.1016/j.radonc.2014.07.015.
Meng, M. B., Wang, H. H., Guo, W. H., Wu, Z. Q., Zeng, X. L., Zaorsky, N. G., et al. (2015). Targeting pyruvate kinase M2 contributes to radiosensitivity of non-small cell lung cancer cells in vitro and in vivo. Cancer Letters, 356(2 Pt B), 985–993. https://doi.org/10.1016/j.canlet.2014.11.016.
Zhong, J. T., & Zhou, S. H. (2017). Warburg effect, hexokinase-II, and radioresistance of laryngeal carcinoma. Oncotarget, 8(8), 14133–14146. https://doi.org/10.18632/oncotarget.13044.
Isebaert, S. F., Swinnen, J. V., McBride, W. H., Begg, A. C., & Haustermans, K. M. (2011). 5-aminoimidazole-4-carboxamide riboside enhances effect of ionizing radiation in PC3 prostate cancer cells. International Journal of Radiation Oncology, Biology, Physics, 81(5), 1515–1523. https://doi.org/10.1016/j.ijrobp.2011.06.1964.
Efimova, E. V., Takahashi, S., Shamsi, N. A., Wu, D., Labay, E., Ulanovskaya, O. A., Weichselbaum, R. R., Kozmin, S. A., & Kron, S. J. (2016). Linking cancer metabolism to DNA repair and accelerated senescence. Molecular Cancer Research, 14(2), 173–184. https://doi.org/10.1158/1541-7786.Mcr-15-0263.
Lee, M., & Yoon, J. H. (2015). Metabolic interplay between glycolysis and mitochondrial oxidation: the reverse Warburg effect and its therapeutic implication. World Journal of Biological Chemistry, 6(3), 148–161. https://doi.org/10.4331/wjbc.v6.i3.148.
Fischer, K., Hoffmann, P., Voelkl, S., Meidenbauer, N., Ammer, J., Edinger, M., Gottfried, E., Schwarz, S., Rothe, G., Hoves, S., Renner, K., Timischl, B., Mackensen, A., Kunz-Schughart, L., Andreesen, R., Krause, S. W., & Kreutz, M. (2007). Inhibitory effect of tumor cell-derived lactic acid on human T cells. Blood, 109(9), 3812–3819. https://doi.org/10.1182/blood-2006-07-035972.
Zeng, R. J., Zheng, C. W., Gu, J. E., Zhang, H. X., Xie, L., Xu, L. Y., & Li, E. M. (2019). RAC1 inhibition reverses cisplatin resistance in esophageal squamous cell carcinoma and induces downregulation of glycolytic enzymes. Molecular Oncology, 13(9), 2010–2030. https://doi.org/10.1002/1878-0261.12548.
Yang, Y., Du, J., Hu, Z., Liu, J., Tian, Y., Zhu, Y., et al. (2011). Activation of Rac1-PI3K/Akt is required for epidermal growth factor-induced PAK1 activation and cell migration in MDA-MB-231 breast cancer cells. Journal of Biomedical Research, 25(4), 237–245. https://doi.org/10.1016/s1674-8301(11)60032-8.
Zhang, C., Liu, J., Liang, Y., Wu, R., Zhao, Y., Hong, X., Lin, M., Yu, H., Liu, L., Levine, A. J., Hu, W., & Feng, Z. (2013). Tumour-associated mutant p53 drives the Warburg effect. Nature Communications, 4, 2935. https://doi.org/10.1038/ncomms3935.
Baxter, E., Windloch, K., Gannon, F., & Lee, J. S. (2014). Epigenetic regulation in cancer progression. Cell & Bioscience, 4, 45. https://doi.org/10.1186/2045-3701-4-45.
Chen, Q. W., Zhu, X. Y., Li, Y. Y., & Meng, Z. Q. (2014). Epigenetic regulation and cancer (review). Oncology Reports, 31(2), 523–532. https://doi.org/10.3892/or.2013.2913.
Wan, J., Su, Y., Song, Q., Tung, B., Oyinlade, O., Liu, S., et al. (2017). Methylated cis-regulatory elements mediate KLF4-dependent gene transactivation and cell migration. Elife, 6. https://doi.org/10.7554/eLife.20068.
Dopeso, H., Rodrigues, P., Bilic, J., Bazzocco, S., Cartón-García, F., Macaya, I., de Marcondes, P. G., Anguita, E., Masanas, M., Jiménez-Flores, L. M., Martínez-Barriocanal, Á., Nieto, R., Segura, M. F., Schwartz Jr, S., Mariadason, J. M., & Arango, D. (2018). Mechanisms of inactivation of the tumour suppressor gene RHOA in colorectal cancer. British Journal of Cancer, 118(1), 106–116. https://doi.org/10.1038/bjc.2017.420.
Mazières, J., Tovar, D., He, B., Nieto-Acosta, J., Marty-Detraves, C., Clanet, C., Pradines, A., Jablons, D., & Favre, G. (2007). Epigenetic regulation of RhoB loss of expression in lung cancer. BMC Cancer, 7, 220. https://doi.org/10.1186/1471-2407-7-220.
Gómez Del Pulgar, T., Valdés-Mora, F., Bandrés, E., Pérez-Palacios, R., Espina, C., Cejas, P., et al. (2008). Cdc42 is highly expressed in colorectal adenocarcinoma and downregulates ID4 through an epigenetic mechanism. International Journal of Oncology, 33(1), 185–193.
Barrio-Real, L., Benedetti, L. G., Engel, N., Tu, Y., Cho, S., Sukumar, S., & Kazanietz, M. G. (2014). Subtype-specific overexpression of the Rac-GEF P-REX1 in breast cancer is associated with promoter hypomethylation. Breast Cancer Research, 16(5), 441. https://doi.org/10.1186/s13058-014-0441-7.
Kasuya, K., Nagakawa, Y., Hosokawa, Y., Sahara, Y., Takishita, C., Nakajima, T., et al. (2016). RhoA activity increases due to hypermethylation of ARHGAP28 in a highly liver-metastatic colon cancer cell line. Biomedical Reports, 4(3), 335–339. https://doi.org/10.3892/br.2016.582.
Delarue, F. L., Adnane, J., Joshi, B., Blaskovich, M. A., Wang, D. A., Hawker, J., Bizouarn, F., Ohkanda, J., Zhu, K., Hamilton, A. D., Chellappan, S., & Sebti, S. M. (2007). Farnesyltransferase and geranylgeranyltransferase I inhibitors upregulate RhoB expression by HDAC1 dissociation, HAT association and histone acetylation of the RhoB promoter. Oncogene, 26(5), 633–640. https://doi.org/10.1038/sj.onc.1209819.
Wahid, F., Shehzad, A., Khan, T., & Kim, Y. Y. (2010). MicroRNAs: synthesis, mechanism, function, and recent clinical trials. Biochimica et Biophysica Acta, 1803(11), 1231–1243. https://doi.org/10.1016/j.bbamcr.2010.06.013.
Wang, P., Chen, L., Zhang, J., Chen, H., Fan, J., Wang, K., Luo, J., Chen, Z., Meng, Z., & Liu, L. (2014). Methylation-mediated silencing of the miR-124 genes facilitates pancreatic cancer progression and metastasis by targeting Rac1. Oncogene, 33(4), 514–524. https://doi.org/10.1038/onc.2012.598.
Ge, F., Wang, C., Wang, W., Liu, W., & Wu, B. (2017). MicroRNA-31 inhibits tumor invasion and metastasis by targeting RhoA in human gastric cancer. Oncology Reports, 38(2), 1133–1139. https://doi.org/10.3892/or.2017.5758.
Niu, S., Ma, X., Zhang, Y., Liu, Y. N., Chen, X., Gong, H., Yao, Y., Liu, K., & Zhang, X. (2018). MicroRNA-19a and microRNA-19b promote the malignancy of clear cell renal cell carcinoma through targeting the tumor suppressor RhoB. PLoS One, 13(2), e0192790. https://doi.org/10.1371/journal.pone.0192790.
Ke, T. W., Hsu, H. L., Wu, Y. H., Chen, W. T., Cheng, Y. W., & Cheng, C. W. (2014). MicroRNA-224 suppresses colorectal cancer cell migration by targeting Cdc42. Disease Markers, 2014, 617150–617111. https://doi.org/10.1155/2014/617150.
Mishima, T., Naotsuka, M., Horita, Y., Sato, M., Ohashi, K., & Mizuno, K. (2010). LIM-kinase is critical for the mesenchymal-to-amoeboid cell morphological transition in 3D matrices. Biochemical and Biophysical Research Communications, 392(4), 577–581.
Yamazaki, D., Kurisu, S., & Takenawa, T. (2009). Involvement of Rac and Rho signaling in cancer cell motility in 3D substrates. Oncogene, 28(13), 1570–1583.
Zhang, Y., & Weinberg, R. A. (2018). Epithelial-to-mesenchymal transition in cancer: complexity and opportunities. Frontiers of Medicine, 12(4), 361–373.
Algayadh, I. G., Dronamraju, V., & Sylvester, P. W. (2016). Role of Rac1/WAVE2 signaling in mediating the inhibitory effects of γ-tocotrienol on mammary cancer cell migration and invasion. Biological and Pharmaceutical Bulletin, 39(12), 1974–1982.
Deng, Q., Tian, Y.-X., & Liang, J. (2018). Mangiferin inhibits cell migration and invasion through Rac1/WAVE2 signalling in breast cancer. Cytotechnology, 70(2), 593–601.
Takenawa, T., & Miki, H. (2001). WASP and WAVE family proteins: key molecules for rapid rearrangement of cortical actin filaments and cell movement. Journal of Cell Science, 114(10), 1801–1809.
Liu, C., Zhang, L., Cui, W., Du, J., Li, Z., Pang, Y., et al. (2019). Epigenetically upregulated GEFT-derived invasion and metastasis of rhabdomyosarcoma via epithelial mesenchymal transition promoted by the Rac1/Cdc42-PAK signalling pathway. EBioMedicine, 50, 122–134.
Fan, G. (2018). FER mediated HGF-independent regulation of HGFR/MET activates RAC1-PAK1 pathway to potentiate metastasis in ovarian cancer. Small GTPases, 11(3), 155–159.
Fang, D., Chen, H., Zhu, J. Y., Wang, W., Teng, Y., Ding, H.-F., Jing, Q., Su, S. B., & Huang, S. (2017). Epithelial–mesenchymal transition of ovarian cancer cells is sustained by Rac1 through simultaneous activation of MEK1/2 and Src signaling pathways. Oncogene, 36(11), 1546–1558.
Zhang, C., Guo, F., Xu, G., Ma, J., & Shao, F. (2015). STAT3 cooperates with Twist to mediate epithelial-mesenchymal transition in human hepatocellular carcinoma cells. Oncology Reports, 33(4), 1872–1882.
Zhou, K., Rao, J., Zhou, Z.-H., Yao, X.-H., Wu, F., Yang, J., et al. (2018). RAC1-GTP promotes epithelial-mesenchymal transition and invasion of colorectal cancer by activation of STAT3. Laboratory Investigation, 98(8), 989–998.
Jiang, K., Lu, Q., Li, Q., Ji, Y., Chen, W., & Xue, X. (2017). Astragaloside IV inhibits breast cancer cell invasion by suppressing Vav3 mediated Rac1/MAPK signaling. International Immunopharmacology, 42, 195–202.
Liu, Y., Cheng, Z., Pan, F., & Yan, W. (2017). MicroRNA-373 promotes growth and cellular invasion in osteosarcoma cells by activation of the PI3K/AKT-Rac1-JNK pathway: the potential role in spinal osteosarcoma. Oncology Research Featuring Preclinical and Clinical Cancer Therapeutics, 25(6), 989–999.
Sipes, N. S., Feng, Y., Guo, F., Lee, H.-O., Chou, F.-S., Cheng, J., Mulloy, J., & Zheng, Y. (2011). Cdc42 regulates extracellular matrix remodeling in three dimensions. Journal of Biological Chemistry, 286(42), 36469–36477.
Gadea, G., Sanz-Moreno, V., Self, A., Godi, A., & Marshall, C. J. (2008). DOCK10-mediated Cdc42 activation is necessary for amoeboid invasion of melanoma cells. Current Biology, 18(19), 1456–1465.
Wilkinson, S., Paterson, H. F., & Marshall, C. J. (2005). Cdc42–MRCK and Rho–ROCK signalling cooperate in myosin phosphorylation and cell invasion. Nature Cell Biology, 7(3), 255–261.
Matsuoka, T., & Yashiro, M. (2014). Rho/ROCK signaling in motility and metastasis of gastric cancer. World journal of gastroenterology: WJG, 20(38), 13756–13766.
Wei, L., Surma, M., Shi, S., Lambert-Cheatham, N., & Shi, J. (2016). Novel insights into the roles of Rho kinase in cancer. Archivum Immunologiae et Therapiae Experimentalis, 64(4), 259–278.
Campbell, H., Fleming, N., Roth, I., Mehta, S., Wiles, A., Williams, G., et al. (2018). ∆ 133p53 isoform promotes tumour invasion and metastasis via interleukin-6 activation of JAK-STAT and RhoA-ROCK signalling. Nature Communications, 9(1), 254.
Amano, M., Nakayama, M., & Kaibuchi, K. (2010). Rho-kinase/ROCK: a key regulator of the cytoskeleton and cell polarity. Cytoskeleton, 67(9), 545–554.
Hwang, S. Y., Jung, J. W., Jeong, J. S., Kim, Y. J., Oh, E. S., Kim, T. H., Kim, J. Y., Cho, K. H., & Han, I. O. (2006). Dominant-negative Rac increases both inherent and ionizing radiation-induced cell migration in C6 rat glioma cells. International Journal of Cancer, 118(8), 2056–2063.
Hamalukic, M., Huelsenbeck, J., Schad, A., Wirtz, S., Kaina, B., & Fritz, G. (2011). Rac1-regulated endothelial radiation response stimulates extravasation and metastasis that can be blocked by HMG-CoA reductase inhibitors. PLoS One, 6(10), e26413.
Murata, K., Noda, S.-E., Oike, T., Takahashi, A., Yoshida, Y., Suzuki, Y., et al. (2014). Increase in cell motility by carbon ion irradiation via the Rho signaling pathway and its inhibition by the ROCK inhibitor Y-27632 in lung adenocarcinoma A549 cells. Journal of Radiation Research, 55(4), 658–664.
Zhai, G. G., Malhotra, R., Delaney, M., Latham, D., Nestler, U., Zhang, M., Mukherjee, N., Song, Q., Robe, P., & Chakravarti, A. (2006). Radiation enhances the invasive potential of primary glioblastoma cells via activation of the Rho signaling pathway. Journal of Neuro-Oncology, 76(3), 227–237.
Fujita, M., Imadome, K., Endo, S., Shoji, Y., Yamada, S., & Imai, T. (2014). Nitric oxide increases the invasion of pancreatic cancer cells via activation of the PI3K–AKT and RhoA pathways after carbon ion irradiation. FEBS Letters, 588(17), 3240–3250.
Fujita, M., Otsuka, Y., Imadome, K., Endo, S., Yamada, S., & Imai, T. (2012). Carbon-ion radiation enhances migration ability and invasiveness of the pancreatic cancer cell, PANC-1, in vitro. Cancer Science, 103(4), 677–683.
Teng, Y., Xie, X., Walker, S., White, D. T., Mumm, J. S., & Cowell, J. K. (2013). Evaluating human cancer cell metastasis in zebrafish. BMC Cancer, 13(1), 453.
Zheng, C.-W., Zeng, R.-J., Xu, L.-Y., & Li, E.-M. (2020). Rho GTPases: promising candidates for overcoming chemotherapeutic resistance. Cancer Letters, 475, 65–78.
Duquette, P. M., & Lamarche-Vane, N. (2014). Rho GTPases in embryonic development. Small GTPases, 5(2), 8. https://doi.org/10.4161/sgtp.29716.
Sugihara, K., Nakatsuji, N., Nakamura, K., Nakao, K., Hashimoto, R., Otani, H., Sakagami, H., Kondo, H., Nozawa, S., Aiba, A., & Katsuki, M. (1998). Rac1 is required for the formation of three germ layers during gastrulation. Oncogene, 17(26), 3427–3433. https://doi.org/10.1038/sj.onc.1202595.
Takenaka, N., Nihata, Y., Ueda, S., & Satoh, T. (2017). In situ detection of the activation of Rac1 and RalA small GTPases in mouse adipocytes by immunofluorescent microscopy following in vivo and ex vivo insulin stimulation. Cellular Signalling, 39, 108–117. https://doi.org/10.1016/j.cellsig.2017.08.004.
Asahara, S., Shibutani, Y., Teruyama, K., Inoue, H. Y., Kawada, Y., Etoh, H., Matsuda, T., Kimura-Koyanagi, M., Hashimoto, N., Sakahara, M., Fujimoto, W., Takahashi, H., Ueda, S., Hosooka, T., Satoh, T., Inoue, H., Matsumoto, M., Aiba, A., Kasuga, M., & Kido, Y. (2013). Ras-related C3 botulinum toxin substrate 1 (RAC1) regulates glucose-stimulated insulin secretion via modulation of F-actin. Diabetologia, 56(5), 1088–1097. https://doi.org/10.1007/s00125-013-2849-5.
Sylow, L., Jensen, T. E., Kleinert, M., Højlund, K., Kiens, B., Wojtaszewski, J., et al. (2013). Rac1 signaling is required for insulin-stimulated glucose uptake and is dysregulated in insulin-resistant murine and human skeletal muscle. Diabetes, 62(6), 1865–1875. https://doi.org/10.2337/db12-1148.
Saoudi, A., Kassem, S., Dejean, A., & Gaud, G. (2014). Rho-GTPases as key regulators of T lymphocyte biology. Small GTPases, 5, e983862. https://doi.org/10.4161/sgtp.28208.
Funding
This work was supported by the Natural Science Foundation of China-Guangdong Joint Fund (U1601229), the Special Funds for the Cultivation of Guangdong College Students’ Scientific and Technological Innovation (“Climbing Program” Special Funds, pdjh2020a0218) and and the National Undergraduate Training Program for Innovation and Entrepreneurship (201810560037).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that there is no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zeng, RJ., Zheng, CW., Chen, WX. et al. Rho GTPases in cancer radiotherapy and metastasis. Cancer Metastasis Rev 39, 1245–1262 (2020). https://doi.org/10.1007/s10555-020-09923-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10555-020-09923-5