
Abstract
Radiation therapy (RT) continues to be one of the most popular treatment options for localized prostate cancer (CaP). Local CaP recurrence after RT is a pattern of treatment failure attributable to radioresistance of cancer cells. One major obstacle to RT is that there is a limit to the amount of radiation that can be safely delivered to the target organ. Recent results indicate that phosphoinositide 3-kinase (PI3K)/Akt/phosphatase and tensin homolog (PTEN)/mammalian target of rapamycin (mTOR) signaling pathway, autophagy, epithelial–mesenchymal transition (EMT) and cancer stem cells (CSCs) are involved in CaP metastasis and radioresistance. Emerging evidence also suggests that combining a radiosensitizer with RT increases the efficacy of CaP treatment. Understanding the mechanisms of radioresistance will help to overcome recurrence after RT in CaP patients and prevent metastasis. In this review, we discuss the novel findings of PI3K/Akt/PTEN/mTOR signaling pathway, autophagy, EMT and CSCs in the regulation of CaP metastasis and radioresistance, and focus on combination of radiosensitizers with RT in the treatment of CaP in preclinical studies to explore novel approaches for future clinical trials.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Prostate cancer (CaP) remains a significant medical burden in developed countries and accounts for an estimated 94,000 deaths in Europe in 2008 and 33,720 in the USA in 2011 [1]. Around 70 % of these patients present with organ-confined disease with the majority presenting with low- or intermediate-risk CaP [2]. The median 5-year disease-free survival rate for local stage T2 or locally advanced stage T3 CaP patients varies from 30 % to 90 % in different series. Despite increased awareness and earlier diagnosis, therapy with curative intent seems to fail to achieve long-term effect. The patients at early-stage disease can be treated effectively with androgen ablation treatment, surgery, or radiation therapy (RT). However, a significant portion of men are diagnosed with advanced stage/high-risk disease, and despite recent advances these patients can still relapse after definitive hormone treatment and/or RT [3] indicating that a resistant population of cancer cells may have survived the RT. One possible reason for these failures from RT may be due to the intrinsic radioresistance of a subpopulation of CaP clonogen within the tumor. When CaPs progress and metastasize, the tumors frequently become hormone refractory; classical chemotherapy regimens do not offer a curative approach.
Due to CaP relapse after RT, it is very important to optimize CaP treatments and investigate the mechanisms with regard to impacting radiosensitivity. Emerging data indicate that phosphoinositide 3-kinase (PI3K)/Akt/phosphatase and tensin homolog (PTEN)/mammalian target of rapamycin (mTOR) [4–6], autophagy [5, 7], epithelial–mesenchymal transition (EMT) [8, 9], and cancer stem cells (CSCs) [10–12] are involved in CaP metastasis, play very important roles in radioresistance and are believed to be the cause of tumor recurrence. Combination of a radiosensitizer with RT is promising to improve the efficacy of current RT approaches and overcome radioresistance in CaP patients.
Here, we discuss the roles of PI3K/Akt/PTEN/mTOR signaling pathway, autophagy, EMT, and CSCs on CaP metastasis and radioresistance. We also provide a comprehensive summary of radiosensitizers combined with RT in the treatment of CaP in vitro and in vivo to explore possible implications for future clinical trials. The combination of androgen deprivation (AD) with RT in CaP has been recently reviewed [13, 14] and will not be discussed in the current review.
2 Current obstacle in prostate cancer RT
Radical prostatectomy (RP) and RT including external beam radiotherapy (EBRT) and brachytherapy are the three main treatment options for organ-confined or locally advanced CaP. Their therapeutic efficacies are similar, being approximately 75–80 % for stages T1–T2 CaP [15]. While these primary therapies are associated with a high cancer control rate for the localized disease, up to a third of patients undergoing these therapies will have a biochemical recurrence (BCR) after local therapy [16, 17]. Doses used in EBRT or brachytherapy are highly associated with therapeutic efficacy; however, the incidences of related side effects increase as the dose of radiation increases [18].
It was reported that the fast neutron radiation can be delivered safely and has an efficacy that is superior to what has been seen with conformal photon irradiation by itself in phases II/III clinical trials in the treatment of CaP patients [19]. However, the cellular and molecular mechanisms and targets of action through which neutron radiation exerts its beneficial effect are still unclear. Contemporary RT approaches such as intensity modulated radiation therapy (IMRT) and image-guided radiation therapy (IGRT) have permitted enhanced delivery of radiation to the prostate to spare adjacent organs and reduce the potential for acute and chronic toxicity [20–22]. Recent advances in volumetric-based IMRT and IGRT have permitted external RT dose escalation beyond 75 Gy [23, 24]. This has reduced both biochemical failure rate and the development of metastasis [25–28]. Efforts to improve the outcome after EBRT for CaP patients have focused on delivering a higher dose to tumor. Several randomized trials have shown a benefit of dose escalation to >70 Gy with EBRT for localized CaP [29, 30]. Eade et al. recommend doses of ≥80 Gy for most men with CaP due to significant benefit on patients’ treatment outcome [31]. However, there is a concern that further dose increase may lead to more toxicity. Further dose escalation to 82 Gy in American College of Radiology 03–12 phase II trials yielded significant acute and late morbidity [32]. Therefore, a modality for improving the therapeutic efficacy of RT for locally confined or advanced CaP is warranted via enhancing radiation-induced cytotoxicity and reducing related side effects.
Local CaP recurrence after RT is a pattern of treatment failure attributable to radioresistance of cancer cells. Understanding the mechanisms of radioresistance will help to improve treatment outcome, overcome recurrence after RT, and prevent metastasis in CaP patients. Combination of radiosensitizers with RT will be very promising for future CaP clinical trials. The recent progress in understanding the mechanisms of CaP radioresistance and updated combination approaches with radiosensitizers in CaP treatment will be discussed in the following sections.
3 The roles of PI3K/Akt/PTEN/mTOR signaling pathway in CaP metastasis and radioresistance
PI3K/Akt/PTEN/mTOR signaling pathway is important for regulating cell growth and survival, particularly during tumor progression and metastasis. This pathway is activated in a large percentage of human cancers through a variety of mechanisms including Ras mutation, loss of PTEN, activation of growth factor receptors such as epidermal growth factor receptor (EGFR), and mutations in PIK3A [33]. PI3K activates a number of downstream targets including the serine/threonine kinase Akt and mTOR; a downstream member of the PI3K cascade, which plays an important role in cell growth, death, adhesion, and migration; and is frequently activated in cancer cells [34, 35] (Fig. 1).

Overview of PI3K/Akt/PTEN/mTOR signaling pathway in the regulation of cancer metastasis, apoptosis, and autophagy. This pathway plays a crucial role in regulating a broad range of cellular functions including cell growth, death, adhesion and migration, chemoresistance, and radioresistance in cancer cells. PI3K converts PIP2 into PIP3, while PTEN antagonizes PI3K function by converting PIP3 back to PIP2, and thus inhibiting downstream signaling. Akt, which is the downstream in the pathway, is activated and phosphorylated by PIP3 which subsequently causes alteration of numerous cell functions including the activation of mTOR and its substrates
3.1 PI3K/Akt in CaP metastasis and radioresistance
Altered signaling pathways within the tumor cells that affect tumor cell survival are in focus for the development of innovative anticancer treatments. The PI3K/Akt signaling pathway represents a major cell survival pathway and plays a critical role in oncogenesis and tumor cell growth [36]. PI3K is a heterodimeric protein with a 85 kDa regulatory subunit and a 110 kDa catalytic subunit (PIK3CA). PI3K serves to phosphorylate a series of membrane phospholipids including phosphatidylinositol 4-phosphate (PtdIns(4)P) and phosphatidylinositol 4,5-bisphosphate (PtdIns(4,5)P2), catalyzing the transfer of ATP-derived phosphate to the D-3 position of the inositol ring of membrane phosphoinositides, thereby forming the second messenger lipid phosphatidylinositol 3,4-bisphosphate (PtdIns(3,4)P2) and phosphatidylinositol 3,4,5-trisphosphate (PtdIns(3,4,5)P3) [37].
PI3K/Akt pathway is one of the most important survival signaling cascades altered in human solid tumors including CaP [33, 38], and known to promote cell proliferation, cell cycle progression, and resistance to cytotoxic therapies in CaP [39]. Recent studies highlight the importance of the PI3K/Akt/mTOR signaling pathway in CaP invasion, progression, and angiogenesis [4, 40–42]. Clinical CaP specimens were reported to show upregulation of the PI3K/Akt pathway associated with phosphorylation of the androgen receptor (AR) during the development of castration-resistant prostate cancer (CRPC) [43]. PI3K activation leads to the development of chemoresistant CaP cells, through the upregulation of multidrug resistance protein 1 (MRP-1) [44]. Successful progression to an androgen-independent state of CaP requires intact PI3K signaling [45]. Furthermore, using a sphere-forming model, Dubrovska et al. demonstrated that the PI3K/Akt/PTEN pathway is critical for the maintenance of CaP stem-like features and that targeting PI3K signaling is beneficial in CaP treatment by eliminating CaP stem-like cells [46].
PI3K/Akt pathway plays an important role in CaP radioresistance. Hyperactivation of PI3K/Akt confers cancer cells resistance to radiation-induced cell death [47, 48]. It has been reported that the PI3K/Akt activity contributes to the resistance of human cancer cells to RT via three major mechanisms: intrinsic radioresistance, tumor cell proliferation, and hypoxia [49]. Gottschalk et al. tested the in vitro radiosensitization effect of LY294002, a broad inhibitor of PI3K, in a LNCaP CaP cell line and found that inhibition of PI3K causes the increased sensitivity to RT in CaP cells through a protein kinase B (PKB)-dependent mechanism [50]. Although LY294002 is promising in preclinical studies, it has not progressed through clinical trials because it also inhibits a number of proteins nonspecifically and is toxic to patients. More specific PI3K inhibitors are under development, such as IC486068 [51] and IC87114 [52], and potentially could be useful as radiosensitization agents.
Akt is a serine/threonine protein kinase that plays a critical role in suppressing apoptosis by regulating its downstream pathways [53]. It is implicated in cellular processes such as cell survival, proliferation, growth, glucose metabolism, apoptosis, angiogenesis, transcription, and migration [54]. After activation, Akt is able to translocate to the nucleus [55], where it affects the activity of a number of transcriptional regulators. Akt serves as an intermediate signaling molecule for mTOR, which is also a serine/threonine kinase that mediates cell growth, proliferation, survival, protein translation, and other oncogenic functions (Fig. 1). Activation of the PI3K/Akt pathway, a well-known method to inhibit apoptosis, also inhibits autophagy [56] via inhibition of mTOR [57]. Upregulated activity of the kinase Akt is associated with malignant transformation characterized by accelerated tumor growth, metastasis, and angiogenesis. It was reported that the Akt/mTOR pathway plays a crucial role in the regulation of both apoptosis and autophagy [58].
Recent studies have indicated that Akt activation contributes to resistance to radiation, chemotherapy, and tyrosine kinase inhibitors (TKIs) by promoting survival signals which protect cancer cells from undergoing apoptosis [38, 59–61]. Thus, the inhibition of the Akt pathway is emerging as an attractive clinical objective for the prevention of hormone refractory disease. As a major regulator of the PI3K pathway (Fig. 1), Akt is a target for radiosensitization. Palomid 529 (P529) (an inhibitor for Akt) has been shown to target Akt without in vivo toxicity [62]. Diaz et al. reported that P529 combined with RT could increase radiosensitivity in PC-3 CaP cells in vitro compared to RT alone and retard tumor growth in a PC-3 xenograft animal model [63]. Chiu et al. have recently demonstrated that the arsenic trioxide (ATO) enhances the radiation sensitivity in androgen-dependent (LNCaP) and androgen-independent (PC-3) human CaP cells primarily through the inhibition of Akt/mTOR signaling pathway [5]. These data indicate that Akt inhibitors are promising in combination therapies to enhance the sensitivity of RT in CaP treatment.
3.2 Roles of PTEN in CaP radioresistance
PTEN, the gene for which is located on chromosome l0q23, is a PI(3,4,5)P3 phosphatase which antagonizes the PI3K/Akt signaling pathway by dephosphorylation of PI(3,4,5)P3 to PI(3,4)P2 (Fig. 1) [64]. PTEN has both plasma membrane and nuclear localized activities. The PTEN phosphatase serves at the molecular level to counteract the functions of PI3K, which promotes proliferation and cell survival, in part through activation of mTOR [65]. Functional studies demonstrate that PTEN is a highly effective tumor suppressor, but it is frequently mutated, deleted, or epigenetically silenced in various human cancers [66–69] including CaP [70–72]. Inactivations or deletions of PTEN, which occur frequently in metastatic CaP, leads to Akt activation [73]. At least 70 % of CaP patients show loss or alteration of at least one PTEN allele, which may result in activation of the PI3K/Akt pathway [74]. Loss of PTEN activity plays a role in tumor resistance to chemo-agents and molecular-targeted antineoplastic agents [75–79]. Since PTEN mutations and deletions can lead to abnormal Akt activation, it is thought to play an important role in the resistance of CaP to RT [80, 81].
Teng et al. reported that 42 % of CaP tissues have abnormal PTEN/Akt expression [82]. Jendrossek et al. found that PTEN expression was diminished in 20 % of the CaP tissues compared with benign tissues, and the rate was 30 % in those with Gleason scores of ≥6, while the expression level of phospho-Akt (p-Akt) was elevated without obvious abrogation of PTEN function in a proportion of the patients [83]. These results suggest both PTEN-dependent and PTEN-independent mechanisms of Akt activation in localized CaP and demonstrate the important role of deregulation of PI3K/PTEN/Akt pathway in localized CaP.
It was found that the radiosensitization effect of parthenolide in CaP cells is mediated by nuclear factor-κB (NF-κB) inhibition and enhanced by the presence of PTEN [84]. Using a gene therapy, Rosser et al. demonstrated that PTEN restoration sensitizes PC-3 and LNCaP CaP cells to RT in vitro [85]. In a subsequent study, this group further confirmed the radiosensitization effect of PTEN gene therapy in vivo in a PC-3-Bcl-2 CaP xenograft animal model [86]. In another study, Tomioka et al. generated a new type of gene transfer drug, GelaTen, which is a microsphere of cationized gelatin hydrogels incorporating PTEN plasmid DNA and designed for sustained release of PTEN plasmid DNA in vitro and in vivo [87]. They demonstrated a synergistic effect of GelaTen with RT in PC-3 and LNCaP cell lines and a subcutaneous (s.c) PC-3-Bcl-2 xenograft animal model [87]. All data indicate that PTEN plays a critical role in the regulation of the sensitivity to RT in CaP cells and can be used as a therapeutic target for future CaP therapy.
3.3 mTOR in the regulation of CaP radioresistance
mTOR is a 289 kDa serine–threonine kinase which acts as a downstream effector for Akt [88]. It regulates key processes such as cell growth and proliferation, cell cycle progression, and protein translation through two distinct pathways: one involving the ribosomal p70S6 kinase (p70S6K) and the other one involving eukaryotic translation initiation factor 4E (eIF4E) binding proteins (4E-BPs) [89]. mTOR signaling has been implicated as a determinant of cell survival in response to DNA damage [90]. The p70S6K regulates the efficiency of translation of certain mRNAs and also functions in a negative feedback loop to control Akt activity [37, 91]. Akt, mTOR, and p70S6K activation have been associated with a poor prognosis in breast and other cancers [37, 92]. mTOR activity is often deregulated in CaP [93], in part due to the prevalence of PTEN dysfunction.
Aberrant upregulation of PI3K/mTOR signaling pathway occurs in many human malignancies and is implicated in resistance to RT in preclinical [94, 95] and clinical studies [96–98]. The ability of RT or chemotherapy to induce cell death in cancer cell lines that display resistance to apoptosis depends on type II-programmed cell death executed by autophagy [99]. There is ample evidence that radiation-induced cell death is affected by various intertwined biochemical processes in the autophagic and apoptotic pathways. Irradiation upregulates autophagic-programmed cell death in cells that are unable to undergo Bax/Bak-mediated apoptotic cell death [100]. Activation of PI3K/Akt/mTOR biochemical cascade confers survival advantage in neoplastic cells by both inhibitory effects of mTOR on autophagy and the inhibitory effect of Akt on apoptosis.
mTOR is an established therapeutic target and mTOR inhibitors appear to be reasonably tolerated. Cao et al. tested the ability of the mTOR inhibitor RAD001 (everolimus) to enhance the cytotoxic effects of radiation on PC-3 and DU145 CaP cell lines, and found that both cell lines became more vulnerable to irradiation after treatment with RAD001, with the PTEN-deficient PC-3 cell line showing greater sensitivity [101]. They also found that the zVAD (an apoptosis inhibitor)-induced inhibition of apoptosis or the RAD001-induced autophagy result in an increased radiosensitivity when employed alone, while combination of zVAD and RAD001 led to additive, rather than synergistic, effects on cell death [101]. Schiewer et al. demonstrated that mTOR is a selective effector of the RT response in AR-positive CaP, and mTOR inhibitors (sirolimus and temsirolimus) exhibit schedule-dependent effects on the RT response in CaP cells and confer significant radiosensitization effects when used in the adjuvant setting [6]. mTOR is a promising target for CaP RT in the future.
4 The double faces of autophagy in cancer RT
4.1 Paradox of autophagy in cancer treatment
The interest in discovering the mechanism of autophagy has increased in the last decade. Autophagy is a cellular response to stress or nutrient deprivation, which is a way to supply amino acids as an alternative energy source by degradation of damaged cytoplasmic organelles or protein [102]. On one hand, autophagy eliminates toxic and damaged cellular components. On the other hand, this process delivers new precursors for synthesis of macromolecules. Autophagy, a process which involves autophagic/lysosomal compartment, is a genetically regulated form of programmed cell death in which the cell digests itself. It is characterized by the formation of double-membrane vacuoles in the cytoplasm, which sequester organelles such as condensed nuclear chromatin and ribosomes [103, 104].
Depending on context, autophagy can act as oncogenic or tumor-suppressing mechanism [105]. In cancer therapy, the role of autophagy is also paradoxical, in which this cellular process may serve as a prosurvival or pro-death mechanism to counteract or mediate the cytotoxic effect of anticancer agents [106]. Autophagy frequently exerts cytoprotective functions by acting as a stress response mechanism [107]. Upregulation of autophagy has been observed in many types of cancer and it has been demonstrated to promote both cell survival and cell death [108]. There is an accumulation of evidence that highlights the important function of autophagy in cancer [56, 109–112]. Data reported in the literature indicate that whether autophagy enables cells to survive or induces their death depends on many factors, including the genotype and phenotype of the tumor cells, stress factors, and the status of the apoptotic machinery [113]. Although it is still controversial about whether autophagy kills cancer cells or sustains their survival under stressful conditions, increasing reports provide data to support that autophagy promotes cancer cell survival after chemotherapy or RT [112, 114].
In recent years, the role of autophagy as an alternative cell death mechanism has been a topic of debate. Autophagy was believed as a non-apoptotic program of cell death or “type-II” cell death to distinguish from apoptosis [115]. However, it is still fundamentally important to clarify whether autophagy is a main strategy for cell survival, or if it also serves as a trigger for cell death [115]. Although autophagy and apoptosis cell death pathways are predominantly distinct from each other, many studies have demonstrated that extensive crosstalk exists between the two [116, 117]. The interplay between apoptosis and autophagy may need to be exploited to improve cancer therapy. Studies are ongoing to define optimal strategies to modulate autophagy for cancer prevention and therapy and to exploit autophagy as a target for anticancer drug discovery [118]. Nevertheless, the molecular mechanism governing cell fate decision during autophagy is still poorly understood and the Janus-faced nature of autophagy may complicate the clinical development of its modulators. It is important to determine if the prodeath or prosurvival action of autophagy is associated with a particular class of cancer therapeutics.
The PI3K/Akt/mTOR pathway is a central repressor of autophagy. PTEN overexpression has been shown to promote autophagy [119], whereas the targeted deletion of PTEN in mouse liver causes a strong inhibition of autophagy [120]. Akt inhibition also strongly promotes autophagy whereas constitutively active Akt has the opposite action [121]. Inhibitors of mTOR have also been shown to induce autophagy in various cell types [101, 122, 123]. In addition, stabilization of tuberous sclerosis complex 2 (TSC2), which inhibits the mTOR signaling, promotes autophagy and suppresses tumorigenesis [124]. The inhibitory effect of PI3K/Akt/mTOR axis on autophagy is mainly mediated through the unc-51-like kinase 1/2 (ULK1/2)/mAtg13/focal adhesion kinase family interacting protein of 200 kDa (FIP200) complex [125, 126]. Although the link between mTOR inhibition and autophagy is well established, it is worthwhile to notice that in some situations, mTOR may stimulate autophagy. In this regard, Zeng and Kinsella demonstrated that mTOR and its downstream mediator S6 kinase 1 may positively regulate autophagy in 6-thioguanine-treated cells, possibly through the negative feedback inhibition of Akt. Thus, a better understanding of the PI3K/Akt/PTEN/mTOR signaling pathways that regulate autophagy and cellular fate will hopefully open new possibilities for cancer treatment.
4.2 Autophagy in prostate cancer RT
Autophagy is an interesting research area in cancer metastasis and radioresistance. Recent studies have identified autophagy as a cell death pathway that may mediate ionizing radiation (IR) sensitivity [127]. Existing data indicate that autophagy increases in tumor cells especially in response to radiation and DNA damage [114, 128–130]. Autophagy was found to contribute to resistance of MDA-MB-231 breast cancer cell line to IR in vitro [131].
Gwak et al. demonstrated that microRNA 21 (miR-21) is a pivotal molecule for circumventing radiation-induced cell death in malignant glioma cells through the regulation of autophagy in malignant glioma cell lines and this molecule could be a novel therapeutic target for future treatment of malignant glioma to overcome radiation resistance [132]. Cao et al. showed that the mTOR inhibitor RAD001 (everolimus) can enhance radiation sensitivity in PC-3 and DU145 CaP cell lines with the PTEN-deficient PC-3 cell line showing the greater sensitivity, and this increased susceptibility to radiation is associated with induction of autophagy [101]. Atorvastatin (statin), an inhibitor of 3-hydroxyl-3-methylglutaryl coenzyme A (HMG-CoA) reductase, is an autophagy inducer. Parikh et al. reported that statins induce autophagy and autophagy-associated cell death in PC-3 cells via inhibition of eranylgeranylation [133]. They further confirmed that the effect of statin on autophagy in PC-3 cells is mediated by the Erk and JNK pathways through activation of LC3 transcription [134]. He et al. have also reported that statin is capable of radiosensitizing PC-3 CaP cells and has superior effect in inducing possibly both autophagic and apoptotic cell deaths, that activation of the autophagy pathway may be responsible for apoptosis inducing effect of statin [135]. Thus, these data indicate that a combined treatment with radiation and autophagic inducer, such as statin, may be synergistic in inducing cell death of CaP cells. Monascuspiloin (MP), a yellow pigment first isolated from Monascus pilosus M93-fermented rice, is structurally similar to the well-known Monascus pigment monascin. Chiu et al. demonstrated that IR combined with MP increases the therapeutic efficacy compared to each individual treatment alone in PC-3 CaP cells in vitro and in vivo with induced autophagy, endoplasmic reticulum (ER) stress and enhanced DNA damage, and this combined treatment-induced autophagy occurred primarily via inhibition of the Akt/mTOR signaling pathways, suggesting that IR combined with MP could provide a novel therapy for the treatment of androgen-independent CaP [5].
The autophagic response of cancer cells to antineoplastic therapy, including IR, is controversial. It can originate a protective mechanism against the treatment itself by removing proteins and organelles that are damaged, or, alternatively, produce an effective cell-death process. The autophagic paradox in cancer therapy has been recently reviewed [136]. Thus, autophagy seems to play a pivotal role on both survival and death processes: these processes, in fact, might be cell and tissue specific and highly dependent on the expression profile of genes and proteins regulating apoptosis. In principle, most cancers have certain defects in their apoptotic pathway, whereas therapeutic targeting of autophagy pathways might yield better clinical outcomes for patients undergoing RT and cytotoxic drug therapy. As modulation of autophagy represents a novel approach for enhancing the therapeutic efficacies of cancer therapy including IR, research efforts have been put forth to identify agents that can induce or inhibit autophagy.
5 EMT in CaP metastasis and radioresistance
5.1 Roles of EMT in CaP metastasis and progression
Progression of most carcinomas toward malignancy is associated with the loss of epithelial differentiation and by switching toward mesenchymal phenotype, which is accompanied by increased cell motility and invasion. EMT can lead to increased cellular adhesion, apical–basal polarity, cellular motility, and increasing the potential for invasion/metastasis. This phenomenon is characterized by the loss of cell–cell adhesion molecules, downregulation of epithelial differentiation markers, and transcriptional induction of mesenchymal markers [137] (Fig. 2). This process is regulated by many signaling pathways (Fig. 2). EMT plays a critical role not only in tumor metastasis but also in tumor recurrence that is believed to be tightly linked with the biology of cancer stem-like cells or cancer-initiating cell [138, 139]. In order to establish new tumors at the metastatic sites, it is believed that the cells which transition from an epithelial to a mesenchymal state and migrate must undergo the reverse procedure, mesenchymal to epithelial transition (MET) [140]. Therefore, metastasis is considered to be a dynamic and complex process involving cellular plasticity. E-cadherin is a cell-to-cell adhesion molecule in which loss of expression is a hallmark of EMT, leading to increased cell motility and invasion [141]. On the other hand, N-cadherin and fibronectin are mesenchymal markers [137] in which expression is regulated by several transcription factors including a basic helix-loop-helix (bHLH) transcription factor Twist1, Slug, and Snail [142, 143].

A schematic model of EMT in cancer metastasis. Chemoresistant or radioresistant cancer cells with EMT lose their cell-cell contacts and re-arrange the cytoskeleton so that they can migrate, invade the neighboring tissue and metastasize to distant organs via blood. During EMT, metastatic potential is acquired by the loss of epithelial markers and the acquisition of mesenchymal markers. This process is regulated by several EMT-related signaling pathways
Emerging evidence is suggesting that EMT plays a crucial role in the aggressiveness in CaP, including increased migration and invasion ability, and contributing to chemoresistance, radiation resistance, and CSC populations [9, 144, 145]. CaP is a highly metastatic disease during which cells undergoing EMT lose their epithelial morphology, reorganize their cytoskeleton (CK), and acquire a motile phenotype through the downregulation of adherent junction proteins (such as cadherins) and upregulation of mesenchymal markers (Snail, Slug, and Vimentin) [146, 147]. EMT is a characteristic of cancer cell intravasation and metastasis and is closely associated with CRPC. It was reported that CaP cells with more mesenchymal features exhibit a more-invasive phenotype in vitro and display a more aggressive behavior in metastatic colonization models [148]. Pathological EMT events have been shown to potentiate the transition from localized CaP to invasive CaP and subsequent metastasis [149–153]. Conversely, repression of EMT events blocks the metastatic potential of CaP cells [154]. In clinical specimens, measures of cancer progression correlate with loss of E-cadherin and upregulation of EMT-inducing transcriptional factors [142, 152, 154–156]. EMT events are correlated with metastatic CaP recurrence following surgery [151, 152], and have recently been observed concurrently following androgen withdrawal therapy [157]. Therefore, the ability to identify primary tumor cells with an increased propensity to undergo EMT-like events would improve diagnostic approaches to discriminate patients at risk for progression.
Behnsawy et al. recently found that measurement of the expression of potential EMT markers (Twist and Vimentin) combined with conventional prognostic parameters in RP specimens, would contribute to a more accurate prediction of the biochemical outcome in localized CaP patients following RP [158]. Mulholland et al. demonstrated that PTEN loss and RAS/mitogen-activated protein kinase (MAPK) activation cooperate to promote EMT and metastasis initiated from CaP stem/progenitor cells in the conditional activatable K-ras (G12D/WT) mice with the prostate conditional PTEN deletion model [144]. It was reported that SIRT1 induces EMT by cooperating with EMT transcription factors and enhances CaP cell migration and metastasis in CaP cell lines and in an immunodeficient mouse model [145]. Sethi et al. examined EMT markers including E-cadherin, Vimentin, ZEB1, Notch-1, platelet-derived growth factor (PDGF)-D, and NF-κB using an immunohistochemical approach in primary CaP and bone metastases and found that Notch-1 plays an important role in CaP bone metastasis [159].
Zhu and Kyprianou found that androgens induce the EMT pattern in CaP epithelial cell with Snail activation and lead to significant changes in CaP cell migration and invasion potential [160]. It was reported that the majority (>80 %) of the circulating tumor cells (CTCs) in patients with metastatic CRPC co-express epithelial proteins such as epithelial cell adhesion molecule (EpCAM), CK, and E-cadherin, as well as mesenchymal proteins including Vimentin, N-cadherin, and O-cadherin, and the stem cell marker CD133, suggesting that the improved detection of these cells in vivo can be achieved to assist in developing novel therapeutic strategies [8]. Tanaka et al. demonstrated a clear link between the expression of N-cadherin and metastatic CRPC and developed the N-cadherin-specific monoclonal antibodies (MAbs) shown to delay the progression to castration resistance, inhibit the invasion of surrounding tissues, suppress tumor growth, and reduce metastasis in castrated mice [161]. This work provides further support for the critical role of EMT in CaP progression and the potential of immunotherapy as a strategy to combat CRPC disease.
5.2 EMT in cancer radioresistance
The investigation of the relationship between EMT and radioresistance in cancer is a new and developing research area. Until recently, the association between radiation and EMT has not been intensively investigated, and only a few studies have examined the underlying mechanism. Clinical and laboratory data suggest that IR may promote the metastatic ability of cancer cells and elicit changes in the host microenvironment that may facilitate tumor progression and the development of second malignancies [162, 163]. EMT was reported to be related to radioresistence in many cancers [164–166].
Andarawewa et al. have proven that radiation can predispose nonmalignant human mammary epithelial cells to undergo transforming growth factor-β (TGF-β)-mediated EMT through MAPK signaling pathways, thereby elicits heritable phenotypes that could contribute to neoplastic progression [167]. Tsukamoto et al. indicated that radiation can induce EMT through promoting the expression of Twist, an organizer of EMT, thus enhance the invasive potential of endometrial carcinoma cells [168]. Zhang et al. reported that low doses IR enhances the invasiveness of breast cancer cells by inducing EMT with downregulation of epithelial differentiation markers and transcriptional induction of mesenchymal markers in MCF-7 breast cancer cell line [169]. Jung et al. showed that IR induces changes associated with EMT and increased cell motility in the A549 lung epithelial cancer cell line in vitro, suggesting that a subset of lung cancer patients may benefit from a combination of RT with inhibitors of EMT on cell migration [170]. Li et al. demonstrated that radiation enhances long-term metastasis potential of residual hepatocellular carcinoma (HCC) in nude mice through TMPRSS4-induced EMT and these findings provide new clues to suppress the radiation-induced dissemination and metastasis of tumor cells to improve the prognosis of HCC patients [171]. All these findings suggest that EMT is involved in radioresistance and specifically targeting EMT may provide a new targeted approach for improving the therapeutic effectiveness of radiation in cancers.
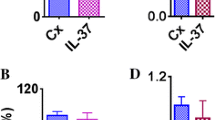
To the best of our knowledge, the investigation of the role of EMT in CaP radioresistance has not been reported until now. Our research group has recently developed three radiation resistance CaP cell lines (PC-3, DU145, and LNCaP) with a 2 Gy dose irradiation each day for five consecutive days. After 5-week treatment, these radiation-treated CaP cells demonstrated the morphological changes including loss of glandular pattern, vacuolated cell plasma, pleomorphic nuclei, and enlarged size as well as increased colony growth and invasion ability (unpublished data). These treated CaP cells are consistent with previous reports for EMT characteristics such as reduced E-cadherin and increased Vimentin, SOX2, and OCT3/4 (Fig. 3). These preliminary data indicate that EMT is involved in CaP radioresistance and may play an important role in CaP metastasis and recurrence after RT. It is worthwhile to investigate the role of EMT in CaP animal models and clinical tissue samples after RT to further confirm its significance. The findings may be useful in developing novel biomarkers to monitor CaP RT and therapeutic targets to overcome radiation resistance which is the most common problem in the current CaP therapy.

EMT is induced in CaP cell lines after RT treatment. Androgen-nonresponsive (PC-3 and DU145) and androgen-responsive (LNCaP) CaP cell lines were treated by irradiation at a 2 Gy dose each day for five consecutive days. The expression of E-cadherin (epithelial marker) was reduced in RT-treated CaP cells compared to those without RT treatment (control) while the expression of Vimentin, SOX2 and OCT3/4 (mesenchymal markers) in RT-treated CaP cells were increased in RT-treated CaP cells. Representative confocal images with variable levels of E-cadherin, Vimentin, SOX2 and OCT3/4 are shown (green). Nuclei are stained with PI (red). Magnification, × 600 in all images
6 CSCs in CaP radioresistance
6.1 Concept of CSCs
CSCs, also known as tumor-initiating cells, are malignant cell subsets capable of tumor initiation and self-renewal and give rise to bulk population of nontumorigenic cancer cell progeny through differentiation [172]. CSCs share signature characteristics with benign stem cells: the ability to self-renew and to differentiate. CSCs expand the CSC pool by self-renewal and also divide to generate the bulky tumors. They may also divide and differentiate into heterogeneous lineages of all nontumorigenic cancer cell types (non-CSCs) [173]. These cells express high levels of ATP-binding cassette drug transporters and exhibit a lowered ability to enter apoptosis. They embody the refractory nature observed among many cancers: very competent initial tumor establishment, extremely aggressive metastatic nature, resistance to chemo- and radiotherapy, correlation with advanced disease, and resistance to current therapies. Therefore, if CSCs survive after anticancer treatment, recurrence and metastasis are expected due to the ability of these cells to give rise to new tumors. Thus, investigation of CSCs has been a hot spot of basic cancer research and is rapidly expanding into many related aspects of cancer research, including chemosensitization and radiosensitization.
Despite continuous improvements in cancer management, locoregional recurrence or metastatic spread still occurs in a high proportion of patients after RT or combined treatments. One underlying reason might be a low efficacy of current treatments on the eradication of CSCs. Despite the ongoing debate on the abundance and origin of CSCs, it is generally accepted that they represent the root of cancer that must be eradicated in order to cure cancer. However, an effective therapeutic modality targeting CSCs is yet to be developed.
6.2 Putative prostate CSC markers
Although some studies suggested the cellular origins of CaP are terminally differentiated luminal cells [174], evidence still supports the existence of CSCs in CaP [175]. We and others have recently reviewed the literature on CSCs origin, the identification and characterization in CaP, as well as their clinical implications and therapeutic challenges [10, 176]. There are also several reviews published by other authors elaborating the current status of research on CSCs in CaP, including characteristics of CSCs [177], methodologies of assaying CSCs [178], and the relationship of stem cells with therapy resistance [179]. In this section, we only summarize putative CSC markers from human CaP cell lines, xenografts, and primary tissues.
CSCs appear to express many of the same markers as normal tissue stem cells. Prostate CSCs express a number of the same markers as prostate stem cells, such as CD44, CD133, integrins, breast cancer resistance protein (BCRP), and Sca-1, all of which have been utilized to identify prostate CSCs or prostate stem cells. The most frequently identified potential CSCs markers in CaP are summarized in Table 1. These surface markers combined with cell sorting technology have been used to identify and isolate CSC subpopulations in CaP. Collin et al. reported the identification and characterization of a population (CD44+α2β1highCD133+) from human prostate tumors, which possesses a significant capacity for self-renewal and is also able to regenerate the phenotypically mixed populations of nonclonogenic cells such as AR and prostatic acid phosphatase (PAP)-positive CaP cells [180]. They suggested that this population of CSCs can be used as a therapeutic target for CaP treatment [196, 197]. Later on, using a side population of cells isolated from LAPC-4 and LAPC-9 CaP xenografts, Patrawala et al. found that highly purified CD44+ CaP cells are enriched in tumorigenic and metastatic progenitor cells [181]. After adding other potential CSC markers, they demonstrated that the CD44+α2β1+/high cell population from the LAPC-9 CaP tumor xenografts reveal a hierarchy in tumorigenic potential [182]. Previous study reported that one population of CD133high/CD44high cells isolated from established aggressive prostate PC-3-MM2 cell line have CSC characteristics and are potentially useful to model and study stem cell behavior, and their responses to CaP treatment [183]. Furthermore, Dubrovska et al. confirmed that the CD133+/CD44+ population of cells enriched in CaP progenitors from PC-3 and DU145 cell lines have tumor-initiating potential and that these progenitors can be expanded under non-adherent, serum-free, and sphere-forming conditions [46].
Using flow cytometry, Hurt et al. isolated a population of CD44+/CD24− CaP cells from LNCaP and DU145 cell lines that display stem cell characteristics as well as gene expression patterns that predict overall survival in CaP patients [185]. CD44+/CD24− LNCaP cells could form prostaspheres in vitro [185]. CD44+/CD24− cells form colonies in soft agar and form tumors in non-obese diabetic/severe combined immunodeficiency (NOD/SCID) mice when as few as 100 cells were injected [185]. They concluded that the CD44+/CD24− LNCaP CaP cells offer an attractive model system to explore the biology important to the maintenance and differentiation of prostate CSCs as well as to develop the therapeutics, as the gene expression pattern in these cells is consistent with poor survival in CaP patients. Furthermore, they also demonstrated that the genomic profile of the invasive CaP cells closely resembles that of CD44+/CD24− prostate CSCs and showed evidence for increased Hedgehog signaling [184]. Using CaP spheres model, Bisson and Prowse showed that prostate spheres from PC-3, VCAP, LNCaP, 22RV1 DU145, and C4-2B CaP cell lines exhibit heterogeneous expression of proliferation, differentiation, and stem cell-associated makers CD44, ABCG2 and CD133, and WNT signaling regulates self-renewal and differentiation of CaP cells with stem cell characteristics [186]. Qin et al. recently demonstrated that prostate specific antigen (PSA)−/lo CaP cells can initiate robust tumor development and resist androgen ablation in castrated hosts, and they harbor highly tumorigenic castration-resistant CaP cells that can be prospectively enriched using aldehyde dehydrogenase (ALDH)+/CD44+/α2β1+ phenotype in CaP cell lines [187].
CD133 has been proposed to be a putative surface marker in a number of tumors. Richardson et al. found a small population (approximately 1 %) of human prostate basal cells express the cell surface marker CD133 in primary CaP tissues and are restricted to the α2β1high population, and showed that CD133+ cells exhibit characteristics of stem cells including prostasphere formation and the development of prostatic-like acini in SCID mice [188]. Within a series of AR+ human CaP cell lines including LAPC-4, LNCaP and CWR22Rv1 cells, CD133+ cells are present at a low frequency, self-renew, express AR, generate phenotypically heterogeneous progeny negative for CD133, and possess an unlimited proliferative capacity [189]. However, other investigators found that CD133 was only expressed in DU145 cells but not in DuCaP, LAPC-4, CWR22Rv1, LNCaP and PC-3 CaP cells, and that CD133+ cells from the DU145 cell line were not more clonogenic than CD133− cells [198]. They considered CD133 selection does not enrich for stem-like cells in CaP cell lines. The reasons for this variance may be caused by the application of different antibodies to CD133, different passages of tissue culture, or experimental methodology.
ALDH is an enzyme involved in intracellular retinoic acid production [199]. In prostate CSCs studies, the high expression of ALDH1A1, a member of ALDH family, was found to be positively correlated with Gleason score and pathologic stage, and inversely associated with overall survival and cancer-specific survival of the CaP patients, indicating ALDH1A1 could be a potential prostate CSC-related marker [10]. In one study, it was reported that ALDHhigh CaP cells from CaP cell lines (PC-3M-Pro4 and C4-2B) and primary CaP tissues not only display strongly elevated clonogenicity and migratory behavior in vitro, but also show enhanced tumorigenicity and metastatic ability in vivo [190]. In another study, Doherty et al. demonstrated that PC-3 cells contain a stem cell hierarchy, and isolation of ALDHhigh PC-3 cells enriches for the most primitive holoclone population [191]. By ALDEFLUOR assay and fluorescence-activated cell sorting (FACS), Li et al. isolated ALDH1A1+ cells from PC-3 and LNCaP CaP cell lines and the isolated ALDH1A1+ CaP cells demonstrated high clonogenic and tumorigenic capacities in vitro, and serially reinitiated transplantable tumors that resembled histopathologic characteristics and heterogeneity of the parental CaP cells in vivo [10]. Therefore, ALDH and ALDH1A1 activity are promising prostate CSC-related markers for future therapy. Rajasekhar et al. recently performed a thorough investigation on prostate CSCs and identified two noteworthy new features of prostate CSCs: expression of TRA-1-60, CD151, and CD166 and elevated NF-κB signaling [192]. This minor subset of TRA-1-60+/CD151+/CD166+ cells do not express AR or PSA, but possess stem cell characteristics and multipotency as demonstrated by in vitro sphere formation and in vivo tumor initiation, respectively [192].
The cell adhesion molecule E-cadherin has an important role in maintaining the undifferentiated stage of embryonic CSCs [200]. E-cadherin downregulation is thought to correlate with highly invasive tumors and poor prognosis in CaP patients [201, 202]. Bae et al. isolated E-cadherin+ cell population from DU145 and PC-3 CaP cell lines by flow cytometry and found that this population of cells show high expression of CD44 and integrin-α2β1, OCT3/4, and SOX2 and have high tumorigenicity in immunodeficient mice in vivo [203]. They further confirmed that this population of cells is also highly invasive and capable of altering its E-cadherin expression during the process of invasion [203]. These data support that E-cadherin may play an important role in CaP invasion and promote the dissemination of cancer cells. Using a magnetic activated cell sorting (MACS) system, Liu et al. found that CD117+/ABCG2+ cells from 22RV1 CaP cell line overexpress stem cell markers such as Nanog, Oct4, Sox2, estin, and CD133, and can readily establish tumors in vivo in a relatively short time [194]. In addition, this population of cells is also resistant to treatment with a variety of chemotherapeutics such as casplatin, paclitaxel, adriamycin, and methotrexate [194]. Kong et al. demonstrated that CaP cells with EMT phenotype displays stem-like cell features characterized by increased expression of Sox2, Nanog, Oct4, Lin28B, and/or Notch1, consistent with enhanced clonogenic and sphere (prostasphere)-forming ability in vitro and tumorigenicity in mice in vivo [204]. Selective elimination of this population of Sox2+/Nanog+/Oct4+/Lin28B+ cancer stem-like cells by reversing the EMT phenotype to MET phenotype using novel agents would be useful for the prevention of CaP recurrence via targeting the “Root Cause” of tumor development and recurrence.
6.3 Different response of CSCs and non-CSCs to RT
The current stem cell hypothesis implies that permanent local tumor control or recurrence after treatment depends on the inactivation or survival of CSCs after treatment [205]. There is considerable evidence to suggest that, under certain experimental conditions, CSCs exhibit radioresistant features [206]. Tumor radioresistance leads to recurrence after RT. The radioresistant phenotype has been hypothesized to reside in the CSC component of tumors and is considered to be an inherent property of CSC. In CSCs and radiation research, it is generally suggested that CSC subpopulations are relatively radioresistant compared with non-CSC subpopulations.
Using CD24−/low/CD44+ cancer-initiating cells isolated from MCF-7 and MDA-MB-231 breast cancer cell lines, Phillips et al. demonstrated that surviving fraction at 2 Gy [SF (2 Gy)] was elevated from 0.2 to 0.5 for monolayer cultures and mammospheres (a clump of mammary epithelial cells that form under specialized suspension culture conditions in vitro) [207]. Furthermore, MCF-7 mammospheres displayed greater survival and less expression of γH2AX than adherent cultures exposed to radiation [207]. These results suggest that CD24−/low/CD44+ cells are more resistant to RT. In one study, radiation induced enrichment of breast cancer cells with stem or progenitor characteristics (measured by Hoechst 33342 dye efflux or LIN−/CD24+/CD29+), γH2AX foci, which are markers of DNA double strand breaks (DSBs), resolved more rapidly in mammospheres derived from LIN−/CD24+/CD29+ cells, suggesting more effective DNA repair in cells with stem cell characteristics after irradiation [208]. In another study, Zhang et al. collected tumor cells from syngeneic p53-null mouse mammary gland tumor models and identified a subpopulation of cells with Lin−/CD29high/CD24high phenotype by limiting dilution transplantation and in vitro mammosphere assay, which possessed tumor initiation capacity [209]. After single-dose irradiation from 2 to 6 Gy, gene microarray demonstrated an increased DNA damage response and expression of DNA repair genes among Lin−/CD29high/CD24high cells including Nek1, Brca1, Chek1, Hus1, Ung, Xrcc5, Sfpq, and Uhrf1, which was validated by quantitative polymerase chain reaction (PCR) [209]. These results further confirmed the existence of radiation resistance in tumor initiating cell-enriched mammospheres in breast cancer cells. Using non-breast cancer stem cells (BCSCs) sorted from patient samples, Lagadec et al. found that IR reprogrammed differentiated breast cancer cells into induced BCSCs (iBCSCs) [210]. iBCSCs showed increased mammosphere formation, increased tumorigenicity, and expressed the same stemness-related genes as BCSCs from nonirradiated samples. However, one recent study found that based on CD44+/CD24−/lin− phenotype and ALDH1, not all breast tumor CSCs are radioresistant but can respond uniquely to RT [211]. In addition, two recent studies have also suggested that radioresistance may not be a general property of CSCs [212, 213]; among CSCs isolated from nine cell lines of brain, breast, colon, and pancreas cancers by FACS, only one breast cancer cell line (MDA-MB-231) showed radioresistance [212].
RT represents one of the most effective therapies for glioma [214]. CD133 has been regarded as the marker for CSCs in malignant glioma in a number of studies [215–218]. In vitro and in vivo experiments demonstrated enrichment of CD133+ cells after irradiation with clinically relevant doses, which represented selective survival of CD133+ cells and death of CD133− populations [219]. In glioblastoma, CD133+ CSCs are dramatically increased after irradiation, and radioresistant glioblastomas exhibit a higher percentage of CD133 expressing CSCs [219]. Brain CSCs preferentially activate the DNA damage checkpoint proteins in response to radiation, and repair radiation-induced DNA damage more effectively than non-CSCs [219, 220]. In atypical teratoid/rhabdoid brain tumors, the number of CD133+ cells is positively correlated with the degree of radioresistance [221]. The relative radioresistance of CD133+ cancer cells in glioma is also demonstrated in a study of clinical patients’ tissue sections after high-dose irradiation [222]. Data yielded from histopathological examination of glioma patients who underwent surgical removal of remnant tumors after Gamma Knife surgery (GKS) and EBRT demonstrated marked accumulation of CD133+ glioma cells, particularly in remnant tumors within the necrotic areas, while CD133+ cells appeared sparse in primary sections prior to GKS and EBRT [222]. These results suggested that CD133+ cells can survive high-dose irradiation and may account for tumor regrowth. Taken together, all the data support the contribution of CD133+ CSC marker in glioma radioresistance, although the mechanisms through which CSCs alter radiosensitivity of glioma remain elusive.
Piao et al. recently demonstrated the CD133+ cells from HCC Huh-7 cell line are associated with radioresistance through the activation of MAPK/ERK survival pathway, and have enhanced proliferating activity compared to CD133− cells following irradiation [223]. Therefore, CD133+ cell surface marker has a potential as therapeutic target to improve the effect of the RT of HCC. Interestingly, the EMT accompanied by E-cadherin loss has recently been associated with CSCs [138]. These cells have also been associated with tumor relapse and resistance to radiation [205]. Whether the effect of E-cadherin loss in radioresistance is direct or indirect as a consequence of deregulation of the DNA repair and cell cycle checkpoints by EMT [165] or by the acquisition of stem-cell like properties remains to be investigated.
6.4 Current progress of CSCs in CaP radiation research
As far as we know, data related with the difference of CSC and non-CSCs in CaP are very limited until now. Both CD44 and CD133 are the most frequent CSC markers in CaP used in related research [180–182, 185, 196, 224, 225]. The results from our studies indicate that the downregulation of CD44 using small interfering RNA (siRNA) enhances radiosensitivity in PC-3, PC-3M-luc, and LNCaP CaP cells, and that the delay of DNA DSBs repair in CD44 low-expressing knock down CaP cells is correlated with ineffective cell cycle arrest and the delayed phosphorylation of Chk1 and Chk2[12]. These findings suggest that CD44 may be a valuable biomarker and a predictor of radiosensitivity in CaP treatment. Another aspect to consider in CSCs and CaP radiation research is the existence of splicing variants of CD44 (CD44v or CD44 isoforms). The multiple isoforms of CD44 are involved in cellular functions such as motility and proliferation. Although the value of CD44v as CSC-dependent cell surface markers has not been sufficiently investigated so far, the targeting of such variants appears to be a promising strategy for combined radio-oncologic treatment approaches. It was reported that anti-CD44v6-directed antibodies that were conjugated with a cytotoxic chemotherapeutic agent significantly improved local tumor control in combination with fractionated irradiation in a head and neck squamous cell carcinoma (HNSCC) model in vivo [226]. It will be very interesting to validate the stemness of CD44v6-positive tumor cells in CaP for future RT.
Cho et al. recently found that irradiation favors increased survival and showed an increase in CSC properties (CD44, CD133, Nanog, and Oct3/4) with long-term recovery (after 33–35 days of RT treatment) in LNCaP and DU145 CaP cells in vitro [5]. These data suggest that the combination of RT with a CSC-targeted therapeutic strategy may prevent CaP recurrence. We have recently developed three radioresistant CaP cell lines (PC-3, DU145, and LNCaP) after RT with EMT characteristics, enhanced expression of CSC markers (CD44, CD326, Nanog, and Oct3/4), increased proliferation, invasion ability, and colony formation in vitro (unpublished data). Although the mechanisms of CSCs in CaP radioresistance are still unclear, these results indicate that CSCs may be involved in CaP radioresistance and can be useful therapeutic targets to prevent metastasis and recurrence. Investigating the roles of EMT and CSCs in CaP metastasis, chemoresistance, and radioresistance is a very interesting research area which is currently under investigation in our laboratory now. Although a lot of controversies still exist in the field of CSCs, future work to validate the importance of CSCs and characterize the mechanisms responsible for CSCs resistance to radiation is quite necessary and will pave the avenue for developing CSC-specific radiosensitizors.
The main hurdle for investigating CSCs in radioresistance is the limitation of appropriate models available as CSCs are a dynamic process and the expression of CSC markers can be affected by many factors including tumor microenvironment. We have recently developed CaP-radioresistant (RR) cell lines using the maximum dose of radiation treatment and found that these CaP-RR (PC-3, DU145, and LNCaP) cells can induce EMT; enrich CSCs such as CD44, CD44v6, CD326, ALDH, Nanog, and Snail; easily form more spheres; and activate the PI3K/Akt/mTOR signaling pathways (unpublished data), indicating that these RT-treated cells are a good model to mimic clinical radioresistant condition and study the roles of CSCs in CaP radioresistance. We also found these radioresistant CaP cells have increased metastatic potential compared to the radiosensitive CaP cells (unpublished data), suggesting that this population of cells should be eradicated to prevent CaP metastasis. We believe this model is not only suitable for CaP radioresistance research but also useful for other cancer.
7 Combination of radiation with radiosensitizers in the treatment of CaP
EBRT and brachytherapy are the two main treatment options for organ-confined or locally advanced CaP. There is now abundant evidence supporting the benefits of high-dose EBRT in patients with clinically localized CaP [227]. However, high-dose RT causes considerable collateral damage to normal cell populations at the treatment site [228]. Another challenge in RT is that CaP cells develop radioresistance which results in local relapses [18, 229] as localized CaP is sensitive to conventional RT using X-rays and residual disease causes clinical relapse [230]. Therefore, it is important to find agents that sensitize malignant tumor cells to RT, thus minimizing radiation toxicity to surrounding organs by lowering effective therapeutic doses. The use of different radiosensitizers in combination with low-dose irradiation may increase the overall therapeutic efficacy and overcome radioresistance. In the current section, we focus on EBRT combined with radiosensitizers in CaP treatment. The different approaches by using radiosensitizers in combination with RT in preclinical studies are summarized in Table 2.
7.1 Small molecular inhibitors
Didox (DX; 3,4-dihydroxybenzohydroxamic acid) is a novel ribonucleotide reductase inhibitor. It was reported that Didox mediates its radiosensitizing effects by abrogating the radiation induced upregulation of Bcl-2 expression and NF-κB activity in PC-3 cells in vitro [231]. Celecoxibs represent a structural class of nonsteroidal anti-inflammatory drugs (NSAIDs) and belong to the most potent specific inhibitors of cyclooxygenase-2 (COX-2). COX-2 plays an important role in CaP progression [275]. It was demonstrated that COX-2 was upregulated after IR in PC-3 CaP cells in vitro [276]. Handrick et al. found that Celecoxib can sensitize CaP cell lines to IR via a pro-apoptotic Bax-independent death pathway [236]. In a phase I clinical trial, combination of Celecoxib with RT was performed in 22 localized CaP patients and was not associated with an increased level of side effects [277]. These data indicate that COX-2 inhibitors are promising for phase II and III trials to overcome CaP radiation resistance.
Pajonk et al. demonstrated the proteasome inhibitor MG-132 sensitizes PC-3 CaP cells to IR and indices apoptosis by a DNA-PK-independent mechanism [232]. An et al. reported that HA14-1 (a small molecular Bcl-2 inhibitor) potently sensitizes radioresistant LNCaP and PC-3 cells to γ radiation, regardless of the status of p53, and that combination of HA14-1 and γ radiation induces apoptosis through activation of oxidative injury and JNK signals and triggers both caspase dependent and independent cell death pathways [234]. Nutlins are small molecules that inhibit MDM2 binding to p53 [278]. These compounds bind in the p53-binding pocket of MDM2 to displace p53 from the complex and induce p53 stabilization. P53 then activates downstream targets leading to p21WAF induction, cell cycle arrest, and apoptosis. It was reported that Nutlin-3 can act as a radiosensitizer via p53-independent mechanisms under low O2 levels in CaP cell lines in vitro, indicating that Nutlin-3 can be a useful adjunct to target hypoxic cells and improve the efficacy of RT [235].
Dichloroacetate (DCA), a known inhibitor of mitochondrial pyruvate dehydrogenase kinase (PDK) and drug utilized for hereditary lactic acidosis disorders, can shift cellular metabolism from glycolysis to glucose oxidation. One study demonstrated that DCA can effectively sensitize Bcl-2wt and Bcl-2high human CaP cells to RT by modulating the expression of key members of the Bcl-2 family [279]. Palomid 529 (P529) is an Akt inhibitor which enhances the effect of RT in PC-3 CaP cells in vitro and in a s.c animal model in vivo [63].
Sodium selenite (SSE) is an inorganic Se compound and has been reported to radiosensitize both androgen-responsive (LAPC-4) and androgen-nonresponsive (DU145) CaP cells [233]. SSE significantly enhances the effect of RT on LAPC-4 and PC-3 s.c xenografts and does not sensitize the intestinal epithelial cells to radiation, suggesting that SSE has a very good therapeutic potential for the treatment of CaP [237]. PARP inhibitor ABT-888 (veliparib) can enhance radiosensitivity in PC-3 and DU145 CaP cell lines in vitro and PC-3 s.c animal model in vivo, suggesting that in vitro assays of radiosensitivity may not predict in vivo efficacy of PARP inhibitors with radiation [238]. Perifosine is a membrane-targeted alkylphospholipid developed to inhibit the PI3K/Akt pathway and has been suggested as a favorable candidate for combined use with RT. Perifosine enhances CaP radiosensitivity in a CWR22RV1 cell line in vitro and its s.c animal mode in vivo [239]. MK-1775 is a small molecule inhibitor of wee1. Bridges et al. found that MK-1775 radiosensitizes p53-defective PC-3 CaP cells but not p53 wild-type LNCaP cells in vitro [240]. Using a micro RNA (miRNA) microarray assay, Li et al. screened 132 cancerous miRNAs in LNCaP cells in response to RT and found that miR-106b is able to render radiation resistance in CaP cells, suggesting that miR-106b is a potential therapeutic target to overcome CaP radiation resistance [280].
7.2 Growth factor inhibitors
It was reported that PI3K inhibitor LY294002 increases sensitivity of CaP cell line to IR through inactivation of PKB [50]. Insulin-like growth factor-type 1 receptor (IGF1R) signaling in the malignant transformation and progression of many tumor types is well established and is ascribed to its pivotal role in cellular proliferation, survival, and differentiation, leading to resistance to RT, chemotherapy, and other targeted therapies. Rochester et al. indicated that the IGF1R transfected with IGF1R siRNA enhances IR response in PC-3, DU145, and LNCaP CaP cell lines in vitro [241]. A small molecule IGF1R kinase inhibitor NVP-AEW541 induced radiosensitization in the PTEN wild-type DU145 and 22Rv1 CaP cell lines but not in the PTEN-deficient PC-3 CaP cell line and NVP-AEW541-induced radiosensitization coincided with downregulation of p-Akt levels and high levels of residual DSBs [247].
AEE788, a dual TKI of both EGFR and vascular endothelial growth factor receptor (VEGFR), provides an avenue to investigate the effect of simultaneous blockade of EGFR and VEGFR in cancer cells [281]. It was reported that combination of AEE788 with RT can enhance treatment efficacy in DU145 CaP s.c model but not in PC-3 s.c model [242]. C225 (cetuximab) is a chimeric human-mouse IgG1 MAb and an EGFR inhibitor. Wagner et al. demonstrated that C225 MAb augments the radiation killing of DU145 CaP cells in vitro, and inhibits the growth of implanted DU145 tumors and increases the efficacy of RT in vivo via a combination of cytostatic, necrotic, and apoptotic mechanisms [243]. The C225 MAb was further demonstrated to increase the radiosensitivity of DU145 cells through antiproliferative effect, inhibition of clonal growth, G0/G1 phase arrest, apoptosis induction, and inhibition of EGFR-signaling pathways by the downregulation of MAPK activation [195].
Matsubara et al. demonstrated that restoration of fibroblast growth factor receptor 2IIIb (FGFR2IIIb) to PC-3 cells enhances their sensitivity to irradiation through acceleration of apoptosis and cell cycle arrest [244]. Timke et al. showed that the combined VEGF (SU5416) and PDGF (SU6668) receptor tyrosine kinase can improve the RT effect in PC-3 s.c animal model in vivo [245]. Imatinib mesylate (Gleevec, STI571) is a TKI. It was reported that STI571 inhibits IR-induced RelB nuclear translocation, leading to increased radiosensitivity in aggressive androgen-nonresponsive PC-3 and DU145 CaP cells [246]. Sunitinib, a potent inhibitor of several tyrosine kinase receptors, has demonstrated both antitumor and anti-angiogenic activity. Preclinical biochemical and cellular assay studies tested its activity against different kinases and proved it to be a potent inhibitor of all three members of the VEGFR family, both PDGFR α and β, C-KIT, and Fms-like tyrosine kinase-3 [282]. Brooks et al. found that Sunitinib modestly enhances the radiosensitivity of androgen-nonresponsive DU145 and PC-3 CaP cells, respectively, but does not sensitize the androgen-responsive LNCaP cells [248]. Sunitinib and RT do not interact directly to radiosensitize the PC-3 tumor cells in vivo [248].
7.3 Gene therapies
Several studies have demonstrated that the function of the p53 gene is one of the major determinants of intrinsic cellular sensitivity to the cytotoxic effects of IR. IR can induce p53 protein production, which can then result in either cell cycle arrest or apoptosis [283]. Colletier et al. demonstrated that adenoviral-mediated p53 (adv-p53) transgene expression sensitizes human p53 wild-type LNCaP and p53 null PC-3 CaP cells to IR in vitro and the radiosensitization is independent of p53 status [249]. It was reported that the combination of IR and wild-type p53 gene (Ad5CMV-p53) gene therapy results in remarkable synergistic effects in human CaP cells in vitro [250]. Kaliberov et al. reported that the human VEGF promoter element (AdVEGF-sKDR) can radiosensitize CaP cells in vitro and in vivo [251]. Anai et al. developed PC-3-Bcl2 and PC-3-Neo s.c xenograft modes and found that the combination of adenoviral vector-expressed PTEN (AdPTEN) and RT significantly inhibits xenograft tumor growth by the induction of apoptosis, inhibition of angiogenesis, and cellular proliferation [86]. Forced overexpression of PTEN has been shown in vitro and in vivo to downregulate Bcl-2, increase apoptosis, inhibit angiogenesis, and most importantly sensitize Bcl-2-overexpressing CaP cells to the killing effects of radiation [86]. These data indicate that gene therapy is a useful approach to increase the radiosensitivity in CaP radiation treatment.
7.4 Antisense therapies
Antisense (AS) therapy is another option for increasing radiosensitivity. Mu et al. found that AS-MDM2 sensitizes CaP cells not only to AD or RT given individually, but also to combination of AD and RT in vitro, makes this strategy ideal for the men with high-risk CaP [252]. Stoyanova et al. reported that AS-MDM2 sensitizes LNCaP CaP cells to AD, RT, and combination of AD and RT in vivo [256]. Truman et al. found that treatment of LNCaP, CWR22RV1, PC-3, and DU145 CaP cells with AS-ataxia telangiectasia mutated (ATM) oligonucleotides can reduce cellular ATM levels, which sensitizes human CaP cells to radiation-induced apoptosis [253]. Teimourian et al. demonstrate that AS-Hsp27 cDNA can reduce Hsp27 expression and significantly radiosensitize DU145 CaP cells in vitro [254].
AS-Bcl-2 oligodeoxynucleotide (ASODN) reagents have been shown to be effective in reducing Bcl-2 expression in a number of systems. Anai et al. demonstrated that combination of Bcl2-ASODN with IR sensitizes both PC-3-Bcl-2 and PC-3-Neo CaP cells to the killing effects of radiation in vitro and enhances radiation effect in two xenograft models in vivo [255]. E2F1 and MDM2 are two key proteins that promote apoptosis through common and independent apoptotic pathways. Both AS-MDM2 and adenoviral-mediated E2F1 (Ad-E2F1) combined with RT can significantly increase CaP cell death when exposed to RT and that this effect occurs regardless of AR and p53 status [257]. They further demonstrated that Ad-E2F1 overexpression sensitizes LNCaP and PC-3 CaP cells to RT in vivo [257].
7.5 Histone deacetylase inhibitors
Histone deacetylase inhibitors (HDACIs) are promising radiosensitizers. Chinnaiyan et al. demonstrated that the suberoylanilide hydroxamic acid (SAHA) can enhance radiation-induced cytotoxicity in DU145 CaP cells in vitro via inhibiting PI3K/Akt signaling pathway [259]. Konsoula et al. found that that H6CAHA (an adamantyl-hydroxamate histone deacetylase inhibitor) enhances the in vitro and in vivo sensitivity of CaP cells to RT while protecting normal cells from radiation-induced damage through modulating DNA damage repair processes [260]. Chen et al. showed that valproic acid (VPA) at low concentrations has minimal cytotoxic effects and can significantly increase radiation-induced apoptosis in CaP cell line in vitro and an animal model in vivo via a specific p53 acetylation and its mitochondrial-based pathway [261].
LBH589 (panobinostat) is another popular HDACI, a hydroxamic acid derivative and a novel pan-HDACI [284]. Our recently results indicate that LBH589 inhibited PC-3 and LNCaP CaP cell proliferation in a time- and-dose-dependent manner; low-dose of LBH589 (IC20) combined with RT greatly improved efficiency of cell killing in CaP cells; compared to RT alone, the combination treatment of LBH589 and RT induced more apoptosis and led to a steady increase of sub-G1 population and abolishment of RT-induced G2/M arrest, increased and persistent DSBs, less activation of Ku70/Ku80, and a panel of cell cycle related proteins (unpublished data). These data suggest that HDACIs are very promising radiosensitizers for future clinical trials for CaP therapy.
7.6 Natural products
(−)-Gossypol, a natural polyphenol product from cotton seed, has recently been identified as a small-molecule inhibitor of both Bcl-2 and Bcl-xL and potently induces apoptosis in several cancer cell lines [285, 286]. Studies indicated that (−)-Gossypol can radiosensitize PC-3 CaP cells in vitro and PC-3 s.c model in vivo without augmenting toxicity, suggesting that (−)-Gossypol combined with RT represents a promising novel anticancer regime for molecular targeted therapy of hormone-refractory CaP with Bcl-2/Bcl-xL overexpression [262]. Parthenolide is a major active component of the herbal medicine feverfew (Tanacetum parthenium) and has been shown to inhibit growth or induce apoptosis in a number of tumor cell lines [287, 288]. It was reported that the radiosensitization effect of parthenolide in CaP cells is mediated by NF-κB inhibition and enhanced by the presence of PTEN [84]. Romero et al. demonstrated that Trabectedin (ET-743), a natural product derived from the marine tunicate Ectenascidia turbinate, has significant in vitro radiosensitizing effect and induces cell cycle changes and apoptosis in several human cancer cell lines including DU145 CaP cell line [263].
A dehydroxymethyl derivative of epoxyquinomicin (DHMEQ) was from a natural product and is a novel and potent NF-kB inhibitor [289]. Kozakai et al. reported that DHMEQ enhances the therapeutic effect of radiation in CaP cells in vitro and in a s.c PC-3 animal mode in vivo via inhibiting NF-kB binding activity [264]. Chiu et al. showed that IR combined with MP (isolated from M. pilosus M93-fermented rice) increases the therapeutic efficacy compared to individual treatments in PC-3 CaP cells in vitro, and induces autophagy, ER stress, and enhanced DNA damage primarily via inhibition of the Akt/mTOR signaling pathways [265]. This combination treatment also demonstrated antitumor growth effects in a nude mouse PC-3 xenograft model [265].
7.7 Other novel agents
Hydroxymethylacylfulvene (HMAF; Irofulven, MGI 114) is a novel agent with alkylating activity and a potent inducer of apoptosis. The combination of HMAF with radiation can reduce the radiation dose needed for the same level of clonogenic survival up to 2.5-fold and induce more apoptosis compared with any single-treatment alone in CaP cell lines in vitro [266]. Genistein is an isoflavone, a major metabolite of soy produced by the intestinal bacteria, which is believed to be one of the anticancer agents found in soybeans [290]. Hillman et al. demonstrated that genistein combined with radiation inhibits DNA synthesis, resulting in inhibition of cell division and growth, and potentiates radiation effect on PC-3 CaP cells [267]. In the following study, they found that the mechanism of increased cell death by genistein and radiation is proposed to occur via inhibition of NF-κB, leading to altered expression of regulatory cell cycle proteins such as cyclin B and/or p21WAF1/Cip1, thus promoting G2/M arrest and increased radiosensitivity in PC-3 CaP cells [270]. They also showed that this combination treatment caused a significantly greater inhibition of primary tumor growth (87 %) in a PC-3 orthotopic model compared with genistein (30 %) or radiation (73 %) alone, and prevented lymph node metastasis [268]. However, it was discovered that pure genistein causes increased spontaneous metastasis to lymph nodes when given as a single modality [268, 291]. These findings indicate that genistein promotes metastatic spread from the primary tumor to regional lymph nodes via the lymphatic system.
Soy isoflavones (genistein, daidzein, and glycitein) as soy pills of similar composition are used in human interventions but not pure genistein. One study found that the combination of soy isoflavones with IR potentiates radiation-induced cell killing in PC-3 cells in vitro, enhances control of primary CaP growth and metastasis in vivo [273]. However, treatment with soy isoflavones did not increase lymph node metastasis in CaP orthotopic animal model [273], suggesting that soy isoflavones is more suitable for future clinical trials and has potential to improve CaP radiosensitivity. They also confirmed that the molecular mechanism of radiosensitization by soy isoflavones is through downregulation of apurinic/apyrimidinic endonuclease 1/redox factor-1 expression using a CaP cell line in vitro and a CaP animal model in vivo [292]. Algur et al. reported that the combined use of zoledronic acid and RT shows enhanced in vitro cytotoxicity for C4-2B CaP cell line compared with each treatment alone [269]. It was found that MG-132 enhances radiosensitivity in PC-3 CaP cells in vitro with concomitant NF-κB inhibition [271].
β-lapachone (β-lap) is a bioreductive anticancer drug. Suzuki et al. demonstrated the synergistic effects of RT and β-lap in DU145 CaP cells in vitro with two distinct mechanisms: first, radiation sensitizes cells to β-lap by upregulating NAD(P)H/quinone oxidoreductase 1 (NQO1), and second, β-lap sensitizes cells to radiation by inhibiting sublethal radiation damage (SLD) repair [272]. Nitric oxide donating nonsteroidal anti-inflammatory drugs (NO-NSAIDs) are novel pharmaceutical agents which were developed to allow NSAIDs to be better tolerated due to their associated gastroprotection. Stewart et al. demonstrated that NO-NSAID radiosensitises PC-3 sphere (CaP epithelial cells) but not prostate stromal cells in vitro and possible mechanisms for this effect could be the enhanced formation and reduced repair of radiation-induced DNA strand breaks and inhibition of the radioresistant hypoxia response [274]. Chiu et al. recently demonstrated that IR combined with ATO increases the therapeutic efficacy compared to individual treatments in LNCaP and PC-3 CaP cells, induces autophagy and apoptosis in LNCaP cells, and mainly induces autophagy in PC-3 cells through inhibition of the Akt/mTOR signaling pathways [5]. This combination treatment also demonstrated antitumor growth effects in a nude mouse PC-3 xenograft model [5].
8 Conclusions and future perspectives
Radiation remains an important modality for organ-confined or locally advanced CaP treatment with ongoing efforts towards designing new radiation treatment modalities and techniques which continue to improve the survival and quality of life of CaP patients. With the improved clinical outcomes of CaP treatment, minimizing RT-related toxicities has become a priority. RT has curative potential in treating CaP. However, tumor recurrences still frequently occur, requiring stratification of patients into different groups with distinct recurrence risk and further improvement of treatment methods to reduce the recurrence rate. If the biomarkers for predicting the treatment response of individual CaP patient and potential targets for radiosensitization are identified and further validated, it will achieve a more favorable therapeutic ratio in clinics. The future of radiation oncology is a close combination of modern treatment techniques, biomarker-guided personalized treatments, and metabolic/molecular imaging [293].
It is increasingly clear that a dynamic and multifactorial process is involved in the response of CaP cells to radiation. Emerging evidence suggests that PI3K/Akt/PTEN/mTOR signaling pathways, autophagy, EMT, and CSCs play important roles in CaP metastasis and progression and are related with radioresistance, and targeting these molecules or their corresponding pathways by gene therapy, antisense therapy, specific inhibitor, or other methods may enhance the radiosensitivity of CaP.
The PI3K/Akt/PTEN/mTOR pathway is implicated in all major mechanisms of radioresistance including CaP. Targeting this pathway is very promising for improving CaP radiosensitivity. In the future, using multiple inhibitors to target the signaling proteins in this pathway could improve the survival of CaP patients. The study of autophagy is a very exciting and highly promising area of cancer research. There has been much recent progress in our understanding the pathways that control autophagy. Further exploration of these pathways holds great potential for improving the treatment efficacy of IR in CaP. However, despite this potential, one of the most difficult questions remains to be answered: whether autophagy should be inhibited or stimulated to improve clinical outcomes? Thus, autophagy seems to play a pivotal role between survival and death processes: these processes, in fact, might be cell and tissue specific and highly dependent on the expression profile of genes and proteins regulating apoptosis. The interplay between apoptosis and autophagy is a very interesting area and needs to be further exploited in the future.
Since CSCs and EMT have both been implicated in tumorigenesis and radioresistance, it is critical to examine both populations and determine their expression of phenotypes in order to develop strategies to target these populations using targeting therapy. The rapid progress in EMT research and the various facets of innovative insights into the molecular mechanisms underlying EMT and metastasis will open novel avenues for the establishment of appropriate surrogate markers for improved diagnosis and prognosis, and, most importantly, for the design of specific antimetastasis therapies. Tanaka and colleagues have recently developed novel anti-N-cadherin MAbs, which are active in preclinical models of CRPC [161]. These MAbs could be also promising in improving CaP radiosensitivity. Yet, while we have made substantial progress in the understanding of the molecular mechanisms underlying EMT, we still lack sufficient insights into the functional contribution of EMT in cancer patients, especially in CaP radiation research.
The recent advances in CSCs have unlocked a new avenue for radiosensitivity research. Elucidating the role of CSCs in the cancer cells’ response to radiation will enhance our understanding of CaP recurrence after RT, and may direct research towards novel and specific radiosensitization agents that target CSCs. We expect that there will be increased understanding of the intrinsic and extrinsic factors that control the plasticity and maintenance of the CSC state (e.g., expression factors, miRNA expression, post-translational modifications of molecules that control stem cell fate, and niche factors that control stem cell renewal). It needs to be recognized that the complex mixture of radiosensitivity determining factors is probably highly dynamic during fractionated RT. Thus, the development of future therapeutic strategies based on targeting potential CSC radioresistance mechanisms must take into account these complex and dynamic processes, whereby different radioresistance pathways may be better targeted at different stages of therapy. In addition, if tumor and normal tissue stem cell regulatory pathways can be separately selectively targeted, then not only could CSCs be radiosensitized, but normal tissue stem cells could also be radioprotected to improve the therapeutic ratio. Furthermore, it may differ between tumor types, as well as between different individuals’ tumors within a tumor type. Therefore, any therapeutic strategy in the long term will need to take into account the biological features that control CSC behavior in each individual tumor (i.e., personalization of therapy).
With the advent of novel imaging technologies for CSCs [294], biology-guided RT planning may offer ways for specifically delivering high radiation doses to areas with high CSCs numbers. CSCs also offer novel targets to enhance the efficacy of RT [295] and future targeted therapies should have this aim in CaP radiation research. Targeting CSCs with radiation holds enormous potential for eventual cure for CaP patients.
Combination of RT with different radiosensitizers has demonstrated to be promising in preclinical studies with CaP cell lines and animal models. However, only very limited data could be found in phase I trials. These combination approaches should be further explored in clinical trials to validate their clinical effects in CaP therapy.
Abbreviations
- AD:
-
Androgen deprivation
- Ad-E2F1:
-
Adenoviral-mediated E2F1
- ALDH:
-
Aldehyde dehydrogenase
- AR:
-
Androgen receptor
- AS:
-
Antisense
- ASODN:
-
Antisense Bcl-2 oligodeoxynucleotide
- ATM:
-
Ataxia telangiectasia mutated
- ATO:
-
Arsenic trioxide
- BCR:
-
Biochemical recurrence
- BCRP:
-
Breast cancer resistance protein
- BCSCs:
-
Breast cancer stem cells
- bHLH:
-
Basic helix-loop-helix
- β-lap:
-
β-lapachone
- CaP:
-
Prostate cancer
- CD44v:
-
CD44 variants
- CK:
-
Cytoskeleton
- COX-2:
-
Cyclooxygenase-2
- CRPC:
-
Castration-resistant prostate cancer
- CSCs:
-
Cancer stem cells
- CTCs:
-
Circulating tumor cells
- DCA:
-
Dichloroacetate
- DHMEQ:
-
Dehydroxymethyl derivative of epoxyquinomicin
- Didox:
-
DX; 3,4-dihydroxybenzohydroxamic acid
- DSBs:
-
Double-strand breaks
- EBRT:
-
External beam radiotherapy
- EGFR:
-
Epidermal growth factor receptor
- EMT:
-
Epithelial–mesenchymal transition
- EpCAM:
-
Epithelial cell adhesion molecule
- ER:
-
Endoplasmic reticulum
- FACS:
-
Fluorescence-activated cell sorting
- FGFR2IIIb:
-
Fibroblast growth factor receptor 2IIIb
- FLT3:
-
Fms-like tyrosine kinase-3
- GKS:
-
Gamma knife surgery
- HCC:
-
Hepatocellular carcinoma
- HDACIs:
-
Histone deacetylase inhibitors
- HMAF:
-
Hydroxymethylacylfulvene
- HMG-CoA:
-
Hydroxyl-3-methylglutaryl coenzyme A
- HNSCC:
-
Head and neck squamous cell carcinoma
- IGF1R:
-
Insulin-like growth factor-type 1 receptor
- IGRT:
-
Image-guided radiation therapy
- IMRT:
-
Intensity modulated radiation therapy
- IR:
-
Ionizing radiation
- MAb:
-
Monoclonal antibody
- MACS:
-
Magnetic activated cell sorting
- MAPK:
-
Mitogen-activated protein kinase
- MET:
-
Mesenchymal to epithelial transition
- miRNA:
-
MicroRNA
- MP:
-
Monascuspiloin
- MRP-1:
-
Multidrug resistance protein 1
- mTOR:
-
Mammalian target of rapamycin
- NF-kB:
-
Nuclear factor-κB
- NOD/SCID:
-
Non-obese diabetic/severe combined immunodeficiency
- NO-NSAIDs:
-
Nitric oxide donating nonsteroidal anti-inflammatory drugs
- NQO1:
-
NAD(P)H:quinone oxidoreductase 1
- NSAIDs:
-
Nonsteroidal anti-inflammatory drugs
- P529:
-
Palomid 529
- p-Akt:
-
Phospho-Akt
- PAP:
-
Prostatic acid phosphatise
- PCR:
-
Polymerase chain reaction
- PDGF:
-
Platelet-derived growth factor
- PDK:
-
Pyruvate dehydrogenase kinase
- PI3K:
-
Phosphoinositide 3-kinase
- PKB:
-
Protein kinase B
- PSA:
-
Prostate-specific antigen
- PtdIns(3,4)P2:
-
Phosphatidylinositol 3,4-bisphosphate
- PtdIns(3,4,5)P3:
-
Phosphatidylinositol 3,4,5-trisphosphate
- PtdIns(4)P:
-
Phosphatidylinositol 4-phosphate
- PtdIns(4,5)P2:
-
Phosphatidylinositol 4,5-bisphosphate
- PTEN:
-
Phosphatase and tensin homolog
- RP:
-
Radical prostatectomy
- RR:
-
Radioresistant
- RT:
-
Radiation therapy
- SAHA:
-
Suberoylanilide hydroxamic acid
- s.c:
-
Subcutaneous
- siRNA:
-
Small interfering RNA
- SLD:
-
Sublethal radiation damage
- SSE:
-
Sodium selenite
- TGF-β:
-
Transforming growth factor-β
- TKIs:
-
Tyrosine kinase inhibitors
- TSC2:
-
Tuberous sclerosis complex 2
- VPA:
-
Valproic acid
- VEGFR:
-
Vascular endothelial growth factor receptor
References
Beltran, H., Beer, T. M., Carducci, M. A., de Bono, J., Gleave, M., Hussain, M., et al. (2011). New therapies for castration-resistant prostate cancer: efficacy and safety. European Urology, 60, 279–290.
Jemal, A., Bray, F., Center, M. M., Ferlay, J., Ward, E., & Forman, D. (2011). Global cancer statistics. CA: A Cancer Journal for Clinicians, 61, 69–90.
Catton, C., Milosevic, M., Warde, P., Bayley, A., Crook, J., Bristow, R., et al. (2003). Recurrent prostate cancer following external beam radiotherapy: follow-up strategies and management. The Urologic Clinics of North America, 30, 751–763.
Burgio, S. L., Fabbri, F., Seymour, I. J., Zoli, W., Amadori, D., & De Giorgi, U. (2012). Perspectives on mTOR inhibitors for castration-refractory prostate cancer. Current Cancer Drug Targets, 12, 940–949.
Chiu, H. W., Chen, Y. A., Ho, S. Y., & Wang, Y. J. (2012). Arsenic trioxide enhances the radiation sensitivity of androgen-dependent and -independent human prostate cancer cells. PloS ONE, 7, e31579.
Schiewer, M. J., Den, R., Hoang, D. T., Augello, M. A., Lawrence, Y. R., Dicker, A. P., et al. (2012). mTOR is a selective effector of the radiation therapy response in androgen receptor-positive prostate cancer. Endocrine-Related Cancer, 19, 1–12.
Griffin, C., McNulty, J., & Pandey, S. (2011). Pancratistatin induces apoptosis and autophagy in metastatic prostate cancer cells. International Journal of Oncology, 38, 1549–1556.
Armstrong, A. J., Marengo, M. S., Oltean, S., Kemeny, G., Bitting, R. L., Turnbull, J. D., et al. (2011). Circulating tumor cells from patients with advanced prostate and breast cancer display both epithelial and mesenchymal markers. Molecular Cancer Research: MCR, 9, 997–1007.
Nauseef, J. T., & Henry, M. D. (2011). Epithelial-to-mesenchymal transition in prostate cancer: paradigm or puzzle? Nature reviews. Urology, 8, 428–439.
Li, Y., Cozzi, P. J., & Russell, P. J. (2010). Promising tumor-associated antigens for future prostate cancer therapy. Medicinal Research Reviews, 30, 67–101.
Li, H., & Tang, D. G. (2011). Prostate cancer stem cells and their potential roles in metastasis. Journal of Surgical Oncology, 103, 558–562.
Xiao, W., Graham, P. H., Power, C. A., Hao, J., Kearsley, J. H., & Li, Y. (2012). CD44 is a biomarker associated with human prostate cancer radiation sensitivity. Clinical & Experimental Metastasis, 29, 1–9.
Dal Pra, A., Cury, F. L., & Souhami, L. (2010). Combining radiation therapy and androgen deprivation for localized prostate cancer—a critical review. Current Oncology, 17, 28–38.
Myklak, K., & Wilson, S. (2011). An update on the changing indications for androgen deprivation therapy for prostate cancer. Prostate Cancer, 2011, 419174.
Kupelian, P. A., Potters, L., Khuntia, D., Ciezki, J. P., Reddy, C. A., Reuther, A. M., et al. (2004). Radical prostatectomy, external beam radiotherapy <72 Gy, external beam radiotherapy > or =72 Gy, permanent seed implantation, or combined seeds/external beam radiotherapy for stage T1-T2 prostate cancer. International Journal of Radiation Oncology, Biology, Physics, 58, 25–33.
Djavan, B., Moul, J. W., Zlotta, A., Remzi, M., & Ravery, V. (2003). PSA progression following radical prostatectomy and radiation therapy: new standards in the new millennium. European Urology, 43, 12–27.
Khan, M. A., Han, M., Partin, A. W., Epstein, J. I., & Walsh, P. C. (2003). Long-term cancer control of radical prostatectomy in men younger than 50 years of age: update 2003. Urology, 62, 86–91. discussion 91-82.
Pollack, A., Zagars, G. K., Starkschall, G., Antolak, J. A., Lee, J. J., Huang, E., et al. (2002). Prostate cancer radiation dose response: results of the M. D. Anderson phase III randomized trial. International Journal of Radiation Oncology, Biology, Physics, 53, 1097–1105.
Forman, J. D., Yudelev, M., Bolton, S., Tekyi-Mensah, S., & Maughan, R. (2002). Fast neutron irradiation for prostate cancer. Cancer Metastasis Reviews, 21, 131–135.
Biagioli, M. C., & Hoffe, S. E. (2010). Emerging technologies in prostate cancer radiation therapy: improving the therapeutic window. Cancer Control: Journal of the Moffitt Cancer Center, 17, 223–232.
Gill, S., Thomas, J., Fox, C., Kron, T., Rolfo, A., Leahy, M., et al. (2011). Acute toxicity in prostate cancer patients treated with and without image-guided radiotherapy. Radiation Oncology (London, England), 6, 145.
Amin, N., & Konski, A. A. (2012). Intensity-modulated radiation therapy for prostate cancer is cost effective and improves therapeutic ratio. Expert Review of Pharmacoeconomics & Outcomes Research, 12, 447–450.
Sung, W., Park, J. M., Choi, C. H., Ha, S. W., & Ye, S. J. (2012). The effect of photon energy on intensity-modulated radiation therapy (IMRT) plans for prostate cancer. Radiation Oncology Journal, 30, 27–35.
Eade, T. N., Guo, L., Forde, E., Vaux, K., Vass, J., Hunt, P., et al. (2012). Image-guided dose-escalated intensity-modulated radiation therapy for prostate cancer: treating to doses beyond 78 Gy. BJU International, 109, 1655–1660.
Pisansky, T. M. (2006). External-beam radiotherapy for localized prostate cancer. The New England Journal of Medicine, 355, 1583–1591.
Spratt, D. E., Pei, X., Yamada, J., Kollmeier, M. A., Cox, B., & Zelefsky, M. J. (2012). Long-term survival and toxicity in patients treated with high-dose intensity modulated radiation therapy for localized prostate cancer. International Journal of Radiation Oncology, Biology, Physics, 85(3), 686–692.
Adkison, J. B., McHaffie, D. R., Bentzen, S. M., Patel, R. R., Khuntia, D., Petereit, D. G., et al. (2012). Phase I trial of pelvic nodal dose escalation with hypofractionated IMRT for high-risk prostate cancer. International Journal of Radiation Oncology, Biology, Physics, 82, 184–190.
Zelefsky, M. J., Kollmeier, M., Cox, B., Fidaleo, A., Sperling, D., Pei, X., et al. (2012). Improved clinical outcomes with high-dose image guided radiotherapy compared with non-IGRT for the treatment of clinically localized prostate cancer. International Journal of Radiation Oncology, Biology, Physics, 84, 125–129.
Kuban, D. A., Levy, L. B., Cheung, M. R., Lee, A. K., Choi, S., Frank, S., et al. (2011). Long-term failure patterns and survival in a randomized dose-escalation trial for prostate cancer. Who dies of disease? International Journal of Radiation Oncology, Biology, Physics, 79, 1310–1317.
Zapatero, A., Garcia-Vicente, F., Martin de Vidales, C., Cruz Conde, A., Ibanez, Y., Fernandez, I., et al. (2011). Long-term results after high-dose radiotherapy and adjuvant hormones in prostate cancer: how curable is high-risk disease? International Journal of Radiation Oncology, Biology, Physics, 81, 1279–1285.
Eade, T. N., Hanlon, A. L., Horwitz, E. M., Buyyounouski, M. K., Hanks, G. E., & Pollack, A. (2007). What dose of external-beam radiation is high enough for prostate cancer? International Journal of Radiation Oncology, Biology, Physics, 68, 682–689.
Coen, J. J., Bae, K., Zietman, A. L., Patel, B., Shipley, W. U., Slater, J. D., et al. (2011). Acute and late toxicity after dose escalation to 82 GyE using conformal proton radiation for localized prostate cancer: initial report of American College of Radiology Phase II study 03-12. International Journal of Radiation Oncology, Biology, Physics, 81, 1005–1009.
Yuan, T. L., & Cantley, L. C. (2008). PI3K pathway alterations in cancer: variations on a theme. Oncogene, 27, 5497–5510.
Jiang, B. H., Aoki, M., Zheng, J. Z., Li, J., & Vogt, P. K. (1999). Myogenic signaling of phosphatidylinositol 3-kinase requires the serine-threonine kinase Akt/protein kinase B. Proceedings of the National Academy of Sciences of the United States of America, 96, 2077–2081.
Lin, H. K., Hu, Y. C., Yang, L., Altuwaijri, S., Chen, Y. T., Kang, H. Y., et al. (2003). Suppression versus induction of androgen receptor functions by the phosphatidylinositol 3-kinase/Akt pathway in prostate cancer LNCaP cells with different passage numbers. The Journal of Biological Chemistry, 278, 50902–50907.
Nicholson, K. M., & Anderson, N. G. (2002). The protein kinase B/Akt signalling pathway in human malignancy. Cellular Signalling, 14, 381–395.
Martelli, A. M., Evangelisti, C., Chappell, W., Abrams, S. L., Basecke, J., Stivala, F., et al. (2011). Targeting the translational apparatus to improve leukemia therapy: roles of the PI3K/PTEN/Akt/mTOR pathway. Leukemia: Official Journal of the Leukemia Society of America, Leukemia Research Fund, UK, 25, 1064–1079.
Vivanco, I., & Sawyers, C. L. (2002). The phosphatidylinositol 3-kinase AKT pathway in human cancer. Nature Reviews Cancer, 2, 489–501.
Cantley, L. C. (2002). The phosphoinositide 3-kinase pathway. Science, 296, 1655–1657.
Pommery, N., & Henichart, J. P. (2005). Involvement of PI3K/Akt pathway in prostate cancer—potential strategies for developing targeted therapies. Mini Reviews in Medicinal Chemistry, 5, 1125–1132.
Fang, J., Ding, M., Yang, L., Liu, L. Z., & Jiang, B. H. (2007). PI3K/PTEN/AKT signaling regulates prostate tumor angiogenesis. Cellular Signalling, 19, 2487–2497.
Shukla, S., Maclennan, G. T., Hartman, D. J., Fu, P., Resnick, M. I., & Gupta, S. (2007). Activation of PI3K-Akt signaling pathway promotes prostate cancer cell invasion. International Journal of Cancer. Journal International Du Cancer, 121, 1424–1432.
McCall, P., Gemmell, L. K., Mukherjee, R., Bartlett, J. M., & Edwards, J. (2008). Phosphorylation of the androgen receptor is associated with reduced survival in hormone-refractory prostate cancer patients. British Journal of Cancer, 98, 1094–1101.
Lee, J. T., Jr., Steelman, L. S., & McCubrey, J. A. (2004). Phosphatidylinositol 3′-kinase activation leads to multidrug resistance protein-1 expression and subsequent chemoresistance in advanced prostate cancer cells. Cancer Research, 64, 8397–8404.
Murillo, H., Huang, H., Schmidt, L. J., Smith, D. I., & Tindall, D. J. (2001). Role of PI3K signaling in survival and progression of LNCaP prostate cancer cells to the androgen refractory state. Endocrinology, 142, 4795–4805.
Dubrovska, A., Kim, S., Salamone, R. J., Walker, J. R., Maira, S. M., Garcia-Echeverria, C., et al. (2009). The role of PTEN/Akt/PI3K signaling in the maintenance and viability of prostate cancer stem-like cell populations. Proceedings of the National Academy of Sciences of the United States of America, 106, 268–273.
McKenna, W. G., Muschel, R. J., Gupta, A. K., Hahn, S. M., & Bernhard, E. J. (2003). The RAS signal transduction pathway and its role in radiation sensitivity. Oncogene, 22, 5866–5875.
Cheng, J. C., Chou, C. H., Kuo, M. L., & Hsieh, C. Y. (2006). Radiation-enhanced hepatocellular carcinoma cell invasion with MMP-9 expression through PI3K/Akt/NF-kappaB signal transduction pathway. Oncogene, 25, 7009–7018.
Bussink, J., van der Kogel, A. J., & Kaanders, J. H. (2008). Activation of the PI3-K/AKT pathway and implications for radioresistance mechanisms in head and neck cancer. The Lancet Oncology, 9, 288–296.
Gottschalk, A. R., Doan, A., Nakamura, J. L., Stokoe, D., & Haas-Kogan, D. A. (2005). Inhibition of phosphatidylinositol-3-kinase causes increased sensitivity to radiation through a PKB-dependent mechanism. International Journal of Radiation Oncology, Biology, Physics, 63, 1221–1227.
Geng, L., Tan, J., Himmelfarb, E., Schueneman, A., Niermann, K., Brousal, J., et al. (2004). A specific antagonist of the p110delta catalytic component of phosphatidylinositol 3′-kinase, IC486068, enhances radiation-induced tumor vascular destruction. Cancer Research, 64, 4893–4899.
Soond, D. R., Bjorgo, E., Moltu, K., Dale, V. Q., Patton, D. T., Torgersen, K. M., et al. (2010). PI3K p110delta regulates T-cell cytokine production during primary and secondary immune responses in mice and humans. Blood, 115, 2203–2213.
Wang, J., Yang, L., Yang, J., Kuropatwinski, K., Wang, W., Liu, X. Q., et al. (2008). Transforming growth factor beta induces apoptosis through repressing the phosphoinositide 3-kinase/AKT/survivin pathway in colon cancer cells. Cancer Research, 68, 3152–3160.
Scheid, M. P., & Woodgett, J. R. (2003). Unravelling the activation mechanisms of protein kinase B/Akt. FEBS Letters, 546, 108–112.
Lee, J. T., Lehmann, B. D., Terrian, D. M., Chappell, W. H., Stivala, F., Libra, M., et al. (2008). Targeting prostate cancer based on signal transduction and cell cycle pathways. Cell Cycle, 7, 1745–1762.
Mathew, R., Karantza-Wadsworth, V., & White, E. (2007). Role of autophagy in cancer. Nature Reviews Cancer, 7, 961–967.
Kondo, Y., Kanzawa, T., Sawaya, R., & Kondo, S. (2005). The role of autophagy in cancer development and response to therapy. Nature Reviews Cancer, 5, 726–734.
Takeuchi, H., Kondo, Y., Fujiwara, K., Kanzawa, T., Aoki, H., Mills, G. B., et al. (2005). Synergistic augmentation of rapamycin-induced autophagy in malignant glioma cells by phosphatidylinositol 3-kinase/protein kinase B inhibitors. Cancer Research, 65, 3336–3346.
Nakashio, A., Fujita, N., Rokudai, S., Sato, S., & Tsuruo, T. (2000). Prevention of phosphatidylinositol 3′-kinase-Akt survival signaling pathway during topotecan-induced apoptosis. Cancer Research, 60, 5303–5309.
Janmaat, M. L., Kruyt, F. A., Rodriguez, J. A., & Giaccone, G. (2003). Response to epidermal growth factor receptor inhibitors in non-small cell lung cancer cells: limited antiproliferative effects and absence of apoptosis associated with persistent activity of extracellular signal-regulated kinase or Akt kinase pathways. Clinical Cancer Research: An Official Journal of the American Association for Cancer Research, 9, 2316–2326.
Bjornsti, M. A., & Houghton, P. J. (2004). The TOR pathway: a target for cancer therapy. Nature Reviews Cancer, 4, 335–348.
Xue, Q., Hopkins, B., Perruzzi, C., Udayakumar, D., Sherris, D., & Benjamin, L. E. (2008). Palomid 529, a novel small-molecule drug, is a TORC1/TORC2 inhibitor that reduces tumor growth, tumor angiogenesis, and vascular permeability. Cancer Research, 68, 9551–9557.
Diaz, R., Nguewa, P. A., Diaz-Gonzalez, J. A., Hamel, E., Gonzalez-Moreno, O., Catena, R., et al. (2009). The novel Akt inhibitor Palomid 529 (P529) enhances the effect of radiotherapy in prostate cancer. British Journal of Cancer, 100, 932–940.
Steelman, L. S., Bertrand, F. E., & McCubrey, J. A. (2004). The complexity of PTEN: mutation, marker and potential target for therapeutic intervention. Expert Opinion on Therapeutic Targets, 8, 537–550.
Sansal, I., & Sellers, W. R. (2004). The biology and clinical relevance of the PTEN tumor suppressor pathway. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology, 22, 2954–2963.
Birck, A., Ahrenkiel, V., Zeuthen, J., Hou-Jensen, K., & Guldberg, P. (2000). Mutation and allelic loss of the PTEN/MMAC1 gene in primary and metastatic melanoma biopsies. The Journal of Investigative Dermatology, 114, 277–280.
Harima, Y., Sawada, S., Nagata, K., Sougawa, M., Ostapenko, V., & Ohnishi, T. (2001). Mutation of the PTEN gene in advanced cervical cancer correlated with tumor progression and poor outcome after radiotherapy. International Journal of Oncology, 18, 493–497.
Byun, D. S., Cho, K., Ryu, B. K., Lee, M. G., Park, J. I., Chae, K. S., et al. (2003). Frequent monoallelic deletion of PTEN and its reciprocal associatioin with PIK3CA amplification in gastric carcinoma. International Journal of Cancer. Journal International Du Cancer, 104, 318–327.
Pedrero, J. M., Carracedo, D. G., Pinto, C. M., Zapatero, A. H., Rodrigo, J. P., Nieto, C. S., et al. (2005). Frequent genetic and biochemical alterations of the PI 3-K/AKT/PTEN pathway in head and neck squamous cell carcinoma. International Journal of Cancer. Journal International Du Cancer, 114, 242–248.
Sircar, K., Yoshimoto, M., Monzon, F. A., Koumakpayi, I. H., Katz, R. L., Khanna, A., et al. (2009). PTEN genomic deletion is associated with p-Akt and AR signalling in poorer outcome, hormone refractory prostate cancer. The Journal of Pathology, 218, 505–513.
de Muga, S., Hernandez, S., Agell, L., Salido, M., Juanpere, N., Lorenzo, M., et al. (2010). Molecular alterations of EGFR and PTEN in prostate cancer: association with high-grade and advanced-stage carcinomas. Modern Pathology: An Official Journal of the United States and Canadian Academy of Pathology, Inc, 23, 703–712.
Reid, A. H., Attard, G., Ambroisine, L., Fisher, G., Kovacs, G., Brewer, D., et al. (2010). Molecular characterisation of ERG, ETV1 and PTEN gene loci identifies patients at low and high risk of death from prostate cancer. British Journal of Cancer, 102, 678–684.
Wang, S., Gao, J., Lei, Q., Rozengurt, N., Pritchard, C., Jiao, J., et al. (2003). Prostate-specific deletion of the murine Pten tumor suppressor gene leads to metastatic prostate cancer. Cancer Cell, 4, 209–221.
Gray, I. C., Stewart, L. M., Phillips, S. M., Hamilton, J. A., Gray, N. E., Watson, G. J., et al. (1998). Mutation and expression analysis of the putative prostate tumour-suppressor gene PTEN. British Journal of Cancer, 78, 1296–1300.
Faratian, D., Goltsov, A., Lebedeva, G., Sorokin, A., Moodie, S., Mullen, P., et al. (2009). Systems biology reveals new strategies for personalizing cancer medicine and confirms the role of PTEN in resistance to trastuzumab. Cancer Research, 69, 6713–6720.
Sos, M. L., Koker, M., Weir, B. A., Heynck, S., Rabinovsky, R., Zander, T., et al. (2009). PTEN loss contributes to erlotinib resistance in EGFR-mutant lung cancer by activation of Akt and EGFR. Cancer Research, 69, 3256–3261.
Loupakis, F., Pollina, L., Stasi, I., Ruzzo, A., Scartozzi, M., Santini, D., et al. (2009). PTEN expression and KRAS mutations on primary tumors and metastases in the prediction of benefit from cetuximab plus irinotecan for patients with metastatic colorectal cancer. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology, 27, 2622–2629.
Negri, F. V., Bozzetti, C., Lagrasta, C. A., Crafa, P., Bonasoni, M. P., Camisa, R., et al. (2010). PTEN status in advanced colorectal cancer treated with cetuximab. British Journal of Cancer, 102, 162–164.
Mao, C., Liao, R. Y., & Chen, Q. (2010). Loss of PTEN expression predicts resistance to EGFR-targeted monoclonal antibodies in patients with metastatic colorectal cancer. British Journal of Cancer, 102, 940.
Li, H. F., Kim, J. S., & Waldman, T. (2009). Radiation-induced Akt activation modulates radioresistance in human glioblastoma cells. Radiation Oncology, 4, 43.
Zafarana, G., Ishkanian, A. S., Malloff, C. A., Locke, J. A., Sykes, J., Thoms, J., et al. (2012). Copy number alterations of c-MYC and PTEN are prognostic factors for relapse after prostate cancer radiotherapy. Cancer, 118, 4053–4062.
Teng, D. H., Hu, R., Lin, H., Davis, T., Iliev, D., Frye, C., et al. (1997). MMAC1/PTEN mutations in primary tumor specimens and tumor cell lines. Cancer Research, 57, 5221–5225.
Jendrossek, V., Henkel, M., Hennenlotter, J., Vogel, U., Ganswindt, U., Muller, I., et al. (2008). Analysis of complex protein kinase B signalling pathways in human prostate cancer samples. BJU International, 102, 371–382.
Sun, Y., St Clair, D. K., Fang, F., Warren, G. W., Rangnekar, V. M., Crooks, P. A., et al. (2007). The radiosensitization effect of parthenolide in prostate cancer cells is mediated by nuclear factor-kappaB inhibition and enhanced by the presence of PTEN. Molecular Cancer Therapeutics, 6, 2477–2486.
Rosser, C. J., Tanaka, M., Pisters, L. L., Tanaka, N., Levy, L. B., Hoover, D. C., et al. (2004). Adenoviral-mediated PTEN transgene expression sensitizes Bcl-2-expressing prostate cancer cells to radiation. Cancer Gene Therapy, 11, 273–279.
Anai, S., Goodison, S., Shiverick, K., Iczkowski, K., Tanaka, M., & Rosser, C. J. (2006). Combination of PTEN gene therapy and radiation inhibits the growth of human prostate cancer xenografts. Human Gene Therapy, 17, 975–984.
Tomioka, A., Tanaka, M., De Velasco, M. A., Anai, S., Takada, S., Kushibiki, T., et al. (2008). Delivery of PTEN via a novel gene microcapsule sensitizes prostate cancer cells to irradiation. Molecular Cancer Therapeutics, 7, 1864–1870.
Guertin, D. A., & Sabatini, D. M. (2007). Defining the role of mTOR in cancer. Cancer Cell, 12, 9–22.
Hay, N., & Sonenberg, N. (2004). Upstream and downstream of mTOR. Genes & Development, 18, 1926–1945.
Shen, C., Lancaster, C. S., Shi, B., Guo, H., Thimmaiah, P., & Bjornsti, M. A. (2007). TOR signaling is a determinant of cell survival in response to DNA damage. Molecular and Cellular Biology, 27, 7007–7017.
Martelli, A. M., Evangelisti, C., Chiarini, F., Grimaldi, C., Cappellini, A., Ognibene, A., et al. (2010). The emerging role of the phosphatidylinositol 3-kinase/Akt/mammalian target of rapamycin signaling network in normal myelopoiesis and leukemogenesis. Biochimica Et Biophysica Acta, 1803, 991–1002.
Tokunaga, E., Kimura, Y., Mashino, K., Oki, E., Kataoka, A., Ohno, S., et al. (2006). Activation of PI3K/Akt signaling and hormone resistance in breast cancer. Breast Cancer, 13, 137–144.
Kremer, C. L., Klein, R. R., Mendelson, J., Browne, W., Samadzedeh, L. K., Vanpatten, K., et al. (2006). Expression of mTOR signaling pathway markers in prostate cancer progression. The Prostate, 66, 1203–1212.
Brognard, J., Clark, A. S., Ni, Y., & Dennis, P. A. (2001). Akt/protein kinase B is constitutively active in non-small cell lung cancer cells and promotes cellular survival and resistance to chemotherapy and radiation. Cancer Research, 61, 3986–3997.
Tanno, S., Yanagawa, N., Habiro, A., Koizumi, K., Nakano, Y., Osanai, M., et al. (2004). Serine/threonine kinase AKT is frequently activated in human bile duct cancer and is associated with increased radioresistance. Cancer Research, 64, 3486–3490.
Chakravarti, A., Zhai, G., Suzuki, Y., Sarkesh, S., Black, P. M., Muzikansky, A., et al. (2004). The prognostic significance of phosphatidylinositol 3-kinase pathway activation in human gliomas. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology, 22, 1926–1933.
Gupta, A. K., McKenna, W. G., Weber, C. N., Feldman, M. D., Goldsmith, J. D., Mick, R., et al. (2002). Local recurrence in head and neck cancer: relationship to radiation resistance and signal transduction. Clinical Cancer Research: An Official Journal of the American Association for Cancer Research, 8, 885–892.
Gupta, A. K., Soto, D. E., Feldman, M. D., Goldsmith, J. D., Mick, R., Hahn, S. M., et al. (2004). Signaling pathways in NSCLC as a predictor of outcome and response to therapy. Lung, 182, 151–162.
Gozuacik, D., & Kimchi, A. (2004). Autophagy as a cell death and tumor suppressor mechanism. Oncogene, 23, 2891–2906.
Moretti, L., Attia, A., Kim, K. W., & Lu, B. (2007). Crosstalk between Bak/Bax and mTOR signaling regulates radiation-induced autophagy. Autophagy, 3, 142–144.
Cao, C., Subhawong, T., Albert, J. M., Kim, K. W., Geng, L., Sekhar, K. R., et al. (2006). Inhibition of mammalian target of rapamycin or apoptotic pathway induces autophagy and radiosensitizes PTEN null prostate cancer cells. Cancer Research, 66, 10040–10047.
Hait, W. N., Jin, S., & Yang, J. M. (2006). A matter of life or death (or both): understanding autophagy in cancer. Clinical Cancer Research: An Official Journal of the American Association for Cancer Research, 12, 1961–1965.
Ito, H., Daido, S., Kanzawa, T., Kondo, S., & Kondo, Y. (2005). Radiation-induced autophagy is associated with LC3 and its inhibition sensitizes malignant glioma cells. International Journal of Oncology, 26, 1401–1410.
Kuwahara, Y., Oikawa, T., Ochiai, Y., Roudkenar, M. H., Fukumoto, M., Shimura, T., et al. (2011). Enhancement of autophagy is a potential modality for tumors refractory to radiotherapy. Cell Death & Disease, 2, e177.
White, E. (2012). Deconvoluting the context-dependent role for autophagy in cancer. Nature Reviews Cancer, 12, 401–410.
Zhou, S., Zhao, L., Kuang, M., Zhang, B., Liang, Z., Yi, T., et al. (2012). Autophagy in tumorigenesis and cancer therapy: Dr. Jekyll or Mr. Hyde? Cancer Letters, 323, 115–127.
Kroemer, G., & Levine, B. (2008). Autophagic cell death: the story of a misnomer. Nature Reviews Molecular Cell Biology, 9, 1004–1010.
Kimmelman, A. C. (2011). The dynamic nature of autophagy in cancer. Genes & Development, 25, 1999–2010.
Jin, S., & White, E. (2007). Role of autophagy in cancer: management of metabolic stress. Autophagy, 3, 28–31.
Chen, N., & Karantza, V. (2011). Autophagy as a therapeutic target in cancer. Cancer Biology & Therapy, 11, 157–168.
Levine, B. (2006). Unraveling the role of autophagy in cancer. Autophagy, 2, 65–66.
Chen, N., & Karantza-Wadsworth, V. (2009). Role and regulation of autophagy in cancer. Biochimica Et Biophysica Acta, 1793, 1516–1523.
Rosenfeldt, M. T., & Ryan, K. M. (2011). The multiple roles of autophagy in cancer. Carcinogenesis, 32, 955–963.
Apel, A., Herr, I., Schwarz, H., Rodemann, H. P., & Mayer, A. (2008). Blocked autophagy sensitizes resistant carcinoma cells to radiation therapy. Cancer Research, 68, 1485–1494.
Rami, A. (2009). Review: autophagy in neurodegeneration: firefighter and/or incendiarist? Neuropathology and Applied Neurobiology, 35, 449–461.
Maiuri, M. C., Criollo, A., & Kroemer, G. (2010). Crosstalk between apoptosis and autophagy within the Beclin 1 interactome. The EMBO Journal, 29, 515–516.
Fimia, G. M., & Piacentini, M. (2010). Regulation of autophagy in mammals and its interplay with apoptosis. Cellular and Molecular Life Sciences: CMLS, 67, 1581–1588.
Yang, Z. J., Chee, C. E., Huang, S., & Sinicrope, F. (2011). Autophagy modulation for cancer therapy. Cancer Biology & Therapy, 11, 169–176.
Arico, S., Petiot, A., Bauvy, C., Dubbelhuis, P. F., Meijer, A. J., Codogno, P., et al. (2001). The tumor suppressor PTEN positively regulates macroautophagy by inhibiting the phosphatidylinositol 3-kinase/protein kinase B pathway. The Journal of Biological Chemistry, 276, 35243–35246.
Ueno, T., Sato, W., Horie, Y., Komatsu, M., Tanida, I., Yoshida, M., et al. (2008). Loss of Pten, a tumor suppressor, causes the strong inhibition of autophagy without affecting LC3 lipidation. Autophagy, 4, 692–700.
Laane, E., Tamm, K. P., Buentke, E., Ito, K., Kharaziha, P., Oscarsson, J., et al. (2009). Cell death induced by dexamethasone in lymphoid leukemia is mediated through initiation of autophagy. Cell Death and Differentiation, 16, 1018–1029.
Paglin, S., Lee, N. Y., Nakar, C., Fitzgerald, M., Plotkin, J., Deuel, B., et al. (2005). Rapamycin-sensitive pathway regulates mitochondrial membrane potential, autophagy, and survival in irradiated MCF-7 cells. Cancer Research, 65, 11061–11070.
Iwamaru, A., Kondo, Y., Iwado, E., Aoki, H., Fujiwara, K., Yokoyama, T., et al. (2007). Silencing mammalian target of rapamycin signaling by small interfering RNA enhances rapamycin-induced autophagy in malignant glioma cells. Oncogene, 26, 1840–1851.
Kuo, H. P., Lee, D. F., Chen, C. T., Liu, M., Chou, C. K., Lee, H. J., et al. (2010). ARD1 stabilization of TSC2 suppresses tumorigenesis through the mTOR signaling pathway. Science Signaling, 3, ra9.
Ganley, I. G., Lam du, H., Wang, J., Ding, X., Chen, S., & Jiang, X. (2009). ULK1.ATG13.FIP200 complex mediates mTOR signaling and is essential for autophagy. The Journal of Biological Chemistry, 284, 12297–12305.
Jung, C. H., Jun, C. B., Ro, S. H., Kim, Y. M., Otto, N. M., Cao, J., et al. (2009). ULK-Atg13-FIP200 complexes mediate mTOR signaling to the autophagy machinery. Molecular Biology of the Cell, 20, 1992–2003.
Palumbo, S., & Comincini, S. (2013). Autophagy and ionizing radiation in tumors: the “survive or not survive” dilemma. Journal of Cellular Physiology, 228, 1–8.
Kim, K. W., Moretti, L., Mitchell, L. R., Jung, D. K., & Lu, B. (2010). Endoplasmic reticulum stress mediates radiation-induced autophagy by perk-eIF2alpha in caspase-3/7-deficient cells. Oncogene, 29, 3241–3251.
Lomonaco, S. L., Finniss, S., Xiang, C., Decarvalho, A., Umansky, F., Kalkanis, S. N., et al. (2009). The induction of autophagy by gamma-radiation contributes to the radioresistance of glioma stem cells. International Journal of Cancer. Journal International Du Cancer, 125, 717–722.
Gewirtz, D. A., Hilliker, M. L., & Wilson, E. N. (2009). Promotion of autophagy as a mechanism for radiation sensitization of breast tumor cells. Radiotherapy and Oncology: Journal of the European Society for Therapeutic Radiology and Oncology, 92, 323–328.
Chaachouay, H., Ohneseit, P., Toulany, M., Kehlbach, R., Multhoff, G., & Rodemann, H. P. (2011). Autophagy contributes to resistance of tumor cells to ionizing radiation. Radiotherapy and Oncology: Journal of the European Society for Therapeutic Radiology and Oncology, 99, 287–292.
Gwak, H. S., Kim, T. H., Jo, G. H., Kim, Y. J., Kwak, H. J., Kim, J. H., et al. (2012). Silencing of microRNA-21 confers radio-sensitivity through inhibition of the PI3K/AKT pathway and enhancing autophagy in malignant glioma cell lines. PloS ONE, 7, e47449.
Parikh, A., Childress, C., Deitrick, K., Lin, Q., Rukstalis, D., & Yang, W. (2010). Statin-induced autophagy by inhibition of geranylgeranyl biosynthesis in prostate cancer PC3 cells. The Prostate, 70, 971–981.
Toepfer, N., Childress, C., Parikh, A., Rukstalis, D., & Yang, W. (2011). Atorvastatin induces autophagy in prostate cancer PC3 cells through activation of LC3 transcription. Cancer Biology & Therapy, 12, 691–699.
He, Z., Mangala, L. S., Theriot, C. A., Rohde, L. H., Wu, H., & Zhang, Y. (2012). Cell killing and radiosensitizing effects of atorvastatin in PC3 prostate cancer cells. Journal of Radiation Research, 53, 225–233.
Wu, W. K., Coffelt, S. B., Cho, C. H., Wang, X. J., Lee, C. W., Chan, F. K., et al. (2012). The autophagic paradox in cancer therapy. Oncogene, 31, 939–953.
Zeisberg, M., & Neilson, E. G. (2009). Biomarkers for epithelial-mesenchymal transitions. The Journal of Clinical Investigation, 119, 1429–1437.
Mani, S. A., Guo, W., Liao, M. J., Eaton, E. N., Ayyanan, A., Zhou, A. Y., et al. (2008). The epithelial-mesenchymal transition generates cells with properties of stem cells. Cell, 133, 704–715.
Santisteban, M., Reiman, J. M., Asiedu, M. K., Behrens, M. D., Nassar, A., Kalli, K. R., et al. (2009). Immune-induced epithelial to mesenchymal transition in vivo generates breast cancer stem cells. Cancer Research, 69, 2887–2895.
Brabletz, T., Jung, A., Spaderna, S., Hlubek, F., & Kirchner, T. (2005). Opinion: migrating cancer stem cells—an integrated concept of malignant tumour progression. Nature Reviews Cancer, 5, 744–749.
Schmalhofer, O., Brabletz, S., & Brabletz, T. (2009). E-cadherin, beta-catenin, and ZEB1 in malignant progression of cancer. Cancer Metastasis Reviews, 28, 151–166.
Kwok, W. K., Ling, M. T., Lee, T. W., Lau, T. C., Zhou, C., Zhang, X., et al. (2005). Up-regulation of TWIST in prostate cancer and its implication as a therapeutic target. Cancer Research, 65, 5153–5162.
Alexander, N. R., Tran, N. L., Rekapally, H., Summers, C. E., Glackin, C., & Heimark, R. L. (2006). N-cadherin gene expression in prostate carcinoma is modulated by integrin-dependent nuclear translocation of Twist1. Cancer Research, 66, 3365–3369.
Mulholland, D. J., Kobayashi, N., Ruscetti, M., Zhi, A., Tran, L. M., Huang, J., et al. (2012). Pten loss and RAS/MAPK activation cooperate to promote EMT and metastasis initiated from prostate cancer stem/progenitor cells. Cancer Research, 72, 1878–1889.
Byles, V., Zhu, L., Lovaas, J. D., Chmilewski, L. K., Wang, J., Faller, D. V., et al. (2012). SIRT1 induces EMT by cooperating with EMT transcription factors and enhances prostate cancer cell migration and metastasis. Oncogene, 31, 4619–4629.
Hugo, H., Ackland, M. L., Blick, T., Lawrence, M. G., Clements, J. A., Williams, E. D., et al. (2007). Epithelial—mesenchymal and mesenchymal—epithelial transitions in carcinoma progression. Journal of Cellular Physiology, 213, 374–383.
Mimeault, M., & Batra, S. K. (2011). Frequent gene products and molecular pathways altered in prostate cancer- and metastasis-initiating cells and their progenies and novel promising multitargeted therapies. Molecular Medicine, 17, 949–964.
Drake, J. M., Barnes, J. M., Madsen, J. M., Domann, F. E., Stipp, C. S., & Henry, M. D. (2010). ZEB1 coordinately regulates laminin-332 and {beta}4 integrin expression altering the invasive phenotype of prostate cancer cells. The Journal of Biological Chemistry, 285, 33940–33948.
Xu, J., Wang, R., Xie, Z. H., Odero-Marah, V., Pathak, S., Multani, A., et al. (2006). Prostate cancer metastasis: role of the host microenvironment in promoting epithelial to mesenchymal transition and increased bone and adrenal gland metastasis. The Prostate, 66, 1664–1673.
Acevedo, V. D., Gangula, R. D., Freeman, K. W., Li, R., Zhang, Y., Wang, F., et al. (2007). Inducible FGFR-1 activation leads to irreversible prostate adenocarcinoma and an epithelial-to-mesenchymal transition. Cancer Cell, 12, 559–571.
Zhang, Q., Helfand, B. T., Jang, T. L., Zhu, L. J., Chen, L., Yang, X. J., et al. (2009). Nuclear factor-kappaB-mediated transforming growth factor-beta-induced expression of vimentin is an independent predictor of biochemical recurrence after radical prostatectomy. Clinical Cancer Research: An Official Journal of the American Association for Cancer Research, 15, 3557–3567.
Mak, P., Leav, I., Pursell, B., Bae, D., Yang, X., Taglienti, C. A., et al. (2010). ERbeta impedes prostate cancer EMT by destabilizing HIF-1alpha and inhibiting VEGF-mediated snail nuclear localization: implications for Gleason grading. Cancer Cell, 17, 319–332.
Lue, H. W., Yang, X., Wang, R., Qian, W., Xu, R. Z., Lyles, R., et al. (2011). LIV-1 promotes prostate cancer epithelial-to-mesenchymal transition and metastasis through HB-EGF shedding and EGFR-mediated ERK signaling. PloS ONE, 6, e27720.
Xie, D., Gore, C., Liu, J., Pong, R. C., Mason, R., Hao, G., et al. (2010). Role of DAB2IP in modulating epithelial-to-mesenchymal transition and prostate cancer metastasis. Proceedings of the National Academy of Sciences of the United States of America, 107, 2485–2490.
Graham, T. R., Zhau, H. E., Odero-Marah, V. A., Osunkoya, A. O., Kimbro, K. S., Tighiouart, M., et al. (2008). Insulin-like growth factor-I-dependent up-regulation of ZEB1 drives epithelial-to-mesenchymal transition in human prostate cancer cells. Cancer Research, 68, 2479–2488.
Contreras, H. R., Ledezma, R. A., Vergara, J., Cifuentes, F., Barra, C., Cabello, P., et al. (2010). The expression of syndecan-1 and -2 is associated with Gleason score and epithelial-mesenchymal transition markers, E-cadherin and beta-catenin, in prostate cancer. Urologic Oncology, 28, 534–540.
Sun, Y., Wang, B. E., Leong, K. G., Yue, P., Li, L., Jhunjhunwala, S., et al. (2012). Androgen deprivation causes epithelial-mesenchymal transition in the prostate: implications for androgen-deprivation therapy. Cancer Research, 72, 527–536.
Behnsawy, H. M., Miyake, H., Harada, K. I., & Fujisawa, M. (2012). Expression patterns of epithelial-mesenchymal transition markers in localized prostate cancer: significance in clinicopathological outcomes following radical prostatectomy. BJU International, 111, 30–37.
Sethi, S., Macoska, J., Chen, W., & Sarkar, F. H. (2010). Molecular signature of epithelial-mesenchymal transition (EMT) in human prostate cancer bone metastasis. American Journal of Translational Research, 3, 90–99.
Zhu, M. L., & Kyprianou, N. (2010). Role of androgens and the androgen receptor in epithelial-mesenchymal transition and invasion of prostate cancer cells. FASEB Journal: Official Publication of the Federation of American Societies for Experimental Biology, 24, 769–777.
Tanaka, H., Kono, E., Tran, C. P., Miyazaki, H., Yamashiro, J., Shimomura, T., et al. (2010). Monoclonal antibody targeting of N-cadherin inhibits prostate cancer growth, metastasis and castration resistance. Nature Medicine, 16, 1414–1420.
Barcellos-Hoff, M. H., Park, C., & Wright, E. G. (2005). Radiation and the microenvironment—tumorigenesis and therapy. Nature Reviews Cancer, 5, 867–875.
Madani, I., De Neve, W., & Mareel, M. (2008). Does ionizing radiation stimulate cancer invasion and metastasis? Bulletin Du Cancer, 95, 292–300.
Escriva, M., Peiro, S., Herranz, N., Villagrasa, P., Dave, N., Montserrat-Sentis, B., et al. (2008). Repression of PTEN phosphatase by Snail1 transcriptional factor during gamma radiation-induced apoptosis. Molecular and Cellular Biology, 28, 1528–1540.
Kurrey, N. K., Jalgaonkar, S. P., Joglekar, A. V., Ghanate, A. D., Chaskar, P. D., Doiphode, R. Y., et al. (2009). Snail and slug mediate radioresistance and chemoresistance by antagonizing p53-mediated apoptosis and acquiring a stem-like phenotype in ovarian cancer cells. Stem Cells, 27, 2059–2068.
Creighton, C. J., Chang, J. C., & Rosen, J. M. (2010). Epithelial-mesenchymal transition (EMT) in tumor-initiating cells and its clinical implications in breast cancer. Journal of Mammary Gland Biology and Neoplasia, 15, 253–260.
Andarawewa, K. L., Erickson, A. C., Chou, W. S., Costes, S. V., Gascard, P., Mott, J. D., et al. (2007). Ionizing radiation predisposes nonmalignant human mammary epithelial cells to undergo transforming growth factor beta induced epithelial to mesenchymal transition. Cancer Research, 67, 8662–8670.
Tsukamoto, H., Shibata, K., Kajiyama, H., Terauchi, M., Nawa, A., & Kikkawa, F. (2007). Irradiation-induced epithelial-mesenchymal transition (EMT) related to invasive potential in endometrial carcinoma cells. Gynecologic Oncology, 107, 500–504.
Zhang, X., Li, X., Zhang, N., Yang, Q., & Moran, M. S. (2011). Low doses ionizing radiation enhances the invasiveness of breast cancer cells by inducing epithelial-mesenchymal transition. Biochemical and Biophysical Research Communications, 412, 188–192.
Jung, J. W., Hwang, S. Y., Hwang, J. S., Oh, E. S., Park, S., & Han, I. O. (2007). Ionising radiation induces changes associated with epithelial-mesenchymal transdifferentiation and increased cell motility of A549 lung epithelial cells. European Journal of Cancer, 43, 1214–1224.
Li, T., Zeng, Z. C., Wang, L., Qiu, S. J., Zhou, J. W., Zhi, X. T., et al. (2011). Radiation enhances long-term metastasis potential of residual hepatocellular carcinoma in nude mice through TMPRSS4-induced epithelial-mesenchymal transition. Cancer Gene Therapy, 18, 617–626.
Zhou, B. B., Zhang, H., Damelin, M., Geles, K. G., Grindley, J. C., & Dirks, P. B. (2009). Tumour-initiating cells: challenges and opportunities for anticancer drug discovery. Nature Reviews Drug Discovery, 8, 806–823.
Dick, J. E. (2008). Stem cell concepts renew cancer research. Blood, 112, 4793–4807.
Nagle, R. B., Ahmann, F. R., McDaniel, K. M., Paquin, M. L., Clark, V. A., & Celniker, A. (1987). Cytokeratin characterization of human prostatic carcinoma and its derived cell lines. Cancer research, 47, 281–286.
Gu, G., Yuan, J., Wills, M., & Kasper, S. (2007). Prostate cancer cells with stem cell characteristics reconstitute the original human tumor in vivo. Cancer Research, 67, 4807–4815.
Tu, S. M., & Lin, S. H. (2012). Prostate cancer stem cells. Clinical Genitourinary Cancer, 10, 69–76.
Li, H., Chen, X., Calhoun-Davis, T., Claypool, K., & Tang, D. G. (2008). PC3 human prostate carcinoma cell holoclones contain self-renewing tumor-initiating cells. Cancer Research, 68, 1820–1825.
Li, H., Jiang, M., Honorio, S., Patrawala, L., Jeter, C. R., Calhoun-Davis, T., et al. (2009). Methodologies in assaying prostate cancer stem cells. Methods in Molecular Biology, 568, 85–138.
Lang, S. H., Frame, F. M., & Collins, A. T. (2009). Prostate cancer stem cells. The Journal of Pathology, 217, 299–306.
Collins, A. T., Berry, P. A., Hyde, C., Stower, M. J., & Maitland, N. J. (2005). Prospective identification of tumorigenic prostate cancer stem cells. Cancer Research, 65, 10946–10951.
Patrawala, L., Calhoun, T., Schneider-Broussard, R., Li, H., Bhatia, B., Tang, S., et al. (2006). Highly purified CD44+ prostate cancer cells from xenograft human tumors are enriched in tumorigenic and metastatic progenitor cells. Oncogene, 25, 1696–1708.
Patrawala, L., Calhoun-Davis, T., Schneider-Broussard, R., & Tang, D. G. (2007). Hierarchical organization of prostate cancer cells in xenograft tumors: the CD44 + alpha2beta1+ cell population is enriched in tumor-initiating cells. Cancer Research, 67, 6796–6805.
Rowehl, R. A., Crawford, H., Dufour, A., Ju, J., & Botchkina, G. I. (2008). Genomic analysis of prostate cancer stem cells isolated from a highly metastatic cell line. Cancer Genomics & Proteomics, 5, 301–310.
Klarmann, G. J., Hurt, E. M., Mathews, L. A., Zhang, X., Duhagon, M. A., Mistree, T., et al. (2009). Invasive prostate cancer cells are tumor initiating cells that have a stem cell-like genomic signature. Clinical & Experimental Metastasis, 26, 433–446.
Hurt, E. M., Kawasaki, B. T., Klarmann, G. J., Thomas, S. B., & Farrar, W. L. (2008). CD44+ CD24(−) prostate cells are early cancer progenitor/stem cells that provide a model for patients with poor prognosis. British Journal of Cancer, 98, 756–765.
Bisson, I., & Prowse, D. M. (2009). WNT signaling regulates self-renewal and differentiation of prostate cancer cells with stem cell characteristics. Cell Research, 19, 683–697.
Qin, J., Liu, X., Laffin, B., Chen, X., Choy, G., Jeter, C. R., et al. (2012). The PSA(−/lo) prostate cancer cell population harbors self-renewing long-term tumor-propagating cells that resist castration. Cell Stem Cell, 10, 556–569.
Richardson, G. D., Robson, C. N., Lang, S. H., Neal, D. E., Maitland, N. J., & Collins, A. T. (2004). CD133, a novel marker for human prostatic epithelial stem cells. Journal of Cell Science, 117, 3539–3545.
Vander Griend, D. J., Karthaus, W. L., Dalrymple, S., Meeker, A., DeMarzo, A. M., & Isaacs, J. T. (2008). The role of CD133 in normal human prostate stem cells and malignant cancer-initiating cells. Cancer Research, 68, 9703–9711.
van den Hoogen, C., van der Horst, G., Cheung, H., Buijs, J. T., Lippitt, J. M., Guzman-Ramirez, N., et al. (2010). High aldehyde dehydrogenase activity identifies tumor-initiating and metastasis-initiating cells in human prostate cancer. Cancer Research, 70, 5163–5173.
Doherty, R. E., Haywood-Small, S. L., Sisley, K., & Cross, N. A. (2011). Aldehyde dehydrogenase activity selects for the holoclone phenotype in prostate cancer cells. Biochemical and Biophysical Research Communications, 414, 801–807.
Rajasekhar, V. K., Studer, L., Gerald, W., Socci, N. D., & Scher, H. I. (2011). Tumour-initiating stem-like cells in human prostate cancer exhibit increased NF-kappaB signalling. Nature Communications, 2, 162.
Bae, K. M., Su, Z., Frye, C., McClellan, S., Allan, R. W., Andrejewski, J. T., et al. (2010). Expression of pluripotent stem cell reprogramming factors by prostate tumor initiating cells. The Journal of Urology, 183, 2045–2053.
Liu, T., Xu, F., Du, X., Lai, D., Liu, T., Zhao, Y., et al. (2010). Establishment and characterization of multi-drug resistant, prostate carcinoma-initiating stem-like cells from human prostate cancer cell lines 22RV1. Molecular and Cellular Biochemistry, 340, 265–273.
Liu, F., Wang, J. J., You, Z. Y., Zhang, Y. D., & Zhao, Y. (2010). Radiosensitivity of prostate cancer cells is enhanced by EGFR inhibitor C225. Urologic Oncology, 28, 59–66.
Collins, A. T., & Maitland, N. J. (2006). Prostate cancer stem cells. European Journal of Cancer, 42, 1213–1218.
Maitland, N. J., & Collins, A. T. (2008). Prostate cancer stem cells: a new target for therapy. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology, 26, 2862–2870.
Pfeiffer, M. J., & Schalken, J. A. (2010). Stem cell characteristics in prostate cancer cell lines. European Urology, 57, 246–254.
Yoshida, A., Hsu, L. C., & Dave, V. (1992). Retinal oxidation activity and biological role of human cytosolic aldehyde dehydrogenase. Enzyme, 46, 239–244.
Eastham, A. M., Spencer, H., Soncin, F., Ritson, S., Merry, C. L., Stern, P. L., et al. (2007). Epithelial-mesenchymal transition events during human embryonic stem cell differentiation. Cancer Research, 67, 11254–11262.
Umbas, R., Schalken, J. A., Aalders, T. W., Carter, B. S., Karthaus, H. F., Schaafsma, H. E., et al. (1992). Expression of the cellular adhesion molecule E-cadherin is reduced or absent in high-grade prostate cancer. Cancer Research, 52, 5104–5109.
Ikonen, T., Matikainen, M., Mononen, N., Hyytinen, E. R., Helin, H. J., Tommola, S., et al. (2001). Association of E-cadherin germ-line alterations with prostate cancer. Clinical Cancer Research: an Official Journal of the American Association for Cancer Research, 7, 3465–3471.
Bae, K. M., Parker, N. N., Dai, Y., Vieweg, J., & Siemann, D. W. (2011). E-cadherin plasticity in prostate cancer stem cell invasion. American Journal of Cancer Research, 1, 71–84.
Kong, D., Banerjee, S., Ahmad, A., Li, Y., Wang, Z., Sethi, S., et al. (2010). Epithelial to mesenchymal transition is mechanistically linked with stem cell signatures in prostate cancer cells. PloS ONE, 5, e12445.
Baumann, M., Krause, M., & Hill, R. (2008). Exploring the role of cancer stem cells in radioresistance. Nature Reviews Cancer, 8, 545–554.
Eyler, C. E., & Rich, J. N. (2008). Survival of the fittest: cancer stem cells in therapeutic resistance and angiogenesis. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology, 26, 2839–2845.
Phillips, T. M., McBride, W. H., & Pajonk, F. (2006). The response of CD24(−/low)/CD44+ breast cancer-initiating cells to radiation. Journal of the National Cancer Institute, 98, 1777–1785.
Woodward, W. A., Chen, M. S., Behbod, F., Alfaro, M. P., Buchholz, T. A., & Rosen, J. M. (2007). WNT/beta-catenin mediates radiation resistance of mouse mammary progenitor cells. Proceedings of the National Academy of Sciences of the United States of America, 104, 618–623.
Zhang, M., Behbod, F., Atkinson, R. L., Landis, M. D., Kittrell, F., Edwards, D., et al. (2008). Identification of tumor-initiating cells in a p53-null mouse model of breast cancer. Cancer Research, 68, 4674–4682.
Lagadec, C., Vlashi, E., Della Donna, L., Dekmezian, C., & Pajonk, F. (2012). Radiation-induced reprogramming of breast cancer cells. Stem Cells, 30, 833–844.
Zielske, S. P., Spalding, A. C., & Lawrence, T. S. (2010). Loss of tumor-initiating cell activity in cyclophosphamide-treated breast xenografts. Translational Oncology, 3, 149–152.
Al-Assar, O., Muschel, R. J., Mantoni, T. S., McKenna, W. G., & Brunner, T. B. (2009). Radiation response of cancer stem-like cells from established human cell lines after sorting for surface markers. International Journal of Radiation Oncology, Biology, Physics, 75, 1216–1225.
Dittfeld, C., Dietrich, A., Peickert, S., Hering, S., Baumann, M., Grade, M., et al. (2009). CD133 expression is not selective for tumor-initiating or radioresistant cell populations in the CRC cell lines HCT-116. Radiotherapy and Oncology: Journal of the European Society for Therapeutic Radiology and Oncology, 92, 353–361.
Fiveash, J. B., & Spencer, S. A. (2003). Role of radiation therapy and radiosurgery in glioblastoma multiforme. Cancer Journal, 9, 222–229.
Beier, D., Hau, P., Proescholdt, M., Lohmeier, A., Wischhusen, J., Oefner, P. J., et al. (2007). CD133(+) and CD133(−) glioblastoma-derived cancer stem cells show differential growth characteristics and molecular profiles. Cancer Research, 67, 4010–4015.
Gunther, H. S., Schmidt, N. O., Phillips, H. S., Kemming, D., Kharbanda, S., Soriano, R., et al. (2008). Glioblastoma-derived stem cell-enriched cultures form distinct subgroups according to molecular and phenotypic criteria. Oncogene, 27, 2897–2909.
Liu, Q., Nguyen, D. H., Dong, Q., Shitaku, P., Chung, K., Liu, O. Y., et al. (2009). Molecular properties of CD133+ glioblastoma stem cells derived from treatment-refractory recurrent brain tumors. Journal of Neuro-Oncology, 94, 1–19.
Annabi, B., Lachambre, M. P., Plouffe, K., Sartelet, H., & Beliveau, R. (2009). Modulation of invasive properties of CD133+ glioblastoma stem cells: a role for MT1-MMP in bioactive lysophospholipid signaling. Molecular Carcinogenesis, 48, 910–919.
Bao, S., Wu, Q., McLendon, R. E., Hao, Y., Shi, Q., Hjelmeland, A. B., et al. (2006). Glioma stem cells promote radioresistance by preferential activation of the DNA damage response. Nature, 444, 756–760.
Hambardzumyan, D., Becher, O. J., Rosenblum, M. K., Pandolfi, P. P., Manova-Todorova, K., & Holland, E. C. (2008). PI3K pathway regulates survival of cancer stem cells residing in the perivascular niche following radiation in medulloblastoma in vivo. Genes & Development, 22, 436–448.
Chiou, S. H., Kao, C. L., Chen, Y. W., Chien, C. S., Hung, S. C., Lo, J. F., et al. (2008). Identification of CD133-positive radioresistant cells in atypical teratoid/rhabdoid tumor. PloS ONE, 3, e2090.
Tamura, K., Aoyagi, M., Wakimoto, H., Ando, N., Nariai, T., Yamamoto, M., et al. (2010). Accumulation of CD133-positive glioma cells after high-dose irradiation by Gamma Knife surgery plus external beam radiation. Journal of Neurosurgery, 113, 310–318.
Piao, L. S., Hur, W., Kim, T. K., Hong, S. W., Kim, S. W., Choi, J. E., et al. (2012). CD133+ liver cancer stem cells modulate radioresistance in human hepatocellular carcinoma. Cancer Letters, 315, 129–137.
Wei, C., Guomin, W., Yujun, L., & Ruizhe, Q. (2007). Cancer stem-like cells in human prostate carcinoma cells DU145: the seeds of the cell line? Cancer Biology & Therapy, 6, 763–768.
Tang, D. G., Patrawala, L., Calhoun, T., Bhatia, B., Choy, G., Schneider-Broussard, R., et al. (2007). Prostate cancer stem/progenitor cells: identification, characterization, and implications. Molecular Carcinogenesis, 46, 1–14.
Gurtner, K., Hessel, F., Eicheler, W., Dorfler, A., Zips, D., Heider, K. H., et al. (2012). Combined treatment of the immunoconjugate bivatuzumab mertansine and fractionated irradiation improves local tumour control in vivo. Radiotherapy and Oncology: Journal of the European Society for Therapeutic Radiology and Oncology, 102, 444–449.
Zelefsky, M. J., Yamada, Y., Fuks, Z., Zhang, Z., Hunt, M., Cahlon, O., et al. (2008). Long-term results of conformal radiotherapy for prostate cancer: impact of dose escalation on biochemical tumor control and distant metastases-free survival outcomes. International Journal of Radiation Oncology, Biology, Physics, 71, 1028–1033.
Probert, J. C., & Parker, B. R. (1975). The effects of radiation therapy on bone growth. Radiology, 114, 155–162.
Zietman, A. L., DeSilvio, M. L., Slater, J. D., Rossi, C. J., Jr., Miller, D. W., Adams, J. A., et al. (2005). Comparison of conventional-dose vs high-dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate: a randomized controlled trial. JAMA: The Journal of the American Medical Association, 294, 1233–1239.
Zietman, A. L., Shipley, W. U., & Willett, C. G. (1993). Residual disease after radical surgery or radiation therapy for prostate cancer. Clinical significance and therapeutic implications. Cancer, 71, 959–969.
Inayat, M. S., Chendil, D., Mohiuddin, M., Elford, H. L., Gallicchio, V. S., & Ahmed, M. M. (2002). Didox (a novel ribonucleotide reductase inhibitor) overcomes Bcl-2 mediated radiation resistance in prostate cancer cell line PC-3. Cancer Biology & Therapy, 1, 539–545.
Pajonk, F., van Ophoven, A., Weissenberger, C., & McBride, W. H. (2005). The proteasome inhibitor MG-132 sensitizes PC-3 prostate cancer cells to ionizing radiation by a DNA-PK-independent mechanism. BMC Cancer, 5, 76.
Husbeck, B., Peehl, D. M., & Knox, S. J. (2005). Redox modulation of human prostate carcinoma cells by selenite increases radiation-induced cell killing. Free Radical Biology & Medicine, 38, 50–57.
An, J., Chervin, A. S., Nie, A., Ducoff, H. S., & Huang, Z. (2007). Overcoming the radioresistance of prostate cancer cells with a novel Bcl-2 inhibitor. Oncogene, 26, 652–661.
Supiot, S., Hill, R. P., & Bristow, R. G. (2008). Nutlin-3 radiosensitizes hypoxic prostate cancer cells independent of p53. Molecular Cancer Therapeutics, 7, 993–999.
Handrick, R., Ganswindt, U., Faltin, H., Goecke, B., Daniel, P. T., Budach, W., et al. (2009). Combined action of celecoxib and ionizing radiation in prostate cancer cells is independent of pro-apoptotic Bax. Radiotherapy and Oncology: Journal of the European Society for Therapeutic Radiology and Oncology, 90, 413–421.
Tian, J., Ning, S., & Knox, S. J. (2010). Sodium selenite radiosensitizes hormone-refractory prostate cancer xenograft tumors but not intestinal crypt cells in vivo. International Journal of Radiation Oncology, Biology, Physics, 78, 230–236.
Barreto-Andrade, J. C., Efimova, E. V., Mauceri, H. J., Beckett, M. A., Sutton, H. G., Darga, T. E., et al. (2011). Response of human prostate cancer cells and tumors to combining PARP inhibition with ionizing radiation. Molecular Cancer Therapeutics, 10, 1185–1193.
Gao, Y., Ishiyama, H., Sun, M., Brinkman, K. L., Wang, X., Zhu, J., et al. (2011). The alkylphospholipid, perifosine, radiosensitizes prostate cancer cells both in vitro and in vivo. Radiation Oncology (London, England), 6, 39.
Bridges, K. A., Hirai, H., Buser, C. A., Brooks, C., Liu, H., Buchholz, T. A., et al. (2011). MK-1775, a novel Wee1 kinase inhibitor, radiosensitizes p53-defective human tumor cells. Clinical Cancer Research: An Official Journal of the American Association for Cancer Research, 17, 5638–5648.
Rochester, M. A., Riedemann, J., Hellawell, G. O., Brewster, S. F., & Macaulay, V. M. (2005). Silencing of the IGF1R gene enhances sensitivity to DNA-damaging agents in both PTEN wild-type and mutant human prostate cancer. Cancer Gene Therapy, 12, 90–100.
Huamani, J., Willey, C., Thotala, D., Niermann, K. J., Reyzer, M., Leavitt, L., et al. (2008). Differential efficacy of combined therapy with radiation and AEE788 in high and low EGFR-expressing androgen-independent prostate tumor models. International Journal of Radiation Oncology, Biology, Physics, 71, 237–246.
Wagener, M., Zhang, X., Villarreal, H. G., Levy, L., Allen, P., Shentu, S., et al. (2008). Effect of combining anti-epidermal growth factor receptor antibody C225 and radiation on DU145 prostate cancer. Oncology Reports, 19, 1071–1077.
Matsubara, A., Teishima, J., Mirkhat, S., Yasumoto, H., Mochizuki, H., Seki, M., et al. (2008). Restoration of FGF receptor type 2 enhances radiosensitivity of hormone-refractory human prostate carcinoma PC-3 cells. Anticancer Research, 28, 2141–2146.
Timke, C., Zieher, H., Roth, A., Hauser, K., Lipson, K. E., Weber, K. J., et al. (2008). Combination of vascular endothelial growth factor receptor/platelet-derived growth factor receptor inhibition markedly improves radiation tumor therapy. Clinical Cancer Research: An Official Journal of the American Association for Cancer Research, 14, 2210–2219.
Xu, Y., Fang, F., Sun, Y., St Clair, D. K., & St Clair, W. H. (2010). RelB-dependent differential radiosensitization effect of STI571 on prostate cancer cells. Molecular Cancer Therapeutics, 9, 803–812.
Isebaert, S. F., Swinnen, J. V., McBride, W. H., & Haustermans, K. M. (2011). Insulin-like growth factor-type 1 receptor inhibitor NVP-AEW541 enhances radiosensitivity of PTEN wild-type but not PTEN-deficient human prostate cancer cells. International Journal Of Radiation Oncology, Biology, Physics, 81, 239–247.
Brooks, C., Sheu, T., Bridges, K., Mason, K., Kuban, D., Mathew, P., et al. (2012). Preclinical evaluation of sunitinib, a multi-tyrosine kinase inhibitor, as a radiosensitizer for human prostate cancer. Radiation Oncology, 7, 154.
Colletier, P. J., Ashoori, F., Cowen, D., Meyn, R. E., Tofilon, P., Meistrich, M. E., et al. (2000). Adenoviral-mediated p53 transgene expression sensitizes both wild-type and null p53 prostate cancer cells in vitro to radiation. International Journal of Radiation Oncology, Biology, Physics, 48, 1507–1512.
Sasaki, R., Shirakawa, T., Zhang, Z. J., Tamekane, A., Matsumoto, A., Sugimura, K., et al. (2001). Additional gene therapy with Ad5CMV-p53 enhanced the efficacy of radiotherapy in human prostate cancer cells. International Journal of Radiation Oncology, Biology, Physics, 51, 1336–1345.
Kaliberov, S. A., Kaliberova, L. N., & Buchsbaum, D. J. (2005). Combined ionizing radiation and sKDR gene delivery for treatment of prostate carcinomas. Gene Therapy, 12, 407–417.
Mu, Z., Hachem, P., Agrawal, S., & Pollack, A. (2004). Antisense MDM2 sensitizes prostate cancer cells to androgen deprivation, radiation, and the combination. International Journal of Radiation Oncology, Biology, Physics, 58, 336–343.
Truman, J. P., Gueven, N., Lavin, M., Leibel, S., Kolesnick, R., Fuks, Z., et al. (2005). Down-regulation of ATM protein sensitizes human prostate cancer cells to radiation-induced apoptosis. The Journal of Biological Chemistry, 280, 23262–23272.
Teimourian, S., Jalal, R., Sohrabpour, M., & Goliaei, B. (2006). Down-regulation of Hsp27 radiosensitizes human prostate cancer cells. International Journal of Urology: Official Journal of the Japanese Urological Association, 13, 1221–1225.
Anai, S., Goodison, S., Shiverick, K., Hirao, Y., Brown, B. D., & Rosser, C. J. (2007). Knock-down of Bcl-2 by antisense oligodeoxynucleotides induces radiosensitization and inhibition of angiogenesis in human PC-3 prostate tumor xenografts. Molecular Cancer Therapeutics, 6, 101–111.
Stoyanova, R., Hachem, P., Hensley, H., Khor, L. Y., Mu, Z., Hammond, M. E., et al. (2007). Antisense-MDM2 sensitizes LNCaP prostate cancer cells to androgen deprivation, radiation, and the combination in vivo. International Journal of Radiation Oncology, Biology, Physics, 68, 1151–1160.
Udayakumar, T. S., Hachem, P., Ahmed, M. M., Agrawal, S., & Pollack, A. (2008). Antisense MDM2 enhances E2F1-induced apoptosis and the combination sensitizes androgen-sensitive [corrected] and androgen-insensitive [corrected] prostate cancer cells to radiation. Molecular Cancer Research: MCR, 6, 1742–1754.
Udayakumar, T. S., Stoyanova, R., Hachem, P., Ahmed, M. M., & Pollack, A. (2011). Adenovirus E2F1 overexpression sensitizes LNCaP and PC3 prostate tumor cells to radiation in vivo. International Journal of Radiation Oncology, Biology, Physics, 79, 549–558.
Chinnaiyan, P., Vallabhaneni, G., Armstrong, E., Huang, S. M., & Harari, P. M. (2005). Modulation of radiation response by histone deacetylase inhibition. International Journal of Radiation Oncology, Biology, Physics, 62, 223–229.
Konsoula, Z., Cao, H., Velena, A., & Jung, M. (2011). Adamantanyl-histone deacetylase inhibitor H6CAHA exhibits favorable pharmacokinetics and augments prostate cancer radiation sensitivity. International Journal of Radiation Oncology, Biology, Physics, 79, 1541–1548.
Chen, X., Wong, J. Y., Wong, P., & Radany, E. H. (2011). Low-dose valproic acid enhances radiosensitivity of prostate cancer through acetylated p53-dependent modulation of mitochondrial membrane potential and apoptosis. Molecular Cancer Research: MCR, 9, 448–461.
Xu, L., Yang, D., Wang, S., Tang, W., Liu, M., Davis, M., et al. (2005). (-)-Gossypol enhances response to radiation therapy and results in tumor regression of human prostate cancer. Molecular Cancer Therapeutics, 4, 197–205.
Romero, J., Zapata, I., Cordoba, S., Jimeno, J. M., Lopez-Martin, J. A., Tercero, J. C., et al. (2008). In vitro radiosensitisation by trabectedin in human cancer cell lines. European Journal of Cancer, 44, 1726–1733.
Kozakai, N., Kikuchi, E., Hasegawa, M., Suzuki, E., Ide, H., Miyajima, A., et al. (2012). Enhancement of radiosensitivity by a unique novel NF-kappaB inhibitor, DHMEQ, in prostate cancer. British Journal of Cancer, 107, 652–657.
Chiu, H. W., Fang, W. H., Chen, Y. L., Wu, M. D., Yuan, G. F., Ho, S. Y., et al. (2012). Monascuspiloin enhances the radiation sensitivity of human prostate cancer cells by stimulating endoplasmic reticulum stress and inducing autophagy. PloS ONE, 7, e40462.
Woynarowska, B. A., Roberts, K., Woynarowski, J. M., MacDonald, J. R., & Herman, T. S. (2000). Targeting apoptosis by hydroxymethylacylfulvene in combination with gamma radiation in prostate tumor cells. Radiation Research, 154, 429–438.
Hillman, G. G., Forman, J. D., Kucuk, O., Yudelev, M., Maughan, R. L., Rubio, J., et al. (2001). Genistein potentiates the radiation effect on prostate carcinoma cells. Clinical Cancer Research: An Official Journal of the American Association for Cancer Research, 7, 382–390.
Hillman, G. G., Wang, Y., Kucuk, O., Che, M., Doerge, D. R., Yudelev, M., et al. (2004). Genistein potentiates inhibition of tumor growth by radiation in a prostate cancer orthotopic model. Molecular Cancer Therapeutics, 3, 1271–1279.
Algur, E., Macklis, R. M., & Hafeli, U. O. (2005). Synergistic cytotoxic effects of zoledronic acid and radiation in human prostate cancer and myeloma cell lines. International Journal of Radiation Oncology, Biology, Physics, 61, 535–542.
Raffoul, J. J., Wang, Y., Kucuk, O., Forman, J. D., Sarkar, F. H., & Hillman, G. G. (2006). Genistein inhibits radiation-induced activation of NF-kappaB in prostate cancer cells promoting apoptosis and G2/M cell cycle arrest. BMC Cancer, 6, 107.
Warren, G., Grimes, K., Xu, Y., Kudrimoti, M., & St Clair, W. (2006). Selectively enhanced radiation sensitivity in prostate cancer cells associated with proteasome inhibition. Oncology Reports, 15, 1287–1291.
Suzuki, M., Amano, M., Choi, J., Park, H. J., Williams, B. W., Ono, K., et al. (2006). Synergistic effects of radiation and beta-lapachone in DU-145 human prostate cancer cells in vitro. Radiation Research, 165, 525–531.
Raffoul, J. J., Banerjee, S., Che, M., Knoll, Z. E., Doerge, D. R., Abrams, J., et al. (2007). Soy isoflavones enhance radiotherapy in a metastatic prostate cancer model. International Journal of Cancer. Journal International Du Cancer, 120, 2491–2498.
Stewart, G. D., Nanda, J., Katz, E., Bowman, K. J., Christie, J. G., Brown, D. J., et al. (2011). DNA strand breaks and hypoxia response inhibition mediate the radiosensitisation effect of nitric oxide donors on prostate cancer under varying oxygen conditions. Biochemical Pharmacology, 81, 203–210.
Hussain, T., Gupta, S., & Mukhtar, H. (2003). Cyclooxygenase-2 and prostate carcinogenesis. Cancer Letters, 191, 125–135.
Steinauer, K. K., Gibbs, I., Ning, S., French, J. N., Armstrong, J., & Knox, S. J. (2000). Radiation induces upregulation of cyclooxygenase-2 (COX-2) protein in PC-3 cells. International Journal of Radiation Oncology, Biology, Physics, 48, 325–328.
Ganswindt, U., Budach, W., Jendrossek, V., Becker, G., Bamberg, M., & Belka, C. (2006). Combination of celecoxib with percutaneous radiotherapy in patients with localised prostate cancer—a phase I study. Radiation Oncology (London, England), 1, 9.
Vassilev, L. T., Vu, B. T., Graves, B., Carvajal, D., Podlaski, F., Filipovic, Z., et al. (2004). In vivo activation of the p53 pathway by small-molecule antagonists of MDM2. Science, 303, 844–848.
Cao, W., Yacoub, S., Shiverick, K. T., Namiki, K., Sakai, Y., Porvasnik, S., et al. (2008). Dichloroacetate (DCA) sensitizes both wild-type and over expressing Bcl-2 prostate cancer cells in vitro to radiation. The Prostate, 68, 1223–1231.
Li, B., Shi, X. B., Nori, D., Chao, C. K., Chen, A. M., Valicenti, R., et al. (2011). Down-regulation of microRNA 106b is involved in p21-mediated cell cycle arrest in response to radiation in prostate cancer cells. The Prostate, 71, 567–574.
Traxler, P., Allegrini, P. R., Brandt, R., Brueggen, J., Cozens, R., Fabbro, D., et al. (2004). AEE788: a dual family epidermal growth factor receptor/ErbB2 and vascular endothelial growth factor receptor tyrosine kinase inhibitor with antitumor and antiangiogenic activity. Cancer Research, 64, 4931–4941.
Motzer, R. J., Hoosen, S., Bello, C. L., & Christensen, J. G. (2006). Sunitinib malate for the treatment of solid tumours: a review of current clinical data. Expert Opinion on Investigational Drugs, 15, 553–561.
Kastan, M. B., Canman, C. E., & Leonard, C. J. (1995). P53, cell cycle control and apoptosis: implications for cancer. Cancer Metastasis Reviews, 14, 3–15.
Prince, H. M., Bishton, M. J., & Johnstone, R. W. (2009). Panobinostat (LBH589): a potent pan-deacetylase inhibitor with promising activity against hematologic and solid tumors. Future Oncology, 5, 601–612.
Kitada, S., Leone, M., Sareth, S., Zhai, D., Reed, J. C., & Pellecchia, M. (2003). Discovery, characterization, and structure-activity relationships studies of proapoptotic polyphenols targeting B-cell lymphocyte/leukemia-2 proteins. Journal of Medicinal Chemistry, 46, 4259–4264.
Zhang, M., Liu, H., Guo, R., Ling, Y., Wu, X., Li, B., et al. (2003). Molecular mechanism of gossypol-induced cell growth inhibition and cell death of HT-29 human colon carcinoma cells. Biochemical Pharmacology, 66, 93–103.
Zhang, S., Ong, C. N., & Shen, H. M. (2004). Critical roles of intracellular thiols and calcium in parthenolide-induced apoptosis in human colorectal cancer cells. Cancer Letters, 208, 143–153.
Kim, J. H., Liu, L., Lee, S. O., Kim, Y. T., You, K. R., & Kim, D. G. (2005). Susceptibility of cholangiocarcinoma cells to parthenolide-induced apoptosis. Cancer Research, 65, 6312–6320.
Matsumoto, N., Ariga, A., To-e, S., Nakamura, H., Agata, N., Hirano, S., et al. (2000). Synthesis of NF-kappaB activation inhibitors derived from epoxyquinomicin C. Bioorganic & Medicinal Chemistry Letters, 10, 865–869.
Knight, D. C., & Eden, J. A. (1996). A review of the clinical effects of phytoestrogens. Obstetrics and Gynecology, 87, 897–904.
Wang, Y., Raffoul, J. J., Che, M., Doerge, D. R., Joiner, M. C., Kucuk, O., et al. (2006). Prostate cancer treatment is enhanced by genistein in vitro and in vivo in a syngeneic orthotopic tumor model. Radiation Research, 166, 73–80.
Raffoul, J. J., Banerjee, S., Singh-Gupta, V., Knoll, Z. E., Fite, A., Zhang, H., et al. (2007). Down-regulation of apurinic/apyrimidinic endonuclease 1/redox factor-1 expression by soy isoflavones enhances prostate cancer radiotherapy in vitro and in vivo. Cancer Research, 67, 2141–2149.
Bibault, J. E., Fumagalli, I., Ferte, C., Chargari, C., Soria, J. C., & Deutsch, E. (2013). Personalized radiation therapy and biomarker-driven treatment strategies: a systematic review. Cancer Metastasis Reviews, 32, 479–92.
Vlashi, E., Kim, K., Lagadec, C., Donna, L. D., McDonald, J. T., Eghbali, M., et al. (2009). In vivo imaging, tracking, and targeting of cancer stem cells. Journal of the National Cancer Institute, 101, 350–359.
Diehn, M., & Clarke, M. F. (2006). Cancer stem cells and radiotherapy: new insights into tumor radioresistance. Journal of the National Cancer Institute, 98, 1755–1757.
Acknowledgments
Our prostate cancer radiation research project was supported in part by a NH&MRC Career Development Fellowship; Cancer Research Trust Fund at Cancer Care Centre, St George Hospital; and Prostate and Breast Cancer Foundation. The authors thank the technical support from Mr Ken Hopper, Mr Ese Enari, Mr Alex Wallace, and Mr Peter Treacy from the Cancer Care Centre, Sydney, Australia.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chang, L., Graham, P.H., Hao, J. et al. Emerging roles of radioresistance in prostate cancer metastasis and radiation therapy. Cancer Metastasis Rev 33, 469–496 (2014). https://doi.org/10.1007/s10555-014-9493-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10555-014-9493-5