
Abstract
Purpose
The reasons behind socio-economic disparities in prostate cancer incidence remain unclear. We tested the hypothesis that individual-level factors act jointly with neighborhood-level social and built environment factors to influence prostate cancer risk and that specific social and built environment factors contribute to socio-econmic differences in risk.
Methods
We used multi-level data, combining individual-level data (including education and known prostate cancer risk factors) for prostate cancer cases (n = 775) and controls (n = 542) from the San Francisco Bay Area Prostate Cancer Study, a population-based case–control study, with contextual-level data on neighborhood socio-economic status (nSES) and specific social and built environment factors from the California Neighborhoods Data System. Multivariable logistic regression models were used to compute adjusted odds ratios separately for localized and advanced stage prostate cancer while controlling for neighborhood clustering.
Results
We found a more than twofold increased risk of both localized and advanced prostate cancer with increasing levels of nSES, and decreased risk of advanced prostate cancer with increasing levels of education. For localized disease, the nSES association was largely explained by known prostate cancer risk factors and specific neighborhood environment factors; population density, crowding, and residential mobility. For advanced disease, associations with education and nSES were not fully explained by any available individual- or neighborhood-level factors.
Conclusions
These results demonstrate the importance of specific neighborhood social and built environment factors in understanding risk of localized prostate cancer. Further research is needed to understand the factors underpinning the associations between individual- and neighborhood-level SES and risk of advanced prostate cancer.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Prostate cancer is the most common cancer in the United States (US); it is expected that over 164,000 men will be diagnosed with prostate cancer in 2018 [1]. Disparities in prostate cancer risk are multi-level and complex. There is a large disparity in incidence of prostate cancer between non-Hispanic White (NHW) and African-American (AA) men: from 2009 to 2013, the incidence rate (per 100,000) for prostate cancer was 204 for AA men and 125 for NHW men in the US [2]. In addition, AA men have greater odds of being diagnosed with advanced stages of prostate cancer, compared to NHW men [3, 4]. Disparities according to both individual- and contextual-level socio-economic status (SES) have also been reported [5,6,7,8,9]. Higher neighborhood SES (nSES) has been associated with higher prostate cancer risk [7,8,9,10], independent of disease aggressiveness [7]. The direction of this association contrasts with that of many other cancer sites in which lower nSES is frequently associated with higher cancer incidence [11]. In some instances, the association between higher nSES and higher prostate cancer incidence is observed exclusively among NHW men [12, 13] and has been attributed to greater prostate cancer screening among men residing in higher SES neighborhoods [6, 14]. However, several large population-based studies have observed nSES gradients for both NHW and AA populations [9, 10, 15]. Measures of individual-level SES (i.e., education) have also been associated with prostate cancer risk, but studies differ as to the direction of this association and, when an association between higher individual-level education and greater risk is observed, whether it is mediated by prostate cancer screening [5, 6, 16]. Few studies have examined the independent and/or joint associations between individual-level SES and nSES and prostate cancer risk [8]. The VITamins And Lifestyle (VITAL) cohort reported that the association between higher area-level SES and increased prostate cancer risk were attenuated, but not eliminated when individual-level education was taken into account [8].
Neighborhood SES captures features of the neighborhood environment over-and-above individual-level characteristics of neighborhood residents [17,18,19]. Differences in health outcomes related to nSES may be influenced by aspects of both the built and social environment. Associations between specific neighborhood factors and cancer risk have been examined for aspects of the neighborhood built environment (e.g., outdoor light at night) and social environment (e.g., crime, racial segregation, ethnic enclave) for individuals of specific racial/ethnic groups and select cancer sites [20], but not for prostate cancer. Ultimately, prostate cancer risk is likely due to complex relationships between multi-level factors, including, but not limited to, race/ethnicity and individual-level SES, in addition to other factors previously associated with prostate cancer risk (e.g., prostate cancer screening and health behaviors) [5, 21], such that new breakthroughs in our understanding of differences in risk according to SES will require a multi-level approach.
We hypothesized that further examination of individual- and neighborhood-level SES and specific neighborhood social and built environment factors may help identify contextual factors that contribute most to SES risk differences. Thus, we created a multi-level dataset, combining individual-level data (including education and other putative risk factors) from the San Francisco Bay Area Prostate Cancer Study, a population-based case–control study of prostate cancer, and contextual-level data on nSES and specific social and built environment factors from the California Neighborhoods Data System [22]. Our objectives were to examine (1) independent and joint contributions of individual- and neighborhood-level SES to risk of localized and advanced prostate cancer, and (2) the extent to which specific neighborhood factors contribute to SES differences in analyses stratified by race/ethnicity and prostate cancer stage at diagnosis.
Methods
Study population and data collection
The San Francisco Bay Area Prostate Cancer Study, approved by the investigators’ Institutional Review Board, is a population-based case–control study of AA (non-Hispanic) and NHW men [23, 24]. Newly diagnosed cases were identified through the population-based Greater Bay Area Cancer Registry, which participates in the National Cancer Institute’s (NCI’s) Surveillance, Epidemiology, and End Results (SEER) Program and the California Cancer Registry (CCR). Eligible cases and controls were contacted for interview. Resulting interview data were merged with CCR data and neighborhood data from the California Neighborhoods Data Systems (CNDS) [22].
Eligible cases included AA and NHW men aged 40–79 years with a first primary localized prostate cancer diagnosed between 1 October 1997 and 30 September 1998; NHW men with a first primary advanced prostate cancer diagnosed between 1 July 1997 and 29 February 2000; and AA men with a first primary advanced prostate cancer diagnosed between 1 July 1997 and 31 December 2000. Advanced prostate cancer was defined as a tumor invading and extending beyond the prostatic capsule and/or extending into adjacent tissue or involving regional lymph nodes or distant metastatic sites [23]. The study included random samples of localized cases (60% of AAs, 15% of NHWs) and all advanced cases to allow for adequate sample sizes for AAs and advanced cases. Controls aged 40–79 years were identified through random-digit dialing and those aged 65–79 years also through random selections from the beneficiary rosters of the Health Care Financing Administration (HCFA).
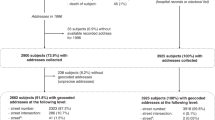
In-person interviews were conducted in English by trained interviewers at the participants’ home using a structured questionnaire that asked about socio-demographic background, medical history, family history of cancer (first degree relative), and lifestyle factors. Medical care was defined with information from medical history on regular source of care (MD/RN/ER/Public clinic) and whether the participant had insurance. Dietary intake during the previous calendar year was assessed using the Block Food Frequency Questionnaire. Data on age and stage (localized, advanced) at diagnosis were obtained from the CCR. Of 319 localized cases, 274 were alive and met the eligbibility criteria described above, and 208 (73 AAs and 135 NHWs) completed the interview. Of 1,015 advanced cases, 788 were alive and met the eligibility criteria described above, and 568 (118 AAs and 450 NHWs) completed the interview [23, 24]. Of 868 eligible controls frequency matched on race/ethnicity and 5-year age group who were contacted, 545 (90 AAs and 455 NHWs) completed the interview.
Cases and controls with a residential address (at diagnosis for cases and at the time of selection for controls) were geocoded to latitude/longitude coordinates and then assigned to a 2000 census block group. Addresses were standardized to conform to U.S. Postal Service specifications using ZP4 software [25]. Batch geocoding was performed using the Texas A&M Geocoder [26], resulting in the geocoding of 1,286 addresses to a building centroid and 3 to street address range interpolation. The remaining 32 addresses were manually geocoded using ArcGIS [27], of which 26 were geocoded to a parcel centroid and 2 to street address range interpolation. We were not able to geocode 4 addresses (3 controls and 1 advanced case). The final geocoded study population thus comprised 542 controls and 775 cases (208 localized and 567 advanced). Of the 650 unique block groups represented by cases, 58% were represented by a single case: of the 490 unique block groups represented by controls, 71% were represented by a single control. Geocodes for the study population were linked with neighborhood data obtained from the CNDS [28].
Socio-economic status
Self-reported education, a measure of individual-level SES, was categorized as having a high school diploma (or equivalent) or below, vocational/technical degree or some college, and college degree or higher. Neighborhood SES was measured at the census block-group level and was based on a previously described index, created through principle components analysis, that incorporates 2000 census data on education, occupation, unemployment, household income, house values, rent values, and poverty [29]. The nSES index was scaled according to statewide quintiles. A joint variable of education and nSES was created, where low education was defined as high school diploma or below and low nSES included quintiles 1–3.
Specific social and built environment factors
Data on several specific neighborhood social and built environment factors, measured at the block group or tract level or for a residential buffer, were obtained from the CNDS for the census year 2000 (Table 1). Measures of neighborhood housing, commuting, residential mobility, and population density were at the block-group level [30, 31]. Street connectivity or street network-based measures of walkability (Table 2, footnote) were calculated for census tracts using ArcGIS software, including the gamma measure (ratio of actual number of street segments to the maximum possible given the number of intersections) [30]. At the time of the study, measures of street connectivity at the block-group level were not available. Variables measured according to a residential buffer were defined for each control and case, blinded to case–control status, in order to capture access to amenities within a walking distance of 1600 meters [32] along a network of pedestrian-accessible pathways [33]. Information regarding the total number of businesses, parks, and farmers markets originated from several geocoded data sources for business listings [34], farmers markets [35], and NavStreets [33]. Quintile/quartile cut-points for these measures were based on distributions among the study controls with the exception of nSES and population density which were based on statewide distributions. In addition, two previously developed food environment indices to describe the retail food and restaurant environment were included: the Retail Food Environment Index (RFEI) and the Restaurant Environment Index (REI) are ratios of unhealthy to healthy retail food outlets and restaurants, respectively, within the residential buffer (Table 3, footnotes), such that higher values indicate a less healthy neighborhood retail or restaurant food environment; values are presented with categories of “0” (no unhealthy outlets or restaurants) or tertiles based on the control distribution [31, 36]. The traffic density measure was developed from the database of traffic counts from the California Department of Transportation for each measured road segment within a smaller residential buffer of 500 meters as described previously [36, 37].
Statistical analysis
Multivariable logistic regression models were used to compute adjusted odds ratios (ORs) separately for localized and advanced prostate cancer while controlling for clustering by census block groups. In the base model adjusted for age, race/ethnicity, and clustering by census block groups, individual-level covariates and specific social and built environment factors (Table 1) were examined to assess the extent to which these factors were associated with odds of localized or advanced prostate cancer. Then, a series of nested models was created to assess the effect of multi-level factors on socio-economic disparities in odds of prostate cancer by sequentially including individual-level covariates and specific social and built environment factors that were associated with increased odds of prostate cancer with p < 0.05 in the base model. Pair-wise correlations among specific social and built environment factors added to sequential models were examined and none were correlated with an absolute correlation coefficient greater than or equal to 0.80. We examined the independent effects of education and nSES with odds of prostate cancer, as well as their joint effects using a single combination variable. In order to assess the underlying correlations (multicollinearity) between individual- and neighborhood-level predictors in the multi-variable models, we calculated variance inflation factors and found no violating predictors with significiant multicollinearity requiring model correction. We did not have enough study participants to stratify analyses by race/ethnicity or PSA screening.
Results
Multi-level characteristics for controls and localized and advanced prostate cancer cases are presented in Table 1. The majority of cases in our study were diagnosed with advanced prostate cancer, reflecting the over-sampling of advanced cases. Approximately 47% of controls and advanced cases were college graduates, compared to 41% of localized cases. 84% of controls were NHW, compared to 79.4% of advanced cases and 64.9% of localized cases. Approximately half of controls and localized cases resided in the highest SES (Q5) neighborhoods (49.1% and 49.5%, respectively), while 61.0% of advanced cases resided in the highest SES neighborhoods.
Associations between each multi-level factor and risk of localized and advanced prostate cancer were examined using the base model (adjusted for age, race/ethnicity, and clustering by census block groups) (Table 2). Individual-level factors associated with greater risk of both localized and advanced prostate cancer were family history of prostate cancer (localized: OR 1.85, 95% CI 1.21–2.84; advanced: OR 1.69, 95% CI 1.22–2.35), personal history of benign prostatic hyperplasia (localized: OR 1.75, 95% CI 1.24–2.48; advanced: OR 2.07, 95% CI 1.59–2.70), and prostatitis (localized: OR 2.48, 95% CI 1.65–3.73; advanced: OR 2.70, 95% CI 1.95–3.73). Increasing numbers of PSA tests in the last 5 years exhibited a significant trend with greater risk of localized prostate cancer (p trend, 0.01), while having 1–2 PSA tests in the last 5 years was associated with a lower risk of advanced prostate cancer (1–2 vs. 0: OR 0.63, 95% CI 0.44–0.89). Obesity was associated with a lower risk of localized prostate cancer only (BMI ≥ 30 vs. < 25: OR 0.56; 95% CI 0.35–0.89; p trend = 0.10). Specific social and built environment factors showing statistically significant trends of lower risk of both localized and advanced prostate cancer were greater population density (p trends < 0.01), more household crowding (p trends < 0.01), and more businesses (p trend < 0.01 for localized and p trend = 0.02 for advanced). Street connectivity (p trend = 0.02), a less favorable REI (T3 vs. 0: OR 0.55, 95% CI 0.33–0.91), a greater number of parks (p trend = 0.02), and greater traffic density (p trend < 0.01) were associated only with a lower risk of localized prostate cancer, while greater residential mobility was associated only with a lower risk of advanced prostate cancer (p trend < 0.01).
We examined independent and joint associations of education and nSES with localized prostate cancer in the base model (Table 3): education was not associated with risk of localized prostate cancer, whereas a two-fold increase in risk was associated with higher nSES (p trend < 0.01). The positive association with nSES was attenuated, but remained statistically significant after adjustment for medical history and BMI (Model 2, highest vs. lowest: OR 2.15, 95% CI 1.11–4.18). The further addition of census-derived environmental factors (i.e., population density, crowding, and residential mobility) eliminated the association of higher nSES with localized prostate cancer risk (Model 3a, highest vs. lowest: OR 1.59, 95% CI 0.71–3.59). On the other hand, addition of walkability and buffer-derived environmental factors (i.e., total businesses, traffic density, REI, parks) did not alter the association of nSES with localized prostate cancer risk (Model 3b). There were no statistically significant associations with the joint education/nSES variable.
For advanced prostate cancer (Table 4), there were independent associations between both education and nSES and risk; higher education was associated with lower risk (college graduate or more vs. high school or less: OR 0.68, 95% CI 0.49–0.95) and higher nSES was associated with higher risk (highest vs. lowest: OR 2.67, 95% CI 1.64–4.35). These associations were not explained by individual or specific neighborhood environment factors, however, adjusting for population density, crowding, and residential mobility somewhat attenuated the association between high nSES and higher risk of advanced disease. Considering the joint effects of education and nSES, associations between high nSES with higher advanced prostate cancer risk were similar for men with a high school education or less and men with college education. However, compared to individuals with a high school education or less and low nSES, those with college education and low nSES had lower risk (OR 0.62, 95% CI 0.41–0.95) even after adjusting for other individual and specific neighborhood environment factors.
Discussion
Our study utilized extensive multi-level data comprising individual-level and contextual-level measures to examine SES disparities in the risk of localized and advanced prostate cancer for a population-based series of NHW and AA prostate cancer cases and controls in the San Francisco Bay Area. We analyzed independent and joint effects of individual- and neighborhood-level SES and the mediating role of specific social and built environment factors. Education was not associated with risk of localized prostate cancer, but greater education was associated with a lower risk of advanced disease. There was a two-fold increased risk of both localized and advanced prostate cancer associated with higher nSES. For localized disease, the association with nSES was largely explained by known prostate cancer risk factors as well as certain specific neighborhood environment factors, specifically population density, crowding, and residential mobility. For advanced disease, independent associations between nSES and education with risk were not fully explained by available multi-level factors, although associations between high nSES and risk of advanced disease were attenuated by the addition of population density, crowding, and residential mobility. Higher education was protective for advanced prostate cancer among men residing in low SES neighborhoods, but not for men residing in high SES neighborhoods.
Few studies have examined multi-level SES and prostate cancer risk [6, 8]. A case–control study utilizing zip code-level SES and education reported a negative association between area-level SES and prostate cancer risk, potentially owing to the zip-code level of analysis [6]. A study of VITAL cohort reported that the positive association between area-level SES (according to a block-group level SES index) and prostate cancer risk was attenuated, but not eliminated when individual-level SES (education and household income) was taken into account [8]. We observed nSES to be positively associated with advanced prostate cancer risk, but independently of education. Also, the VITAL study did not adjust for medical history or behavioral factors nor stratify localized and advanced disease [8]. The latter point may be particularly relevant, since we observed an association between education and risk for advanced, but not localized, disease. Our study thus establishes the independence of nSES amongst a number of individual-level factors and illustrates the importance of considering modification of SES disparities by stage of disease.
Some studies have suggested that increased prostate cancer risk among residents of higher SES neighborhoods is due to greater use of prostate cancer screening [6, 14]. It follows from this hypothesis that higher nSES would be associated with risk of localized prostate cancer, but would not be associated with risk of advanced prostate cancer, or would be associated with lower risk of advanced prostate cancer. Our results, however, indicate that higher nSES is associated with risk of both localized and advanced disease. Furthermore, our analyses included information on PSA testing; while, as expected, having a PSA test in the last 5 years was associated with increased risk of localized disease and decreased risk of advanced disease in base models, adjustment for this factor did not effect the association between higher nSES and greater prostate cancer risk. Adjustment for other available individual characteristics did not alter associations between individual- or neighborhood-level SES and risk, but larger studies by subgroups of prostate cancer screening and race/ethnicity are warranted.
Our study is the first, to our knowledge, to examine a suite of specific social and built environment factors in relation to prostate cancer risk. Associations were more pronounced for localized prostate cancer, as residential mobility was the only specific neighborhood environment factor exclusively associated with advanced disease. Of note, the association between higher nSES and greater risk of localized prostate cancer was largely explained by three specific neighborhood environment factors (i.e., population density, household crowding, and residential mobility), which also attenuated the association between higher nSES and greater risk of advanced disease. In base models, lower population density, less crowding, and less residential mobility were associated with higher risk of prostate cancer. Ours is the first study to examine neighborhood crowding and mobility with prostate cancer risk. The association of lower population density with higher risk of localized and advanced prostate cancer seemingly contrasts the few studies that have examined population density and prostate cancer incidence and reported higher risk of prostate cancer among residents of more populated or more urban areas [38,39,40,41]. These studies suggested that greater access to care, and thus more regular PSA screening, contributed to higher rates of prostate cancer among those living in more populated and more urban areas, but, unlike the current study, these previous studies were ecological and did not have access to multi-level data, including individual-level PSA screening and access to care [38]. Furthermore, the types of neighborhoods associated with increased risk of prostate cancer in our study (higher nSES, less populated, less crowded, and less mobile) may not be completely captured by measures of urbanicity which don’t generally take SES into account. Our results thus suggest a more complicated risk landscape than explained by increased access to care and screening.
Education and nSES were independently associated with risk of advanced prostate cancer, but while higher nSES was associated with increased risk, greater education was associated with lower risk. Results of the joint variable indicate that, while higher education was protective against risk of advanced disease among men residing in lower SES neighborhoods, it had no effect on risk among men residing in higher SES neighborhoods. This suggests complex influences of education and nSES on risk of advanced disease, perhaps related to interactions among risk exposures and prevention behaviors. Thus, additional research is needed to determine the mechanisms underlying the association between joint individual- and neighborhood-level SES and risk of advanced prostate cancer.
Although we assessed several specific neighborhood social and built environment factors in relation to prostate cancer risk, these variables are based on secondary data and thus may not capture how patients use and perceive their environments [20]. There may also be other unmeasured neighborhood environment factors relevant to prostate cancer risk. For example, healthcare factors (e.g., access, insurance, care quality, and continuity) [11] at the individual or neighborhood level may be important to consider. We included a measure of medical care as a proxy for medical home, which, conceptually, involves a personal physician, a whole-person orientation to care, a physician-directed team, coordination of care, and enhanced access to care that is often associated with increased use of preventive and screening services [42,43,44]. However, this measure was not associated with risk of localized or advanced disease. It may be that our proxy measure insufficiently captures an effective medical home [45] or that other aspects of healthcare access, not provided by the medical home concept, may be more influential in regards to prostate cancer diagnosis (e.g., insurance status, payment responsibility, or other issues of access and quality of care) [3, 46]. In addition, there may be factors that mediate effects of SES on risk that are not directly related to healthcare access. Chronic stress that ultimately increases cellular oxidative stress and DNA-damage in the prostate or toxic exposures (e.g., endocrine disrupting chemicals and trace elements) [21] may affect prostate cancer risk. For any of these hypothesized prostate cancer risk factors, the strength and direction of associations with individual- or neighborhood-level SES and ultimately prostate cancer risk need to be explored.
Our study combines interview and secondary data, including specific social and built environment factors, in order to explore potential mediators of SES disparities in prostate cancer risk. However, our study does have some limitations. Education was the only measure of individual-level SES assessed by self-report, and previously published studies of prostate cancer risk also utilized education as a measure of individual SES [5, 6, 8, 16]. However, other measures (i.e., financial stability or occupational class) may capture different aspects of an individuals’ cancer risk and so will be important to consider in future studies. Neighborhood variables derived from census data are subject to administrative boundaries that may not accurately portray the real or perceived neighborhood environments experienced by individuals. However, we utilized the smallest level of geography for which robust data were available, census block group and census tract, which have been shown to perform well to detect SES gradients in health outcomes [47]. For cases and controls, only one address is available to approximate neighborhood exposures for the entire at-risk period. Insurance type (private, public) was not collected by interview [48]. We did not have adequate numbers of subjects to stratify analyses by race/ethnicity or PSA screening. Finally, the relatively high nSES in the San Francisco Bay Area may preclude observation of effects of the lowest levels of nSES on prostate cancer risk.
Conclusions
Our analyses demonstrate the importance of specific neighborhood social and built environment factors in risk of prostate cancer, and suggest further research is needed to determine the mechanisms by which these neighborhood factors influence risk. While only nSES was associated with localized disease, education and nSES were independently associated with risk of advanced disease. Further research is needed to understand the factors underpinning the complex associations between individual- and neighborhood-level SES and risk of advanced prostate cancer.
References
American Cancer Society (2017) Cancer facts and figs (2017). American Cancer Society, Atlanta
Howlader N, Noone AM, Krapcho M, Miller DC, Bishop K, Altekruse S, CL. K, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA SEER cancer statistics review, 1975–2013, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2013/, based on November 2015 SEER data submission, posted to the SEER web site, April 2016
Hoffman RM, Gilliland FD, Eley JW, Harlan LC, Stephenson RA, Stanford JL, Albertson PC, Hamilton AS, Hunt WC, Potosky AL (2001) Racial and ethnic differences in advanced-stage prostate cancer: the Prostate Cancer Outcomes Study. J Natl Cancer Inst 93(5):388–395
Chornokur G, Dalton K, Borysova ME, Kumar NB (2011) Disparities at presentation, diagnosis, treatment, and survival in African American men, affected by prostate cancer. Prostate 71(9):985–997
Pudrovska T, Anishkin A (2015) Clarifying the positive association between education and prostate cancer: a Monte Carlo simulation approach. J Appl Gerontol 34(3):293–316
Sanderson M, Coker AL, Perez A, Du XL, Peltz G, Fadden MK (2006) A multilevel analysis of socioeconomic status and prostate cancer risk. Ann Epidemiol 16(12):901–907. https://doi.org/10.1016/j.annepidem.2006.02.006
Cheng I, Witte JS, McClure LA, Shema SJ, Cockburn MG, John EM, Clarke CA (2009) Socioeconomic status and prostate cancer incidence and mortality rates among the diverse population of California. Cancer Causes Control 20(8):1431–1440. https://doi.org/10.1007/s10552-009-9369-0
Hastert TA, Beresford SA, Sheppard L, White E (2015) Disparities in cancer incidence and mortality by area-level socioeconomic status: a multilevel analysis. J Epidemiol Community Health 69(2):168–176. https://doi.org/10.1136/jech-2014-204417
Yin D, Morris C, Allen M, Cress R, Bates J, Liu L (2010) Does socioeconomic disparity in cancer incidence vary across racial/ethnic groups? Cancer Causes Control 21(10):1721–1730. https://doi.org/10.1007/s10552-010-9601-y
Singh GK, Jemal A (2017) Socioeconomic and racial/ethnic disparities in cancer mortality, incidence, and survival in the United States, 1950–2014: over six decades of changing patterns and widening inequalities. J Environ Public Health. https://doi.org/10.1155/2017/2819372
Ward E, Jemal A, Cokkinides V, Singh GK, Cardinez C, Ghafoor A, Thun M (2004) Cancer disparities by race/ethnicity and socioeconomic status. CA Cancer J Clin 54(2):78–93
Oliver MN, Smith E, Siadaty M, Hauck FR, Pickle LW (2006) Spatial analysis of prostate cancer incidence and race in Virginia, 1990–1999. Am J Prev Med 30(2 Suppl):S67–S76. https://doi.org/10.1016/j.amepre.2005.09.008
Major JM, Norman Oliver M, Doubeni CA, Hollenbeck AR, Graubard BI, Sinha R (2012) Socioeconomic status, healthcare density, and risk of prostate cancer among African American and Caucasian men in a large prospective study. Cancer Causes Control 23(7):1185–1191. https://doi.org/10.1007/s10552-012-9988-8
Liu L, Cozen W, Bernstein L, Ross RK, Deapen D (2001) Changing relationship between socioeconomic status and prostate cancer incidence. J Natl Cancer Inst 93(9):705–709
Clegg LX, Reichman ME, Miller BA, Hankey BF, Singh GK, Lin YD, Goodman MT, Lynch CF, Schwartz SM, Chen VW, Bernstein L, Gomez SL, Graff JJ, Lin CC, Johnson NJ, Edwards BK (2009) Impact of socioeconomic status on cancer incidence and stage at diagnosis: selected findings from the surveillance, epidemiology, and end results: National Longitudinal Mortality Study. Cancer Causes Control 20(4):417–435. https://doi.org/10.1007/s10552-008-9256-0
Steenland K, Rodriguez C, Mondul A, Calle EE, Thun M (2004) Prostate cancer incidence and survival in relation to education (United States). Cancer Causes Control 15(9):939–945. https://doi.org/10.1007/s10552-004-2231-5
Shariff-Marco S, Yang J, John EM, Sangaramoorthy M, Hertz A, Koo J, Nelson DO, Schupp CW, Shema SJ, Cockburn M (2014) Impact of neighborhood and individual socioeconomic status on survival after breast cancer varies by race/ethnicity: the Neighborhood and Breast Cancer Study. Cancer Epidemiol Prev Biomark 23(5):793–811
Macintyre S, Ellaway A, Cummins S (2002) Place effects on health: how can we conceptualise, operationalise and measure them? Soc Sci Med 55(1):125–139
DeRouen MC, Schupp CW, Koo J, Yang J, Hertz A, Shariff-Marco S, Cockburn M, Nelson DO, Ingles SA, John EM (2018) Impact of individual and neighborhood factors on disparities in prostate cancer survival. Cancer Epidemiol 53:1–11
Gomez SL, Shariff-Marco S, DeRouen M, Keegan TH, Yen IH, Mujahid M, Satariano WA, Glaser SL (2015) The impact of neighborhood social and built environment factors across the cancer continuum: current research, methodological considerations, and future directions. Cancer 121(14):2314–2330. https://doi.org/10.1002/cncr.29345
Bostwick DG, Burke HB, Djakiew D, Euling S, Ho S, Landolph J, Morrison H, Sonawane B, Shifflett T, Waters DJ (2004) Human prostate cancer risk factors. Cancer 101(S10):2371–2490
Gomez SL, Glaser SL, McClure LA, Shema SJ, Kealey M, Keegan TH, Satariano WA (2011) The California Neighborhoods Data System: a new resource for examining the impact of neighborhood characteristics on cancer incidence and outcomes in populations. Cancer Causes Control 22(4):631–647
John EM, Schwartz GG, Koo J, Van Den Berg D, Ingles SA (2005) Sun exposure, vitamin D receptor gene polymorphisms, and risk of advanced prostate cancer. Cancer Res 65(12):5470–5479. https://doi.org/10.1158/0008-5472.CAN-04-3134
John EM, Stern MC, Sinha R, Koo J (2011) Meat consumption, cooking practices, meat mutagens, and risk of prostate cancer. Nutr Cancer 63(4):525–537. https://doi.org/10.1080/01635581.2011.539311
Semaphore Corporation (2011) ZP4: Address correction data and software. http://www.semaphorecorp.com/zp4/zp4.html
Goldberg DW (2009) The Texas A&M WebGIS Open Source Geocoding Platform. Technical Report No 11. University of South California GIS Research Laboratory, Los Angeles CA
ArcGIS. Version 10 (2011) Environmental Systems Research Institute, Inc.
Gomez SL, Glaser SL, McClure LA, Shema SJ, Kealey M, Keegan TH, Satariano WA (2011) The California Neighborhoods Data System: a new resource for examining the impact of neighborhood characteristics on cancer incidence and outcomes in populations. Cancer Causes Control 22(4):631–647. https://doi.org/10.1007/s10552-011-9736-5
Yost K, Perkins C, Cohen R, Morris C, Wright W (2001) Socioeconomic status and breast cancer incidence in California for different race/ethnic groups. Cancer Causes Control 12(8):703–711
Keegan TH, Hurley S, Goldberg D, Nelson DO, Reynolds P, Bernstein L, Horn-Ross PL, Gomez SL (2012) The association between neighborhood characteristics and body size and physical activity in the California teachers study cohort. Am J Public Health 102(4):689–697
Keegan TH, Shariff-Marco S, Sangaramoorthy M, Koo J, Hertz A, Schupp CW, Yang J, John EM, Gomez SL (2014) Neighborhood influences on recreational physical activity and survival after breast cancer. Cancer Causes Control 25(10):1295–1308. https://doi.org/10.1007/s10552-014-0431-1
Thornton LE, Pearce JR, Kavanagh AM (2011) Using Geographic Information Systems (GIS) to assess the role of the built environment in influencing obesity: a glossary. Int J Behav Nutr Phys Act 8(1):71
Robbins AS, Yin D, Parikh-Patel A (2007) Differences in prognostic factors and survival among White men and Black men with prostate cancer, California, 1995–2004. Am J Epidemiol 166(1):71–78. https://doi.org/10.1093/aje/kwm052
National Establishment Time-Series (NETS) Database 2009 (2008). Oakland, CA
California Department of Food and Agriculture (2010) California Certified Farmers’ Market Database
Shariff-Marco S, Gomez SL, Sangaramoorthy M, Yang J, Koo J, Hertz A, John EM, Cheng I, Keegan TH (2015) Impact of neighborhoods and body size on survival after breast cancer diagnosis. Health Place 36:162–172. https://doi.org/10.1016/j.healthplace.2015.10.003
Gunier RB, Hertz A, Von Behren J, Reynolds P (2003) Traffic density in California: socioeconomic and ethnic differences among potentially exposed children. J Expo Anal Environ Epidemiol 13(3):240–246. https://doi.org/10.1038/sj.jea.7500276
Baade PD, Yu XQ, Smith DP, Dunn J, Chambers SK (2015) Geographic disparities in prostate cancer outcomes–review of international patterns. Asian Pac J Cancer Prev 16(3):1259–1275
Baquet CR, Horm JW, Gibbs T, Greenwald P (1991) Socioeconomic factors and cancer incidence among blacks and whites. J Natl Cancer Inst 83(8):551–557
Meijer M, Bloomfield K, Engholm G (2013) Neighbourhoods matter too: the association between neighbourhood socioeconomic position, population density and breast, prostate and lung cancer incidence in Denmark between 2004 and 2008. J Epidemiol Community Health 67(1):6–13. https://doi.org/10.1136/jech-2011-200192
Obertova Z, Brown C, Holmes M, Lawrenson R (2012) Prostate cancer incidence and mortality in rural men—a systematic review of the literature. Rural Remote Health 12(2):2039
Blewett LA, Johnson PJ, Lee B, Scal PB (2008) When a usual source of care and usual provider matter: adult prevention and screening services. J Gen Intern Med 23(9):1354
Sarfaty M, Wender R, Smith R (2011) Promoting cancer screening within the patient centered medical home. CA Cancer J Clin 61(6):397–408. https://doi.org/10.3322/caac.20125
Ferrante JM, Balasubramanian BA, Hudson SV, Crabtree BF (2010) Principles of the patient-centered medical home and preventive services delivery. Ann Fam Med 8(2):108–116. https://doi.org/10.1370/afm.1080
Fisher ES (2008) Building a medical neighborhood for the medical home. N Engl J Med 359(12):1202–1205. https://doi.org/10.1056/NEJMp0806233
Zafar SY, Peppercorn JM, Schrag D, Taylor DH, Goetzinger AM, Zhong X, Abernethy AP (2013) The financial toxicity of cancer treatment: a pilot study assessing out-of-pocket expenses and the insured cancer patient’s experience. Oncologist 18(4):381–390
Krieger N, Chen JT, Waterman PD (2010) Decline in US breast cancer rates after the Women’s Health Initiative: socioeconomic and racial/ethnic differentials. Am J Public Health 100(Suppl 1):S132–S139. https://doi.org/10.2105/AJPH.2009.181628
Gomez SL, Hurley S, Canchola AJ, Keegan TH, Cheng I, Murphy JD, Clarke CA, Glaser SL, Martinez ME (2016) Effects of marital status and economic resources on survival after cancer: a population-based study. Cancer 122(10):1618–1625. https://doi.org/10.1002/cncr.29885
Acknowledgments
The authors thank Jennifer Jain for her help with manuscript preparation.
Funding
This work was supported by Grant W81XWH-10-1-0374 (SLG) from the United States Army Medical Research and Material Command. Data collection for the parent study was funded by Grants 864A-8702-S3514 and 99-00527V-10182 (EMJ) from the Cancer Research Fund, under Interagency Agreement #97-12013 (University of California contract #98-0092-V) with the Department of Health Services Cancer Research Program. The collection of cancer incidence data used in this study was supported by the California Department of Public Health as part of the statewide cancer reporting program mandated by California Health and Safety Code Section 103885; the National Cancer Institute’s Surveillance, Epidemiology and End Results Program under contract HHSN261201000140C awarded to the Cancer Prevention Institute of California, contract HHSN261201000035C awarded to the University of Southern California, and contract HHSN261201000034C awarded to the Public Health Institute; and the Centers for Disease Control and Prevention’s National Program of Cancer Registries, under agreement U58DP003862-01 awarded to the California Department of Public Health. The ideas and opinions expressed herein are those of the author(s) and endorsement by the State of California, Department of Public Health the National Cancer Institute, and the Centers for Disease Control and Prevention or their Contractors and Subcontractors is not intended nor should be inferred.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
DeRouen, M.C., Schupp, C.W., Yang, J. et al. Impact of individual and neighborhood factors on socioeconomic disparities in localized and advanced prostate cancer risk. Cancer Causes Control 29, 951–966 (2018). https://doi.org/10.1007/s10552-018-1071-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-018-1071-7