
Abstract
Research over the past 40 years has convincingly shown that lifestyle factors play a huge role in cancer incidence and mortality. The public, though, can often discount the preventability of cancer. That health information on the Internet is a vast and often scientifically suspect commodity makes promoting important and sound cancer prevention messages to the public even more difficult. To help address these issues and improve the public’s knowledge of, and attitudes toward, cancer prevention, there need to be concerted efforts to create evidence-based, user-friendly information about behaviors that could greatly reduce overall cancer risk. Toward this end, we condensed the current scientific evidence on the topic into eight key behaviors. While not an end in themselves, “Eight Ways to Stay Healthy and Prevent Cancer” forms an evidence-based and targeted framework that supports broader cancer prevention efforts.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Research over the past 40 years has convincingly shown that lifestyle factors play a large role in cancer incidence and mortality. Doll and Peto’s groundbreaking analyses in the 1980s and the cascade of research they inspired estimate that over half of all cancers—and up to three quarters of some specific cancers—could be avoided by a combination of healthy lifestyle and regular screening (Table 1) [1–12].
Despite this large weight of evidence and the important role it plays in public health activities and policies, it also seems to be one that is evading much of the public [13, 14]. Cancer remains one of the public’s primary health fears, yet a quarter to nearly half the public discounts the preventability of cancer [13, 15].
To help address this and improve the public’s knowledge of, and attitudes toward, cancer prevention, there need to be concerted efforts to create evidence-based, user-friendly information for the public about behaviors that could greatly reduce overall cancer risk. Toward this end, we developed eight key messages, collected under the name “Eight Ways to Stay Healthy and Prevent Cancer” and linked it with our validated risk assessment website, “Your Disease Risk” (http://www.yourdiseaserisk.wustl.edu) [16].
While the full “Eight Ways” document includes supporting text and tips for individuals as well as parents and grandparents, one-line summaries of the messages are as follows:
-
1.
Don’t smoke
-
2.
Maintain a healthy weight
-
3.
Exercise regularly
-
4.
Eat a healthy diet
-
5.
Drink alcohol only in moderation, if at all
-
6.
Protect yourself from the sun
-
7.
Protect yourself from infections
-
8.
Get screening tests regularly
(Full print version online: http://tinyurl.com/8waysPDF)
There are additional steps beyond these eight that could reduce the risk of some individual cancers, yet these eight provide the greatest benefit for the most cancers and can also substantially reduce the risk of other serious chronic diseases (e.g., cardiovascular disease, type 2 diabetes, osteoporosis, and chronic obstructive pulmonary disease) adding even more force to their messages.
Below we summarize the rationale behind each of the eight messages.
Don’t smoke
In the United States, smoking causes approximately 30 percent of all cancers and 90 percent of lung cancers. About half of all smokers will die from a smoking-related disease, like cancer, heart disease, and chronic obstructive lung disease. Globally, tobacco is estimated to cause just under five million deaths a year—a number that will likely rise dramatically over the next two generations [17].
Linked primarily in the public’s mind with lung cancer, smoking, and use of smokeless tobacco, cause or greatly increase the risk of many other cancers, including cancers of the head and neck, bladder, kidney, cervix, esophagus, pancreas, stomach, colon, and rectum, as well as myeloid leukemia [18, 19].
The single best way to prevent cancer and other chronic diseases is not to smoke. In the United States alone, over 150,000 cancer deaths could be avoided each year if tobacco use were eliminated completely [20]. Globally, it is estimated that if half of smoking adults stopped by 2020, 150–180 million smoking-related deaths could be avoided over the next three decades [21].
Preventing teens and young adults from taking up smoking provides the biggest health benefits, yet despite stepped up efforts to prevent tobacco use, over 20 percent of the U.S. population still smokes [22]. Cessation has large, demonstrated benefits and should be a key part of any prevention recommendations. Within 2 years of quitting, the risk of many smoking-related diseases begin to drop, and after 10–20 years, the risk of lung cancer and most other tobacco-related diseases nearly equals that of non-smokers [8, 23].
Maintain a healthy weight
Although weight is one of the most important risk factors for cancer, an American Cancer Society commissioned survey found that less than 10 percent of the public were aware that being overweight could increase the risk of cancer [24]. Yet convincing evidence shows that about 90,000 deaths from cancer could be avoided each year in the United States if everyone maintained a healthy weight throughout life [25].
Carrying extra weight, particularly being obese (BMI ≥ 30), has been strongly linked in prospective data from over 2 million women and men to an increased risk of developing cancers of the breast (after menopause), colon, kidney, pancreas, endometrium, and esophagus (adenocarcinoma) [26]. There is growing evidence that obesity also increases the risk of leukemia, lymphoma, multiple myeloma, and cancers of the liver and gallbladder [26] (Table 2).
Evidence showing that weight loss can lead to a demonstrated lower cancer risk is still developing [12]. This is likely due in large part to the general difficultly of losing weight and then maintaining the loss over time. Most research studies have not had enough subjects with large enough weight differences maintained over a long enough follow-up period to reveal any possible benefits for direct cancer endpoints.
However, there is substantial evidence that weight loss has beneficial effects on biomarkers that serve as intermediate endpoints in the pathway to cancer. Lowering BMI has been shown, for example, to improve insulin levels and also to lower circulating estrogen levels [27].
For direct evidence, a 28-year follow-up in the Nurses’ Health Study found that sustained weight loss could cut the risk of postmenopausal breast cancer by over half, with weight loss of as little as five pounds significantly decreasing risk [7].
The well-documented trends in the rising prevalence of overweight and obesity in the United States predict a growing burden of not only weight-related cancers but also heart disease, stroke, and diabetes. The latest data show that a full two-thirds of the population is either overweight (BMI 25–29.9) or obese [28]. Over the last two decades, rates of obesity have significantly increased across the nation, with over a third of the population now considered obese [28, 29]. Such trends, while most pronounced in the United States, are being expressed worldwide as well, pointing to a huge future global burden from weight-related diseases [30].
Exercise regularly
Overall, in the United States, it is estimated that 5 percent of cancers are linked to lack of regular exercise, which is largely accounted for through two common cancers, breast cancer and colon cancer [2]. Regular physical activity lowers the risk of colon adenomas and colon cancer by about 15–20 percent [31, 32]. For breast cancer, the benefits of regular exercise seem largest for premenopausal women, but postmenopausal women see lower risks from regular physical activity as well [33–35]. Though data are still developing, some evidence supports the theory that adolescent activity level may be even more important to breast cancer risk than adult activity level, as it can lower lifetime estrogen exposure through increased leanness and delayed menarche [35].
Despite its demonstrated health benefits, over 50 percent of the U.S. population does not get the recommended amount of activity each week—either 30 min of moderate activity (like brisk walking) 5 or more days per week, or 20 min of vigorous activity (like running) 3 or more days per week [36]. About a third of the U.S. population gets no leisure-time activity [37], and in some counties, the rate of inactivity crests 40 percent [38]. Two-thirds of people do not know how much physical activity they should be getting [14].
Eat a healthy diet
A healthy diet is key to overall health and can help lower the risk of numerous cancers. The most important aspect of diet for cancer prevention is overnutrition [39]. Overconsumption of calories, and the weight gain it causes, contributes greatly to cancer burden. Keeping calories in check, so weight stays in check, is therefore a key part of any healthy diet recommendation and is reflected in the 2010 Dietary Guidelines for Americans and the American Cancer Society Guidelines on Nutrition and Physical Activity for Cancer Prevention [40, 41].
Outside of overnutrition, good evidence shows that a cancer risk reducing diet is as follows: largely plant based (with a lot of fruits, vegetables, and whole grains); low in animal products (like animal fat, red meat, and processed meat); low in sodium; and, for men, not too high in calcium (less than 1,500 mg/day) [42] .
A daily multivitamin can provide added protection against certain cancers and other chronic diseases [43, 44]. Although some recent trials have had null results when looking at supplement use and cancer risk, there is a growing body of evidence that calcium and vitamin D (found in increasing levels in most multivitamins) protect against colon cancer [45–54]. Long-term folate intake has also been shown to lower the risk of colon cancer, as well as breast cancer in women who regularly drink alcohol [55–59].
Cancers with a link to diet include: breast cancer, colon cancer, esophageal cancer, lung cancer, oral cancer, pancreatic cancer, prostate cancer, pharyngeal cancer, laryngeal cancer, and stomach cancer, as well as kidney and uterine cancer, which are linked through weight gain [3, 5, 42].
Drink alcohol in moderation, if at all
The dual health effects of alcohol give it a complex role in public health. While studies consistently show that moderate alcohol consumption can significantly lower the risk of cardiovascular disease, drinking even a small amount of alcohol (less than one drink/day) can raise the risk of numerous cancers, including two of the most common—breast and colon [42, 60]. For both breast cancer and colon cancer, alcohol likely increases risk by acting as a folate antagonist and therefore lowering serum levels of folate, among other possible causal mechanisms. Good evidence, though, suggests that taking a folate supplement can help eliminate some of the cancer risk linked to alcohol [61–63].
Balancing these risks and benefits is key to the pubic health messages about alcohol intake. Although the benefits of moderate intake are well established, the cancer risk and potential for alcohol dependence means that non-drinkers should not be encouraged to start drinking. Most of those who already drink moderately, though, do not need to be encouraged to stop. While cancer risk may be increased slightly in this group, the cardiovascular benefits are significant as well. All heavy drinkers, though, should be encouraged to cut back to moderate levels, or stop altogether.
Protect yourself from the sun
With melanoma rates rising steadily from year to year both in the United States and worldwide, proper sun protection is a key public health message [64]. Yet in the United States, the percent of the population reporting a sun burn over the past year is rising, with a third reporting at least one sunburn, and about 20 percent reporting four or more [65].
Severe sunburns and unprotected sun exposure can greatly increase the risk of melanoma, particularly in susceptible groups, such as those with fair skin and hair [66–68]. Over exposure in youth seems especially linked to increased risk later in life.
Yet, it is estimated that about 50 percent of the adult population rarely uses sunscreen, and 50–80 percent do not wear sun-protective clothing when outside on sunny days [69].
There is some evidence promoting unprotected “safe sun” exposure, which could help elevate serum vitamin D (25(OH)D) levels, which in turn could lower risk of osteoporosis and certain cancers [54, 70, 71]. One recent study found that whites who stayed out of the sun or wore long sleeve shirts increased their risk of vitamin D deficiency [72].
Currently, though, population rates of sun-protection practices are so low, that for now the public should be encouraged to properly protect themselves (and their children) from the sun whenever possible, which includes: avoiding the sun as much as possible during peak burning hours (10 am–4 pm); wearing long-sleeve shirts, long pants, and wide-brimmed hats, and; properly applying broad-spectrum sun screen.
Protect yourself from infections
Infections play an important role in the development of certain cancers. Worldwide, approximately 15 percent of all cancers have been linked to infections. In developing countries marked by poor living conditions and inadequate health care, this number reaches almost 25 percent [73].
At least ten infectious agents are known to increase the risk of cancer (Table 3), several of which are quite common. Of particular importance are human papillomavirus (HPV), hepatitis B and C viruses, and Helicobacter pylori. HPV is a sexually transmitted virus that is linked to numerous cancers, with cervical cancer being the most important. Hepatitis B and C infect the liver and together account for the large majority of liver cancer. Finally, Helicobacter pylori has been estimated to cause upward of 75 percent of all stomach cancers, the second leading cancer worldwide [74].
Concrete steps like avoiding blood exposure (e.g., by not sharing needles), practicing safer sex and, for women, getting regular Pap tests and possibly HPV tests can help lower risk. There is also very strong evidence that vaccinating girls (around age 11 or 12) effectively protects against major types of HPV that can cause cervical cancer later in life [75, 76]. Vaccinating boys against HPV is also likely to lower risk of anal cancer and further protect girls by lowering the overall presence and transmission rates of cancer-associated HPV [77]. The hepatitis B vaccine reduces liver cancer risk, and its growing use worldwide is expected to result in similar benefits to those expected with the HPV vaccine [11, 78]. Advances on vaccines for other agents also offer much promise.
Get screening tests regularly
Cancer screening at regular intervals with effective tests is established to protect against some specific cancers. Regular screening with sigmoidoscopy, for example, has been shown in a large randomized controlled trial to cut the risk of colorectal cancer by about 25 percent, and the risk of dying of the disease by nearly a third [79]. Fecal occult blood test cuts colorectal cancer mortality by up to a quarter [80, 81]. Modeling data estimate that modest compliance to recommendations for colonoscopy every 10 years can reduce colorectal cancer incidence by 58 percent [82].
Pap tests, along with the addition of the newer human papillomavirus (HPV) test, help assess future cancer risk and allow treatment of identified precursor lesions. With widespread use of the Pap test, incidence and mortality rates of invasive cervical cancer have dropped by over 40 percent in the United States since 1973 [83].
Though clinical breast examination and mammography are not preventive, they are keys to early detection and successful, less aggressive treatment of breast cancer, conferring significant survival benefit [84].
Despite its common use, the benefits of prostate-specific antigen (PSA) screening for prostate cancer are not as clear as those of other recommended screening tests and should be offered to men only in concert with a clear discussion of its limitations and potential risks and benefits [85].
Recently, the large National Lung Screening Trial has shown significant lung cancer and all-cause mortality benefits with low-dose-computed tomographic scans in current and former heavy smokers [86]. Open questions remain, though, on exactly how to translate these findings to effective population-wide screening recommendations [87].
Statistics show a clear need for improvement in rates and implementation of cancer screening, with half of all colorectal and cervical cancers, and a third of all breast cancers, still diagnosed in late stages [88].
Importance of policy
As various social science models show, individuals do not often act in a vacuum [89]. So, while the “Eight Ways” are intended to help guide and promote healthy behaviors in individuals, their messages must be broadly reflected across the environmental and social influences that surround people if they are going to result in successful and sustained behavior change in people and populations.
Policies—whether those of workplaces, insurers, schools, or governments—can help create environments that promote and support a healthy, cancer-preventing lifestyle [90]. Momentum for positive policy changes has been slowly gaining in some areas [91]. Awareness of the need to stem the tide of childhood obesity is spurring action by many groups, and restrictions on tobacco use continue to grow, even across Europe, which once seemed impervious to such policies [92–95].
Still much more needs to be done at both the local, state, and federal levels to help individual make healthier choices that will realize the huge potential of cancer prevention.
Conclusion
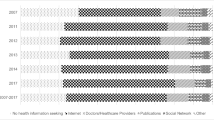
Approximately eighty percent of all Internet users search online for health information [96]. With much of this information scientifically suspect, there is benefit in developing sound, evidence-based messages the public can both trust and find useful. That should be a major goal for any health communication program and is the genesis behind the “Eight Ways to Stay Healthy and Prevent Cancer.” While such messages are not an end in themselves, they form an evidence-based and targeted framework that supports broader cancer prevention efforts. They can be readily used by cancer center outreach programs and community groups to focus priority on prevention efforts in local communities and to guide policy strategies that will make our population healthier, save health care expenditures, and avoid future pain and suffering.
References
Doll R, Peto R (1981) The causes of cancer: quantitative estimates of avoidable risks of cancer in the United States today. J Natl Cancer Inst 66:1191–1308
Colditz G, DeJong D, Hunter DJ, Trichopoulos D, Willett WC (1996) Harvard report on cancer prevention. Volume 1: causes of human cancer. Cancer Causes Control 7(Suppl 1):S3–59
(1997) Harvard report on cancer prevention. Volume 2: prevention of human cancer. Cancer Causes Control 8(Suppl 1):1–50. http://www.jstor.org/stable/i284404
Colditz GA, Sellers TA, Trapido E (2006) Epidemiology—identifying the causes and preventability of cancer? Nat Rev Cancer 6(1):75–83
Colditz G, DeJong D, Hunter DJ, Trichopoulos D, Willett WC (1996) Harvard report on cancer prevention. Volume 1: causes of human cancer, summary. Cancer Causes Control 7(Suppl 1):S55–S58
Flood DM, Weiss NS, Cook LS, Emerson JC, Schwartz SM, Potter JD (2000) Colorectal cancer incidence in Asian migrants to the United States and their descendants. Cancer Causes Control 11(5):403–411
Eliassen AH, Colditz GA, Rosner B, Willett WC, Hankinson SE (2006) Adult weight change and risk of postmenopausal breast cancer. JAMA 296(2):193–201
Speizer FE, Colditz GA, Hunter DJ, Rosner B, Hennekens C (1999) Prospective study of smoking, antioxidant intake, and lung cancer in middle-aged women (USA). Cancer Causes Control 10(5):475–482
Cuzick J, Forbes JF, Sestak I, Cawthorn S, Hamed H, Holli K, Howell A (2007) Long-term results of tamoxifen prophylaxis for breast cancer—96-month follow-up of the randomized IBIS-I trial. J Natl Cancer Inst 99(4):272–282
Martino S, Cauley JA, Barrett-Connor E, Powles TJ, Mershon J, Disch D, Secrest RJ, Cummings SR (2004) Continuing outcomes relevant to Evista: breast cancer incidence in postmenopausal osteoporotic women in a randomized trial of raloxifene. J Natl Cancer Inst 96(23):1751–1761
Chang MH, You SL, Chen CJ, Liu CJ, Lee CM, Lin SM, Chu HC, Wu TC, Yang SS, Kuo HS, Chen DS (2009) Decreased incidence of hepatocellular carcinoma in hepatitis B vaccinees: a 20-year follow-up study. J Natl Cancer Inst 101(19):1348–1355
Wolin KY, Carson K, Colditz GA (2010) Obesity and cancer. Oncologist 15(6):556–565
National Cancer Institute (2008) Health information national trends survey: hints brief—number 9. http://hints.cancer.gov/brief_9.jsp?t=brief9. Accessed April 20, 2011
Bennett GG, Wolin KY, Puleo EM, Masse LC, Atienza AA (2009) Awareness of national physical activity recommendations for health promotion among US adults. Med Sci Sports Exerc 41(10):1849–1855
American Institute for Cancer Research (2007) Facts vs. fears survey
Colditz GA, Atwood KA, Emmons K, Monson RR, Willett WC, Trichopoulos D, Hunter DJ (2000) Harvard report on cancer prevention volume 4: Harvard cancer risk index. Risk Index Working Group, Harvard Center for Cancer Prevention. Cancer Causes Control 11(6):477–488
Ezzati M, Lopez AD (2003) Estimates of global mortality attributable to smoking in 2000. Lancet 362(9387):847–852
Colditz GA, Stein CJ (2004) Handbook of cancer risk assessment and prevention. Jones and Bartlett Publishers, Sudbury
United States Public Health Service. Office of the Surgeon General, United States. Office on Smoking and Health. (2010) How tobacco smoke causes disease: the biology and behavioral basis for smoking-attributable disease: a report of the surgeon general. U.S. Department of Health and Human Services, Public Health Service for sale by the Supt. of Documents, U.S. G.P.O., Rockville, MD, Washington, DC
Centers for Disease Control and Prevention (CDC) (2002) Annual smoking-attributable mortality, years of potential life lost, and economic costs—United States, 1995–1999. MMWR Morb Mortal Wkly Rep 51(14):300–303
Jha P (2009) Avoidable global cancer deaths and total deaths from smoking. Nat Rev Cancer 9(9):655–664
Centers for Disease Control and Prevention (CDC) (2007) Cigarette smoking among adults—United States, 2006. MMWR Morb Mortal Wkly Rep 56(44):1157–1161
Peto R, Darby S, Deo H, Silcocks P, Whitley E, Doll R (2000) Smoking, smoking cessation, and lung cancer in the UK since 1950: combination of national statistics with two case-control studies. BMJ 321(7257):323–329
American Cancer Society (2006) Few Americans know connection between excess weight and cancer risk, survey finds
Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ (2003) Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med 348(17):1625–1638
Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M (2008) Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet 371(9612):569–578
McTiernan A, Rajan KB, Tworoger SS, Irwin M, Bernstein L, Baumgartner R, Gilliland F, Stanczyk FZ, Yasui Y, Ballard-Barbash R (2003) Adiposity and sex hormones in postmenopausal breast cancer survivors. J Clin Oncol 21(10):1961–1966
Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM (2006) Prevalence of overweight and obesity in the United States, 1999–2004. JAMA 295(13):1549–1555
Centers for Disease Control and Prevention (2007) U.S. obesity trends 1985–2006
World Cancer Research Fund (2011) cancer facts and figures—obesity. http://www.wcrf.org/cancer_facts/obesity.php. Accessed April 14, 2011
Wolin KY, Yan Y, Colditz GA, Lee IM (2009) Physical activity and colon cancer prevention: a meta-analysis. Br J Cancer 100(4):611–616
Wolin KY, Yan Y, Colditz GA (2011) Physical activity and risk of colon adenoma: a meta-analysis. Br J Cancer 104(5):882–885
Bernstein L, Henderson BE, Hanisch R, Sullivan-Halley J, Ross RK (1994) Physical exercise and reduced risk of breast cancer in young women. J Natl Cancer Inst 86(18):1403–1408
Bernstein L, Patel AV, Ursin G, Sullivan-Halley J, Press MF, Deapen D, Berlin JA, Daling JR, McDonald JA, Norman SA, Malone KE, Strom BL, Liff J, Folger SG, Simon MS, Burkman RT, Marchbanks PA, Weiss LK, Spirtas R (2005) Lifetime recreational exercise activity and breast cancer risk among black women and white women. J Natl Cancer Inst 97(22):1671–1679
Maruti SS, Willett WC, Feskanich D, Rosner B, Colditz GA (2008) A prospective study of age-specific physical activity and premenopausal breast cancer. J Natl Cancer Inst 100(10):728–737
Centers for Disease Control and Prevention (CDC) (2005) Adult participation in recommended levels of physical activity—United States, 2001 and 2003. MMWR Morb Mortal Wkly Rep 54(47):1208–1212
Pleis JR, Ward BW, Lucas JW (2010) Summary health statistics for U.S. adults: national health interview survey, 2009, vol 10. National Center for Health Statistics
Centers for Disease Control and Prevention: National Diabetes Surveillance System (2011) County-level estimates of leisure-time physical inactivity—US maps
Willett WC (2000) Diet and cancer. Oncologist 5(5):393–404
U.S. Department of Agriculture and U.S. Department of Health and Human Services (2010) Dietary guidelines for Americans, 2010, 7th edn. Government Printing Office, Washington, DC
American Cancer Society (2011) ACS guidelines on nutrition and physical activity for cancer prevention
World Cancer Research Fund, American Institute for Cancer Research (2007) Food, nutrition, physical activity, and the prevention of cancer: a global perspective. WCRF/AICR, Washington, DC
Fairfield KM, Fletcher RH (2002) Vitamins for chronic disease prevention in adults: scientific review. JAMA 287(23):3116–3126
Fletcher RH, Fairfield KM (2002) Vitamins for chronic disease prevention in adults: clinical applications. JAMA 287(23):3127–3129
Huang HY, Caballero B, Chang S, Alberg AJ, Semba RD, Schneyer CR, Wilson RF, Cheng TY, Vassy J, Prokopowicz G, Barnes GJ 2nd, Bass EB (2006) The efficacy and safety of multivitamin and mineral supplement use to prevent cancer and chronic disease in adults: a systematic review for a National Institutes of Health state-of-the-science conference. Ann Intern Med 145(5):372–385
Park SY, Murphy SP, Wilkens LR, Henderson BE, Kolonel LN (2011) Multivitamin use and the risk of mortality and cancer incidence: the multiethnic cohort study. Am J Epidemiol 173(8):906−914
Garland CF, Gorham ED, Mohr SB, Garland FC (2009) Vitamin D for cancer prevention: global perspective. Ann Epidemiol 19(7):468–483
Garland CF, Garland FC, Gorham ED (1991) Can colon cancer incidence and death rates be reduced with calcium and vitamin D? Am J Clin Nutr 54(1 Suppl):193S–201S
Garland CF, Comstock GW, Garland FC, Helsing KJ, Shaw EK, Gorham ED (1989) Serum 25-hydroxyvitamin D and colon cancer: eight-year prospective study. Lancet 2(8673):1176–1178
Wu K, Willett WC, Fuchs CS, Colditz GA, Giovannucci EL (2002) Calcium intake and risk of colon cancer in women and men. J Natl Cancer Inst 94(6):437–446
Platz EA, Hankinson SE, Hollis BW, Colditz GA, Hunter DJ, Speizer FE, Giovannucci E (2000) Plasma 1,25-dihydroxy- and 25-hydroxyvitamin D and adenomatous polyps of the distal colorectum. Cancer Epidemiol Biomarkers Prev 9(10):1059–1065
Martinez ME, Giovannucci EL, Colditz GA, Stampfer MJ, Hunter DJ, Speizer FE, Wing A, Willett WC (1996) Calcium, vitamin D, and the occurrence of colorectal cancer among women. J Natl Cancer Inst 88(19):1375–1382
Kearney J, Giovannucci E, Rimm EB, Ascherio A, Stampfer MJ, Colditz GA, Wing A, Kampman E, Willett WC (1996) Calcium, vitamin D, and dairy foods and the occurrence of colon cancer in men. Am J Epidemiol 143(9):907–917
Giovannucci E (2005) The epidemiology of vitamin D and cancer incidence and mortality: a review (United States). Cancer Causes Control 16(2):83–95
Kim DH, Smith-Warner SA, Spiegelman D, Yaun SS, Colditz GA, Freudenheim JL, Giovannucci E, Goldbohm RA, Graham S, Harnack L, Jacobs EJ, Leitzmann M, Mannisto S, Miller AB, Potter JD, Rohan TE, Schatzkin A, Speizer FE, Stevens VL, Stolzenberg-Solomon R, Terry P, Toniolo P, Weijenberg MP, Willett WC, Wolk A, Zeleniuch-Jacquotte A, Hunter DJ (2010) Pooled analyses of 13 prospective cohort studies on folate intake and colon cancer. Cancer Causes Control 21(11):1919–1930
Lee JE, Willett WC, Fuchs CS, Smith-Warner SA, Wu K, Ma J, Giovannucci E (2011) Folate intake and risk of colorectal cancer and adenoma: modification by time. Am J Clin Nutr 93(4):817–825
Giovannucci E (2003) Diet, body weight, and colorectal cancer: a summary of the epidemiologic evidence. J Womens Health (Larchmt) 12(2):173–182
Giovannucci E, Stampfer MJ, Colditz GA, Hunter DJ, Fuchs C, Rosner BA, Speizer FE, Willett WC (1998) Multivitamin use, folate, and colon cancer in women in the Nurses’ Health Study. Ann Intern Med 129:517
Kennedy DA, Stern SJ, Moretti M, Matok I, Sarkar M, Nickel C, Koren G (2011) Folate intake and the risk of colorectal cancer: a systematic review and meta-analysis. Cancer Epidemiol 35(1):2–10
Gunzerath L, Faden V, Zakhari S, Warren K (2004) National institute on alcohol abuse and alcoholism report on moderate drinking. Alcohol Clin Exp Res 28(6):829–847
Linos E, Willett WC (2007) Diet and breast cancer risk reduction. J Natl Compr Canc Netw 5(8):711–718
Giovannucci E, Chen J, Smith-Warner SA, Rimm EB, Fuchs CS, Palomeque C, Willett WC, Hunter DJ (2003) Methylenetetrahydrofolate reductase, alcohol dehydrogenase, diet, and risk of colorectal adenomas. Cancer Epidemiol Biomarkers Prev 12(10):970–979
Giovannucci E (2002) Epidemiologic studies of folate and colorectal neoplasia: a review. J Nutr 132(8 Suppl):2350S–2355S
Centers for Disease Control and Prevention (2010) Skin cancer trends
Centers for Disease Control and Prevention (CDC) (2007) Sunburn prevalence among adults—United States, 1999, 2003, and 2004. MMWR Morb Mortal Wkly Rep 56(21):524–528
Han J, Colditz GA, Hunter DJ (2006) Risk factors for skin cancers: a nested case-control study within the Nurses’ Health Study. Int J Epidemiol 35(6):1514–1521
Cho E, Rosner BA, Colditz GA (2005) Risk factors for melanoma by body site. Cancer Epidemiol Biomarkers Prev 14(5):1241–1244
Cho E, Rosner BA, Feskanich D, Colditz GA (2005) Risk factors and individual probabilities of melanoma for whites. J Clin Oncol 23(12):2669–2675
Coups EJ, Manne SL, Heckman CJ (2008) Multiple skin cancer risk behaviors in the U.S. population. Am J Prev Med 34(2):87–93
Holick MF (2007) Vitamin D deficiency. N Engl J Med 357(3):266–281
Garland CF, Garland FC, Gorham ED, Lipkin M, Newmark H, Mohr SB, Holick MF (2006) The role of vitamin D in cancer prevention. Am J Public Health 96(2):252–261
Linos E, Keiser E, Kanzler M, Sainani KL, Lee W, Vittinghoff E, Chren MM, Tang JY (2012) Sun protective behaviors and vitamin D levels in the US population: NHANES 2003–3006. Cancer Causes Control 23(1):133–140
Franceschi S (2000) Strategies to reduce the risk of virus-related cancers. Ann Oncol 11(9):1091–1096
Scheiman JM, Cutler AF (1999) Helicobacter pylori and gastric cancer. Am J Med 106(2):222–226
Markowitz LE, Dunne EF, Saraiya M, Lawson HW, Chesson H, Unger ER (2007) Quadrivalent human papillomavirus vaccine: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 56(RR-2):1–24
The GlaxoSmithKline Vaccine HPV-007 Study Group (2009) Sustained efficacy and immunogenicity of the human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine: analysis of a randomised placebo-controlled trial up to 6·4 years. Lancet. doi:10.1016/S0140-6736(09)61567-1
Kim JJ (2011) Focus on research: weighing the benefits and costs of HPV vaccination of young men. N Engl J Med 364(5):393–395
Lavanchy D (2005) Worldwide epidemiology of HBV infection, disease burden, and vaccine prevention. J Clin Virol 34(Suppl 1):S1–S3
Atkin WS, Edwards R, Kralj-Hans I, Wooldrage K, Hart AR, Northover JM, Parkin DM, Wardle J, Duffy SW, Cuzick J (2010) Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicentre randomised controlled trial. Lancet 375(9726):1624–1633
Towler BP, Irwig L, Glasziou P, Weller D, Kewenter J (2000) Screening for colorectal cancer using the faecal occult blood test, hemoccult. Cochrane Database Syst Rev 2:CD001216. doi:10.1002/14651858.CD001216
Tomeo CA, Colditz GA, Willett WC, Giovannucci E, Platz E, Rockhill B, Dart H, Hunter DJ (1999) Harvard report on cancer prevention. Volume 3: prevention of colon cancer in the United States. Cancer Causes Control 10(3):167–180
Frazier AL, Colditz GA, Fuchs CS, Kuntz KM (2000) Cost-effectiveness of screening for colorectal cancer in the general population. JAMA 284(15):1954–1961
McCrory DC, Matchar DB, Bastian L, Datta S, Hasselblad V, Hickey J, Myers E, Nanda K (1999) Evaluation of cervical cytology. Evid Rep Technol Assess (Summ) 5:1–6
Smith RA, Cokkinides V, Brooks D, Saslow D, Brawley OW (2010) Cancer screening in the United States, 2010: a review of current American Cancer Society guidelines and issues in cancer screening. CA Cancer J Clin 60(2):99–119
Wolf AM, Wender RC, Etzioni RB, Thompson IM, D’Amico AV, Volk RJ, Brooks DD, Dash C, Guessous I, Andrews K, DeSantis C, Smith RA (2010) American Cancer Society guideline for the early detection of prostate cancer: update 2010. CA Cancer J Clin 60(2):70–98
The National Lung Screening Trial Research Team (2011) Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 365(5):395–409
Sox HC (2011) Better evidence about screening for lung cancer. N Engl J Med 365(5):455–457
Henley SJ, King JB, German RR, Richardson LC, Plescia M (2010) Surveillance of screening-detected cancers (colon and rectum, breast, and cervix)—United States, 2004–2006. MMWR Surveill Summ 59(9):1–25
National Cancer Institute (2005) Theory at a glance: a guide for health promotion practice. http://www.cancer.gov/cancertopics/cancerlibrary/theory.pdf. Accessed 15 July 2011
Colditz GA, Samplin-Salgado M, Ryan CT, Dart H, Fisher L, Tokuda A, Rockhill B (2002) Harvard report on cancer prevention, volume 5: fulfilling the potential for cancer prevention: policy approaches. Cancer Causes Control 13(3):199–212
Sorensen G, Landsbergis P, Hammer L, Amick BC 3rd, Linnan L, Yancey A, Welch LS, Goetzel RZ, Flannery KM, Pratt C (2011) Preventing chronic disease in the workplace: a workshop report and recommendations. Am J Public Health 101(Suppl 1):S196–S207
Strasburger VC (2006) Children, adolescents, and advertising. Pediatrics 118(6):2563–2569
William J. Clinton Foundation (2007) Alliance for a healthier generation. http://www.clintonfoundation.org/what-we-do/alliance-for-a-healthier-generation/. Accessed 21 Feb 2012
Let’s Move (2011) Let’s move: America’s move to raise a healthier generation of kids. http://www.letsmove.gov/. Accessed 14 Feb 2011
Lagiou P, Trichopoulos D (2007) Legislative measures and tobacco control in Europe. Prev Med 45(2–3):121–122
Pew Internet and American Life Project (2011) Health topics. http://pewinternet.org/Reports/2011/HealthTopics/Summary-of-Findings.aspx?view=all. Accessed 2 January 2012
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dart, H., Wolin, K.Y. & Colditz, G.A. Commentary: eight ways to prevent cancer: a framework for effective prevention messages for the public. Cancer Causes Control 23, 601–608 (2012). https://doi.org/10.1007/s10552-012-9924-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-012-9924-y