
Abstract
Purpose
Composition of dietary fatty acid intake, which influences cytokine production, may contribute to the development of non-Hodgkin’s lymphoma (NHL). Serum lipid levels may serve as biomarkers of inflammation associated with NHL risk.
Methods
We conducted a case–control analysis (275 cases and 549 controls) nested within the Multiethnic Cohort Study (whites, Japanese Americans, Latinos, African Americans, and Native Hawaiians) to examine the association of prediagnostic, erythrocyte membrane phospholipid fatty acid composition, and serum cholesterol and triglyceride (TG) concentrations with the risk of NHL. Conditional logistic regression was used to calculate odds ratios (OR) and 95 % confidence intervals (CI) by tertiles of biomarker concentrations.
Results
Higher total saturated fatty acids (SFA) were associated with an increase in NHL risk (ORT3 vs. T1 = 1.57 [95 % CI: 1.03–2.39]; p trend = 0.01), whereas no associations were detected for total n−3 or n−6 polyunsaturated fatty acids. Inverse associations were observed for total cholesterol (TC; OR T3 vs. T1 = 0.51 [95 % CI: 0.35–0.74]; p trend < 0.0001) and high-density lipoprotein cholesterol (HDL-C; OR T3 vs. T1 = 0.47 [95 % CI: 0.31–0.71]; p trend = 0.0001) but not for low-density lipoprotein cholesterol or TG. Adjustment for the use of lipid-lowering medication did not modify the results substantially.
Conclusions
This prospective biomarker investigation offers supportive evidence for an adverse effect of higher erythrocyte membrane SFA levels on NHL risk, but preclinical effects cannot be excluded. Inverse relations between prediagnostic, circulating TC and HDL-C and NHL risk may be due to reverse causation or a result of protective actions of these lipids and lipoproteins.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The incidence of non-Hodgkin’s lymphoma (NHL) has increased over the past few decades, although incidence rates differ by ethnicity and region [1]. While the large variety and heterogeneity of NHL subtypes complicate the study of etiology, immune dysfunction has been linked to the rise in overall NHL risk. Among the potential risk factors that have been investigated, dietary fatty acids, which are essential components of cell membranes and affect eicosanoid and cytokine production, are thought to alter inflammatory responses and contribute to lymphomagenesis [2–6]. In particular, the ratio of n−3 and n−6 polyunsaturated fatty acids (PUFAs) may play a key role in influencing NHL risk, as these essential fatty acids compete in the release of anti- and pro-inflammatory eicosanoids, respectively, and n−3 PUFAs suppress pro-inflammatory cytokine production. Previous studies have also shown a positive association of dietary saturated fatty acid (SFA) intake with higher NHL risk, possibly through pro-inflammatory mediator production [7–11]. Given the possible etiologic differences among NHL subtypes, dietary composition of fatty acids may affect disease development differentially just as reported for mutagens from meat products [12]. In exploring the influences of dietary fatty acids, self-reported intake using food frequency questionnaires (FFQ) and dietary recalls is often used, but these methods are subject to an appreciable degree of measurement error. Biologic measures of dietary exposure may be more relevant in evaluating hypothesized associations with disease risk [13]. Erythrocyte membrane phospholipid fatty acid composition provides a measure of relative dietary fatty acid intake over several months by estimating the proportion of each fatty acid to total fatty acids in red blood cells (RBCs) [14]. Other biomarkers serving as proxies of dietary fatty acid intake include high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), total cholesterol (TC), and triglycerides (TG) [2, 15, 16]. In this case–control analysis nested within the Multiethnic Cohort Study (MEC), we examined the associations between prediagnostic erythrocyte membrane fatty acid composition and serum HDL-C, LDL-C, TC, and TG, and risk of NHL in a population of whites, Japanese Americans, Latinos, African Americans, and Native Hawaiians residing in California and Hawaii.
Materials and methods
Study population
The MEC is a longitudinal study designed to investigate the association of dietary, lifestyle, and genetic factors with the incidence of cancer. The cohort was assembled in Hawaii and Los Angeles in 1993–1996, and details on recruitment and baseline information have been reported previously [17]. Briefly, subjects from five ethnic groups (whites, Japanese Americans, Latinos, African Americans, and Native Hawaiians) were identified primarily through drivers’ license files, supplemented with voter registration lists in Hawaii and Medicare files in California, and were recruited by mailing a self-administered, 26-page questionnaire on diet, anthropometric measures, medical history, family history of cancer, and lifestyle. A total of 215,251 men and women aged 45–75 years were included at baseline and formed a representative group of the general population as verified by a comparison of the cohort distributions across educational levels and marital status with corresponding census data for the two geographical areas [17]. The study protocol was approved by the Institutional Review Boards of the University of Hawaii and the University of Southern California.
The prospective MEC biospecimen subcohort was established in 2001–2008 by asking surviving cohort members to provide specimens of blood and urine [18]. In total, 67,594 cohort members contributed to the biorepository. When comparing the characteristics of individuals who provided specimens with those who did not, there was no substantial difference by several demographical characteristics and cancer risk factors including body mass index (BMI), dietary fat and vegetable intake, physical activity, and family history of cancer, suggesting that the biospecimen repository participants are broadly representative of all cohort members. At the time of specimen collection, a medication inventory was collected, which was used to determine the use of lipid-lowering medications.
Identification and selection of cases and controls
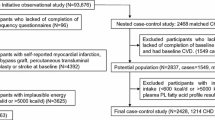
Incident cancer cases within the MEC were identified by routine linkages to the Hawaii Tumor Registry, the Los Angeles County Cancer Surveillance Program, and the State of California Cancer Registry, which are participants of the Surveillance, Epidemiology, and End Results (SEER) program [19]. NHL cases were classified according to the International Classification of Diseases for Oncology, Third Edition (ICD-O-3) and aggregated into subtypes in accordance with the proposed hierarchical classification of lymphoid neoplasms for epidemiologic research [20]. The subtypes included diffuse large B-cell lymphoma (DLBCL), chronic lymphocytic leukemia or small lymphocytic lymphoma (CLL/SLL), follicular lymphoma (FL), T-cell lymphoma (all types), and all other NHL subtypes. Controls were identified from the biospecimen subcohort who were alive and free of NHL at the age of the case’s diagnosis and matched on sex, birth date (within ± 1 year), ethnicity (white, Japanese American, Latino, African American, or Native Hawaiian), location (California or Hawaii), date of blood draw (within ± 1 year), time of day of blood draw, and fasting hours prior to blood draw (0–<6, 6–<8, 8–<10, or ≥10). Death dates were obtained through linkages with the state death certificate files in California and Hawaii and the National Death Index. Only cases with a date of blood draw before diagnosis were included in the present study. A total of 824 participants (275 cases and 549 controls) were evaluated in the current analyses: 274 cases were matched with two controls, and one case could only be matched with one control. Moreover, the specimen volume was insufficient, or the blood sample was missing for two controls for the fatty acid analyses and for up to eight cases and 21 controls for the lipid analyses. For four NHL cases and 13 controls with no available RBC specimens at the blood draw date of interest who had an additional blood sample, the second (not matched) blood sample was analyzed for fatty acids.
Laboratory analyses
Frozen RBC and serum samples stored at −180 °C were retrieved from the MEC biorepository in matched case–control sets, thawed, and analyzed together within batches. The laboratory personnel were blinded to the case–control status of the samples. Quantification of fatty acids in the erythrocyte membrane phospholipids was performed using gas chromatography (GC) [21]. A standardized protocol was used to collect, process, and store blood components at both study sites. Heparinized blood was centrifuged, and the plasma was removed. Approximately 8 mL of the packed heparinized red cells were suspended in phosphate-buffered saline (PBS) buffer, mixed, and centrifuged for 5 min. After a second wash, the clear supernatant was again removed. A dilution of the red cells was made: 3 mL of washed RBC to 1 mL of PBS. This thick mixture was aspirated into the straws and stored in vapor-phase liquid nitrogen freezers. Samples were thawed, and RBCs were lysed with two volumes of distilled water and membranes collected by centrifugation at 11,400×g for 30 min at 4 °C. The pellets were washed twice with PBS and dispersed in 100 μl of PBS and used for fatty acid analysis. Total fatty acid was converted to methyl esters (FAMEs) using a methanol/benzene mixture [21]. The FAMEs were separated and quantified by use of an Agilent Technologies (San Diego, CA) 5890A series II GC fitted with a model 7673 automatic split-injection system and flame ionization detector and SP2380 stabilized phase fused silica capillary column (30 m × 0.32 mm i.d., 0.25 um film thickness, Supelco, Inc, Bellefonte, PA). Quantification was based on the recovery of a known quantity of the internal standard (heptadecanoic acid, NuChek Preparation Inc., Elysian, MN) and on the response ratio of fatty acid standards purchased from NuChek Preparation Inc. (Elysian, MN). Specific fatty acids were presented as percentage of total fatty acid measured in the erythrocyte membrane phospholipids. Based on 16 triplet pooled samples, the within- and between-batch coefficients of variation (CV) of fatty acids (expressed as % total FA) ranged from 0.8 ± 0.7 and 1.6 ± 1.1 % for stearic acid (C18:0) to 12.6 ± 13.8 and 29.2 ± 18.1 % for α-linolenic acid (C18:3 n−3).
For circulating lipid measures, serum TG, TC, and HDL-C were measured using an automated chemical analyzer (Cobas, MiraPlus, Roche Diagnostics, Switzerland). Subsequently, the LDL-C levels were determined by the Friedwald computation (TC–HDL-C–[TG/5]) [22]. Based on 18 duplicate and nine triplet pooled samples, the within- and between-batch CVs were calculated for serum lipids, respectively, as: 4.8 ± 19.1 and 3.9 ± 3.1 % for HDL-C, 3.6 ± 5.3 and 2.8 ± 2.9 % for LDL-C, 1.5 ± 1.9 and 1.8 ± 1.3 % for TC, and 1.1 ± 1.0 and 6.0 ± 5.6 % for TG.
Statistical analyses
SAS software version 9.2 (SAS Institute, Inc., Cary, NC) was used to perform all statistical analyses, with a two-sided p value of <0.05 considered statistically significant. Characteristics at cohort entry were compared between NHL cases and controls using chi-square tests for categorical variables and student’s t tests for continuous variables. Spearman correlation coefficients were calculated between erythrocyte membrane fatty acids and dietary intake estimated from the baseline FFQ for total monounsaturated fatty acid (MUFA), total PUFA, and total SFA (computed as % total fatty acid) [17]. Odds ratios (OR) and 95 % confidence intervals (CI) were estimated using conditional logistic regression with matched sets as strata relating the tertiles of prediagnostic levels of erythrocyte membrane fatty acids or serum lipids with NHL risk, and linear associations were evaluated using continuous variables that were log-transformed to meet model assumptions. Because the case distribution may be extreme compared to that of the controls due to the small cell sizes, tertiles were based on the exposure distribution of both cases and controls to maximize the number of cases within strata. Potential confounders, that is, years of education (continuous), alcohol consumption (<1 vs. ≥1 drink/month), smoking (current/past vs. never), BMI (kg/m2), physical activity (metabolic equivalents/day), history of blood transfusion (yes vs. no), history of asthma (yes vs. no), antihistamine use (yes/current, yes/not current, or no), aspirin use (yes/current, yes/not current, or no), acetaminophen use (yes/current, yes/not current, or no), and lipid-lowering medication use (yes vs. no), were examined but not included in the final models, as they were not found alone, or in combination, to change the risk estimates by more than 10 % [4, 11, 19, 23, 24].
Sensitivity analyses were performed by excluding the four cases and 13 controls whose fatty acid measures were based on a second blood sample. We also excluded cases and controls whose fasting duration before blood collection were <8 h (31 cases and 58 controls for fatty acid analysis and 33 cases and 58 controls for lipid analysis). In addition, we conducted stratified analyses by follow-up years between blood draw and NHL diagnosis using the median value (2.7 years); to minimize multiple comparisons, the analyses were limited to fatty acid subtypes and cholesterol. Based on previous reports of a reduced NHL risk among statin users [16, 25], we calculated mean biomarker levels and performed stratified analyses by lipid-lowering medication use, with and without including the “unknown” responses as non-users.
We evaluated heterogeneity in risk estimates for overall NHL by sex, ethnicity, and common NHL subtype (DLBCL, CLL/SLL, and FL only). T-cell lymphomas were not included because of the small number of cases, and “other subtypes” because of the wide range of subtypes. Heterogeneity in risk estimates by sex or ethnicity was tested by a Wald test of the cross-product terms of group membership and the log-transformed analyte and across the three major NHL subtypes by a Wald test of the parameter estimates for the log-transformed analyte obtained from unconditional polytomous logistic regression accounting for the matching factors. Finally, we conducted stratified analyses by NHL subtype for fatty acid subtypes (total MUFA, n−3 and n−6 PUFAs, and total SFA) and serum lipids.
Results
The mean age at blood draw was 70.0 ± 7.5 years for both cases and controls, and the mean follow-up time between blood draw and NHL diagnosis for cases was 3.1 ± 2.3 years (Table 1). The ethnic composition for cases and controls combined was 27 % whites, 27 % Japanese Americans, 23 % Latinos, 17 % African Americans, and 6 % Native Hawaiians. The cases were similar to the controls with respect to education level, BMI, physical activity, and alcohol consumption. There were slightly more current/past smokers among NHL cases than controls (61 vs. 54 %; p = 0.07). Lipid-lowering medication use was also similar between cases and controls (27 vs. 26 %; p = 0.96). Total SFA in erythrocyte membranes was significantly higher (p = 0.03) in cases than in controls, but the magnitude of the difference was small (44.82 ± 1.16 vs. 44.65 ± 1.04 %). Individual fatty acids, as well as total MUFA, total n−3 PUFA, total n−6 PUFA, and total PUFA, did not differ between cases and controls. A comparison of relative fatty acid levels between erythrocyte membrane phospholipids and dietary intake estimated from the baseline FFQ showed modest correlations for total SFA (r spearman = 0.12; p < 0.001) and total PUFA (r spearman = 0.11; p < 0.01) and no correlation for total MUFA (r spearman = −0.02; p = 0.53). Serum TG concentrations were similar between cases and controls, whereas NHL cases had significantly lower serum HDL-C and TC concentrations than controls (49 ± 19 vs. 53 ± 19 mg/dL; p < 0.01 and 175 ± 35 vs. 185 ± 34 mg/dL; p < 0.001, respectively). Serum LDL-C concentration was also non-significantly lower in cases than in controls (103 ± 33 vs. 108 ± 34 mg/dL; p = 0.07).
Higher total SFA was associated with an increase in overall NHL risk (ORT3 vs. T1 = 1.57 [95 % CI: 1.03–2.39]; p trend = 0.01; Table 2). Among individual SFAs, only stearic acid (C18:0) indicated a similar, albeit non-significant, relation (ORT3 vs. T1 = 1.40 [95 % CI: 0.96–2.05]; p trend = 0.06). Individual PUFAs, total PUFA, the PUFA/SFA ratio, n−3 and n−6 PUFAs, and the n−3/n−6 ratio were not related to overall NHL or subtype risk (Table 3). In sensitivity analyses, excluding unmatched blood samples or samples collected after <8 h of fasting, the risk estimates did not change for any fatty acid. In stratified analyses by follow-up time, the PUFA/SFA ratio became significant (p trend = 0.02) during the first 2.7 years, whereas the positive association for total SFA was no longer significant for cases diagnosed ≥2.7 years after blood draw. The results for other fatty acid subtypes remained unchanged.
Looking at fatty acids, total n−6 PUFA was lower in users than in non-users of lipid-lowering medication (30.14 ± 2.33 vs. 30.95 ± 2.22 %; p = <0.0001), and total n−3 PUFA and the n−3/n−6 ratio were higher (10.23 ± 2.39 vs. 9.58 ± 2.36 %; p = <0.01 and 0.35 ± 0.11 vs. 0.32 ± 0.10 %; p < 0.001). When stratified by use, the association of total SFA with NHL was no longer significant in users and non-users; however, when the “unknown” responses were included as non-users, total SFA (p trend = 0.01) and the PUFA/SFA ratio (p trend = 0.03) were significant.
Heterogeneity in risk estimates across fatty acids was observed for sex, ethnicity, and NHL subtype (Table 2). Total PUFA (p heterogeneity < 0.01) and the PUFA/SFA ratio (p heterogeneity = 0.02) showed significant heterogeneity by sex. In stratified analyses, total PUFA (ORT3 vs. T1 = 0.45 [95 % CI: 0.23–0.89]; p trend = 0.01) and the PUFA/SFA ratio (ORT3 vs. T1 = 0.52 [95 % CI: 0.27–1.01]; p trend < 0.01) were inversely related to NHL risk in women and not in men (data not shown). Across ethnic groups, heterogeneity was present for palmitic acid (C16:0; p heterogeneity = 0.03) and stearic acid (C18:0; p heterogeneity < 0.01). Palmitic acid (C16:0) was related to higher NHL risk in African Americans only (ORT3 vs. T1 = 3.59 [95 % CI: 1.36–9.52]; p trend = 0.02), and stearic acid (C18:0) was associated with an increased risk in Japanese Americans (ORT3 vs. T1 = 3.47 [95 % CI: 1.54–7.79]; p trend < 0.01) and Latinos (ORT3 vs. T1 = 2.23 [95 % CI: 0.97–5.12]; p trend = 0.03). Heterogeneity by subtype was observed for arachidonic acid (C20:4 n−6; p heterogeneity = 0.02) but not for total n−6 PUFA. In stratified analyses (Table 3), arachidonic acid was related to higher NHL risk in FL only (ORT3 vs. T1 = 1.18 [95 % CI: 0.56–2.48]; p trend = 0.02; data not shown). The positive association of total SFA was not statistically significant in any given subtype.
For serum lipids, inverse associations with NHL risk were found for all of the cholesterol measures but not for TG (Table 2). The observed associations were statistically significant for HDL-C (ORT3–T1 = 0.47 [95 % CI: 0.31–0.71; p trend = 0.0001]) and TC (ORT3–T1: 0.51 [95 % CI: 0.35–0.74; p trend < 0.0001]) but not for LDL-C (OR T3–T1: 0.71 [95 % CI: 0.48–1.03; p trend = 0.08]). When the cases and controls with less than eight fasting hours were excluded, the inverse relation for LDL-C became significant (p trend = 0.04). In stratified analyses by follow-up time, the significant results for HDL-C remained unchanged; however, TC was no longer significant (p trend = 0.06) in cases diagnosed after ≥2.7 years of blood draw. As expected, lipid-lowering medication users had lower levels of LDL-C and TC than non-users (93 ± 29 vs. 110 ± 34 mg/dL; p < 0.0001 and 170 ± 31 vs. 186 ± 35; p < 0.0001); however, HDL and triglycerides did not differ significantly. Adjustment for the use of lipid-lowering medication had little impact on the inverse associations. In additional stratified analyses by user status, the significant results for HDL-C and TC remained unchanged among non-users, whereas the results were no longer significant in users. Unlike fatty acids, no heterogeneity in the risk estimates for overall NHL by sex, ethnicity, or NHL subtype was detected for any of the lipids. In stratified analyses by NHL subtype (Table 3), the inverse association of TC with NHL risk was consistent across DLBLC (ORT3 vs. T1 = 0.43 [95 % CI: 0.21–0.88]; p trend = 0.02), CLL/SLL (ORT3 vs. T1 = 0.73 [95 % CI: 0.29–1.82]; p trend < 0.01), and FL (ORT3 vs. T1 = 0.20 [95 % CI: 0.07–0.52]; p trend < 0.01), but not the association of HDL-C, which remained significant only for FL (ORT3 vs. T1 = 0.17 [95 % CI: 0.05–0.53]; p trend < 0.001).
Discussion
This study found a 60 % increase in risk for the upper tertile of total erythrocyte membrane SFA levels, whereas n−3 or n−6 PUFA levels showed no relation with NHL risk. Among serum lipids, cholesterol levels, especially TC and HDL-C, were inversely associated with NHL risk in this multiethnic population of older adults with generally normal cholesterol levels [26]. However, in light of the short follow-up time, preclinical effects cannot be excluded.
To our knowledge, this is the first study to evaluate the relation of erythrocyte membrane fatty acid composition in prediagnostic blood samples, as a surrogate, long-term measure of dietary fatty acid intake, and NHL risk. The lipid content of erythrocyte membrane phospholipids reflects the composition of fatty acid intake during the cell’s life time of about 120 days [14]. In a study of prostate cancer cases and controls, the investigators found that correlations between omega-3 fatty acid intake estimated from usual fish consumption reported in a one-year FFQ and fatty acid levels in erythrocyte membranes were high for two long-chain n−3 PUFAs (r = 0.44 for eicosapentaenoic acid [EPA] and r = 0.41 for docosahexaenoic acid [DHA]) and were slightly better than the correlations with adipose tissue levels, which reflect a time period of several years but require a more invasive collection procedure [27]. The same study also reported a similar agreement (r = 0.41 for EPA and r = 0.43 for DHA) between erythrocyte membrane and adipose tissue measures, suggesting stability over time. In contrast, baseline intake of PUFA and SFA was weakly associated and MUFA was not associated with fatty acid levels measured a decade later possibly reflecting long-term changes in dietary intake or suggesting that fatty acid levels in the erythrocyte membrane represent a different exposure measure than FFQ-based intake [28]. Given the measurement error associated with FFQs, erythrocyte membrane fatty acid composition provides a desirable measure to supplement questionnaire-based findings and further evaluate dietary fatty acid intake in relation to disease risk.
While past case–control and prospective cohort studies using pre- and postdiagnostic FFQs report significant and non-significant findings on the effect of dietary SFA intake on NHL risk [7–10], they all point to an increased risk with higher intake, which may differ by subtype [12]. For example, one report showed that a higher intake of mutagens from well-done meat was of greater etiologic importance for CLL/SLL than for DLBCL and FL. However, the current study observed no such heterogeneity in risk estimates or subtype-specific associations for SFA also present in high concentrations in meat.
In agreement with our findings, the limited number of reports on MUFAs and PUFAs is inconsistent and generally non-significant. Our results differ from a recent, small case–control study that assessed postdiagnostic, serum phospholipid composition of fatty acids, a shorter-term measure than erythrocyte membrane composition, and described significantly higher SFA and MUFA levels and lower n−3 PUFA and n−6 PUFA levels in NHL patients than controls [6]. For other cancers and diseases, n−3 PUFAs, found largely in fish oils, have been shown to be protective, while n−6 PUFAs, abundant in a typical Western diet, appear to be pro-inflammatory [2, 29]. Unlike the case–control study mentioned above [6], the current study did not observe differences in n−3 and n−6 PUFA levels between cases and controls. Varying findings across studies need to be clarified in future investigations in order to establish whether these dietary fatty acids have a pro- or anticarcinogenic effect. Interestingly, the lower total n−6 PUFA and higher total n−3 PUFA in lipid-lowering medication users suggest a favorable influence of lipid-lowering medication on erythrocyte membrane fatty acid composition not previously reported.
The inverse association of serum HDL-C with overall NHL risk agrees with reports for cancer overall [30, 31], breast cancer [32], colorectal cancer [33], and NHL in a large prospective cohort study in Finland despite notable differences in population characteristics [15]. The Finnish men were all smokers, had much higher baseline TC levels (around 240 mg/dL as compared to around 180 mg/dL in our study population), and had a longer follow-up time (a median of 14.1 vs. 2.7 years), and information on the use of lipid-lowering medications was not available. The fact that the inverse association was only observed during the first 10 years of follow-up suggests that HDL-C levels serve as a potential marker of inflammation-induced NHL development. However, this finding may indicate preclinical effects of disease rather than a causal relation between HDL-C and NHL [15, 30]. Our present analysis also detected an inverse association of TC with NHL risk, whereas the Finnish Study reported null findings for TC and non-HDL-C. While chronic inflammation has been linked with hypertriglyceridemia, we detected no relation between TG levels and NHL risk [34]. Based on these results, the association with NHL appears more consistent for HDL-C than for other lipids.
An etiologic role for HDL-C is supported by findings that use of statin medication was significantly associated with lower NHL risk among mostly older white men and women in a prospective US cohort; longer use was especially protective against NHL risk [16]. In the current study, use of lipid-lowering medication did not differ between cases and controls, but no details about length and pattern of use were known. The lack of statistical significance for the inverse associations of TC and HDL-C with NHL risk in stratified analyses among lipid-lowering medication users was due likely to the small sample size, as no heterogeneity by lipid-lowering medication use was detected. As to mechanisms of action for HDL-C, an inflammatory pathway appears likely due to the known inverse association of HDL-C with pro-inflammatory cytokines [34, 35], but HDL-C may also act through modulation of oxidative stress or insulin resistance pathways suspected to be involved in cancer development [33, 35, 36].
The current investigation had a number of limitations, in particular the short follow-up time between blood collection and NHL diagnosis. With little knowledge about the latency period of NHL subtypes, there is a possibility that our current results represent the underlying physiological changes in subclinical disease state prior to diagnosis rather than capturing the true associations with overall NHL or subtype risk. The lack of matching of cases and controls by lipid-lowering medication use may have affected the findings. The limited sample size did not allow for robust risk estimates, and multiple comparisons may have resulted in possible Type I errors. Although we detected some heterogeneity by ethnicity and sex (Table 2), the small sample size in stratified analyses does not allow firm conclusions and only suggests potential effect modifiers for future research. Nevertheless, given the known differences in the incidence rates of NHL subtypes and dietary fat intake by ethnic group and sex and the previously identified risk factors [37, 38], further investigations into ethnicity and sex difference may increase our understanding of the complex NHL etiology.
On the other hand, this study had several strengths. The total sample size was relatively large for a cancer with low incidence, and the prospective design included multiple ethnic groups from a population-based cohort that likely had a broader range of fat consumption patterns than a more homogeneous population of a single ethnic origin. The interpretation of the results, however, needs caution given the multiple subtypes with etiologic diversity [12], as well as the narrow range of measured fatty acid levels within strata. The measures from prediagnostic specimens are considered valid biomarkers and were not susceptible to change due to the disease process or treatment as FFQ-based information from case–control studies [13]. Also, the NHL diagnosis was confirmed by SEER cancer registries with excellent quality control, and information related to other important potential risk factors was available.
In summary, these findings offer supportive evidence for an adverse effect of higher erythrocyte membrane SFA levels, as a surrogate measure of dietary intake, on NHL risk with the possibility of effect modification by sex, ethnicity, or NHL subtype. Circulating TC and HDL-C levels may serve as biomarkers of inflammation associated with lymphomagenesis and warrant further investigation into their potential physiological mechanisms of action. To differentiate preclinical effects from exposures that determine disease etiology, time-stratified studies in larger populations are needed.
References
Muller AM, Ihorst G, Mertelsmann R, Engelhardt M (2005) Epidemiology of non-Hodgkin’s lymphoma (NHL): trends, geographic distribution, and etiology. Ann Hematol 84:1–12
Kelley DS (2001) Modulation of human immune and inflammatory responses by dietary fatty acids. Nutrition 17:669–673
James MJ, Gibson RA, Cleland LG (2000) Dietary polyunsaturated fatty acids and inflammatory mediator production. Am J Clin Nutr 71:343S–348S
Cross AJ, Lim U (2006) The role of dietary factors in the epidemiology of non-Hodgkin’s lymphoma. Leuk Lymphoma 47:2477–2487
Calder PC, Grimble RF (2002) Polyunsaturated fatty acids, inflammation and immunity. Eur J Clin Nutr 56(Suppl 3):S14–S19
Cvetkovic Z, Vucic V, Cvetkovic B et al (2010) Abnormal fatty acid distribution of the serum phospholipids of patients with non-Hodgkin lymphoma. Ann Hematol 89:775–782
Zhang S, Hunter DJ, Rosner BA et al (1999) Dietary fat and protein in relation to risk of non-Hodgkin’s lymphoma among women. J Natl Cancer Inst 91:1751–1758
Zheng T, Holford TR, Leaderer B et al (2004) Diet and nutrient intakes and risk of non-Hodgkin’s lymphoma in Connecticut women. Am J Epidemiol 159:454–466
Purdue MP, Bassani DG, Klar NS, Sloan M, Kreiger N (2004) Dietary factors and risk of non-Hodgkin lymphoma by histologic subtype: a case-control analysis. Cancer Epidemiol Biomark Prev 13:1665–1676
Chiu BC, Cerhan JR, Folsom AR et al (1996) Diet and risk of non-Hodgkin lymphoma in older women. JAMA 275:1315–1321
Skibola CF (2007) Obesity, diet and risk of non-Hodgkin lymphoma. Cancer Epidemiol Biomark Prev 16:392–395
Morton LM, Wang SS, Cozen W et al. (2008) Etiologic heterogeneity among non-Hodgkin lymphoma subtypes. Blood 112:5150–5160
Arab L, Akbar J (2002) Biomarkers and the measurement of fatty acids. Public Health Nutr 5:865–871
Fuhrman BJ, Barba M, Krogh V et al (2006) Erythrocyte membrane phospholipid composition as a biomarker of dietary fat. Ann Nutr Metab 50:95–102
Lim U, Gayles T, Katki HA et al (2007) Serum high-density lipoprotein cholesterol and risk of non-hodgkin lymphoma. Cancer Res 67:5569–5574
Jacobs EJ, Newton CC, Thun MJ, Gapstur SM (2011) Long-term use of cholesterol-lowering drugs and cancer incidence in a large United States cohort. Cancer Res 71:1763–1771
Kolonel LN, Henderson BE, Hankin JH et al (2000) A multiethnic cohort in Hawaii and Los Angeles: baseline characteristics. Am J Epidemiol 151:346–357
Park SY, Wilkens LR, Henning SM et al (2009) Circulating fatty acids and prostate cancer risk in a nested case-control study: the Multiethnic Cohort. Cancer Causes Control 20:211–223
Maskarinec G, Erber E, Gill J, Cozen W, Kolonel LN (2008) Overweight and obesity at different times in life as risk factors for non-Hodgkin’s lymphoma: the multiethnic cohort. Cancer Epidemiol Biomark Prev 17:196–203
Turner JJ, Morton LM, Linet MS et al (2010) InterLymph hierarchical classification of lymphoid neoplasms for epidemiologic research based on the WHO classification (2008): update and future directions. Blood 116:e90–e98
Bagga D, Capone S, Wang HJ et al (1997) Dietary modulation of omega-3/omega-6 polyunsaturated fatty acid ratios in patients with breast cancer. J Natl Cancer Inst 89:1123–1131
Friedwald WT, Levy RI, Frederickson DS (1972) Estimation of the concentration of low density lipoprotein cholesterol in plasma without use of the ultracentrifuge. Clin Chem 18:527–534
Fisher SG, Fisher RI (2004) The epidemiology of non-Hodgkin’s lymphoma. Oncogene 23:6524–6534
Mickey RM, Greenland S (1989) The impact of confounder selection criteria on effect estimation. Am J Epidemiol 129:125–137
Fortuny J, De SS, Becker N et al (2006) Statin use and risk of lymphoid neoplasms: results from the European case-control study EPILYMPH. Cancer Epidemiol Biomark Prev 15:921–925
Executive summary of the third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) (2001) JAMA 285:2486–2497
Godley PA, Campbell MK, Miller C et al (1996) Correlation between biomarkers of omega-3 fatty acid consumption and questionnaire data in African American and Caucasian United States males with and without prostatic carcinoma. Cancer Epidemiol Biomark Prev 5:115–119
Hodson L, Skeaff CM, Fielding BA (2008) Fatty acid composition of adipose tissue and blood in humans and its use as a biomarker of dietary intake. Prog Lipid Res 47:348–380
Riediger ND, Othman RA, Suh M, Moghadasian MH (2009) A systemic review of the roles of n-3 fatty acids in health and disease. J Am Diet Assoc 109:668–679
Ahn J, Lim U, Weinstein SJ et al (2009) Prediagnostic total and high-density lipoprotein cholesterol and risk of cancer. Cancer Epidemiol Biomark Prev 18:2814–2821
Jafri H, Alsheikh-Ali AA, Karas RH (2010) Baseline and on-treatment high-density lipoprotein cholesterol and the risk of cancer in randomized controlled trials of lipid-altering therapy. J Am Coll Cardiol 55:2846–2854
Furberg AS, Veierod MB, Wilsgaard T, Bernstein L, Thune I (2004) Serum high-density lipoprotein cholesterol, metabolic profile, and breast cancer risk. J Natl Cancer Inst 96:1152–1160
van Duijnhoven FJ, Bueno-de-Mesquita HB, Calligaro M et al (2011) Blood lipid and lipoprotein concentrations and colorectal cancer risk in the European Prospective Investigation into Cancer and Nutrition. Gut 60:1094–1102
Esteve E, Ricart W, Fernandez-Real JM (2005) Dyslipidemia and inflammation: an evolutionary conserved mechanism. Clin Nutr 24:16–31
McGrowder D, Riley C, Morrison EY, Gordon L (2011) The role of high-density lipoproteins in reducing the risk of vascular diseases, neurogenerative disorders, and cancer. Cholesterol 2011:496925
Kontush A, de Faria EC, Chantepie S, Chapman MJ (2005) A normotriglyceridemic, low HDL-cholesterol phenotype is characterised by elevated oxidative stress and HDL particles with attenuated antioxidative activity. Atherosclerosis 182:277–285
Erber E, Lim U, Maskarinec G, Kolonel LN (2009) Common immune-related risk factors and incident non-Hodgkin lymphoma: the multiethnic cohort. Int J Cancer 125:1440–1445
Erber E, Maskarinec G, Gill JK, Park SY, Kolonel LN (2009) Dietary patterns and the risk of non-Hodgkin lymphoma: the Multiethnic Cohort. Leuk Lymphoma 50:1269–1275
Acknowledgments
The Multiethnic Cohort Study is supported by National Cancer Institute grants R37 CA 54281 and P01 CA 033619 (PI: L Kolonel) and U01 CA 63464 (PI: B Henderson). NJO and SMC were supported by a postdoctoral fellowship on grant R25 CA 90956. The tumor registries in Hawaii and Los Angeles are supported by NCI contracts N01 PC 35137 and N01 PC 35139, respectively. Performance of the GC and serum lipid assays was supported in part by NCI award P30 CA71789. Cynthia Morrison is acknowledged for the technical performance of the lipid autoanalyzer assays.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Morimoto, Y., Conroy, S.M., Ollberding, N.J. et al. Erythrocyte membrane fatty acid composition, serum lipids, and non-Hodgkin’s lymphoma risk in a nested case–control study: the multiethnic cohort. Cancer Causes Control 23, 1693–1703 (2012). https://doi.org/10.1007/s10552-012-0048-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-012-0048-1