
Abstract
Objective
Adiposity is positively associated with advanced, metastatic, and fatal prostate cancer. Obesity-related variations in insulin-like growth factors (IGF-I and -II) and their binding proteins (IGFBPs) could underlie these associations.
Methods
We investigated associations of adiposity throughout the life course (determined retrospectively) with serum levels of IGF-I, IGF-II, IGFBP-2 and IGFBP-3 in a population-based study of 1,106 healthy men.
Results
IGF-I and IGF-II showed inverted U-shaped associations with adult body mass index (BMI) (p quadratic model = 0.04 and 0.06, respectively), although differences between quartiles with the highest and lowest IGF-I levels were small (no more than 5 ng/ml). IGFBP-2 was strongly inversely related to adult BMI (−22% change per SD increase in BMI; 95% confidence interval (CI) −24% to −19%) and waist circumference (−18% change per SD increase in waist circumference; 95% CI −20% to −15%) (p < 0.001). IGFBP-3 was positively related to BMI (63.5 ng/ml increase per SD increase in BMI; 95% CI −2.69 to 129.8, p = 0.06). IGFBP-2 and IGFBP-3 were strongly related to body shape change from childhood to adulthood, with men who gained the most weight having the lowest IGFBP-2 (9% lower per category body shape change; 95% CI −11% to −7%, p < 0.001) and the highest IGFBP-3 (50 ng/ml increase per category; 95% CI 8 to 92, p = 0.02).
Conclusions
We provide evidence that adiposity and change in body shape through the life course are related to the IGF system, with the largest effect of adiposity being to lower IGFBP-2, a possible marker of insulin resistance. The results suggest that circulating IGF-I levels may not be important mediators of the association of adiposity with aggressive prostate cancer, but the role of IGFBP-2 deserves further investigation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Although prostate cancer mortality is decreasing in industrialized countries [1, 2], it has been argued that obesity, a growing epidemic that has been linked to increased risk of several cancers in men (including prostate, colorectal, esophageal and renal cancers) [3–5], has obscured a greater decline in prostate cancer mortality [6]. This is because several studies have shown that adiposity in adulthood is associated with an increased risk of prostate cancer, particularly advanced disease [7] and prostate cancer mortality [8–17]. The evidence for localized prostate cancer is less consistent, with studies showing positive, inverse, and null associations [4, 7].
The mechanisms underlying the possible link between obesity and prostate cancer progression are not fully understood, but obesity affects many hormones and metabolic factors that may be involved in carcinogenesis. One hormone system that is modified by obesity involves insulin-like growth factors (IGF-I and -II) and their binding proteins (IGFBPs) [18–25]. IGF-I and IGF-II stimulate cell proliferation and inhibit apoptosis, and IGF-I and possibly IGF-II are associated with increased prostate cancer risk [26–28]. IGFBP-3 has been associated with a small decreased risk of prostate cancer [27], although no relationship was observed in a collaborative analysis of twelve prospective studies after adjusting for IGF-I levels [26, 27].
Studies into the relationship of adult obesity with IGFs and IGFBPs have produced mixed results. Some large cohort studies have found a non-linear association of IGF-I, with the highest levels in the mid-range of BMI and decreased IGF-I in people with the lowest and highest BMIs [18, 29–33]. Low IGF-II has been linked to increased susceptibility to weight gain [34] and associations of adiposity with IGFBP-2 are consistently inverse [19, 25, 35].
Studies reporting the association of childhood BMI with adulthood IGFs have produced intriguing results. Childhood BMI has been inversely related to adulthood IGF-I and IGFBP-3, and weakly positively associated with IGFBP-2 [19–21]. Heavy adults who were thin as children had the lowest IGFBP-2 levels and heavy children who were thin as adults had the highest IGFBP-2 [19]. These associations raise the question of whether adiposity levels at different times during the life course have particular associations with IGF-related cancers, such as prostate cancer.
Our aim was to determine whether variations in circulating IGF and IGFBP levels in relation to measures of adiposity throughout the life course could underlie observed associations of obesity with prostate cancer. To investigate this, we studied associations of adulthood body mass index (BMI), waist circumference, and change in body shape between childhood and adulthood with levels of IGFs and IGFBPs in healthy middle-aged men. Specifically, we hypothesized that if BMI and waist circumference in adulthood are positively associated with prostate cancer risk via the IGF system [4, 36, 37], then we would expect these measures of adiposity to be positively associated with IGF-I, IGF-I/IGFBP-3 molar ratio and IGF-II (because they are positively associated with prostate cancer risk) and possibly inversely associated with IGFBP-2 (because IGFBP-2 is inversely associated with insulin resistance, and insulin resistance is positively associated with prostate cancer risk) [38]. Given previous reports on associations of adiposity in childhood or change in adiposity between childhood and adulthood in relation to the IGF system [19, 20, 39, 40], we investigated whether those who gained the most weight from childhood to adulthood had the lowest IGFBP-2 levels, and the highest levels of IGF-I and IGF-II.
Methods and study participants
Study population
The study participants were controls from a case–control study nested in a population-based investigation into the detection and management of prostate cancer: the Prostate Testing for Cancer and Treatment (ProtecT) study. All participants with no evidence of prostate cancer after PSA testing, digital rectal examination, and/or biopsy were eligible to be controls in nested case–control studies of the mechanisms of prostate cancer development and progression. The study received ethical approval from Trent Multicentre Research and Ethics Committee. Detailed descriptions of ProtecT and the protocol for nested case–control selection are published elsewhere [41].
Selected sample
This analysis is nested within the ProtecT PSA-tested cohort and includes a randomly selected sample of 1,106 men who had a PSA level <3.0 ng/ml or who had a PSA between 3 and 19.9 ng/ml and a negative prostate biopsy, and who provided, with informed consent, non-fasted blood samples at the initial appointment, for research purposes.
Measures of adiposity and co-variables
At the time of recruitment, usually before the result of the PSA test was known, participants completed a self-administered diet, health and lifestyle questionnaire. Included in the questionnaire were self-reported height, weight and waist measurements. The questions were “How tall are you (feet and inches)?” and “What is your weight in light clothing (stones and pounds)?.” Participants were provided with a measuring tape to measure their waist in inches and returned both their reported measurement and the tape, on which was marked their reading, for confirmation. In addition, weight was measured by trained nurses in 93% of participants. We used weight measured to the nearest 0.1 kg (including self-reported weight in the 7% of men without a nurse-measure) and self-reported height, to compute body mass index (BMI, kg/m2), which represents general adiposity. Waist circumference was used to represent central adiposity. In a sensitivity analysis, we assessed whether associations of BMI with IGFs and IGFBPs were similar if the 7% of men with only self-reported weight were excluded.
Participants were also asked to select from nine pictograms those most closely representing their body shape at ages 10, 20, and 40 years and current age (50–69 years) (see “Appendix”, developed by Stunkard [42]). The pictograms were grouped into three categories: lean body shape (pictures 1–3), normal body shape (pictures 4–5), and overweight/obese body shape (pictures 6–9). These categories have been shown to be valid classifications of obesity and thinness in adult men [43]. The questionnaire also collected data on smoking habits, alcohol consumption, family history of prostate cancer, exercise habits, and occupation. Less than 1% of the study population comprised non-white ethnic groups and therefore we could not investigate the effect of ethnicity on associations of IGF/IGFBP levels with adiposity.
Measurement of IGFs and IGFBPs
At the prostate check clinic appointment, non-fasted blood samples were collected for research purposes using the Vacutainer® system. Samples were kept at room temperature to allow clotting and then were centrifuged at 1,640 relative centrifugal force for 20 min within 2 h of collection. Samples were transferred in a cool bag to the laboratory for processing and storage at −80°C. More than 92% of samples underwent two freeze–thaw cycles before analysis, and the remainder went through three freeze thaw cycles.
Serum samples were assayed for total IGF-I, IGF-II, IGFBP-2, and IGFBP-3 at JH’s laboratory in Bristol. Serum IGF-I, IGF-II, and IGFBP-3 were measured by in-house radioimmunoassay (RIA). Serum IGFBP-2 was measured using a one-step sandwich ELISA (Diagnostic Systems Laboratories, Webster). The molar ratio of IGF-I:IGFBP-3, which may reflect tissue bioavailability, was calculated as (0.13 × IGF-I concentration in ng/ml)/(0.025 × IGFBP-3 concentration in ng/ml). Results for all peptides were based on an average of two measures.
Statistical analysis
Pearson correlation coefficients were calculated between measures of adiposity and IGF and IGFBP levels. We used linear regression to calculate age-adjusted mean IGF and IGFBP levels by participant characteristics, and computed p-values for heterogeneity across categories using analysis of variance.
Linear regression was used to compute age-adjusted levels of IGFs and IGFBPs according to the distribution of each adiposity measure (quartiles, or categories). Linear regression models were developed to investigate the change in each growth factor level per standard deviation increase in adiposity measure. We also investigated whether there was evidence of any quadratic relationships by including BMI2 in the model, in addition to the linear term. We categorized BMI into quartiles to ensure even numbers in each group. Categories were 17.7–24.5, 24.5–26.8, 26.8–29.2, and 29.2–45.9 kg/m2. These approximate to the World Health Organization classification categories of underweight/normal, low overweight, high overweight, and obese [44].
We calculated change in body shape from childhood to adulthood by subtracting the childhood body shape (9 pictograms) from current (age 50–69) body shape (9 pictograms). We categorized the resulting difference in body shape between child- and adulthood into three groups of body shape change—lost weight or gained one pictogram (−4 to +1 pictograms change), gained a small amount of weight (+2 to +3 pictograms change), and gained a large amount of weight (+4 to +7 pictograms change). These categorizations were pragmatic and made to ensure a roughly even distribution of numbers of men in each category. We also modeled change in body shape as a continuous (ordinal) variable (from −4 to +7 category change in pictogram). We tested for interaction between current body size and change in body shape (both as categorical variables) on IGF/IGFBP levels, using likelihood ratio tests. Where there was evidence of interaction, we stratified associations by current BMI (above or below the median = 26.8 kg/m2, to ensure equal distribution of numbers of men in each stratum).
A regression model controlling for age (5 groups) was compared with models controlling for age, centre (9 centers), smoking (three categories; current smokers, ex-smokers, and never smokers) social class (three categories; working, intermediate, and managerial/professional), exercise (three groups based on weighted levels of strenuous (exercise that makes the heart beat rapidly), moderate (exercise which isn’t exhausting), and light activity (exercise which requires a minimum of effort)), current alcohol consumption (five categories; never, special occasions only, lowest, middle, and upper thirds of weekly units), duration of serum sample storage (continuous variable), and reagent assay/kit number used for the IGF/IGFBP assay. Our final fully adjusted model controlled for variables that appeared to confound at least one of the adiposity-IGF/IGFBP associations (by altering the regression coefficient by ≥10%). The lowest quartiles of adiposity measure were used as the reference category. We also fitted an additional model controlling for body shape at age 10 in addition to the fully adjusted model, to investigate whether associations of change in body shape with IGF/IGFBPs were independent of childhood weight.
The distribution of IGFBP-2 was positively skewed, and we therefore report geometric means for IGFBP-2 values across categories of adiposity, and the percent change in IGFBP-2 per standard deviation increase in adiposity measure. IGF-I, IGF-II, and IGFBP-3 were approximately normally distributed. All analyses were performed using Stata 11 (Stata Corp., College Station, TX).
Results
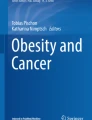
A maximum of 1,106 subjects were included in the study: slightly different numbers of subjects were included in each analysis, based on availability of IGF and covariate data (see Fig. 1). We found evidence that age-adjusted mean IGF-II, IGFBP-2, and IGFBP-3 levels among men who had an adiposity measurement and covariate data differed from those who did not have these data and who were therefore excluded from the analysis. Mean IGF-II was 884.1 ng/ml (95% CI 863.6–904.5 ng/ml) in included subjects and 819.6 ng/ml (95% CI 793.2–846.0 ng/ml) in excluded subjects. Mean IGFBP-2 was 640.2 ng/ml (95% CI 620.0–661.1 ng/ml) in included subjects and 585.5 ng/ml (95% CI 556.0–616.6 ng/ml) in excluded subjects. Mean IGFBP-3 was 4,618 ng/ml (95% CI 4,550–4,686 ng/ml) in included subjects and 4,407 ng/ml (95% CI 4,315–4,499 ng/ml) in excluded subjects. Baseline characteristics of participants are shown in Table 1. The mean age was 61.9 years at the time of blood sampling.

Flow chart of subjects included in the analysis. Of those with an IGF assay result, fewer had had the measures of adiposity and complete covariate data. Percentages shown are the percentage of the total number of subjects with that particular IGF/IGFBP assay. *complete data for multivariable analysis includes measure of adiposity (BMI, waist circumference, or body shape change), age, centre, duration of sample storage, assay kit number, alcohol, smoking, and exercise
BMI and waist circumference were strongly positively correlated (r = 0.79, p < 0.0001). BMI and waist circumference were negatively correlated with ln IGFBP-2 (r = −0.48, p < 0.0001 and r = −0.36, p < 0.0001, respectively) but not correlated with IGF-I, IGF-II, or IGFBP-3 (r ≤ 0.08). IGF-I was positively correlated with IGF-II (r = 0.28, p < 0.0001) and IGFBP-3 (r = 0.48, p < 0.0001), and negatively correlated with ln IGFBP-2 (r = −0.21, p < 0.0001). IGF-II was negatively correlated with ln IGFBP-2 (r = −0.23, p < 0.0001) and positively correlated with IGFBP-3 (r = 0.56, p < 0.0001). There was a weak negative correlation between IGF-II and IGF-I:IGFBP-3 M ratio (r = −0.11, p = 0.001). ln IGFBP-2 and IGFBP-3 were negatively correlated (r = −0.27, p < 0.0001).
Age-adjusted mean levels of IGFs and IGFBPs according to participant characteristics are shown in Table 2. IGF-I, IGF-II, IGFBP-2, and IGFBP-3 were all strongly related to age, with IGF-I, IGF-II, and IGFBP-3 decreasing with age, and IGFBP-2 increasing with age. Body shape was inversely related to IGFBP-2 at all ages, and inversely related to IGFBP-3 levels at age 20 and 40, but positively related to IGFBP-3 at current age.
Age- and fully adjusted means (IGF-I, IGF-II, and IGFBP-3) and geometric means (IGFBP-2) and the molar ratio of IGF-I/IGFBP-3 in relation to adulthood BMI are shown in Table 3. IGF-I and IGF-II showed non-linear associations with BMI (p for quadratic model = 0.04 and 0.06, respectively), being lowest at both low and high BMIs and higher for the mid-distribution of BMI. Adjustment for potential confounders did not materially alter the results. Adjusting for IGFBP-3 levels weakened the curved relationship, with the adjusted mean (95% CI) IGF-I in BMI quartiles 1–4 of 164.6 ng/ml (158.0, 171.2), 163.7 ng/ml (157.4, 170.1), 162.8 ng/ml (156.1, 169.5), and 158.7 ng/ml (152.1, 165.3), respectively (p for quadratic model = 0.47, p for linear trend = 0.21). IGFBP-2 was strongly inversely related to BMI (decrease of 22% in IGFBP-2 per standard deviation increase in BMI (95% CI: decrease of 19% to 24%), p < 0.001 for both linear and quadratic models). This corresponds to a 0.41 standard deviation decrease in ln IGFBP-2 for a standard deviation increase in BMI. IGFBP-3 was positively related to BMI (p = 0.06 for linear trend), with a 63.5 ng/ml (corresponding to a 0.06 standard deviation) increase in IGFBP-3 per standard deviation increase in BMI. The molar ratio of IGF-I/IGFBP-3 was not related to BMI. Adjustment for potential confounders attenuated the effect estimate for IGFBP-3 but the large positive association remained in the fully adjusted model.
Age- and fully adjusted means (IGF-I, IGF-II and IGFBP-3) and geometric means (IGFBP-2) and molar ratio of IGF-I/IGFBP-3 in relation to adulthood waist circumference are shown in Table 4. The associations were similar to those with BMI, but with smaller effects.
Table 5 shows the age- and fully adjusted means (IGF-I, IGF-II and IGFBP-3) and geometric means (IGFBP-2) and molar ratio of IGF-I/IGFBP-3 in relation to change in body shape between childhood and adulthood. IGF-I, IGF-II, and IGF-I/IGFBP-3 molar ratio were unrelated to body shape change (p = 0.97, 0.25, 0.15, respectively). IGFBP-2 was strongly inversely related to body shape change, so that men who gained the most weight had the lowest IGFBP-2, and men who lost weight or gained very little weight had the highest IGFBP-2. In a regression model, IGFBP-2 decreased by 9% per one pictogram increase in body shape from childhood to adulthood (95% CI: decrease of 7% to 11%), (p < 0.001). The association was stronger in a model controlling for body shape at age 10. The relationship also appeared to be independent of current body shape: controlling for current body shape; in line with this, men who were obese throughout life had mean IGFBP-2 levels of 526.1 ng/ml (95% CI: 390.6, 708.5), while men who were lean in childhood and obese as adults had the lowest mean IGFBP-2, at 468.0 ng/ml (95% CI: 439.0, 498.9), and men who had a normal body shape in childhood and were obese as adults had mean IGFBP-2 levels, at 515.1 ng/ml (95% CI:424.0, 625.7), that were intermediate between the two extreme body shape change categories.
IGFBP-3 was positively related to body shape change, with men gaining the most weight having the highest IGFBP-3, and men who lost weight or gained very little weight having the lowest IGFBP-3. IGFBP-3 increased 50.0 ng/ml per one pictogram increase in body shape (p = 0.02).
We found evidence of an interaction between current BMI and change in body shape for IGFBP-2 (p for interaction = 0.06) and IGFBP-3 (p for interaction = 0.05). We therefore stratified the fully adjusted analysis by current BMI, dichotomized into below or above median. For men with a current BMI below the median, IGFBP-2 decreased by 6.5% and IGFBP-3 increased by 76.8 ng/ml per one pictogram increase in body shape change. For men with a current BMI above median, IGFBP-2 decreased by 2.4% and IGFBP-3 decreased by 19.4 ng/ml per one pictogram increase in body shape. However, this result was not seen for IGFBP-2 when we stratified BMI using the World Health Organization cut-point of 25 kg/m2 (IGFBP-2 p for interaction = 0.7) so this interaction may have arisen by chance. The sensitivity analyses excluding the 7% of men with only self-reported weight produced no difference in the results.
Discussion
This study confirms an inverted U-shaped association of IGF-I and IGF-II with adulthood BMI. The highest levels of IGF-I and IGF-II were in the mid-range of the BMI distribution, and there were lower levels in the lowest and highest BMI categories. The relationship of IGFBP-2 (a potential marker of insulin sensitivity) with adulthood BMI and waist circumference was strongly inverse. Men who gained a large amount of weight between childhood and adulthood (i.e., an increase of +4 to +7 body shape pictograms) had the lowest circulating levels of IGFBP-2 and the highest levels of IGFBP-3. The relationship between body shape and IGFBP-3 was inverse in early-mid adulthood and then became positive in later adulthood.
The non-linear association of IGF-I with BMI has been shown in six other large cohort studies, including samples with men and women [18, 29–33]. The inverse relationship between IGFBP-2 and adiposity is in line with previous results [19, 25, 35]. The associations of IGFBP-2 and IGFBP-3 with weight gain are new findings. Previous studies into the relationship of adult obesity with IGFs and IGFBPs have produced mixed results. There are reports of inverse [22, 23, 40, 45–47], positive [48] and null [19, 21, 24, 25, 35, 49–53] associations for IGF-I; inverse [23], positive [19], and null [24, 25, 46] associations for IGF-II; and inverse [48] positive [19, 53], and null [22–25, 35, 49, 54] associations for IGFBP-3.
Strengths and limitations
This is the first study to investigate four measures of the IGF system (IGF-I, IGF-II, IGFBP-2, and IGFBP-3) in relation to adiposity in a large cohort of healthy middle-aged men, selected from the UK general population according to a standard recruitment protocol. Serum samples were assayed using validated robust in-house assays.
There are some limitations to the study. It was conducted in middle-aged men and, therefore, may not be generalized to younger men or to women. There were small numbers of men who reported being overweight or obese in childhood (measured by pictogram choice), and the body shape pictograms used have only been validated in adults over 18 years [43]. However, instead of using actual reported childhood body size in our analyses, we looked at how men perceived their change in body shape from childhood to adulthood. Change in body shape in individuals may be less prone to error compared with recalled actual body shape or other measures of adiposity. Although there was a small difference in IGF-II, IGFBP-2, and IGFBP-3 levels between subjects included and excluded from the analysis, we do not anticipate that this difference would likely affect our conclusions, because it is unlikely that associations of IGFs with adiposity would differ among those who were and were not in the analysis. We did not investigate prostate cancer as an outcome in this study and therefore can only speculate about the role of adiposity-related changes in IGFs and IGFBPs and cancer risk.
Biological roles of IGFs and IGFBPs in prostate cancer
The IGFBPs regulate transport of IGFs to cellular receptors and have been shown to have both inhibitory and stimulatory effects on cell proliferation and migration [55]. IGFBP-3 is the most abundant binding protein with IGF-dependent and IGF-independent inhibitory effects on cell growth. Our previous meta-analysis of published retrospective and prospective studies of IGFs/IGFBPs and prostate cancer found a positive association of IGF-I with prostate cancer, and a negative association of IGFBP-3 with prostate cancer [27]. For IGF-II, IGFBP-2, and IGF-I:IGFBP-3 M ratio, there were positive but weaker associations with prostate cancer risk [27]. A pooled analysis of twelve prospective studies investigating the association of IGFs and IGFBPs with subsequent prostate cancer risk found a similar relationship for IGF-I, but no association of IGF-II, IGFBP-2, or IGFBP-3 (after adjusting the IGFBP-3 model for IGF-I) with risk of prostate cancer [26]. The weak positive association of IGFBP-2 with prostate cancer is not consistent with IGFBP-2 being a marker of insulin sensitivity, which would be anticipated to be inversely associated with prostate cancer. It is important to note, however, that the findings for IGFBP-2 were based on three case–control studies and two cohort studies and that interpretation of these case–control studies may be affected by reverse causality. IGFBP-2 levels have been shown to fall following surgical removal of the prostate [56], suggesting that IGFBP-2 in men with prostate cancer may be a tumor marker (i.e., raised levels may be a secondary tumor effect). Other effects of IGFBP-2 at the cellular level have been noted, for example regulation of the PTEN tumor suppressor gene [57].
IGF-I synthesis by the liver is primarily controlled by pituitary growth hormone (GH) and by nutritional stimuli [58]. The biological activities of the IGFs are modulated by IGFBPs which regulate transport of IGFs to cellular receptors, protect them from degradation, and regulate the interaction between IGFs and the IGF receptor [59]. IGFBPs also have direct effects on cell proliferation, survival, motility and adhesion, independent of their IGF-binding properties [55]. Chronic fasting results in low production of insulin, causing a reduction in hepatic GH receptor levels, resulting in GH resistance and reduced synthesis and blood levels of IGF-I [5]. Excess body weight can lead to prolonged hyperinsulinemia, which reduces the production of IGFBP-2, possibly resulting in increases in the level of bioavailable IGF-I. This may therefore be the mechanism by which adiposity could increase cancer risk, via the insulin-IGFBP-2 pathway. Alternatively, lower IGFBP-2 levels may be acting as a marker of increased insulin resistance. With increasing obesity, there is a fall in serum IGF-I levels, probably consequent to impaired hepatocyte function due to development of a fatty-liver and eventually non-alcoholic steatohepatitis (liver disease) [60]. However, the fall in absolute IGF-I levels is very small compared to the relatively large fall in IGFBP-2 levels: the fall in IGF-I, from BMI quartile 3 (which had the highest IGF-I) to BMI quartile 1, was only 5 ng/ml (approximately 10%), whereas IGFBP-2 decreased by 22% per SD increase in BMI. The observed positive associations of increased adiposity with prostate cancer progression and fatality could therefore result from increased tissue availability of IGF-I due to the relatively large decrease in IGFBP-2, despite the small decrease in absolute IGF-I level. However, given the limited evidence from few prospective studies investigating associations of IGFBP-2 with prostate cancer progression [26, 27], further research on the role of IGFBP-2 is required.
Conclusion
We provide evidence that adiposity and change in body shape from childhood to adulthood are related to the IGF system. Specifically, we have found evidence of non-linear associations of IGF-I and IGF-II with general adiposity (measured by BMI) in middle-aged men, with highest levels of these IGFs in the mid-range of adiposity. The change in IGF-I level between BMI quartile 1 and BMI quartile 3 (which had the highest IGF-I) was only 5 ng/ml. Our previously published meta-analysis [27] showed that there was a 21% increased risk of prostate cancer for a standard deviation increase in IGF-I (which in this group of subjects equals 54.9 ng/ml). Therefore, there is unlikely to be a meaningful change in risk of prostate cancer as a result of BMI-related changes in IGF-I. Serum IGFBP-2 was strongly inversely related to general (BMI) and central adiposity (waist circumference), decreasing by 22% per SD increase in BMI. Men who gained a large amount of weight between childhood and adulthood had the lowest IGFBP-2 and the highest IGFBP-3.
We hypothesize that low IGFBP-2 levels (likely resulting from hyperinsulinaemia in obese individuals) may be one mechanism leading to increased risk of prostate cancer progression in overweight or obese men, and in men who had lean or normal body shapes as children and became obese in adulthood. Although current evidence from only a few prospective studies does not support an association of IGFBP-2 with prostate cancer progression [26, 27], there is evidence from clinical studies of patients with prostate cancer indicating that IGFBP-2 is associated with patient survival [61] with loss of tumor expression of PTEN [62] and with failure of hormone therapy [63]. In addition, there is considerable experimental evidence linking IGFBP-2 with prostate cancer progression [64]. The results suggest that circulating IGF-I levels may not be an important mediator of the association of adiposity with aggressive prostate cancer.
References
Parkin DM, Bray F, Ferlay J, Pisani P (2002) Global Cancer Statistics, 2002. CA Cancer J Clin 55(2):74–108
Baade PD, Coory MD, Aitken JF (2004) International trends in prostate-cancer mortality: the decrease is continuing and spreading. Cancer Causes Control 15:237–241
World Cancer Research Fund: Food, Nutrition, Physical Activity and the Prevention of Cancer: a Global Perspective (2008) 2 edn
Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M (2008) Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet 371(9612):569–578
Calle EE, Kaaks R (2004) Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Cancer 4(8):579–591
Fesinmeyer MD, Gulati R, Zeliadt S, Weiss N, Kristal AR, Etzioni R (2009) Effect of population trends in body mass index on prostate cancer incidence and mortality in the United States. Cancer Epidemiol Biomarkers Prev 18(3):808–815
MacInnis R, English D (2006) Body size and composition and prostate cancer risk: systematic review and meta-regression analysis. Cancer Causes Control 17(8):989–1003
Wright ME, Chang S-C, Schatzkin A et al (2007) Prospective study of adiposity and weight change in relation to prostate cancer incidence and mortality. Cancer 109:675–684
Gong ZH, Neuhouser ML, Goodman PJ et al (2006) Obesity, diabetes, and risk of prostate cancer: results from the prostate cancer prevention trial. Cancer Epidemiol Biomarkers Prev 15(10):1977–1983
Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ (2003) Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med 348(17):1625–1638
Andersson SO, Wolk A, Bergstrom R et al (1997) Body size and prostate cancer: a 20-year follow-up study among 135006 Swedish construction workers. J Natl Cancer Inst 89(5):385–389
Snowdon DA, Phillips RL, Choi WARR (1984) Diet, obesity, and risk of fatal prostate cancer. Am J Epidemiol 120(2):244–250
Giovannucci E, Rimm EB, Stampfer MJ, Colditz GA, Willett WC (1997) Height, body weight, and risk of prostate cancer. Cancer Epidemiol Biomarkers Prev 6(8):557–563
Efstathiou JA, Bae K, Shipley WU et al (2007) Obesity and mortality in men with locally advanced prostate cancer. Cancer 110:2691–2699
Rodriguez C, Freedland SJ, Deka A et al (2007) Body mass index, weight change, and risk of prostate cancer in the cancer prevention study II nutrition cohort. Cancer Epidemiol Biomarkers Prev 16(1):63–69
Ma J, Li H, Giovannucci E et al (2008) Prediagnostic body-mass index, plasma C-peptide concentration, and prostate cancer-specific mortality in men with prostate cancer: a long-term survival analysis. Lancet Oncol 9(11):1039–1047
Giovannucci E, Michaud D (2007) The role of obesity and related metabolic disturbances in cancers of the colon, prostate, and pancreas. Gastroenterology 132:2208–2225
Lukanova A, Soderberg S, Stattin P et al (2002) Nonlinear relationship of insulin-like growth factor (IGF)-I and IGF-I/IGF-binding protein-3 ratio with indices of adiposity and plasma insulin concentrations (Sweden). Cancer Causes Control 13(6):509–516
Martin RM, Holly JMP, Davey Smith G, Gunnell D (2006) Associations of adiposity from childhood into adulthood with insulin resistance and the insulin-like growth factor system: 65 year follow-up of the Boyd Orr Cohort. J Clin Endocrinol Metab 91:3287–3295
Ben-Shlomo Y, Holly J, McCarthy A et al (2003) An investigation of fetal, postnatal and childhood growth with insulin-like growth factor I and binding protein 3 in adulthood. Clin Endocrinol 59(3):366–373
Kajantie E, Fall CHD, Seppala M et al (2003) Serum insulin-like growth factor (IGF)-I and IGF-binding protein-1 in elderly people: relationships with cardiovascular risk factors, body composition, size at birth, and childhood growth. J Clin Endocrinol Metab 88(3):1059–1065
Gapstur SM, Kopp P, Chiu BCH, Gann PH, Colangelo LA, Liu K (2004) Longitudinal associations of age, anthropometric and lifestyle factors with serum total insulin-like growth factor-I and IGF binding protein-3 levels in black and white men: the CARDIA male hormone study. Cancer Epidemiol Biomarkers Prev 13(12):2208–2216
Chang S, Wu XF, Yu H, Spitz MR (2002) Plasma concentrations of insulin-like growth factors among healthy adult men and postmenopausal women: associations with body composition, lifestyle, and reproductive factors. Cancer Epidemiol Biomarkers Prev 11(8):758–766
Benbassat CA, Maki KC, Unterman TG (1997) Circulating levels of insulin-like growth factor (IGF) binding protein-1 and -3 in aging men: relationships to insulin, glucose, IGF, and dehydroepiandrosterone sulfate levels and anthropometric measures. J Clin Endocrinol Metab 82(5):1484–1491
Gunnell D, Oliver SE, Donovan JL et al (2004) Do height-related variations in insulin-like growth factors underlie the associations of stature with adult chronic disease? J Clin Endocrinol Metab 89(1):213–218
Roddam AW, Allen NE, Appleby P et al (2008) Insulin-like growth factors, their binding proteins, and prostate cancer risk: analysis of individual patient data from 12 prospective studies. Ann Intern Med 149(7):461–471
Rowlands M, Gunnell D, Harris R, Vatten LJ, Holly JMP, Martin RM (2009) Circulating insulin-like growth factor peptides and prostate cancer risk: a systematic review and meta-analysis. Int J Cancer 124(10):2416–2429
Oliver SE, Gunnell D, Donovan J et al (2004) Screen-detected prostate cancer and the insulin-like growth factor axis: results of a population-based case-control study. Int J Cancer 108:887–892
Schneider HJ, Saller B, Klotsche J et al (2006) Opposite associations of age-dependent insulin-like growth factor-I standard deviation scores with nutritional state in normal weight and obese subjects. EUR 154(5):699–706
Allen NE, Appleby PN, Kaaks R, Rinaldi S, Davey GK, Key TJ (2003) Lifestyle determinants of serum insulin-like growth-factor-I (IGF-I), C-peptide and hormone binding protein levels in British women. Cancer Causes Control 14:65–74
Bezemer ID, Rinaldi S, Dossus L et al (2005) C-peptide, IGF-I, sex-steroid hormones and adiposity: a cross-sectional study in healthy women within the European Prospective Investigation into Cancer and Nutrition (EPIC). Cancer Causes Control 16(5):561–572
Gram IT, Norat T, Rinaldi S et al (2006) Body mass index, waist circumference and waist-hip ratio and serum levels of IGF-I and IGFBP-3 in European women. Int J Obes 30(11):1623–1631
Fowke J, Matthews C, Yu H et al. (2009) Racial differences in the association between body mass index (BMI) and serum IGF-1, IGF-2, and IGFBP-3. Endocr Relat Cancer: ERC-09
Sandhu MS, Gibson JM, Heald AH, Dunger DB, Wareham NJ (2003) Low circulating IGF-II concentrations predict weight gain and obesity in humans. Diabetes 52(6):1403–1408
van den Beld AW, Blum WF, Pols HA, Grobbee DE, Lamberts SW (2003) Serum insulin-like growth factor binding protein-2 levels as an indicator of functional ability in elderly men. Eur J Endocrinol 148(6):627–634
MacInnis R, English D (2006) Body size and composition and prostate cancer risk: systematic review and meta-regression analysis. Cancer Causes Control 17(8):989–1003
Kristal AR, Gong Z (2007) Obesity and prostate cancer mortality. Future Oncol 3(5):557–567
Albanes D, Weinstein SJ, Wright ME et al (2009) Serum insulin, glucose, indices of insulin resistance, and risk of prostate cancer. J Natl Cancer Inst 101(18):1272–1279
Hernandez BY, Park SY, Wilkens LR, Henderson BE, Kolonel LN (2009) Relationship of body mass, height, and weight gain to prostate cancer risk in the multiethnic cohort. Cancer Epidemiol Biomarkers Prev 18(9):2413–2421
Kajantie E, Fall CHD, Seppala M et al (2003) Serum insulin-like growth factor (IGF)-I and IGF-binding protein-1 in elderly people: relationships with cardiovascular risk factors, body composition, size at birth, and childhood growth. J Clin Endocrinol Metab 88(3):1059–1065
Zuccolo L, Harris R, Gunnell D et al (2008) Height and prostate cancer risk: a large nested case-control study (protect) and meta-analysis. Cancer Epidemiol Biomarkers Prev 17(9):2325–2336
Stunkard AJ, Sorensen T, Schulsinger F (1983) Use of a Danish adoption register for the study of obesity and thinness. The genetics of neurological and psychiatric disorders. Raven Press, New York, pp 115–120
Bulik CM, Wade TD, Heath AC, Martin NG, Stunkard AJ, Eaves LJ (2001) Relating body mass index to figural stimuli: population-based normative data for Caucasians. Int J Obes 25:1517–1524
Expert Panel on Identification EaToOaOiA (1998) Executive summary of the clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. Arch Intern Med 158(17):1855–1867
Tricoli JV, Winter DL, Hanlon AL et al (1999) Racial differences in insulin-like growth factor binding protein-3 in men at increased risk of prostate cancer. Urology 54(1):178–182
Cruickshank JK, Heald AH, Anderson S et al (2001) Epidemiology of the insulin-like growth factor system in three ethnic groups. Am J Epidemiol 154(6):504–513
Landin-Wilhelmsen K, Wilhelmsen L, Lappast G et al (1994) Serum insulin-like growth factor I in a random population sample of men and women: relation to age, sex, smoking habits, coffee consumption and physical activity, blood pressure and concentrations of plasma lipids, fibrinogen, parathyroid hormone and osteocalcin. Clin Endocrinol 41(3):351–357
Laughlin GA, Barrett-Connor E, Criqui MH, Kritz-Silverstein D (2004) The prospective association of serum insulin-like growth factor I (IGF-I) and IGF-binding protein-1 levels with all cause and cardiovascular disease mortality in older adults: the rancho bernardo study. J Clin Endocrinol Metab 89(1):114–120
DeLellis K, Rinaldi S, Kaaks RJ, Kolonel LN, Henderson B, Le ML (2004) Dietary and lifestyle correlates of plasma insulin-like growth factor-I (IGF-I) and IGF binding protein-3 (IGFBP-3): the multiethnic cohort. Cancer Epidemiol Biomarkers Prev 13(9):1444–1451
O’Connor KG, Tobin JD, Harman SM et al (1998) Serum levels of insulin-like growth factor-I are related to age and not to body composition in healthy women and men. J Gerontol A Biol Sci Med Sci 53A(3):M176–M182
Langlois JA, Rosen CJ, Visser M et al (1998) Association between insulin-like growth factor i and bone mineral density in older women and men: the Framingham heart study. J Clin Endocrinol Metab 83(12):4257–4262
Mucci LA, Tamimi R, Lagiou P et al (2001) Are dietary influences on the risk of prostate cancer mediated through the insulin-like growth factor system? BJU Int 87(9):814–820
Probst-Hensch NM, Wang H, Goh VHH, Seow A, Lee H-P, Yu MC (2003) Determinants of circulating insulin-like growth factor I and insulin-like growth factor binding protein 3 concentrations in a cohort of Singapore men and women. Cancer Epidemiol Biomarkers Prev 12(8):739–746
Tricoli JV, Winter DL, Hanlon AL et al (1999) Racial differences in insulin-like growth factor binding protein-3 in men at increased risk of prostate cancer. Urology 54(1):178–182
Holly J, Perks C (2006) The role of insulin-like growth factor binding proteins. Neuroendocrinology 83:154–160
Shariat SF, Lamb DJ, Kattan MW et al (2002) Association of preoperative plasma levels of insulin-like growth factor I and insulin-like growth factor binding proteins-2 and -3 with prostate cancer invasion, progression, and metastasis. J Clin Oncol 20(3):833–841
Perks C, Vernon EG, Rosendahl AH, Tonge D, Holly JMP (2007) IGF-II and IGFBP-2 differentially regulate PTEN in human breast cancer cells. Oncogene 26:5966–5972
Thissen J-P, Ketelslegers J-M, Underwood LE (1994) Nutritional regulation of the insulin-like growth factors. Endocr Rev 15(1):80–101
Yu H, Rohan T (2000) Role of the insulin-like growth factor family in cancer development and progression. J Natl Cancer Inst 92(18):1472–1489
Garcia-Galiano D, Sanchez-Garrido MA, Espejo I et al (2007) IL-6 and IGF-1 are independent prognostic factors of liver steatosis and non-alcoholic steatohepatitis in morbidly obese patients. Obes Surg 17(4):493–503
Inman BA, Harel F, Audet JF et al (2005) Insulin-like growth factor binding protein 2: an androgen-dependent predictor of prostate cancer survival. Eur Urol 47(5):695–702
Mehrian-Shai R, Chen CD, Shi T et al (2007) Insulin growth factor-binding protein 2 is a candidate biomarker for PTEN status and PI3 K/Akt pathway activation in glioblastoma and prostate cancer. Proc Nat Acad Sci 104(13):5563–5568
Bubendorf L, Kolmer M, Kononen J et al (1999) Hormone therapy failure in human prostate cancer: analysis by complementary DNA and tissue microarrays. J Natl Cancer Inst 91(20):1758–1764
Degraff DJ, Aguiar AA, Sikes RA (2009) Disease evidence for IGFBP-2 as a key player in prostate cancer progression and development of osteosclerotic lesions. Am J Transl Res 1(2):115–130
Rose D, O’Reilly K (1998) The ESRC review of government social classifications. Office for national statistics & economic and social research council
Acknowledgments
This work was supported by Cancer Research UK project grant C18281/A7062. The ProtecT study is funded by the UK Health Technology Assessment Programme of the NIHR, HTA 96/20/99; ISRCTN20141297. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Department of Health. The authors would like to acknowledge the support of the National Cancer Research Institute (NCRI) formed by the Department of Health, the Medical Research Council and Cancer Research UK. The NCRI provided funding through ProMPT (Prostate Mechanisms of Progression and Treatment) and this support is gratefully acknowledged. The prostate bio-repository received funding from the Cambridge NIHR Comprehensive Biomedical Research Centre. The authors would like to acknowledge the tremendous contribution of all members of the ProtecT study research group, and especially the following who were involved in this research: Prasad Bollina, Sue Bonnington, Lynne Bradshaw, James Catto, Debbie Cooper, Michael Davis, Liz Down, Andrew Doble, Alan Doherty, Garrett Durkan, Emma Elliott, David Gillatt, Pippa Herbert, Peter Holding, Joanne Howson, Mandy Jones, Roger Kockelbergh, Howard Kynaston, Athene Lane, Teresa Lennon, Norma Lyons, Hing Leung, Malcolm Mason, Hilary Moody, Philip Powell, Alan Paul, Stephen Prescott, Derek Rosario, Patricia O’Sullivan, Pauline Thompson, Lynne Bradshaw, Sarah Tidball. They would also like to thank the men who participated in this study. Val Laundy, Semih Dogan, Li Zeng, Ola Wojtowicz, and Kalina Zdunek performed the IGF assays.
Author information
Authors and Affiliations
Corresponding author
Appendix: Body shape pictograms and associated questions
Appendix: Body shape pictograms and associated questions

Rights and permissions
About this article
Cite this article
Rowlands, MA., Holly, J.M.P., Gunnell, D. et al. The relation between adiposity throughout the life course and variation in IGFs and IGFBPs: evidence from the ProtecT (Prostate testing for cancer and Treatment) study. Cancer Causes Control 21, 1829–1842 (2010). https://doi.org/10.1007/s10552-010-9610-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-010-9610-x