
Abstract
Purpose
Breast cancer (BC) is the most commonly diagnosed cancer and the second leading cause of cancer-related death among women. Given the availability of approved therapies and abundance of phase II and III clinical trials, historically few BC patients have been referred for consideration of participation on a phase I trial. We were interested in determining whether clinical benefit rates differed in patients with BC from other patients enrolled in phase I trials.
Methods
We performed a retrospective analysis of all Cancer Therapy Evaluation Program (CTEP) sponsored phase I trials from 1993 to 2012. We report an analysis of demographic variables, rates of response to treatment, grade 4 toxicities, and treatment-related deaths.
Results
De-identified data from 8087 patients were analyzed, with 1,376 having a diagnosis of BC. The median time from initial cancer diagnosis to enrollment in a CTEP-sponsored phase I clinical trial was 614 days for all patients. Breast cancer patients were enrolled on average 790 days after initial diagnosis, while non-BC patients had a median enrollment time of 582 days (p < 0.001). Breast cancer patients had more clinical responses than non-BC patients (18.3% vs. 4.3%, respectively). Along with the higher rate of response, BC patients remained on phase I trials longer than non-BC patients with a median of 70 days while the latter were on trial for a median of 57 days. The overall rate of death related to the treatment drugs was 0.47%.
Conclusions
Our data confirm our hypothesis that when compared to a general population of patients with cancer enrolled on phase I clinical trials, BC patients tend to derive clinical benefit from these therapies with similar toxicity profile. This evidence further supports enrollment of BC patients on phase I trials.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Phase I clinical trials are a critical component of the long road of innovative oncology drug development. Traditionally, the primary endpoint of these trials has been to determine the safety, tolerability, and recommended phase 2 dose (RP2D) of novel agents for further studies. As a result, the expectation of direct clinical benefit to patients participating on these trials may be perceived as being relatively low, whereas the risks and possible harms potentially substantial, given the early phase development of the drugs. Low response rates of 4–6% have historically been reported [1,2,3,4,5,6,7,8,9]. Although recent phase I studies have reported higher response rates [10, 11] and relatively long progression free survival [12,13,14], phase I studies are still typically reserved for patients who lack other treatment options.
Breast cancer (BC) is the most commonly diagnosed cancer and the second leading cause of cancer-related death among women. The 5-year relative survival for stage IV BC is 26.9% [15] and overall survival (OS) has been reported between 19 and 34 months [16,17,18,19]. Recent drug approvals by the Food and Drug Administration (FDA) have significantly improved the OS to 56.5 months in some subtypes of BC [20].
The representation of cancer patients in phase I trials has been historically low. While only 3–5% of the United States adult cancer patients are enrolled in clinical trials [21, 22] the number of those participating in phase I trials is even lower. Many factors are associated with this fact and include the misconception that phase I trials are a last-ditch effort, misinformation regarding the possibility of receiving placebo, or inconvenience of additional visits and tests. It is also our experience that patients with BC are referred to phase I trials at a late point in time on their disease natural history, possibly also related to the availability of a larger number of active standard treatment options. At that point, life expectancy, performance status, and organ function frequently preclude enrollment. In addition, in the recent years, early phase clinical trials mostly testing targeted agents or immunotherapeutic approaches presented new challenges to design [23], including limitations to the number of previous treatment lines of therapy for eligibility.
In this study, we sought to analyze a cohort of patients enrolled on phase I clinical trials over a 20-year period and to determine whether patients with BC derive similar clinical benefit and toxicities from phase I trials when compared to enrolled patients with other malignancies.
Methods
Patient eligibility
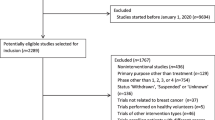
All non-pediatric patients enrolled in phase I oncology trials sponsored by the Cancer Therapy Evaluation Program (CTEP) between 1993 and 2012 were eligible for this study. Protocols including hematologic and solid tumor malignancies were included and consisted of both single and multi-agent investigational targets. These clinical trials were performed at the National Institutes of Health Clinical Center and other National Cancer Institute-sponsored academic centers within the United States.
All protocols were approved by the Protocol and Information Office (PIO) of CTEP prior to enrollment. Regular quality assurance audits were performed by the Clinical Trials Monitoring Service (CTMS) and CTEP. Data were prospectively maintained by individual trial investigators and staff of CTEP. These data were then electronically delivered to the CTMS on a bi-weekly basis for the duration of each trial. The electronic database is maintained by the CTMS which was managed by Theradex (Princeton, NJ, USA) at the time of data analysis.
Pre-enrollment characteristics
Information regarding pre-enrollment characteristics including age, sex, race, performance status (PS), hemoglobin, albumin, and primary disease site were recorded. The PS at enrollment was measured using either the Eastern Cooperative Oncology Group (ECOG) score or the Karnofsky score as specified by each protocol. For analysis, PS measured using the Karnofsky scale was directly converted to the ECOG scoring modality [24].
For the purpose of this study, patients were categorized into breast (BC) and non-breast cancer (non-BC) by using primary disease site. Data pertaining to diagnostic timelines as well as the total amount of prior medical therapies were also obtained.
Study outcomes and tolerability
Outcomes of treatment, including disease response, treatment duration, and data regarding tolerability were evaluated. We sought to analyze the beneficial effects of investigational agents for BC versus non-BC. Response to treatment was assessed using guidelines according to the World Health Organization criteria, Response Evaluation Criteria in Solid Tumors (RECIST) guidelines, or the revised RECIST guidelines with approval from the PIO of CTEP at the time of protocol submission. The response rate in the initial trials was assessed by WHO criteria and more recent trials by RECIST or modified RECIST criteria. The disease response to treatment was categorized as complete response, partial response, less than partial response, stable disease, or progressive disease. For the purposes of our analyses, less than partial response was categorized as stable disease.
The tolerability of investigational agents among BC versus non-BC patients was of interest. Data pertinent to grade 4 and 5 toxicities were included in our study. The attribution of adverse events (AE) was determined by pre-defined criteria outlined by the Common Terminology Criteria for Adverse Events (CTCAE) from CTEP. Attribution of each adverse event was designated as the following: definite, probable, possible, unlikely, and unrelated. For purposes of these analyses, definite, probable, possible, were grouped as related whereas all others were grouped as unrelated. Treatment-related deaths were defined as deaths determined to be at least possibly related to treatment (possible, probable, or definitive). Information regarding overall recovery status and time to recovery were also obtained. We were unable to assess survival benefit as survival data was not recorded for all patients.
Statistical methods
Descriptive statistics were provided to summarize the data. Violin plots were used for visualization of some of the continuous variables. Wilcoxon rank sum test was performed to compare continuous variables while Chi square test or Fisher’s exact test was used to compare categorical variables between two groups. p < 0.05 is considered statistically significant.
Results
Patient characteristics
De-identified data from 8087 patients enrolled in CTEP-sponsored phase I clinical trials between 1993 and 2012 were analyzed. Patient demographic characteristics at phase I clinical trial enrollment are described in detail in Table 1. Of the total number of patients, 1376 were diagnosed with BC. Breast cancer patients had a median age of 52 years (range 23–87 years) which was younger than non-BC patients with a median age of 58 years (range 18–90). Race among BC and non-BC patients was also dissimilar in that there was a higher frequency of black patients in the BC group. The most common non-BC malignancies were gastrointestinal (43.7%), genitourinary (15.5%), and gynecologic cancer (11.2%) (Supplemental Table 1).
Most patients had an ECOG PS of 0 (31.7%) or 1 (59.9%). The BC cohort had a greater frequency of patients with a PS of 0 (35.8%) than those without BC (31.2%). Regarding pre-treatment laboratory values, hemoglobin levels were similar between BC and non-BC patients. Platelet count was slightly lower in BC patients. Albumin was mildly lower in non-BC patients than in BC patients.
Pre-enrollment characteristics
The median time from initial cancer diagnosis to enrollment in a CTEP-sponsored Phase 1 clinical trial was 614 days for all patients (Table 2). Breast cancer patients were found to be enrolled on average 790 days after initial diagnosis while non-BC patients had a median enrollment time of 582 days (p < 0.001). Along with this longer time to enrollment, BC patients were also found to be more heavily pretreated with a median of 4 (range 1–26) prior medical treatments than those with other cancers at 3 prior treatments (range 1–19).
Treatment
Of the 8087 patients enrolled, 84 did not receive any dose of study drug and were thus removed from further analysis. While on phase I study, the best response to treatment was evaluated (Table 3). Disease progression was the best response in slightly less than 40% of all patients. Breast cancer patients had more clinical responses (complete and partial responses) than non-BC patients (18.3% vs. 4.3%, respectively). In addition, 42.7% of BC patients achieved stable disease compared to 57.2% of non-BC patients. Along with the higher rate of response, BC patients were found to be on phase I trials longer than non-BC patients with a median of 70 days while the latter were on trial for a median of 57 days (Table 4).
Treatment tolerability and toxicity
Among the 8003 patients that received treatment, 1680 patients experienced at least one grade 4 or 5 adverse event representing 25.9 (n = 353) and 20.0% (n = 1327) of BC and non-BC patients respectively (Table 5). The overall rate of death related to the treatment drugs was 0.47% (n = 38) and was similar between BC and non-BC patients (0.58 and 0.45% respectively). Of the 38 deaths thought to be related to study drug, 26 were considered “possible”, 3 as “probable” and 9 as “definite”. Of the 3887 grade 4 AEs in which attribution data was recorded, 2790 were treatment-related. Of these, 24.9% occurred in BC patients and 75.1% in patients without BC (Table 6). Breast cancer patients more often had a full recovery of grade 4 AE then non-BC patients (78.5% vs. 54.1%, respectively). The median time to recovery for all grade 4 AEs was 7 days. Breast cancer patients seem to experience a slightly quicker recovery time with a median of 6 days. Statistical significance was not evaluated in here as several patients had multiple AEs and not all AEs were independent events.
Discussion
To our knowledge this study is the first to compare enrollment characteristics, response rates and toxicity between BC and other patients enrolled on the same phase I trials. In our study we confirmed that patients with BC enrolled in CTEP-sponsored phase I trials are more heavily pretreated, have higher response rates and have a similar toxicity profile compared to non-BC patients enrolled on the same trials. Our results also confirm that patients with BC are enrolled in phase I clinical trials later in the course of their disease when compared to patients diagnosed with other malignancies, based on number of previous lines of therapy and time from initial diagnosis to enrollment.
The reported high response rates of BC patients (18.3%) suggest a higher benefit from phase I oncology trials than previously reported. Historically, patients treated on phase I studies have response rates of 4–10.6% [11, 25]. In a small retrospective study of 78 patients with metastatic breast cancer (MBC) treated in phase I trials at MD Anderson [26], there were no complete or partial responses. On another study from the same institution, 8.2% (8 of 98) of evaluable patients with MBC achieved complete (n = 1) or partial response (n = 7) [10], and if treated on matched therapy had improved rate of stable disease for 6 months and partial or complete response when compared with those on nonmatched therapy (33% vs. 8%, p = 0.018). However, our data are derived only from trials sponsored by the CTEP. Although the program is a major sponsor of phase I oncology trials in the United States, there may be differences in terms of response rate with other phase I trials that were not captured in this study.
The overall rate of toxicity-related deaths on phase I trials has remained stable [1,2,3,4,5,6,7,8,9]. Breast cancer patients experienced more grade 4 toxicities while on study than other patients, but fewer were treatment-related and more BC patients had complete resolution of toxicities compared to non-BC patients. These findings, along with a similar rate of treatment-related deaths, confirm that despite being more heavily pretreated, BC patients do not experience increased toxicity. However, one important limitation of this study is the lack of detailed information on patient-specific reported data on grade 4 and 5 events.
Finally, our findings suggest that BC patients are enrolled in phase I clinical trials later in the course of their diseases when compared to non-BC patients. It is unclear whether this reflects the natural history of breast cancer and the fact that there are many available standard therapies for breast cancer. Between 1993 and 2012, eleven drugs received accelerated or regular FDA approval for advanced BC which makes BC the oncologic disease with the most FDA drug approvals in the last decades [27, 28]. Other factors may contribute to this pattern of late referrals, including the type of institution where BC treatment is delivered and the availability of early phase trials, or health provider/patients stigma against phase I clinical trials. Lack of participation by BC patients on phase I trials may represent missed opportunities to detect early signals of response of promising drugs for this disease.
In summary, we showed that phase I clinical trials are associated with clinical benefit in a significant number of BC patients with similar toxicity profile of other non-BC patients, despite being enrolled later in the course of their diseases. Multiple factors are possibly associated with the pattern of late referrals of BC patients to participation in phase I clinical trials and are worth further exploring.
Abbreviations
- AE:
-
Adverse events
- BC:
-
Breast cancer
- CTCAE:
-
Common terminology criteria for adverse events
- CTEP:
-
Cancer therapy evaluation program
- CTMS:
-
Clinical trials monitoring service
- ECOG:
-
Eastern cooperative oncology group
- MBC:
-
Metastatic breast cancer
- OS:
-
Overall survival
- PIO:
-
Protocol and information office
- PS:
-
Performance status
- RECIST:
-
Response evaluation criteria in solid tumors
- RP2D:
-
Recommended phase 2 dose
References
Itoh K, Sasaki Y, Miyata Y et al (1994) Therapeutic response and potential pitfalls in phase I clinical trials of anticancer agents conducted in Japan. Cancer Chemother Pharmacol 34:451–454
Estey E, Hoth D, Simon R et al (1986) Therapeutic response in phase I trials of antineoplastic agents. Cancer Treat Rep 70:1105–1115
Decoster G, Stein G, Holdener EE (1990) Responses and toxic deaths in phase I clinical trials. Ann Oncol 1:175–181
Bachelot T, Ray-Coquard I, Catimel G et al (2000) Multivariable analysis of prognostic factors for toxicity and survival for patients enrolled in phase I clinical trials. Ann Oncol 11:151–156
Han C, Braybrooke JP, Deplanque G et al (2003) Comparison of prognostic factors in patients in phase I trials of cytotoxic drugs vs new noncytotoxic agents. Br J Cancer 89:1166–1171
Roberts TG Jr, Goulart BH, Squitieri L et al (2004) Trends in the risks and benefits to patients with cancer participating in phase 1 clinical trials. JAMA 292:2130–2140
Sekine I, Yamamoto N, Kunitoh H et al (2002) Relationship between objective responses in phase I trials and potential efficacy of non- specific cytotoxic investigational new drugs. Ann Oncol 13:1300–1306
Smith TL, Lee JJ, Kantarjian HM et al (1996) Design and results of phase I cancer clinical trials: three-year experience at M.D Anderson Cancer Center. J Clin Oncol 14:287–295
Von Hoff DD, Turner J (1991) Response rates, duration of response, and dose response effects in phase I studies of antineoplastics. Invest New Drugs 9:115–122
Ganesan P, Moulder S, Lee JJ et al (2014) Triple-Negative Breast Cancer Patients Treated at MD Anderson Cancer Center in phase I trials: improved outcomes with combination chemotherapy and targeted agents. Mol Cancer Ther 13(12):3175–3184
Horstmann E, McCabe MS, Grochow L et al (2005) Risks and benefits of phase 1 oncology trials, 1991 through 2002. N Engl J Med 352:895–904
Agus DB, Gordon MS, Taylor C et al (2005) Phase I clinical study of pertuzumab, a novel her dimerization inhibitor, in patients with advanced cancer. J Clin Oncol 23:2534–2543
Phillips GDL, Fields CT, Li G et al (2013) Dual Targeting of HER2 positive cancer with trastuzumab emtansine and pertuzumab: critical role for neuregulin blockade in antitumor response to combination therapy. Clin Cancer Res 15 20(2):456–468
Nanda R, Chow QL, Dees EC et al (2016) Pembrolizumab in patients with advanced triple-negative breast cancer: phase ib keynote-012 study. J Clin Oncol 34(21):2460–2467
Howlader N, Noone AM, Krapcho M, et al (eds). SEER Cancer Statistics Review, 1975-2014, National Cancer Institute. Bethesda, MD, https://seer.cancer.gov/csr/1975_2014/, based on November 2016 SEER data submission, posted to the SEER web site, April 2017
Sledge GW, Neuberg D, Bernardo P et al (2003) Phase III trial of doxorubicin, paclitaxel, and the combination of doxorubicin and paclitaxel as front- line chemotherapy for metastatic breast cancer: an intergroup trial (E1193). J Clin Oncol 21:588–592
Cresta S, Grasselli G, Mansutti M et al (2004) A randomized phase II study of combination, alternating and sequential regimens of doxorubicin and docetaxel as first-line chemotherapy for women with metastatic breast cancer. Ann Oncol 15(3):433–439
Conte PF, Guarneri V, Bruzzi P et al (2004) Concomitant versus sequential administration of epirubicin and paclitaxel as first-line therapy in metastatic breast carcinoma: results for the Gruppo Oncologico Nord Ovest randomized trial. Cancer 101:704–712
Alba E, Martin M, Ramos M et al (2004) Multicenter randomized trial comparing sequential with concomitant administration of doxorubicin and docetaxel as first-line treatment of metastatic breast cancer: a Spanish Breast Cancer Research Group (GEICAM-9903) phase III study. J Clin Oncol 22:2587–2593
Swain SM, Baselga J, Kim S-B et al (2015) Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N Engl J Med 372:724–734
Tejeda HA, Green SB, Trimble EL et al (1996) Representation of African-Americans, Hispanics, and whites in National Cancer Institute cancer treatment trials. J Natl Cancer Inst 88:812–816
Go RS, Frisby KA, Lee JA et al (2006) Clinical trial accrual among new cancer patients at a community-based cancer center. Cancer 106:426–433
Postel-Vinay S, Aspeslagh S, Lanoy E et al (2016) Challenges of phase 1 clinical trials evaluating immune checkpoint-targeted antibodies. Ann Oncol 27:214–224
Ma C, Bandukwala S, Burman D et al (2010) Interconversion of three measures of performance status: an empirical analysis. Eur J Cancer 46(18):3175–3183
Kurzrock R, Benjamin RS (2005) Risks and benefits of phase 1 oncology trials, revisited. N Engl J Med 352:930–932
Wheler J, Tsimberidou A, Moulder S et al (2010) Clinical Outcomes of patients with breast cancer in a phase I clinic: the MD Anderson Cancer Center Experience. Clinical Breast Cancer 10(1):46–51
Verma S, McLeod D, Batist G et al (2011) In the end what matters most? A review of clinical endpoints in advanced breast cancer. Oncologist 16(1):25–35
FDA Hematology/Oncology (Cancer) Approvals & Safety Notifications (2015) https://wayback.archive-it.org/7993/20170111231726/http://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm381452.htm. Accessed on 5 May 2017
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Lynce, F., Blackburn, M.J., Cai, L. et al. Characteristics and outcomes of breast cancer patients enrolled in the National Cancer Institute Cancer Therapy Evaluation Program sponsored phase I clinical trials. Breast Cancer Res Treat 168, 35–41 (2018). https://doi.org/10.1007/s10549-017-4563-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-017-4563-3