
Abstract
The clinicopathologic, mammographic, and sonographic findings in patients with pure ductal carcinoma in situ (DCIS) were assessed by estrogen receptor (ER) expression. After institutional review board approval, patients with pure DCIS evaluated from January 1996 to July 2009 with known ER status and available imaging were identified. Images were reviewed as per the ACR BI-RADS® lexicon (4th edition). Clinical, pathologic, and imaging characteristics were analyzed by ER status using t test, Chi square test, and Fisher’s exact test. Of 1,219 patients with pure DCIS and known ER status identified, 1,187 with complete data were included. Mammography was performed in all 1,187 patients and sonography in 519 (44 %). There were 972 (82 %) patients with ER-positive and 215 (18 %) with ER-negative disease. ER-negative DCIS was more likely to be high grade (93 vs 44 %, p < 0.0001), associated with comedonecrosis (64 vs 29 %, p < 0.0001), and multifocal (23 vs 15 %, p = 0.009). On sonography, ER-negative DCIS was more likely to be visible (61 vs 46 %, p = 0.004), larger (mean size, 2.3 vs 1.6 cm, p = 0.006), and show posterior shadowing (53 vs 28 %, p = 0.006). Mastectomy was more frequently performed for ER-negative DCIS (47 vs 37 %, p = 0.008). Palpable DCIS was visible on sonography in 55 % of cases and mammography in 81 %. Compared with ER-positive palpable DCIS, ER-negative palpable DCIS was larger and more likely to be visible on sonography. Compared with ER-positive noncalcified DCIS, ER-negative noncalcified DCIS was less likely to be visible on mammography. ER-positive and ER-negative pure DCIS have different clinicopathologic and imaging characteristics. ER-negative DCIS is associated with worse prognostic factors than ER-positive DCIS. On sonography, ER-negative DCIS is more frequently visible than ER-positive DCIS, tends to be larger, and more frequently demonstrates posterior shadowing.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The detection of ductal carcinoma in situ (DCIS) has increased significantly with the widespread use of screening mammography in asymptomatic women. DCIS now accounts for up to 30 % of breast cancers in the screening population [1–4]. Early diagnosis and management of DCIS are critical in preventing the development of invasive cancer [5–9]. Mammography remains the most valuable technique for the detection of DCIS [10, 11].
Ductal carcinoma is a heterogeneous disease with regard to biology and has histopathologic characteristics similar to those of invasive breast cancer. The malignant potential and behavior of DCIS after treatment are influenced by nuclear grade (low, intermediate, or high), architectural pattern (solid, cribriform, papillary, or micropapillary), and the presence of comedonecrosis. High-nuclear grade and comedonecrosis indicate aggressive biological attributes to DCIS and are associated with a higher rate of local recurrence [2, 5, 11–13].
In recent years, molecular profiling has led to improved understanding of the biology and behavior of invasive breast disease [14]. Within the spectrum of invasive breast cancer, intrinsic biological subtypes exist that have different prognoses and responses to local and systemic therapies [15]. The intrinsic biological subtypes can be approximated with immunohistochemical evaluation of estrogen receptor (ER), progesterone receptor, and HER2-neu expression.
Increasing evidence suggests that biomarker expression in cancer patients influences disease detection, staging, response to treatment, and prognosis after treatment [1, 16]. ER is the best studied biomarker in breast cancer, and the expression or lack of expression of ER defines and differentiates the luminal and basal breast cancer biological subtypes. Several studies have demonstrated a relationship between ER expression and nuclear grade [17–24] and risk of local recurrence of DCIS [25–28]. However, reports focusing on the influence of ER expression on the clinicopathologic and imaging features of DCIS are scarce [29]. The purpose of this retrospective study was to describe the clinicopathologic, mammographic, and sonographic findings in patients with pure DCIS by ER expression.
Materials and methods
Following Institutional Review Board approval, our Breast Cancer Management System database was searched to identify all patients with a diagnosis of pure DCIS and known ER status evaluated and treated between January 1, 1996, and July 31, 2009. Demographic characteristics and clinical, pathologic, mammographic, and sonographic findings were retrospectively analyzed by ER status for all the patients (n = 1187) as well as for the subsets of patients with noncalcified lesions (n = 126, 11 %) and palpable lesions (n = 115, 10 %). Breast magnetic resonance imaging (MRI) findings were not included in this analysis, since MRI was not used routinely during the study period.
Clinicopathologic assessment
The following variables were reviewed: age at diagnosis, menopausal status, use of hormone replacement therapy, bilaterality, presence of contralateral breast cancer (DCIS or invasive breast cancer), initial presenting signs (clinical or radiologic), and type of the first definitive surgery (segmentectomy or mastectomy).
The original pathology slides from biopsy and/or surgery were re-reviewed for this study by a dedicated breast pathologist with 20 years experience. The following parameters were recorded: nuclear grade [well differentiated (grade 1), intermediate (grade 2), or poorly differentiated (grade 3)]; presence of comedonecrosis; architectural pattern (solid, cribriform, papillary, micropapillary, unspecified, or combination); size of the DCIS; and presence of multifocality and multicentricity. ER status was defined as positive if nuclear staining was present in at least 1 % of cells.
Mammography
Each mammogram (standard two-view with additional views as necessary) was originally read by one of 14 dedicated breast radiologists with 6–21 years of experience, and re-read by one of four dedicated breast radiologists with 6–12 years of experience. The American College of Radiology-Breast Imaging Report and Data System (ACR BI-RADS®) lexicon, 4th edition [30], was used to classify all the mammographic findings: breast density, masses (shape, margins, density), calcifications (morphology, distribution), architectural distortion, and focal asymmetry. The extent of DCIS was defined as the maximum length for calcifications and maximum diameter for masses. Multifocality was defined as the presence of two or more foci of disease in the same breast quadrant. Multicentricity was defined as the presence of disease in multiple breast quadrants or disease foci separated by more than 5 cm. For cases of multifocality or multicentricity, the size of the largest lesion was recorded.
Sonography
Sonograms were originally read by one of the 14 dedicated breast radiologists with 6–21 years of experience and re-read by one of four dedicated breast radiologists with 6–12 years of experience. Findings were interpreted utilizing the ACR BI-RADS® ultrasound lexicon, 4th edition [31], and classified as masses, parenchymal heterogeneity, or calcifications. Parenchymal heterogeneity was defined as an area of breast tissue that appeared distorted with no definable central mass [13, 32, 33]. Multifocality, multicentricity, and size were determined as for mammography.
Statistical methods
T-tests, Chi square tests, and Fisher’s exact tests were used to assess univariate association between variables of interest and ER status. Multiple logistic regression was performed to evaluate multivariable associations with ER status. P values less than 0.05 were considered statistically significant. No adjustments were performed for multiple comparisons. All the statistical analyses were performed using SAS software, version 9.2, for Windows (SAS Institute Inc., Cary, NC).
Results
Clinicopathologic data
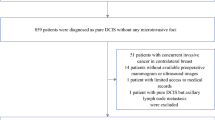
Of the 1,219 patients identified, 32 were excluded because of microinvasion (n = 8) or absent imaging (n = 24), leaving 1,187 patients for analysis. All 1,187 patients had mammography, and 519 (44 %) had whole-breast sonography. A total of 215 patients (18 %) had ER-negative and 972 (82 %) ER-positive disease. The mean age at diagnosis was 56 years [standard deviation (SD) = 11] for all patients, 57 years (SD = 11) for patients with ER-negative lesions, and 55 years (SD = 11) for patients with ER-positive lesions.
Major clinicopathologic differences between the ER-negative and ER-positive patients are summarized in Table 1. Patients with ER-negative DCIS were slightly older (p = 0.008) and more likely to be postmenopausal (p = 0.003). ER-negative DCIS was more likely to be high grade (p < 0.0001), and to demonstrate comedonecrosis (p < 0.0001), multifocality (p = 0.009), multicentricity (p = 0.014), and solid architectural pattern (p < 0.0001). Mastectomy was more common among patients with ER-negative DCIS (p = 0.008). Clinical symptoms were present in 165 (14 %) of patients: 119 (10 %) had palpable masses and 46 (4 %) nipple discharge. Patients with ER-negative DCIS were somewhat more likely to present with a clinical abnormality, but this difference did not reach statistical significance (18 vs 13 %, p = 0.083).
Of the 115 patients with palpable DCIS, 29 (25 %) had ER-negative and 86 (75 %) ER-positive disease. The mean age of these patients was 49 years (SD = 11), which was significantly younger than the mean age for the rest of the population (56 years, SD = 11, p < 0.0001). Mammography and sonography findings were available for 115 patients (100 %) and 78 patients (68 %), respectively. Among patients with palpable DCIS, ER-negative DCIS was more likely than ER-positive DCIS to be high grade (p < 0.0001), multifocal (p = 0.012), multicentric (p = 0.023), and treated by mastectomy (p = 0.147).
Among the 126 patients with noncalcified DCIS, mammography and sonography findings were available for 126 patients (100 %) and 110 patients (96 %), respectively. Compared to ER-positive noncalcified DCIS, ER-negative noncalcified DCIS was larger at histopathology (p = 0.006) and more likely to be high grade (p < 0.0001), multifocal (p = 0.004), multicentric (p = 0.005), and treated by mastectomy (p = 0.034).
Mammography findings
A mammographically detected abnormality was the primary presentation for both ER-negative and ER-positive DCIS (Table 2). In both ER groups, lesions were highly visible on mammography, and calcifications were the dominant mammographic finding. Fine linear and fine pleomorphic calcifications were the most common morphology seen in both ER groups, with increased frequency in high-grade subgroup.
Only 9 % of patients in each ER group presented with a mass. Mass density was distributed differently by ER status (p = 0.045): masses were isodense to breast tissue in all eight ER-negative tumors but isodense in 42 (62 %) and high density in 26 (38 %) of the 68 ER-positive tumors with the available data.
In the subset of 115 patients with palpable DCIS, 93 patients (81 %) had a corresponding mammographic abnormality: 69 (75 %) had calcifications only, 13 (14 %) a mass or focal asymmetry, and 10 (11 %) a mass with calcifications. No significant differences were observed in mammographic findings or in mammographic visibility by ER status.
In the subset of 126 patients with noncalcified DCIS, 85 patients (67 %) had a corresponding mammographic abnormality: 52 (61 %) had a mass, 20 (24 %) focal asymmetry, and 13 (15 %) architectural distortion. ER-negative noncalcified DCIS was less likely than ER-positive noncalcified DCIS to be visible on mammography (p = 0.0335).
Sonography findings
A sonographic abnormality was seen in 254 patients (49 %); 227 (89 %) of these patients had masses and 27 (11 %) had parenchymal heterogeneity (Table 3). Compared to ER-positive DCIS, ER-negative DCIS was more likely to be visible (p = 0.004), was larger (p = 0.006) and more frequently demonstrated posterior shadowing (p = 0.006).
In the subset of 115 patients with palpable DCIS, 43 patients (55 %) had lesions that were visible on sonography. The most common sonographic finding for both ER-negative and ER-positive palpable DCIS was a hypoechoic irregular hypervascular mass, parallel in orientation without posterior features. ER-negative palpable DCIS was larger (p = 0.008) and more likely to be visible (p = 0.079) on sonography than ER-positive palpable DCIS.
In the subset of 126 patients with noncalcified DCIS, 104 patients (95 %) had lesions that were visible on sonography. The most common sonographic appearance for both ER-negative and ER-positive noncalcified DCIS was a hypoechoic, irregular mass. ER-negative noncalcified DCIS was larger (p = 0.037) than ER-positive noncalcified DCIS.
Visibility of DCIS on mammography and sonography
The visibility of DCIS in patients who had both mammography and sonography are summarized in Table 4. ER-positive DCIS was more likely than ER-negative DCIS to be visible only on mammography, while ER-negative DCIS was more likely than ER-positive DCIS to be visible on both mammography and sonography or on sonography only (p = 0.032).
In the subgroup with palpable DCIS, 78 of 115 patients (68 %) had both mammography and sonography; in the subgroup with noncalcified DCIS, 110 of 126 patients (96 %) had both mammography and sonography. There were no differences in visibility on mammography or sonography by ER status in these groups of patients.
Discussion
The National Cancer Institute has identified a need for the investigation and validation of molecular factors that improve risk stratification and facilitate optimal treatment of patients with DCIS [1, 16, 34]. The ER expression rate in DCIS ranges from 49 to 97 % (mean, 69 %) [16]. Relationships have been described between ER status and disease recurrence [25–28], nuclear grade [17, 18, 20, 23], indications for adjuvant hormonal therapy [35–38], and presurgical prediction of disease extent [7, 39]. However, information is scarce regarding the influence of ER expression on clinicopathologic and imaging features of DCIS [29].
Our analysis of 1,187 patients confirmed differences in clinical, pathologic, and imaging features between ER-negative and ER-positive DCIS. Patients with ER-negative DCIS were slightly older and more likely to be postmenopausal than patients with ER-positive disease. ER-negative tumors were larger on sonography, mammography, and pathologic evaluation, and were more likely to be multifocal and multicentric, explaining the higher frequency of mastectomy in this patient group.
The prognosis of DCIS depends on its histopathologic subtype and nuclear grade. A spectrum of mammographic appearances of DCIS have been described in the literature [10, 12, 13, 40–42]. Calcifications are the most common presentation of DCIS; high-grade lesions present predominantly with fine pleomorphic or fine linear branching morphology, while low- and intermediate-grade lesions present predominantly with amorphous or coarse heterogeneous morphology [10–12, 40, 43, 44]. Similarly, in our study, high-grade pure DCIS, independent of ER status, presented predominantly as fine pleomorphic or fine linear branching calcifications.
Analysis of the relationship of nuclear grade with ER status showed that 93 % of ER-negative DCIS lesions and only 44 % of ER-positive DCIS lesions were of high-nuclear grade. ER-negative DCIS was more frequently associated with comedonecrosis (64 %). Both high-nuclear grade and comedonecrosis are associated with higher likelihood of local recurrence and development of invasive cancer [25–28]. Our findings agree with the prior studies showing higher ER expression in well-differentiated lesions than in poorly differentiated lesions [17–24, 45].
The reported sonographic appearance of pure DCIS is a hypoechoic, irregular mass with ductal extension without posterior acoustic shadowing or enhancement [13, 46]. The presence of marked hypoechogenicity, a spiculated margin, a thick echogenic rim, or posterior acoustic shadowing should prompt concern regarding the presence of DCIS with microinvasion or invasive carcinoma [13, 46, 47].
Our analysis showed that ER-negative DCIS was more likely to be visible on sonography than was ER-positive DCIS, whereas ER-positive DCIS was more likely to be visible on mammography only. On sonography, ER-negative DCIS was larger than ER-positive DCIS and more commonly associated with posterior shadowing. These findings suggest that sonography may have a role in the diagnosis and staging of ER-negative DCIS.
Patients with palpable DCIS, an important subgroup, tended to be younger (mean age, 49 years) than other patients. The most common imaging finding for palpable DCIS, independent of ER status, was calcifications. This explains the high visibility of palpable DCIS on mammography and the moderate visibility on sonography. On sonography, ER-negative palpable DCIS was significantly larger and was more likely to be detected than ER-positive palpable DCIS.
Another important subgroup was patients with noncalcified lesions, including masses, architectural distortion, and/or focal asymmetry [10, 11]. Interestingly, we found a significant difference in mammographic visibility by ER status in this subgroup: ER-negative noncalcified DCIS was less likely to be visible on mammography than ER-positive noncalcified DCIS. In our study, approximately one-third of noncalcified DCIS lesions were mammographically occult, which is concordant with prior reports [10, 46]. Almost all (95 %) noncalcified DCIS lesions were visible on sonography, and sonographic visibility did not differ by ER status. All ER-negative noncalcified DCIS lesions were visible on sonography, and ER-negative lesions were significantly larger than ER-positive lesions. These findings underscore the role of sonography in the evaluation of patients with DCIS, especially ER-negative DCIS.
The major limitation of our study was its retrospective design. Not all the variables were available for the entire set of patients. Sonography is currently not standard of care for patients with DCIS, which explains why 56 % of the patients in our sample did not have sonography performed.
In summary, compared to ER-positive DCIS, ER-negative DCIS is more likely to be detected at a larger size, to be of high nuclear grade, to demonstrate comedonecrosis, and to be detected in older postmenopausal patients. When ER-negative DCIS presents as a mass, it usually is visible on sonography or both sonography and mammography, shows posterior shadowing on sonography, and is isodense to the breast tissue on mammography. ER-negative DCIS is more likely than ER-positive DCIS to be multifocal or multicentric and is more frequently associated with mastectomy. ER-negative noncalcified DCIS is less likely to be visible on mammography than ER-positive noncalcified DCIS. In patients with palpable DCIS, 55 % of lesions were visible on sonography and 81 % were visible on mammography; ER-negative tumors tended to be larger and were more likely to be visible on sonography.
To our knowledge, this is the first large clinical study describing the clinicopathologic and imaging differences associated with biological subtypes of DCIS—differences that may impact diagnosis, staging, and therapy. Further studies are warranted to evaluate the roles of biological markers in the diagnosis and treatment of DCIS.
References
Kuerer HM, Albarracin CT, Yang WT, Cardiff RD, Brewster AM, Symmans WF, Hylton NM, Middleton LP, Krishnamurthy S, Perkins GH, Babiera G, Edgerton ME, Czerniecki BJ, Arun BK, Hortobagyi GN (2009) Ductal carcinoma in situ: state of the science and roadmap to advance the field. J Clin Oncol 27:279–288. doi:10.1200/JCO.2008.18.3103
Virnig BA, Tuttle TM, Shamliyan T, Kane RL (2010) Ductal carcinoma in situ of the breast: a systematic review of incidence, treatment, and outcomes. J Natl Cancer Inst 102:170–178. doi:10.1093/jnci/djp482
Ernster VL, Ballard-Barbash R, Barlow WE, Zheng Y, Weaver DL, Cutter G, Yankaskas BC, Rosenberg R, Carney PA, Kerlikowske K, Taplin SH, Urban N, Geller BM (2002) Detection of ductal carcinoma in situ in women undergoing screening mammography. J Natl Cancer Inst 94:1546–1554
Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, Feuer EJ, Thun MJ (2005) Cancer statistics. CA Cancer J Clin 55:10–30
Boughey JC, Gonzalez RJ, Bonner E, Kuerer HM (2007) Current treatment and clinical trial developments for ductal carcinoma in situ of the breast. Oncologist 12:1276–1287. doi:10.1634/theoncologist.12-11-1276
Roses RE, Arun BK, Lari SA, Mittendorf EA, Lucci A, Hunt KK, Kuerer HM (2011) Ductal carcinoma-in situ of the breast with subsequent distant metastasis and death. Ann Surg Oncol 18:2873–2878. doi:10.1245/s10434-011-1707-2
MacDonald HR, Silverstein MJ, Mabry H, Moorthy B, Ye W, Epstein MS, Holmes D, Silberman H, Lagios M (2005) Local control in ductal carcinoma in situ treated by excision alone: incremental benefit of larger margins. Am J Surg 190:521–525. doi:10.1016/j.amjsurg.2005.06.005
Tabar L, Tony Chen HH, Amy Yen MF, Tot T, Tung TH, Chen LS, Chiu YH, Duffy SW, Smith RA (2004) Mammographic tumor features can predict long-term outcomes reliably in women with 1–14-mm invasive breast carcinoma. Cancer 101:1745–1759. doi:10.1002/cncr.20582
Yi M, Krishnamurthy S, Kuerer HM, Meric-Bernstam F, Bedrosian I, Ross MI, Ames FC, Lucci A, Hwang RF, Hunt KK (2008) Role of primary tumor characteristics in predicting positive sentinel lymph nodes in patients with ductal carcinoma in situ or microinvasive breast cancer. Am J Surg 196:81–87. doi:10.1016/j.amjsurg.2007.08.057
Stomper PC, Margolin FR (1994) Ductal carcinoma in situ: the mammographer’s perspective. AJR Am J Roentgenol 162:585–591. doi:10.2214/ajr.162.3.8109501
Barreau B, de Mascarel I, Feuga C, MacGrogan G, Dilhuydy MH, Picot V, Dilhuydy JM, de Lara CT, Bussieres E, Schreer I (2005) Mammography of ductal carcinoma in situ of the breast: review of 909 cases with radiographic-pathologic correlations. Eur J Radiol 54:55–61. doi:10.1016/j.ejrad.2004.11.019
Zunzunegui RG, Chung MA, Oruwari J, Golding D, Marchant DJ, Cady B (2003) Casting-type calcifications with invasion and high-grade ductal carcinoma in situ: a more aggressive disease? Arch Surg 138:537–540. doi:10.1001/archsurg.138.5.537
Yang WT, Tse GM (2004) Sonographic, mammographic, and histopathologic correlation of symptomatic ductal carcinoma in situ. AJR Am J Roentgenol 182:101–110. doi:10.2214/ajr.182.1.1820101
Sorlie T, Tibshirani R, Parker J, Hastie T, Marron JS, Nobel A, Deng S, Johnsen H, Pesich R, Geisler S, Demeter J, Perou CM, Lonning PE, Brown PO, Borresen-Dale AL, Botstein D (2003) Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc Natl Acad Sci USA 100:8418–8423. doi:10.1073/pnas.0932692100
Prat A, Perou CM (2011) Deconstructing the molecular portraits of breast cancer. Mol Oncol 5:5–23. doi:10.1016/j.molonc.2010.11.003
Lari SA, Kuerer HM (2011) Biological markers in DCIS and risk of breast recurrence: a systematic review. J Cancer 2:232–261
Altintas S, Lambein K, Huizing MT, Braems G, Asjoe FT, Hellemans H, Van Marck E, Weyler J, Praet M, Van den Broecke R, Vermorken JB, Tjalma WA (2009) Prognostic significance of oncogenic markers in ductal carcinoma in situ of the breast: a clinicopathologic study. Breast J 15:120–132. doi:10.1111/j.1524-4741.2009.00686.x
Bijker N, Peterse JL, Duchateau L, Robanus-Maandag EC, Bosch CA, Duval C, Pilotti S, van de Vijver MJ (2001) Histological type and marker expression of the primary tumour compared with its local recurrence after breast-conserving therapy for ductal carcinoma in situ. Br J Cancer 84:539–544. doi:10.1054/bjoc.2000.1618
Claus EB, Chu P, Howe CL, Davison TL, Stern DF, Carter D, DiGiovanna MP (2001) Pathobiologic findings in DCIS of the breast: morphologic features, angiogenesis, HER-2/neu and hormone receptors. Exp Mol Pathol 70:303–316. doi:10.1006/exmp.2001.2366
Collins LC, Schnitt SJ (2005) HER2 protein overexpression in estrogen receptor-positive ductal carcinoma in situ of the breast: frequency and implications for tamoxifen therapy. Mod Pathol 18:615–620. doi:10.1038/modpathol.3800360
Hanley K, Wang J, Bourne P, Yang Q, Gao AC, Lyman G, Tang P (2008) Lack of expression of androgen receptor may play a critical role in transformation from in situ to invasive basal subtype of high-grade ductal carcinoma of the breast. Hum Pathol 39:386–392. doi:10.1016/j.humpath.2007.07.007
Lebeau A, Unholzer A, Amann G, Kronawitter M, Bauerfeind I, Sendelhofert A, Iff A, Lohrs U (2003) EGFR, HER-2/neu, cyclin D1, p21 and p53 in correlation to cell proliferation and steroid hormone receptor status in ductal carcinoma in situ of the breast. Breast Cancer Res Treat 79:187–198
Lebrecht A, Buchmann J, Hefler L, Lampe D, Koelbl H (2002) Histological category and expression of hormone receptors in ductal carcinoma in situ of the breast. Anticancer Res 22:1909–1911
Meijnen P, Peterse JL, Antonini N, Rutgers EJ, van de Vijver MJ (2008) Immunohistochemical categorization of ductal carcinoma in situ of the breast. Br J Cancer 98:137–142. doi:10.1038/sj.bjc.6604112
Kerlikowske K, Molinaro AM, Gauthier ML, Berman HK, Waldman F, Bennington J, Sanchez H, Jimenez C, Stewart K, Chew K, Ljung BM, Tlsty TD (2010) Biomarker expression and risk of subsequent tumors after initial ductal carcinoma in situ diagnosis. J Natl Cancer Inst 102:627–637. doi:10.1093/jnci/djq101
Provenzano E, Hopper JL, Giles GG, Marr G, Venter DJ, Armes JE (2003) Biological markers that predict clinical recurrence in ductal carcinoma in situ of the breast. Eur J Cancer 39:622–630
Ringberg A, Anagnostaki L, Anderson H, Idvall I, Ferno M (2001) Cell biological factors in ductal carcinoma in situ (DCIS) of the breast-relationship to ipsilateral local recurrence and histopathological characteristics. Eur J Cancer 37:1514–1522
Roka S, Rudas M, Taucher S, Dubsky P, Bachleitner-Hofmann T, Kandioler D, Gnant M, Jakesz R (2004) High nuclear grade and negative estrogen receptor are significant risk factors for recurrence in DCIS. Eur J Surg Oncol 30:243–247. doi:10.1016/j.ejso.2003.11.004
Kojima Y, Tsunoda H, Honda S, Kikuchi M, Kawauchi N, Yoshida A, Yagata H, Yamauchi H, Suzuki K (2011) Radiographic features for triple negative ductal carcinoma in situ of the breast. Breast Cancer 18:213–220. doi:10.1007/s12282-011-0261-x
D’Orsi C, Mendelson EB, Ikeda D (2003) Breast imaging reporting and data system: ACR BI-RADS - Breast Imaging Atlas. American College of Radiology, Reston
Mendelson EB, Baum J, Berg W (2003) BI-RADS: Ultrasound, 1st edition. In: D’Orsi CJ, Mendelson EB, Ikeda DM et al (eds) Breast imaging reporting and data system: ACR BI-RADS-Breast Imaging Atlas. American College of Radiology, Reston
Samardar P, de Paredes ES, Grimes MM, Wilson JD (2002) Focal asymmetric densities seen at mammography: US and pathologic correlation. Radiographics 22:19–33
Takei J, Tsunoda-Shimizu H, Kikuchi M, Kawasaki T, Yagata H, Tsugawa K, Suzuki K, Nakamura S, Saida Y (2009) Clinical implications of architectural distortion visualized by breast ultrasonography. Breast Cancer 16:132–135. doi:10.1007/s12282-008-0085-5
Allegra CJ, Aberle DR, Ganschow P, Hahn SM, Lee CN, Millon-Underwood S, Pike MC, Reed SD, Saftlas AF, Scarvalone SA, Schwartz AM, Slomski C, Yothers G, Zon R (2010) National Institutes of Health State-of-the-Science Conference statement: diagnosis and management of ductal carcinoma in situ. September 22–24, 2009. J Natl Cancer Inst 102:161–169. doi:10.1093/jnci/djp485
Chen YY, DeVries S, Anderson J, Lessing J, Swain R, Chin K, Shim V, Esserman LJ, Waldman FM, Hwang ES (2009) Pathologic and biologic response to preoperative endocrine therapy in patients with ER-positive ductal carcinoma in situ. BMC Cancer 9:285. doi:10.1186/1471-2407-9-285
Cuzick J, Sestak I, Pinder SE, Ellis IO, Forsyth S, Bundred NJ, Forbes JF, Bishop H, Fentiman IS, George WD (2011) Effect of tamoxifen and radiotherapy in women with locally excised ductal carcinoma in situ: long-term results from the UK/ANZ DCIS trial. Lancet Oncol 12:21–29. doi:10.1016/S1470-2045(10)70266-7
Eng-Wong J, Costantino JP, Swain SM (2010) The impact of systemic therapy following ductal carcinoma in situ. J Natl Cancer Inst Monogr 41:200–203. doi:10.1093/jncimonographs/lgq021
Kuerer HM (2011) Rational individualised selection of adjuvant therapy for ductal carcinoma in situ. Lancet Oncol 12:2–3. doi:10.1016/S1470-2045(10)70277-1
Hayward L, Oeppen RS, Grima AV, Royle GT, Rubin CM, Cutress RI (2011) The influence of clinicopathological features on the predictive accuracy of conventional breast imaging in determining the extent of screen-detected high-grade pure ductal carcinoma in situ. Ann R Coll Surg Engl 93:385–390. doi:10.1308/003588411X579829
Hofvind S, Iversen BF, Eriksen L, Styr BM, Kjellevold K, Kurz KD (2011) Mammographic morphology and distribution of calcifications in ductal carcinoma in situ diagnosed in organized screening. Acta Radiol 52:481–487. doi:10.1258/ar.2011.100357
Mansson E, Bergkvist L, Christenson G, Persson C, Warnberg F (2009) Mammographic casting-type calcifications is not a prognostic factor in unifocal small invasive breast cancer: a population-based retrospective cohort study. J Surg Oncol 100:670–674. doi:10.1002/jso.21405
Burnside ES, Ochsner JE, Fowler KJ, Fine JP, Salkowski LR, Rubin DL, Sisney GA (2007) Use of microcalcification descriptors in BI-RADS 4th edition to stratify risk of malignancy. Radiology 242:388–395. doi:10.1148/radiol.2422052130
Holland R, Hendriks JH (1994) Microcalcifications associated with ductal carcinoma in situ: mammographic-pathologic correlation. Semin Diagn Pathol 11:181–192
Poplack SP, Wells WA (1998) Ductal carcinoma in situ of the breast: mammographic-pathologic correlation. AJR Am J Roentgenol 170:1543–1549. doi:10.2214/ajr.170.6.9609171
Albonico G, Querzoli P, Ferretti S, Rinaldi R, Nenci I (1998) Biological profile of in situ breast cancer investigated by immunohistochemical technique. Cancer Detect Prev 22:313–318
Moon WK, Myung JS, Lee YJ, Park IA, Noh DY, Im JG (2002) US of ductal carcinoma in situ. Radiographics 22:269–280
Mesurolle B, El-Khoury M, Khetani K, Abdullah N, Joseph L, Kao E (2009) Mammographically non-calcified ductal carcinoma in situ: sonographic features with pathological correlation in 35 patients. Clin Radiol 64:628–636. doi:10.1016/j.crad.2008.12.013
Acknowledgments
We thank Stephanie Deming for assistance in editing of this manuscript.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rauch, G.M., Kuerer, H.M., Scoggins, M.E. et al. Clinicopathologic, mammographic, and sonographic features in 1,187 patients with pure ductal carcinoma in situ of the breast by estrogen receptor status. Breast Cancer Res Treat 139, 639–647 (2013). https://doi.org/10.1007/s10549-013-2598-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-013-2598-7