
Abstract
Amplification of chromosome 11q13 is commonly seen in breast carcinomas and candidate genes from this region include CCND1 and EMSY. Here, we investigate the prognostic significance of CCND1 and EMSY amplification in a large series of breast carcinomas and in BRCA1 and BRCA2 mutation positive breast cancers. Amplification of CCND1 and EMSY was assessed by fluorescent in situ hybridization. Both CCND1 and EMSY amplifications were associated with a significantly worse outcome in ER-positive patients treated with tamoxifen only, in contrast to nonamplified tumors (P = 8.55 × 10−4 and P = 8.35 × 10−5, respectively). In multivariable Cox models, which included standard prognostic markers, co-amplification of CCND1 and EMSY was significantly more predictive of outcome than was amplification of either gene alone or neither gene amplified in ER-positive tamoxifen-treated patients (P = 5.47 × 10−5). EMSY gene amplification was a significantly less common event in BRCA2 mutation carriers as compared to BRCA1 mutation carriers (9 versus 24%, respectively). In contrast, CCND1 amplification occurred at a similar frequency in both BRCA1 and BRCA2 breast cancers (22 versus 18%, respectively). In summary, co-amplification of CCND1 and EMSY identified a poor prognostic subset of ER-positive tamoxifen-treated patients. In addition, EMSY amplification occurred at a lower frequency in BRCA2 mutation carriers providing evidence to support EMSY amplification as a somatic surrogate for BRCA2 loss in sporadic breast cancer.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gene amplification is a common mechanism leading to the overexpression of oncogenes in human cancers. Some genomic regions are frequently amplified in tumors; an example is chromosomal band 11q13. Amplification of this region, spanning over 7 Mb, is commonly seen in breast, head and neck, lung and bladder cancer [1, 2]. In breast cancer, four distinct regions of amplification have been identified and these regions may independently be amplified as small amplicons, or part of larger amplicons, resulting in co-amplification of multiple oncogenes [3–5].
CCND1, the gene encoding for cyclin D1, has been the most studied oncogene on 11q13 and has long been thought of as a potential driver of this amplification event in breast cancer [5, 6]. Cyclin D1, an important regulator of the cell cycle, [7, 8] has been found amplified in 15–20% of breast cancers [4, 9, 10] and overexpressed in up to 80% of tumors [1, 5, 11, 12]. Amplification of CCND1 has also been associated with a poor prognosis in estrogen receptor positive breast cancers [13–15]. One possible mechanism by which overexpression of cyclin D1 could lead to a poor prognosis is by conferring resistance to endocrine therapy such as tamoxifen. A recent study has provided experimental evidence that cyclin D1 is required for tamoxifen-induced cell proliferation and growth of tamoxifen-resistant cells in vitro [16]. In addition, analysis of CCND1 amplification in a series of breast cancers randomized to 2 years of adjuvant tamoxifen or no treatment showed that CCND1 gene amplification was a strong independent predictor of tamoxifen response [17]. These results suggest that amplification of CCND1 may be a marker for identifying tumors in which tamoxifen may be having an agonistic effect.
Another candidate oncogene on 11q13 is p-21-activated kinase 1 (PAK1), a serine/threonine kinase, that has been found to regulate anchorage-independent growth, invasiveness and the abnormal organization of mitotic spindles of human breast cancer cells [18]. Amplification of PAK1 has been reported in breast [3] and ovarian cancers [19–21]. PAK1 has been shown to activate estrogen receptor alpha (ERα) by phosphorylation, leading to the upregulation of ER-regulated genes such as CCND1 [22]. In breast cancer, amplification of PAK1 has also been recently shown to be a predictor of tamoxifen resistance in ER-positive patients [23].
Chromosome 11q13 is a gene dense region and in addition to CCND1 and PAK1 several other genes have been implicated in this amplification event. One such gene is EMSY, a novel BRCA2 interacting protein, that has been found amplified in both breast [24] and ovarian cancers [20, 21]. Given the potential role for both CCND1 and PAK1 as predictors of tamoxifen response, we investigated the clinical significance of EMSY and CCND1 amplification in a large cohort of clinically annotated breast cancers. In addition, we also evaluated amplification of EMSY and CCND1 in breast carcinomas associated with known mutations in BRCA1 and BRCA2.
Materials and methods
Breast cancer TMA
The study cohort included 4,046 female patients with newly diagnosed, invasive breast cancer in British Columbia. The clinicopathological characteristics and the treatment strategies of the patients included in this study have previously been reported [25]. The median follow-up was 12.5 years and age at diagnosis was 60 years. All patients had been referred to the British Columbia Cancer Agency and staging, pathology, treatment and follow-up information were available. During the study era, 75% of breast cancer cases in the province were referred; nonreferred patients were generally elderly or treated by mastectomy without indications for adjuvant therapy. Abstracted clinical information included age, histology, grade, tumor size, number of involved axillary nodes, lymphatic or vascular invasion (LVI), ER status, type of local and initial adjuvant systemic therapy (AST), dates of diagnosis and first local, regional or distant recurrence and death. Representative areas of invasive carcinoma were selected and marked on the hematoxylin and eosin slides, and its corresponding tissue block to be sampled for the tissue microarray (TMA). A single core TMA was then assembled as previously described [20]. Fluorescent in situ hybridization (FISH) analysis was performed on 6 μm paraffin TMA sections.
FISH on TMAs
The EMSY probe was created from DNA isolated from the PAC clones B4, DJ18D12, and DJ85A11 (all PCR verified for exons 2 or 8 of EMSY) and was directly labeled with Spectrum Green by nick translation (Vysis, Downer’s Grove, Illinois). The EMSY probe was then combined with the commercially available Spectrum Aqua labeled centromeric probe, CEP11 (Vysis, Downer’s Grove, Illinois) and Spectrum Orange labeled CCND1 probe (Vysis, Downer’s Grove, Illinois). The FISH assay was performed as previously described [20]. The slides were co-denatured for 5 min at 73°C and hybridized for 18 h at 37°C on a HYBrite (Vysis, Downers Grove, Illinois). Posthybridization washes were done as previously described [20]. Slides were then counterstained with 4′,6-diamidino-2-phenylindole (DAPI). Automated analysis of FISH signals was performed using Metasystems™ automated image acquisition and analysis system, Metafer (Metasystems, Altlussheim, Germany). The average gene copy number for each probe was calculated and the amplification ratio was determined. The amplification ratio was calculated as a ratio between the average copy per tumor cell for each gene and the average copy number for centromere 11. An amplification ratio ≥ 1.5 was considered amplified. This definition of amplification has been used in several other studies and was used for this current study [20, 21, 24].
BRCA1, BRCA2 and non-BRCA1/2 familial breast cancers
The collection of these paraffin embedded breast cancers was a collaborative effort between Vancouver General Hospital (Vancouver, BC), Memorial University (St. John’s, Newfoundland), McGill University (Montreal, Quebec), Spanish National Cancer Research Centre (Madrid, Spain) and Lund University Hospital (Lund, Sweden). FISH for EMSY and CCND1 were successfully analyzed in 63 BRCA1 mutation carriers and 55 BRCA2 mutation carriers.
Results
Amplification of CCND1 and EMSY in a population-based cohort of breast carcinomas
To evaluate the amplification of CCND1 and EMSY, a three-color FISH assay was developed that included centromere 11 as a reference probe. FISH signals were successfully scored in 1,318 cases for both CCND1 and EMSY. There was no statistically significant difference in survival between the cases for which results were obtained and those cases with missing data (P = 0.088). Overall for the entire cohort, CCND1 was amplified in 397 (30%) of 1,318 cases, and EMSY was amplified in 191 (14.5%) of 1,318 cases. Amplification of CCND1 correlated significantly with EMSY amplification (P = 5.416 × 10−44), positive-ER status (P = 2.62 × 10−5) and Ki67 (P = 3.10 × 10−4). In addition, CCND1 amplification showed an inverse correlation with the basal subtype of breast cancer (P = 0.01). EMSY amplification showed only a significant correlation with CCND1 amplification (P = 5.416 × 10−44).
Amplification of CCND1 and EMSY and disease-specific survival (DSS)
When DSS was analyzed for patients with amplification of CCND1 and EMSY, associations with several clinicopathological variables were observed (Table 1). For all patients, amplification of CCND1 and EMSY identified a subset of patients associated with a poor prognosis compared to those patients without amplification (Fig. 1a, b). We were then interested in determining whether those patients with co-amplification of CCND1 and EMSY had a poorer outcome as compared to those patients with either CCND1 or EMSY amplified alone or neither amplified. As seen in Fig. 1c, those patients with co-amplification of both CCND1 and EMSY were associated with significantly poorer outcome versus neither gene amplified (log rank P value = 2.78 × 10−4) or versus either CCND1 or EMSY amplified (log rank P value 6.91 × 10−3).

DSS curve for a EMSY amplification in the entire cohort, b CCND1 amplification in the entire cohort and c co-amplification of CCND1 and EMSY in the entire cohort
Cox regression analysis was performed to estimate the hazard ratio for CCND1-amplified cases adjusted for standard clinicopathological variables including age at diagnosis, grade, tumor size, nodal status and Her2 status. CCND1 amplification remained a significantly independent prognostic variable in this model (P value = 0.017) (Supplementary Table 2). The same Cox regression analysis was performed for EMSY amplified cases, and EMSY amplification also remained a significant independent prognostic predictor in this model (P value = 1.53 × 10−3) (Supplementary Table 3). To investigate whether co-amplification of both CCND1 and EMSY were of greater prognostic value than amplification of either gene alone, another Cox regression analysis was performed. The univariable hazard ratios for each covariate in the model can be seen in Table 2. Co-amplification of CCND1 and EMSY remained a significantly independent prognostic variable in this model (P value = 4.62 × 10−4).
Prognostic value of CCND1 and EMSY within the tamoxifen-treated subset
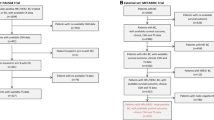
In British Columbia, patients are treated according to provincial guidelines developed by the BC Cancer Agency. To investigate the prognostic value of CCND1 and EMSY amplifications among ER-positive patients treated with tamoxifen only, and the additional effect of co-amplification of both genes, survival estimates were obtained for these subsets.
As seen in Table 1, those patients with amplification of CCND1 and EMSY were associated with a significantly poor outcome in ER-positive tamoxifen-treated patients (P = 0.008 and P = 0.001, respectively). We next determined whether those patients with co-amplification of CCND1 and EMSY were associated with a more adverse outcome in this subset of patients. Those patients with co-amplification of both genes were associated with a significantly adverse outcome in ER-positive tamoxifen-treated patients as compared to neither gene amplified (log rank P value = 5.6 × 10−5) or versus either gene amplified (long rank P value = 3.69 × 10−3) (Fig. 2a).

DSS curve for a co-amplification of CCND1 and EMSY in ER-positive tamoxifen-treated patients and b co-amplification of CCND1 and EMSY within the subset of patients who received no adjuvant systemic therapy
Cox regression analyses showed that amplification of both CCND1 and EMSY was of independent prognostic value in ER-positive tamoxifen-treated patients (P values = 8.55 × 10−4 and 8.35 × 10−5, respectively) (Supplementary Tables 4, 5). A third Cox model, when adjusted for standard clinicopathological variables, showed that co-amplification of both CCND1 and EMSY were associated with a significantly worse survival (P = 3.91 × 10−6) with a hazard ratio of 2.9 versus neither gene amplified (Table 3). In this subset of patients, co-amplification of both genes was the most significant prognosticator ahead of nodal status, grade and tumor size.
To further strengthen this finding, we also evaluated the prognostic significance of CCND1 and EMSY amplification within the subset patients who received no adjuvant systemic therapy (AST). No statistically significant difference in survival was seen in those patients with co-amplification of both genes versus neither gene amplified (log rank P value = 0.302) (Fig. 2b).
Amplification of CCND1 and EMSY in known BRCA1 and BRCA2 mutation carriers
We hypothesized that EMSY gene amplification would be a rare event in BRCA2 mutation carriers (as these cancers are already associated with a loss of BRCA2 function) and would be a frequent event in BRCA1 mutations carriers and familial breast cancers not associated with loss of either BRCA1 or BRCA2. To investigate this hypothesis, the same three-color FISH assay described above was performed on breast cancers associated with known BRCA1 and BRCA2 mutations. CCND1 was also included in this analysis as a control as, we expected to see similar levels of CCND1 amplification in all three subsets of familial breast cancer.
EMSY gene amplification was a frequent event in BRCA1 mutation carriers as expected (Table 4). In comparison, EMSY gene amplification was a significantly less common event in BRCA2 mutation carriers as compared to BRCA1 cases (P = 0.047). CCND1 amplification was a frequent event in both BRCA1 and BRCA2 breast cancers (Table 4).
Discussion
This is the first study to analyze both amplification of CCDN1 and EMSY in a large clinically annotated series of breast cancers. We found CCND1 and EMSY to be amplified in 30 and 15% of breast cancers, respectively. In addition, we also determined that patients with co-amplification of CCND1 and EMSY were associated with a significantly adverse outcome in ER-positive tamoxifen-treated patients. The findings were further strengthened in multivariate analyses, showing a ~threefold higher risk of dying of disease in tumors that were associated with co-amplification of CCND1 and EMSY. In this subset of patients, co-amplification of CCND1 and EMSY was the most significant prognosticator ahead of nodal status, tumor size and grade. These findings suggest that amplification of both CCND1 and EMSY may be a predictor of tamoxifen resistance in breast cancer.
Amplification of CCND1 has been well established in breast cancer, occurring at a frequency of 15–20%. CCND1 amplification has also been associated with a poor prognosis in estrogen receptor positive breast cancers [13–15]. In line with these studies, we have found a similar, although slightly higher, frequency of CCND1 amplification in our present study. One reason for this discrepancy could be the use of different cutoffs or methods used to determine gene amplification. However, all of these studies do confirm that CCND1 is a frequent target of gene amplification in breast cancer. We also confirm in the present study that amplification of CCND1 is associated with a poor prognosis in ER-positive breast cancers and in ER-positive tamoxifen-treated breast cancers as previously reported [17]. Amplification of EMSY, located ~6 Mb telomeric to CCND1, has also been commonly found amplified in breast cancer [24, 26]. The frequency of EMSY amplification found in this study is consistent with our previous findings [24]. Our findings are also consistent with a recent report, which found that EMSY amplification was associated with a decreased survival in ER-positive breast cancers [27].
Experimental studies have provided evidence to support a role for both CCND1 and PAK1 in tamoxifen response [16, 17, 23, 28]. It has been suggested that therapies targeting either CCND1 or PAK1 expression and/or activity may represent a novel strategy to increase endocrine response in breast cancer. Both CCND1 and PAK1 encode proteins that have been shown to activate ER [28], and increased expression of PAK1 has been shown to stimulate expression of CCND1. A recent study evaluating amplification of CCND1 and PAK1 in postmenopausal breast cancer patients randomized to tamoxifen treatment or no adjuvant therapy showed PAK1 amplification to be a better predictor of tamoxifen resistance than amplification of CCND1 [23].
The region of 11q13 contains numerous potential oncogenes, including CCND1, EMSY, PAK1, Rsf-1 and many others. We have recently demonstrated that the 11q13 amplicon is frequently amplified in ovarian cancer and is likely driven by a cassette of genes rather than by a single oncogene [21]. This is likely true for breast cancer, although different genes may be involved. In this current study, we have shown that CCND1 and EMSY, located less than 1 Mb centromeric to PAK1, are frequently amplified in breast cancer. Amplification of either gene alone is a strong independent prognostic indicator in both ER-positive breast cancers and in ER-positive tamoxifen-treated breast cancers. However, this effect on survival is even more pronounced when the two genes are co-amplified together. EMSY is a putative oncogene encoding a protein that interacts with the transactivation domain of BRCA2, and overexpression of a 5′ fragment of EMSY was found to induce chromosomal instability in normal human breast epithelial cells similar to that reported in BRCA2-deficient cells [21]. A role for EMSY in ER regulation has not been established. However, it is likely that amplification of several genes along the 11q13 amplicon may act in concert to drive amplification of this locus in breast cancer.
Lastly, we wanted to evaluate EMSY gene amplification in familial breast cancers associated with known mutations in BRCA1 and BRCA2. EMSY has been shown to interact with the transactivation domain of BRCA2. Mutations in BRCA1 and BRCA2 are rare events in sporadic breast cancer [29–31]. Although epigenetic silencing of BRCA1 has been reported in some sporadic cancers [32–36], no such silencing has been reported for BRCA2 [37–39]. It has been hypothesized that EMSY amplification may be a surrogate for BRCA2 loss in sporadic cancer [40, 41]. Therefore, mutations in BRCA2 may be unnecessary when EMSY is amplified and overexpressed. Indeed, we found that EMSY was less commonly amplified in BRCA2 mutation carriers (i.e., those cancers associated with loss of BRCA2 function) as compared to BRCA1 mutations carriers. Further evidence to support this association between EMSY and BRCA2 mutation carriers came from the parallel study of CCND1 gene amplification in these same subsets of familial breast cancers. Amplification of CCND1 was commonly observed at a similar frequency in BRCA1 and BRCA2 mutation carriers. Two studies have evaluated CCND1 gene amplification in BRCA1 mutation carriers, although they both yielded discordant results. One study reported that CCND1 was not amplified in 30 BRCA1 carcinomas [42], whereas another study reported CCND1 amplification in 2 of 11 (18%) cases [43]. The latter study found a frequency of amplification very similar to what we observed, although the number of BRCA1 cases was much smaller than the 63 cases of BRCA1 carcinomas we analyzed.
In summary, these results demonstrate that co-amplification of CCND1 and EMSY is associated with a poor prognosis in ER-positive tamoxifen-treated patients, and in multivariate analysis co-amplification of both genes was a very strong independent prognosticator. These findings suggest that in addition to CCND1 and PAK1, other genes commonly amplified on 11q13 like EMSY may also be a potential predictor of tamoxifen resistance in breast cancer. Larger clinical studies of patients randomized to tamoxifen treatment or no adjuvant therapy are needed to map the cassette of genes involved in this amplicon. It may be that the 11q13 amplicon in breast cancers is responsible for driving tumorigenesis through the activation of several oncogenes that provide a selective advantage for tumors cells that are resistant to the effects of tamoxifen. Lastly, we found EMSY gene amplification to be a less common event in BRCA2 mutation carriers as compared to BRCA1 mutation carriers, providing evidence to support the potential role of EMSY as a surrogate for BRCA2 loss in sporadic breast cancer.
References
Peters G, Fantl V, Smith R, Brookes S, Dickson C (1995) Chromosome 11q13 markers and D-type cyclins in breast cancer. Breast Cancer Res Treat 33(2):125–135
Schwab M (1998) Amplification of oncogenes in human cancer cells. Bioessays 20(6):473–479
Bekri S, Adelaide J, Merscher S, Grosgeorge J, Caroli-Bosc F, Perucca-Lostanlen D, Kelley PM, Pebusque MJ, Theillet C, Birnbaum D et al (1997) Detailed map of a region commonly amplified at 11q13–>q14 in human breast carcinoma. Cytogenet Cell Genet 79(1–2):125–131
Courjal F, Cuny M, Simony-Lafontaine J, Louason G, Speiser P, Zeillinger R, Rodriguez C, Theillet C (1997) Mapping of DNA amplifications at 15 chromosomal localizations in 1875 breast tumors: definition of phenotypic groups. Cancer Res 57(19):4360–4367
Karlseder J, Zeillinger R, Schneeberger C, Czerwenka K, Speiser P, Kubista E, Birnbaum D, Gaudray P, Theillet C (1994) Patterns of DNA amplification at band q13 of chromosome 11 in human breast cancer. Genes Chromosomes Cancer 9(1):42–48
Hui R, Ball JR, Macmillan RD, Kenny FS, Prall OW, Campbell DH, Cornish AL, McClelland RA, Daly RJ, Forbes JF et al (1998) EMS1 gene expression in primary breast cancer: relationship to cyclin D1 and oestrogen receptor expression and patient survival. Oncogene 17(8):1053–1059
Baldin V, Lukas J, Marcote MJ, Pagano M, Draetta G (1993) Cyclin D1 is a nuclear protein required for cell cycle progression in G1. Genes Dev 7(5):812–821
Ormandy CJ, Musgrove EA, Hui R, Daly RJ, Sutherland RL (2003) Cyclin D1, EMS1 and 11q13 amplification in breast cancer. Breast Cancer Res Treat 78(3):323–335
Champeme MH, Bieche I, Lizard S, Lidereau R (1995) 11q13 amplification in local recurrence of human primary breast cancer. Genes Chromosomes Cancer 12(2):128–133
Lammie GA, Peters G (1991) Chromosome 11q13 abnormalities in human cancer. Cancer Cells 3(11):413–420
Buckley MF, Sweeney KJ, Hamilton JA, Sini RL, Manning DL, Nicholson RI, deFazio A, Watts CK, Musgrove EA, Sutherland RL (1993) Expression and amplification of cyclin genes in human breast cancer. Oncogene 8(8):2127–2133
Gillett C, Fantl V, Smith R, Fisher C, Bartek J, Dickson C, Barnes D, Peters G (1994) Amplification and overexpression of cyclin D1 in breast cancer detected by immunohistochemical staining. Cancer Res 54(7):1812–1817
Bieche I, Olivi M, Nogues C, Vidaud M, Lidereau R (2002) Prognostic value of CCND1 gene status in sporadic breast tumours, as determined by real-time quantitative PCR assays. Br J Cancer 86(4):580–586
Michalides R, Hageman P, van Tinteren H, Houben L, Wientjens E, Klompmaker R, Peterse J (1996) A clinicopathological study on overexpression of cyclin D1 and of p53 in a series of 248 patients with operable breast cancer. Br J Cancer 73(6):728–734
Seshadri R, Lee CS, Hui R, McCaul K, Horsfall DJ, Sutherland RL (1996) Cyclin DI amplification is not associated with reduced overall survival in primary breast cancer but may predict early relapse in patients with features of good prognosis. Clin Cancer Res 2(7):1177–1184
Kilker RL, Planas-Silva MD (2006) Cyclin D1 is necessary for tamoxifen-induced cell cycle progression in human breast cancer cells. Cancer Res 66(23):11478–11484
Jirstrom K, Stendahl M, Ryden L, Kronblad A, Bendahl PO, Stal O, Landberg G (2005) Adverse effect of adjuvant tamoxifen in premenopausal breast cancer with cyclin D1 gene amplification. Cancer Res 65(17):8009–8016
Vadlamudi RK, Adam L, Wang RA, Mandal M, Nguyen D, Sahin A, Chernoff J, Hung MC, Kumar R (2000) Regulatable expression of p21-activated kinase-1 promotes anchorage-independent growth and abnormal organization of mitotic spindles in human epithelial breast cancer cells. J Biol Chem 275(46):36238–36244
Schraml P, Schwerdtfeger G, Burkhalter F, Raggi A, Schmidt D, Ruffalo T, King W, Wilber K, Mihatsch MJ, Moch H (2003) Combined array comparative genomic hybridization and tissue microarray analysis suggest PAK1 at 11q13.5-q14 as a critical oncogene target in ovarian carcinoma. Am J Pathol 163(3):985–992
Brown LA, Irving J, Parker R, Kim H, Press JZ, Longacre TA, Chia S, Magliocco A, Makretsov N, Gilks B et al (2006) Amplification of EMSY, a novel oncogene on 11q13, in high grade ovarian surface epithelial carcinomas. Gynecol Oncol 100(2):264–270
Brown LA, Kalloger SE, Miller MA, Shih I.e. M, McKinney SE, Santos JL, Swenerton K, Spellman PT, Gray J, Gilks CB et al (2008) Amplification of 11q13 in ovarian carcinoma. Genes Chromosomes Cancer 47(6):481–489
Balasenthil S, Barnes CJ, Rayala SK, Kumar R (2004) Estrogen receptor activation at serine 305 is sufficient to upregulate cyclin D1 in breast cancer cells. FEBS Lett 567(2–3):243–247
Bostner J, Ahnstrom Waltersson M, Fornander T, Skoog L, Nordenskjold B, Stal O (2007) Amplification of CCND1 and PAK1 as predictors of recurrence and tamoxifen resistance in postmenopausal breast cancer. Oncogene 26(49):6997–7005
Hughes-Davies L, Huntsman D, Ruas M, Fuks F, Bye J, Chin SF, Milner J, Brown LA, Hsu F, Gilks B et al (2003) EMSY links the BRCA2 pathway to sporadic breast and ovarian cancer. Cell 115(5):523–535
Cheang MC, Voduc D, Bajdik C, Leung S, McKinney S, Chia SK, Perou CM, Nielsen TO (2008) Basal-like breast cancer defined by five biomarkers has superior prognostic value than triple-negative phenotype. Clin Cancer Res 14(5):1368–1376
Rodriguez C, Hughes-Davies L, Valles H, Orsetti B, Cuny M, Ursule L, Kouzarides T, Theillet C (2004) Amplification of the BRCA2 pathway gene EMSY in sporadic breast cancer is related to negative outcome. Clin Cancer Res 10(17):5785–5791
Kirkegaard T, Nielsen KV, Jensen LB, Campbell FM, Muller S, Tovey SM, Brown S, Cooke TG, Bartlett JM (2008) Genetic alterations of CCND1 and EMSY in breast cancers. Histopathology 52(6):698–705
Holm C, Rayala S, Jirstrom K, Stal O, Kumar R, Landberg G (2006) Association between Pak1 expression and subcellular localization and tamoxifen resistance in breast cancer patients. J Natl Cancer Inst 98(10):671–680
Futreal PA, Liu Q, Shattuck-Eidens D, Cochran C, Harshman K, Tavtigian S, Bennett LM, Haugen-Strano A, Swensen J, Miki Y et al (1994) BRCA1 mutations in primary breast and ovarian carcinomas. Science 266(5182):120–122
Lancaster JM, Wooster R, Mangion J, Phelan CM, Cochran C, Gumbs C, Seal S, Barfoot R, Collins N, Bignell G et al (1996) BRCA2 mutations in primary breast and ovarian cancers. Nat Genet 13(2):238–240
Sorlie T, Andersen TI, Bukholm I, Borresen-Dale AL (1998) Mutation screening of BRCA1 using PTT and LOH analysis at 17q21 in breast carcinomas from familial and non-familial cases. Breast Cancer Res Treat 48(3):259–264
Baldwin RL, Nemeth E, Tran H, Shvartsman H, Cass I, Narod S, Karlan BY (2000) BRCA1 promoter region hypermethylation in ovarian carcinoma: a population-based study. Cancer Res 60(19):5329–5333
Catteau A, Harris WH, Xu CF, Solomon E (1999) Methylation of the BRCA1 promoter region in sporadic breast and ovarian cancer: correlation with disease characteristics. Oncogene 18(11):1957–1965
Esteller M, Silva JM, Dominguez G, Bonilla F, Matias-Guiu X, Lerma E, Bussaglia E, Prat J, Harkes IC, Repasky EA et al (2000) Promoter hypermethylation and BRCA1 inactivation in sporadic breast and ovarian tumors. J Natl Cancer Inst 92(7):564–569
Geisler JP, Hatterman-Zogg MA, Rathe JA, Buller RE (2002) Frequency of BRCA1 dysfunction in ovarian cancer. J Natl Cancer Inst 94(1):61–67
Rice JC, Ozcelik H, Maxeiner P, Andrulis I, Futscher BW (2000) Methylation of the BRCA1 promoter is associated with decreased BRCA1 mRNA levels in clinical breast cancer specimens. Carcinogenesis 21(9):1761–1765
Collins N, Wooster R, Stratton MR (1997) Absence of methylation of CpG dinucleotides within the promoter of the breast cancer susceptibility gene BRCA2 in normal tissues and in breast and ovarian cancers. Br J Cancer 76(9):1150–1156
Gras E, Cortes J, Diez O, Alonso C, Matias-Guiu X, Baiget M, Prat J (2001) Loss of heterozygosity on chromosome 13q12–q14, BRCA-2 mutations and lack of BRCA-2 promoter hypermethylation in sporadic epithelial ovarian tumors. Cancer 92(4):787–795
Hilton JL, Geisler JP, Rathe JA, Hattermann-Zogg MA, DeYoung B, Buller RE (2002) Inactivation of BRCA1 and BRCA2 in ovarian cancer. J Natl Cancer Inst 94(18):1396–1406
King MC (2004) A novel BRCA2-binding protein and breast and ovarian tumorigenesis. N Engl J Med 350(12):1252–1253
Livingston DM (2004) EMSY, a BRCA-2 partner in crime. Nat Med 10(2):127–128
Vaziri SA, Tubbs RR, Darlington G, Casey G (2001) Absence of CCND1 gene amplification in breast tumours of BRCA1 mutation carriers. Mol Pathol 54(4):259–263
Palacios J, Honrado E, Osorio A, Cazorla A, Sarrio D, Barroso A, Rodriguez S, Cigudosa JC, Diez O, Alonso C et al (2005) Phenotypic characterization of BRCA1 and BRCA2 tumors based in a tissue microarray study with 37 immunohistochemical markers. Breast Cancer Res Treat 90(1):5–14
Acknowledgments
Research funded by an operating grant from the CBCRI/CIHR awarded to DGH. DGH is a MSFHR senior scholar. The tissue microarray laboratory is supported by a research unit grant from the MSFHR and an unrestricted education grant from Sanofi-avenits Canada. We would like to thank Dr Ake Borg for contributing BRCA1 and BRCA2 mutation positive breast cancers for this study.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Brown, L.A., Johnson, K., Leung, S. et al. Co-amplification of CCND1 and EMSY is associated with an adverse outcome in ER-positive tamoxifen-treated breast cancers. Breast Cancer Res Treat 121, 347–354 (2010). https://doi.org/10.1007/s10549-009-0479-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-009-0479-x