
Abstract
Background The purpose of this retrospective study was to analyze the overall survival of patients with brain metastases due to breast cancer and to identify prognostic factors that affect clinical outcome. Methods Of the 7,872 breast cancer patients histologically diagnosed with breast cancer between January 1990 and July 2006 at the Asan Medical Center, 198 patients with solitary or multiple brain metastases were included in this retrospective study. Central nervous system (CNS) lesions were diagnosed by computed tomography (CT) or magnetic resonance imaging (MRI). Patients with leptomeningeal or dural metastases without co-existent parenchymal metastatic lesions were excluded in this study. We reviewed the medical records and pathologic data of these 198 patients to characterize the clinical features and outcomes. Results The median age of the patients at the diagnosis of brain metastases was 45 years (range 26–78 years). Fifty-five patients (28%) had a single brain metastasis, whereas 143 (72%) had more than two metastases. A total of 157 (79.2%) patients received whole-brain radiation therapy (WBRT). A total of 7 (3.6%) patients underwent resection of solitary brain metastases, 22 (11%) patients underwent gamma-knife surgery, three patients underwent intrathecal chemotherapy (1.5%) and 9 (4.6%) patients received no treatment. The overall median survival time was 5.6 months (95% confidence interval (CI), 4.7–6.5 months) and 23.1% of the patients survived for more than 1 year. The median overall survival time was 5.4 months for patients treated with WBRT, 14.9 months for patients treated with surgery or gamma-knife surgery only, and 2.1 months for patients who received no treatment (P < 0.001). Multivariate analysis demonstrated that Eastern Cooperative Oncology Group (ECOG) performance status (relative risk (RR) = 0.704, 95% CI 0.482–1.028, P = 0.069), number of brain metastases (RR = 0.682, 95% CI 0.459–1.014, P = 0.058), treatment modalities (RR = 1.686, 95% CI 1.022–2.781, P = 0.041), and systemic chemotherapy after brain metastases (RR = 1.871, 95% CI 1.353–2.586, P < 0.001) were independent factors associated with survival. Conclusion Although survival of breast cancer patients with brain metastases was generally short, the performance status, number of brain metastases, treatment modalities and systemic chemotherapy after brain metastases were significantly associated with survival. Patients with single-brain metastasis and good performance status deserve aggressive treatment. The characteristics of initial primary breast lesions did not affect survival after brain metastasis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Breast cancer is the second most common cause of brain metastases, with 10–20% of patients experiencing metastasis to the brain [1, 2]. Recently, however, a trend toward increased central nervous system (CNS) recurrence has been noted: increases of up to 25–34% [3–6] compared with historical rates of 10–20%, owing to the induction of more sensitive and accurate diagnostic methods, the development of improved adjuvant and palliative therapy regimens, and improved survival [7–9].
The median time from diagnosis of breast cancer to CNS metastasis has been reported to be 33 months [2, 10]. Brain metastasis is usually associated with aggressive tumor behavior, negative hormone-receptor status, a relatively young age (premenopausal), and the presence of lung and liver metastases. However, no conclusion can yet be drawn as to whether there is a specific biology that drives a tumor to preferentially metastasize to the brain, or whether the likelihood of brain metastases is simply related to a general metastatic potential.
The median survival of untreated patients may be as short as 1–2 months [2, 11, 12]. After whole-brain radiation therapy (WBRT), an increase in survival of 3–6 months has been reported [13–15]. WBRT is a well-established treatment modality that results in transitory amelioration of neurological deficits in 60–85% of patients. Despite the use of WBRT, however, the prognosis for patients with brain metastases remains poor, with median survival of only 3–6 months, and this figure has not changed over the past 25 years [2, 10, 16]. Selected patients with a small tumor burden, preferably a solitary brain metastasis that can be treated with surgery as well as radiotherapy, may exhibit extended survival [17].
Prognostic factors for the occurrence and clinical outcome of brain metastases remain to be identified. The present retrospective analysis was performed to contribute to our understanding of the natural history of brain metastases in breast cancer, to assess the prognostic significance of patient-related-factors and to evaluate the efficacy of various treatment modalities.
Patients and methods
Of the 7,872 patients histologically diagnosed with breast cancer between January 1990 and July 2006 at the Asan Medical Center, 198 patients with solitary or multiple brain metastases were included in this retrospective study. CNS lesions were diagnosed by computed tomography (CT) or magnetic resonance imaging (MRI) of the brain. Patients with leptomeningeal metastasis or dural metastases without parenchymal brain metastatic lesions were not included in this study. We reviewed the medical records and pathologic data of these 198 patients to summarize the clinicopathological characteristics and effects of different treatments. Performance status at time of diagnosis of brain metastases was estimated retrospectively using the Eastern Cooperative Oncology Group (ECOG) scale.
Categorical variables were compared using the χ2 test or Fisher’s exact test, where appropriate. The brain-metastasis-free interval was defined as the time from histological diagnosis of the primary breast lesion to the time of objective evidence of the brain metastasis. The time of brain metastasis was defined as that time when brain CT or MRI scan was taken. Overall survival time after brain metastasis was measured from the time of detection of the brain metastasis to the time of death or last follow-up. Univariate analysis was performed to identify prognostic factors for survival by modeling Kaplan-Meier survival curves, and the difference in survival was compared using the log-rank test. Multivariate analysis was performed using the Cox proportional hazards regression model. SPSS program (version 12.0) was used for all analysis, and a P-value less than 0.05 was considered statistically significant.
Results
Patient characteristics
Patient characteristics of the 198 breast cancer patients with brain metastases are presented in Table 1. The median age at diagnosis of brain metastasis was 45 years (range 26–78 years), and 151 (75.7%) had ECOG performance status 1 or 2. The brain was the first site of metastatic involvement with or without extracranial metastases in 62 patients (31%), the second in 74 patients (37%), and at least the third in 61 patients (31%). Brain metastases were solitary in 55 patients and multiple in 143 patients. The most common additional metastatic sites at time of diagnosis of brain metastases were the lungs (37.4%) and bones (35.4%).
Analysis of primary breast lesions showed that 61.6% were estrogen receptor (ER) 0–3 (scale of 7) and 20.7% were ER 4–7; 64.1% were progesterone receptor (PR) 0–3 (scale of 7) and 17.7% were PR 4–7; and 36.9% were human epidermal growth factor receptor-2 (HER-2/neu) expression 0–2+ and 34.3% were HER-2/neu expression 3+. Information about primary lesion size was available for 152 (76.8%) patients; of these, 120 (60.6%) had tumors of ≤5 cm. About 42% of these patients had fewer than three positive lymph nodes. A total of 29 patients (15%) received no adjuvant chemotherapy, 47 (24%) were treated with a CMF (cyclophosphamide, methotrexate, 5-fluorouracil) regimen, 48 (24%) with a CAF (cyclophosphamide, doxorubicin, 5-fluorouracil) regimen, 27 (14%) with an AC-based (doxorubicin/cyclophosphamide) regimen, and 29 (15%) with other regimens (Table 1).
Treatment modalities
Whole brain radiation, usually as primary treatment (75.3%), but also as WBRT after gamma-knife or surgery (4%), was administered to 157 (79.3%) patients. A total of 7 (3.6%) patients underwent resection of solitary brain metastases, 22 (11%) patients underwent gamma-knife surgery, three patients underwent intrathecal chemotherapy (1.5%), and 9 (4.6%) received no treatment.
Radiation treatment consisted of a total dose of 3,000 cGy administered in 10 daily fractions of 300 cGy over a period of 2 weeks. Almost all patients received dexamethasone after diagnosis, which was continued throughout subsequent treatment and then gradually tapered after completion of treatment depending on performance status.
Interval from primary breast tumor to brain metastasis and prognostic factor of survival
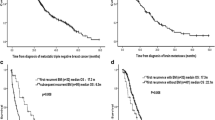
The cumulative incidence rates of brain metastases at 1, 3, and 5 years were 15.7%, 58.9%, and 81.7%, respectively. The median interval from primary diagnosis to brain metastases was 32.3 months. Overall median survival of the 198 patients was 5.6 months (95% CI 4.7–6.5 months), with only 23.1% of patients surviving for more than 1 year (Fig. 1). The patients with a long metastasis-free interval (>5 years) showed small and clinically no significant difference (9.8 months versus 5.3 months, P = 0.06, Fig. 2) in survival from diagnosis of brain metastases compared with those with a shorter metastasis-free interval (≤5 years).

Overall survival (OS) after brain metastasis

There was a difference in survival from diagnosis of brain metastasis (P = 0.06) between patients with a long metastasis-free interval (>5 years, dashed line) and patients with a shorter metastasis-free interval (≤5 years, solid line)
The time from primary diagnosis of breast cancer until diagnosis of brain metastasis and survival time were analyzed according to the patient and tumor characteristics (Table 2). Some of the primary tumor characteristics did affect the interval duration from primary tumor to brain metastasis; however, they had no effect on survival once brain metastasis occurred. Age less than 45 years was associated with a significantly shorter interval from primary diagnosis to brain metastasis compared with age more than 45 years. However, there was no difference in median survival between the two age groups: 5.6 and 5.5 months, respectively. An ER status of 0–3 and a PR status of 0–3 were associated with significantly shorter intervals from primary diagnosis to brain metastases compared with ER status 4–7 and PR status 4–7, respectively; however, there were no significant differences in median survival between the groups. HER-2-positive patients did not develop brain metastases earlier than HER-2-negative patients. Tumor size and lymph-node status of the primary lesion, both of which are known risk factors for distant dissemination, did not affect the time to brain metastasis or the survival from brain metastases. A high histology grade was associated with earlier brain metastases and a slightly but not significantly shorter survival. Lymphovascular invasion of the primary lesion did not affect the interval to brain metastasis. A total of 148 patients received adjuvant chemotherapy depending on the stage of the primary breast lesion. The intracranial metastases-free interval and median survival were not significantly different in the patients who received adjuvant chemotherapy compared with those who did not.
Patients with a good performance (ECOG performance status ≤2) had a median survival time of 6.5 months (range 0.1–44.6 months) after diagnosis of brain metastases, whereas patients with a poor performance (ECOG performance status ≥3) had a median survival of 3.2 months (range 0.1–20.2 months; P < 0.001).
Patients without extracranial metastases had a median survival of 9.0 months, whereas patients with extracranial metastases had a median survival of 5.3 months (P = 0.02). Patients with a solitary brain lesion had median survival of 9.2 months, which was significantly longer than the 5.3 month median survival time of patients with multiple brain lesions (P = 0.01). The median overall survival time was 5.4 months for patients who received WBRT-based therapy (WBRT or WBRT plus surgery/gamma-knife surgery), 14.9 months for patients who received surgery/gamma-knife surgery only, and 2.1 months for those who received no treatment (P < 0.001, Table 2, Fig. 3). The most common sites of extracranial disease were the lung, bone and liver. Univariate analyses revealed that patients with bone metastases at the time of brain metastases had shorter survival than patients with metastases at other sites (P = 0.02).

Overall survival for different treatment modalities: surgery/gamma-knife treatment (black dashed line, n = 29); whole brain radiation therapy (WBRT) (gray dashed line, n = 157); no treatment (black solid line, n = 9)
Multivariate analysis showed that ECOG performance status (RR = 0.704, 95% CI 0.482–1.028, P = 0.069), number of brain metastases (RR = 0.682, 95% CI 0.459–1.014, P = 0.058), treatment modalities (RR = 1.686, 95% CI 1.022–2.781, P = 0.041), and palliative systemic chemotherapy after brain metastases (RR = 1.871, 95% CI 1.353–2.586, P < 0.001, Table 3) were the only significant predictors for survival.
Brain metastases as initial site of recurrence
A total of 62 patients (31.3%) had brain metastasis as their first site of recurrence, and 21 of these patients had brain metastasis without extracranial disease. Of these 21 patients, 7 had solitary brain metastasis and 14 had multiple brain metastases. Of the seven patients with solitary brain metastasis, two had surgical resection, four had gamma-knife surgery without additional WBRT, and one patient had resection followed by WBRT. Of the 14 patients with multiple brain metastases, 12 received WBRT and 2 received gamma-knife treatment. Median survival was 19.3 months for the patients with solitary metastasis and 7.0 months for those with multiple brain metastases (Table 4, P = 0.008).
At the time of this analysis, 4 of the 7 patients with solitary brain metastasis were alive, (survival of 12.0, 13.2, 16.6 and 40.0 months). Three patients died; one of whom had a leptomeningeal relapse at 11.1 months and two who had brain relapses at 14 and 16 months, respectively.
Systemic treatment after brain metastases
About half of the patients received systemic chemotherapy with or without hormonal treatment after the diagnosis of brain metastases. The median survival was 7.8 months (range 0.1–28.7 months) in patients who received palliative chemotherapy versus 3.6 months (range 0.1–44.6 months) for those who did not (Fig. 4, P = 0.001).

Systemic chemotherapy after brain metastasis: palliative chemotherapy (black dashed line, n = 89), no treatment (black solid line, n = 104)
Discussion
In the present study, we retrospectively reviewed the clinical features and treatment of breast cancer patients with brain metastases. This is a single institutional study of Korean patients analyzing the clinical features, survival and prognostic factors of brain metastasis. The median age of the patients at the time of first diagnosis of brain metastases was 45 years. This was not unexpected because the median age of breast cancer at our institution for the period of 1989–2004 was 46 years, and it is well known that the peak incidence of breast cancer in Korea occurs at an earlier age than in western countries [18, 19]. The median interval from primary diagnosis to brain metastasis was 32.3 months, which is in agreement with previous reports [2, 10]. DiStefano et al. reported a median interval between primary diagnosis and CNS metastasis of 33 months.
Several small-scale studies have reported that young age [20, 21] and negative hormone receptor status [22–24] are the main risk factors for brain metastasis. Recently, Tham et al. reported a comparative analysis of risk factors in CNS metastasis patients (n = 383) compared with patients who had no CNS metastasis (n = 2302). They found that ER-negativity, young age, p53 mutation and EGFR, but not Her-2, overexpression were associated with increased risk. They also found that lymph-node status and adjuvant chemotherapy had little effect on the risk of brain metastasis [25]. Interestingly, of the above factors, only HER-2 status had an effect on survival after brain metastasis.
We did not perform a comparative analysis to identify the risk factors for brain metastasis compared with no brain metastasis. However, we did investigate characteristics that could have affected the tumor-free interval from primary breast cancer to brain metastasis, and we found that certain features such as young age, ER-negativity, PR-negativity, and high histology grade were associated with shorter intervals. These findings, indicating that certain factors are associated with increased risk of early brain metastasis, may have similar significance to the results of Tham et al. [25]. Also in agreement with the results of Tham et al., the tumor characteristics associated with a shorter interval to the development of brain metastasis did not affect survival.
In the present study, the overall median survival of the 198 patients was 5.6 months (95% CI 4.7–6.5 months), with only 23.1% of patients surviving for more than 1 year. Tham et al. reported that survival after CNS metastases was poor, with a median survival of 5.5 months, and only 25% of patients were alive at 1 year. Although their study included a large number of patients, they did not investigate whether performance status, the number of brain metastases or the treatment modality were prognostic indicators of survival. Lentzsch et al. used multivariate analysis to show that the performance status, number of brain metastases, dose of radiation and primary tumor size were prognostic factors for survival [26]. In the present study, patients with solitary metastasis also had a significantly better outcome than those with multiple metastases (9.2 months versus 5.3 months, respectively).
Certain treatment modalities seem to be associated with better outcome. The median overall survival time was 5.4 months for patients who received WBRT, 14.9 months for those who received surgery/gamma-knife treatment, and 2.1 months for those who received no treatment. However, this finding should be interpreted with care because the choices of treatment were highly correlated with, and dependent on, the disease status.
About half of the patients received systemic treatment such as palliative chemotherapy after the diagnosis of brain metastases. Patients who received systemic treatment after local treatment for brain lesion had a longer survival than the patients who did not: 7.8 months versus 3.6 months, respectively (P = 0.001). However, this finding warrants further prospective study.
In summary, we found that ECOG performance status, number of brain metastases, treatment modalities, and palliative systemic chemotherapy after brain metastasis were significantly associated with survival. The features of the primary breast lesion did not affect survival once brain metastasis had occurred; however, patients with solitary brain lesions should be managed aggressively.
References
Lee Y-T (1983) Breast carcinoma: pattern of metastasis at autopsy. J Surg Oncol 23:175–180
DiStefano A, Yap HY, Hortobagyi GN et al (1979) The natural history of breast cancer patients with brain metastases. Cancer 44:1913–1918
Bendell JC, Domchek SM, Burstein HJ et al (2003) Central nervous system metastases in women who receive trastuzumab-based therapy for metastatic breast carcinoma. Cancer 97:2972–2977
Shmueli E, Wigler N, Inbar M (2004) Central nervous system progression among patients with metastatic breast cancer responding to trastuzumab treatment. Eur J Cancer 40:379–382
Lower EE, Drosick DR, Blau R et al (2003) Increased rate of brain metastasis with trastuzumab therapy not associated with impaired survival. Clin Breast Cancer 4:114–119
Clayton AJ, Danson S, Jolly S et al (2004) Incidence of cerebral metastases in patients treated with trastuzumab for metastatic breast cancer. Br J Cancer 91:639–643
Crivellari D, Pagani O, Veronesi A et al (2001) High incidence of central nervous system involvement in patients with metastatic or locally advanced breast cancer treated with epirubicin and docetaxel. Ann Oncol 12:353–356
Kosmas C, Malamos NA, Tsavaris NB et al (2002) Leptomeningeal carcinomatosis after major remission to taxane-based front line therapy in patients with advanced breast cancer. J Neurooncol 56:265–273
Chock J, Domchek S, Burstein H et al (2002) Central nervous system (CNS) metastases in women who receive trastuzumab for metastatic breast cancer (MBC) [abstract]. Proc Am Soc Clin Oncol 21:55a
Chang EL, Lo S (2003) Diagnosis and management of central nervous system metastases from breast cancer. Oncologist 8:398–410
Coia LR (1992) The role of radiation therapy in the treatment of brain metastases. Int J Radiat Oncol Biol Phys 23:229–238
Gutin PH (1975) Corticosteroid therapy in patients with cerebral tumors: benefits, mechanisms, problems, practicalities. Semin Oncol 2:49–56
Posner J (1977) Management of central nervous system metastases. Semin Oncol 4:81–91
Pladdet I, Boven E, Nauta J et al (1989) Palliative care for brain metastases of solid tumour types. Neth J Med 34:10–21
Cairncross JG, Kim J-H, Posner JB (1980) Radiation therapy for brain metastases. Ann Neurol 7:529–541
Mahmoud-Ahmed AS, Suh JH, Lee SY et al (2002) Results of whole brain radiotherapy in patients with brain metastases from breast cancer: a retrospective study. Int J Radiat Oncol Biol Phys 54:810–817
Patchell RA, Tibbs PA, Walsh JW et al (1990) A randomized trial of surgery in the treatment of single metastases to the brain [see comments]. N Engl J Med 322:494–500
Ahn SH, Yoo KY, The Korean Breast Cancer Society (2006) Chronological changes of clinical characteristics in 31,115 new breast cancer patients among Koreans during 1996–2004. Breast Cancer Res Treat 99:209–214
Son BH, Kwak BS, Kim JK et al (2006) Changing patterns in the clinical characteristics of Korean patients with breast cancer during the last 15 years. Arch Surg 141:155–160
Tsukada Y, Fouad A, Pickren JW, Lane WW (1983) Central nervous system metastases from breast carcinoma: autopsy study. Cancer 52:2349–2354
Boogerd W, Vos VW, Hart AAM et al (1993) Brain metastases in breast cancer; natural history, prognostic factors, and outcome. J Neurooncol 15:165–174
Maki DD, Grossman RI (2000) Patterns of disease spread in metastatic breast carcinoma: influence of estrogen and progesterone receptor status. Am J Neuroradiol 21:1064–1066
Higashi H, Fukutomi T, Watanabe T et al (2000) Seven cases of breast cancer recurrence limited to the central nervous system without other visceral metastases. Breast Cancer 7:153–156
Samaan NA, Buzdar AU, Aldinger KA et al (1981) Estrogen receptor: a prognostic factor in breast cancer. Cancer 47:554–560
Tham Y-L, Sexton K, Kramer R et al (2006) Primary breast cancer phenotypes associated with propensity for central nervous system metastases. Cancer 107:696–704
Lentzsch S, Reichardt P, Weber F et al (1999) Brain metastases in breast cancer: prognostic factors and management. Eur J Cancer 35:580–585
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lee, S.S., Ahn, JH., Kim, M.K. et al. Brain metastases in breast cancer: prognostic factors and management. Breast Cancer Res Treat 111, 523–530 (2008). https://doi.org/10.1007/s10549-007-9806-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-007-9806-2