
Abstract
PON1 and PON2 have attracted considerable attention as candidate genes for coronary heart disease because their enzymes function as key factors in lipoprotein catabolism pathways. We studied the distribution of PON1 and PON2 polymorphisms, including genotyping, lipid profile, and PON1 activity, and their association with PON1 activity and significant coronary stenosis (SCS) in a Tunisian population. PON1 activity was lower in patients with SCS than in controls. It increased with the R allele (QQ < QR < RR) in PON1-192 genotypes and with the L allele (MM < ML < LL) in PON1-55 genotypes. In the presence of metabolic syndrome and diabetes, PON1-192RR and PON2-311CC were associated with an increased risk of SCS and PON1-55MM seems to have lower risk. This association was evident among nonsmokers for PON1-55MM and among smokers for PON1-192RR and PON2-311CC. The GTGC haplotype seemed to increase the risk of SCS compared with the wild haplotype in a Tunisian population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
High-density lipoprotein (HDL) has a well-established inverse relationship with coronary artery disease risk (Tsompanidi et al. 2010). The oxidative modification of low-density lipoprotein (LDL) is a key event in the initiation and acceleration of atherosclerosis (Aoki et al. 2012). As an antiatherogenic mediator, HDL, aside from playing an important role in reverse cholesterol transport, protects LDL against oxidation (Farmer and Liao 2011). The antioxidant effect of HDL is determined by its enzymes, in particular paraoxonase 1 (PON1), an HDL-associated enzyme capable of hydrolyzing lipid peroxides (Efrat and Aviram 2010).
The PON1 gene is clustered in tandem with PON2 and PON3 on the long arm of chromosome 7q21.3. Human PON enzymes, particularly PON1 and PON2, have been implicated in the pathogenesis of atherosclerosis (Précourt et al. 2011), and decreased PON activity has been documented in patients with coronary events (Mackness et al. 2003).
Studies have shown that PON1, which is expressed mainly in the liver, inhibits oxidation of LDL, preserves HDL function, increases cellular cholesterol efflux from macrophages, and decreases lipid peroxides in atherosclerotic lesions (Durrington et al. 2001). The antioxidant and anti-inflammatory properties of PON2, along with its intracellular localization, ubiquitous expression, and upregulation in times of oxidative stress, suggest an important physiological role for PON2 in host defense against atherosclerosis (Ng et al. 2006). Thus, PON2 plays a similar role to PON1 in the metabolism of lipids and lipoproteins (Mackness et al. 2002).
Several polymorphisms in the coding region of the PON1 and PON2 genes have been investigated in numerous studies for their association with coronary heart disease. The PON1 gene has two common polymorphisms, which lead to a glutamine/arginine substitution at position 192 (Q192R) and a leucine/methionine substitution at position 55 (L55M). PON2 also has two common polymorphic sites, which lead to an alanine/glycine substitution at position 148 (A148G) and a serine/cysteine substitution at position 311 (S311C) (Gupta et al. 2009). The association of these polymorphisms with increased risk for coronary heart disease was controversial (Shin et al. 2008; Pasdar et al. 2006).
Various population studies have reported interethnic differences in allele frequencies for the PON1 and PON2 polymorphisms. This variability suggests that ethnic differences, gene–gene interactions, and susceptibility to environmental factors might modulate the relationship between PON polymorphisms and coronary artery disease. Considering the important contribution of these polymorphisms to genetic susceptibility in atherosclerosis and the variability in allele frequencies among ethnic groups, the aim of the present study was to evaluate the distribution of the PON1 polymorphisms Q192R (rs662) and L55M (rs854560) and the PON2 polymorphisms A148G (rs12026) and S311C (rs7493) and to determine their association with PON1 activity and significant coronary stenosis (SCS) in a Tunisian population.
Materials and Methods
Study Population
The sampling procedures of this study have been described previously in detail (Rejeb et al. 2008). In brief, 316 study subjects underwent coronary angiography because of myocardial infarction (113 patients), angina (169), thoracic pain (18), or heart failure (16), in the Cardiology Department at Sahloul University Hospital, Sousse, Tunisia. The patients were subdivided into two groups, those with and those without SCS, defined as a luminal narrowing ≥50 % of at least one major coronary artery. Metabolic syndrome was defined according to the 2005 International Diabetes Federation definition (Alberti et al. 2005).
Data on lifestyle factors were collected using a questionnaire administered by an interviewer. With informed consent, the participants underwent physical examinations and laboratory tests. Height and weight were measured, and body mass index was calculated as weight in kilograms divided by the square of height in meters (kg/m2). Waist circumference was measured by a trained examiner from the narrowest point between the lower borders of the rib cage and the iliac crest. Blood pressure was measured in a sitting position after a 10 min rest period. Smoking was defined categorically as any positive or negative history of smoking. Hypertension was defined according to the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (Chobanian et al. 2003), and diabetes mellitus was diagnosed according to World Health Organization criteria (Alberti and Zimmet 1998). Patients taking lipid-lowering drugs were excluded. The study was approved by the local medical ethics committee.
Measurement of Lipid Profile
After overnight fasting and before coronary angiography, blood was collected from each subject. Serum total cholesterol, triglyceride, and HDL cholesterol concentrations were determined by a standard method using the Synchrom CX7 Clinical System (Beckman, Fullerton, CA, USA). When the triglyceride concentration was <4 mmol/L, LDL cholesterol concentration was calculated using the Friedewald formula (Friedewald et al. 1972). Otherwise, LDL cholesterol concentration was measured directly using the Synchrom CX7 Clinical System. Serum apolipoprotein (ApoAI and ApoB) concentrations were determined using the Immage Immunochemistry System (Beckman, Fullerton, CA, USA), based on immunonephelometric quantitation. ApoB/ApoAI and total/HDL cholesterol ratios were calculated.
Analysis of PON1 Activity
Serum PON1 activity was measured according to the modified method of Santanam and Parthasarathy (2007) using a Konelab 30 system. PON1 activity toward paraoxon was measured after paraoxon hydrolysis into p-nitrophenol and diethyl phosphate catalyzed by the enzyme. In brief, the activity was measured by adding 5 μL serum to freshly prepared Tris–NaOH buffer (0.26 M, pH 8.5) (Promega) containing 0.5 M NaCl (Fluka), 1.2 mM paraoxon (Sigma Aldrich), and 25 mM calcium chloride (Merck). After 30 s incubation at 37 °C, the liberation of p-nitrophenol was followed at 405 nm for 6 min.
DNA Extraction and Genotyping
Using a salting-out method (Miller et al. 1988), we extracted genomic DNA from whole blood samples treated with EDTA. The method established by Motti et al. (2001), with some modifications, was used to determine simultaneously the three common polymorphisms of the PON cluster (PON1-192, PON1-55, and PON2-311), using a multiplex polymerase chain reaction (PCR) DNA assay with mismatch primers to introduce a unique recognition site for the endonuclease HinfI in the PCR products in the presence of the R allele of PON1-192, of the L allele of PON1-55, and of the S allele of PON2-311.
Three pairs of mismatch primers for genotyping polymorphisms of codon 192 and codon 55 in the PON1 gene were used as described by Motti et al. (2001). The relevant primer sequences were, for PON1-192, 192-forward TTGAATGATATTGTTGCTGTGGGACCTGAG and 192-reverse CGACCACGCTAAACCCAAATACATCTCCCAGaA; for PON1-55, 55-forward GAGTGATGTATAGCCCCAGTTTC and 55-reverse AGTCCATTAGGCAGTATCTCCg; and for PON2-311, 311-forward GGTTCTCCGCATCCAGAACATTgaA and 311-reverse TGTTAAGaTATCGCACTaTCATGCC. (Lowercase italic letters indicate mismatched nucleotides.) This allowed a restriction site for HinfI (G/ANTC) to be introduced into the DNA amplification products in the presence of the polymorphisms arginine-PON1-192/leucine-PON1-55/serine-PON2-311.
The multiplex PCR was carried out using a DNA thermal cycler (LP×2 Thermal Cycler, Thermo Electron Corp., Milford, NE, USA). Each amplification was performed with 100 ng genomic DNA in a 30 μL volume containing 200 μM dNTPs, 2 mM MgCl2, 0.13 μM of both PON1-192 primers, 0.13 μM of both PON1-55 primers, 0.26 μM of both PON1-311 primers, and 2 U EuroTaq DNA polymerase (EuroClone, Italy). DNA was amplified with an initial step of 94 °C for 5 min; followed by 40 cycles of 1 min at 94 °C, 45 s at 55 °C, and 45 s at 72 °C; with a final extension step of 5 min at 72 °C. The multiplex PCR products were separated by electrophoresis on a 2 % agarose gel and visualized by ethidium bromide staining. Multiplex amplification products (15 μL) were digested with 2 U HinfI ((Promega, Madison, WI, USA) in a total volume of 20 μL at 37 °C for 24 h. The digested products were separated by electrophoresis on a 4 % agarose gel and visualized by ethidium bromide staining on a UV transilluminator.
The PON2-148 polymorphism was genotyped by PCR restriction fragment length polymorphism analysis. Primers for genotyping this polymorphism were used as described by Oliveira et al. (2004). The 20 μL reaction for the single PON2-148 amplification contained 0.1 μM each primer, 100 μM dNTPs, 1.5 mM MgCl2, and 1 U EuroTaq DNA polymerase (EuroClone). The PCR products of 232 base pairs (bp) PCR products were digested with 2 U Fnu4HI (New England BioLabs, Ipswich, MA, USA) at 37 °C for 24 h. Digested products were resolved by gel electrophoresis (4 % agarose gel) and visualized by ethidium bromide staining.
Statistical Analysis
Statistical analysis was performed by SPSS 16.0 for Windows. The biological variables were compared using one-way analysis of variance, then with Student’s t-test or Fisher’s exact test, and their values were reported as the mean ± standard deviation. A chi-square analysis was performed to determine Hardy–Weinberg equilibrium of each polymorphism studied in both groups with one degree of freedom. Genotype and allele frequencies were compared using a chi-square test. A single nucleotide polymorphism analyzer program (Yoo et al. 2005) was used to estimate linkage disequilibrium (LD) and to perform haplotype analyses. Pairwise LD coefficients were expressed as D′, which is the ratio of unstandardized coefficient to its minimal/maximal value. The odds ratio (OR) was calculated as a measure of the association of each PON genotype and haplotype with the phenotype. For each OR, the two-tailed p value and 95 % confidence interval (CI) were calculated; p was considered significant when it was <0.05. Adjusted ORs for potential confounders were determined using logistic regression analysis, and corresponding p values were reported.
Results
Population Characteristics
Patients with SCS had significantly lower HDL cholesterol (p = 0.040) and ApoAI (p = 0.009) concentrations, significantly higher triglyceride concentrations (p = 0.022), and a higher ApoB/ApoAI ratio (p = 0.036) than patients without SCS (Table 1). All variables with a p value <0.25 between the two groups were considered confounding factors for further OR adjustment.
Genotype Frequencies
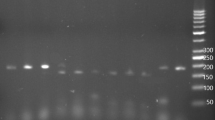
Based on the multiplex PCR with mismatch primers, the three PON polymorphisms could be identified simultaneously. The multiplex PCR amplification yielded products of 111 bp for PON1-192, 144 bp for PON1-55, and 196 bp for PON2-311. After incubation with HinfI, the presence of PON1-192R resulted in digestion of the 111 bp product into fragments of 77 and 34 bp, and the presence of PON1-55L resulted in digestion of the 144 bp product into fragments of 122 and 22 bp. The 196 bp product of PON2-311 was digested into 173 and 23 bp in the presence of the S allele. For PON2-148, the 232 bp product was digested into 161 and 71 bp in the presence of the A allele (Fig. 1).

Separation of (a) PON multiplex PCR products after digestion with HinfI by 4 % agarose gel electrophoresis. The combined genotypes (PON1-192, PON1-55, PON2-311) resulting from the analysis are (left to right) QQ-LM-CC; QR-MM-CS; RR-MM-CS; QQ-LL-SS. Separation of (b) single PCR products relative to the PON2-148 polymorphism after digestion with Fnu4HI by 4 % agarose gel electrophoresis. Genotype analysis (left to right), AG (three bands of 232, 161, and 71 bp), PON2-148, AA (two bands of 161 and 71 bp). M, 25 bp DNA Step Ladder (Promega). Length of digestion products is reported on the left
The polymorphisms of Q192R and L55M were distributed at the PON1 locus, and the S311C and A148G polymorphisms at the PON2 locus (Table 2). All genotypes, at each locus, followed Hardy–Weinberg equilibrium, with all chi-square values <3.84 and p > 0.05. The prevalence of homozygous individuals for the PON1-55M allele was higher in the group without SCS. Carriers of the PON2-311C allele were significantly higher in the SCS group. No mutated genotype for the PON2-148 polymorphism was found in the two groups. No difference in allele frequency was observed between the two groups for any polymorphism.
Associations Between PON1 and PON2 Polymorphisms, Lipid Profile, and PON1 Activity
In our study population, there was no difference in lipid profile among PON1 and PON2 polymorphisms (data not shown). We reported that PON1 activity was lower in the SCS group than in those without SCS; however, this difference was not statistically significant (307.041 ± 206.685 U I/L vs. 353.494 ± 200.392 U I/L, p = 0.571). The analyses of serum PON1 activity for PON1 and PON2 genotypes (Table 3) revealed statistically significant (P < 0.000) differences in PON1 activity among genotypes for the coding region polymorphisms, PON1-L55M and PON1-Q192R. The highest PON1 activities were detected in LL and RR genotypes, intermediate activities in LM and QR genotypes, and the lowest activities in MM and QQ genotypes. No difference was observed between PON1 activity and the two polymorphisms S311C and A148G of the PON2 gene.
Association of PON1 and PON2 Polymorphisms with the Presence of SCS
Odds ratios were calculated for SCS of variant genotypes of the PON polymorphisms (Table 4). After adjustment for confounding variables, the OR of SCS associated with the MM genotype of PON1-55 polymorphism was 0.668 (95 % CI 0.43–0.93; p = 0.042), suggesting that the MM genotype is associated with a 33 % lower risk of SCS. This protective effect seemed to be particularly significant in patients with metabolic syndrome (46 % lower risk; OR 0.556, 95 % CI 0.18–0.894; p = 0.035), in diabetic patients (64 % lower risk; OR 0.359, 95 % CI 0.14–0.94; p = 0.034), and in nonsmokers (35 % lower risk; OR 0.648, 95 % CI 0.36–0.95; p = 0.044). In the present study, we also reported that the RR genotype of the PON1-192 polymorphism and the CC of PON2-311 were associated with an increased risk of SCS (OR 1.83, 95 % CI 1.02–3.29, p = 0.043 for PON1-192RR; OR 1.76, 95 % CI 1.04–3.10, p = 0.035 for PON2-311CC), particularly in diabetics, smokers, and patients with metabolic syndrome (Table 4). No significant association was observed with the risk of SCS for the PON2-148 polymorphism and the PON1-192QR, PON1-55LM, PON2-311SC genotypes, either in the study population or based on smoking or diabetic status or the presence of metabolic syndrome.
Linkage Disequilibrium and Haplotype Analysis
In our population, significant LD was observed between PON1-55 and PON1-192 (D′ = −0.44, p < 0.000). Haplotype reconstruction for the four PON polymorphisms under study resulted in 14 haplotypes, possessing PON1-192 (A672G), PON1-55 (T260A), PON2-311 (C1053G), and PON2-148 (C564G) polymorphisms. We compared frequencies of different haplotypes with different ORs among patients with and without SCS (Table 5). When the four PON polymorphisms were combined, the GTGC haplotype model seemed to be the most atherogenic. It occurred more frequently in patients in the SCS group than in those without SCS (16.7 vs. 11 %; p = 0.028). In the haplotype analysis, after adjustment for confounding variables, the risk of SCS was higher in the GTGC haplotype than in the wild haplotype (possessing all common alleles: ATCC) (OR 1.58, 95 % CI 1.050-4.55; p = 0.039).
Discussion
The PON gene family has drawn much attention in recent years. In a series of association studies between PON1 and PON2 polymorphisms and coronary heart disease, the majority of the reports have revealed significant associations, although some exceptions exist. In the present study, the relationship of PON1-Q192R and -L55M polymorphisms and PON2-S311C and -A148G polymorphisms with lipid profile, PON1 activity, and SCS was investigated.
Associations Between PON1 and PON2 Polymorphisms, Lipid Profile, and PON1 Activity
This study found no association of the PON1 and PON2 genotypes with lipid profile (data not shown). Our results agree with many studies (Watzinger et al. 2002; Sen-Banerjee et al. 2000) but contradict others (Shin et al. 2008; Rios et al. 2007; Gluba et al. 2010). This inconsistency may be due to ethnic differences.
It has been shown that PON1 enzymatic activity is decreased in coronary heart disease patients (Mackness et al. 2003; Azarsiza et al. (2003). In our study, we report that PON1 activity was lower in the SCS group; however, this difference was not statistically significant. Our result is in agreement with Azarsiza et al. (2003) and Mackness et al. (2001).
Putative mechanisms leading to decreased PON1 activity could be the inactivation of enzyme by increased oxidative stress (Aviram et al. 1999). The decrease in PON1 activity could be the result of lower HDL concentrations in patients with coronary artery disease. Lipid peroxides, which are substrates for PON1 (Camps et al. 2009) and which have been shown to be raised in people with coronary artery disease, are inhibitors of PON1. The role of oxidative stress in decreased PON1 activity might be confirmed by the inverse association between lipid peroxidation and PON1 activity (Mackness et al. 2001).
Between individuals, PON1 activity varies approximately 10–40 fold. Part of this variability is explained by two polymorphisms of the PON1 gene. The R allele of the PON1-Q192R polymorphism has higher activity toward paraoxon hydrolysis than the Q allele (Humbert et al. 1993). Regarding lipid peroxidation, preliminary studies suggest that the R/R isoform is less effective in hydrolyzing lipid peroxides than the Q/Q isoform (Mackness et al. 1997; Regieli et al. 2009). On the other hand, the polymorphic site at position 55 (L/M) has been related with differences in PON1 activity, with higher activity for the 55L isoenzyme than for the 55M isoenzyme (Blatter-Garin et al. 1997). The L55M polymorphism occurs in the NH2-terminal region of the peptide, where a highly hydrophobic sequence may facilitate binding of PON to HDL (Brophy et al. 2000). In our study, we reported that significant association was found between both the PON1-192 and -55 polymorphisms and PON1 activity toward PON, which increased with the presence of the R allele (QQ < QR < RR) in the PON1-192 genotype and with the L allele (MM < ML < LL) in the PON1-55 genotype.
Association of PON1 and PON2 Polymorphisms with the Presence of SCS
The association of PON polymorphisms with cardiovascular events is a controversial issue. Our data show that the PON1-192RR genotype was associated with an increased risk of SCS (p = 0.043), consistent with the findings of some studies (Ranade et al. 2005; Gluba et al. 2010; Wang et al. 2011) but not others (Kaman et al. 2009; Bhattacharyya et al. 2008; Pasdar et al. 2006). Despite this high activity, atherogenicity of the PON1-192RR genotype may be explained by less ability to protect LDL from oxidative modification than the PON1-192QQ genotype (Aviram et al. 1999). We report that the PON1-55MM genotype is associated with a 33 % lower risk of SCS. Several reports showed similar results (Oliveira et al. 2004; Kaman et al. 2009); others did not (Can Demirdöğen et al. 2008; Arca et al. 2002). Concerning the PON2 gene, our study and other reports failed to show a significant role for the PON2-A148G variation in atherogenicity (Shin et al. 2008; Oliveira et al. 2004; Ranade et al. 2005). In contrast, Shin (2009) reported an association. Our result, in accordance with other studies (Jalilian et al. 2008; Yang et al. 2006), found that the PON2-311CC genotype was associated with increased risk of SCS. This association may be explained by a possible coding change in the PON2 gene, which could cause a change from serine to cysteine at the active site of PON2, impairing its antioxidation function and consequently changing the metabolic potency of the cell (Qu et al. 2008). However, controversies were found in many studies (Gluba et al. 2010; Guxens et al. 2008; Ranade et al. 2005). Inconsistent association of PON polymorphisms with coronary artery disease may be attributed to differences between studies in several factors, including ethnic factors, the type of population studied, dietary habits, and environmental differences.
Effect of Metabolic Syndrome, Diabetes, and Smoking Status
Because diabetic and metabolic syndrome patients are at greater risk of coronary heart disease and oxidative stress (Sentí et al. 2003; Mackness et al. 2000; Rejeb et al. 2010), we investigated the effect of PON polymorphisms on SCS in relation to these clinical conditions. There are many conflicting genetic results among such studies (Osei-Hyiaman et al. 2001; Martinelli et al. 2005; Ergun et al. 2011). We reported that the PON1-192RR and PON2-311CC genotypes were associated with an increased risk of SCS in diabetics and in patients with metabolic syndrome, and that the PON1-55MM genotype seems to have lower risk. Our results were in accordance with several studies (Aubó et al. 2000; Mackness et al. 2005).
In association with diabetes or metabolic syndrome, which increases peroxide formation, one may hypothesize that the R allele of PON1-192 and the C allele of PON2-311 may promote oxidative stress. This, in turn, might increase cardiovascular risk in diabetic or metabolic syndrome patients. In this context, it has been suggested that the L isoform of PON1-55 protects less well from oxidative stress than the M isoform (Mackness et al. 1997).
Like diabetes and metabolic syndrome, smoking is an established risk factor for coronary artery disease in which oxidative mechanisms play an important role. Thus, we studied the effect of smoking status on the association of these polymorphisms with SCS. According to Nishio and Watanabe (1997), cigarette smoke extract inhibits PON activity in a dose- and time-dependent manner. This inhibition might be caused by steric hindrance resulting from the introduction of a large substituent near a region of the molecule critical for substrate binding or the maintenance of an active enzyme conformation (Kuo and La Du 1995). We reported that the PON1-MM genotype was associated with lower risk in nonsmokers but not in smokers. Smokers may lack the protective effect of the MM genotype because cigarette smoke extract decreases PON activity against nonphysiological substrates (Nishio and Watanabe 1997), and it may also reduce PON1 activities that are involved in cardioprotection. Thus, the deleterious effects of cigarette smoke may equalize or outweigh the differences in potentially positive enzyme activities conferred by the PON1 genotype.
On the other hand, the PON1-192RR and PON2-311CC genotypes were associated with an increased risk of SCS in smokers. Our findings were similar to previous studies (Osei-Hyiaman et al. 2001; Martinelli et al. 2004), but not all (Sen-Banerjee et al. 2000; Rios et al. 2007). It is possible that these results can be explained by large amounts of free radicals in cigarette smoke (Church and Pryor 1985) and by lower antioxidative capacity of PON from the RR and CC genotypes (Princen et al. 1992), so that oxidized LDL particles from smokers with these genotypes generate more lipid peroxidation products than LDL from nonsmokers (Scheffler et al. 1992). In fact, cigarette extracts decrease PON activity from the RR and CC genotypes, which is initially less effective in hydrolyzing lipid peroxidation than that from the QQ and SS genotypes.
In haplotype analysis, after adjustment for confounding variables, the haplotype model of GTGC, with the polymorphisms PON1-192 (A672G), PON1-55 (T260A), PON2-311 (C1053G), and PON2-148 (C564G), seemed to increase the risk of SCS compared with the wild haplotype (possessing all common alleles, ATCC). Our result was confirmed by some studies (Kallel et al. 2010; Arca et al. 2002).
Some limitations of our study should be noted. We studied only four polymorphisms in the PON gene. It is possible that haplotype analysis with additional genotyping might increase the power to find these potential associations. In addition, the study population consisted of a relatively small number of subjects.
In conclusion, the PON1-192RR and -55LL genotypes increased PON1 activity. In the presence of metabolic syndrome and diabetes, PON1-192RR and PON2-311CC were associated with an increased risk of SCS, and PON1-55MM appears to be protective against SCS. This association was evident among nonsmokers for PON1-55MM and among smokers for PON1-192RR and PON2-311CC. The haplotype GTGC was associated with an atherogenic effect.
References
Alberti KG, Zimmet PZ (1998) Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med 15:539–553
Alberti KG, Zimmet P, Shaw J (2005) The metabolic syndrome: a new worldwide definition. Lancet 366:1059–1062
Aoki T, Abe T, Yamada E, Matsuto T, Okada M (2012) Increased LDL susceptibility to oxidation accelerates future carotid artery atherosclerosis. Lipids Health Dis 11:4
Arca M, Ombres D, Montali A, Campagna F, Mangieri E, Tanzilli G, Campa PP, Ricci G, Verna R, Pannitteri G (2002) PON1 L55M polymorphism is not a predictor of coronary atherosclerosis either alone or in combination with Q192R polymorphism in an Italian population. Eur J Clin Invest 32:9–15
Aubó C, Sentí M, Marrugat J, Tomás M, Vila J, Sala J, Masiá R (2000) Risk of myocardial infarction associated with Gln/Arg 192 polymorphism in the human paraoxonase gene and diabetes mellitus The regicor investigators. Eur Heart J 21:33–38
Aviram M, Rosenblat M, Billecke S, Erogul J, Sorenson R, Bisgaier CL (1999) Human serum paraoxonase (PON1) is inactivated by oxidized low-density lipoprotein and preserved by antioxidants. Free Radic Biol Med 26:892–904
Azarsiza E, Kayikcioglu M, Payzinb S, Sözmen EY (2003) PON1 activities and oxidative markers of LDL in patients with angiographically proven coronary artery disease. Int J Cardiol 91:43–51
Bhattacharyya T, Nicholls SJ, Topol EJ, Zhang R, Yang X, Schmitt D, Fu X, Shao M, Brennan DM, Ellis SG, Brennan ML, Allayee H, Lusis AJ, Hazen SL (2008) Relationship of paraoxonase 1 (PON1) gene polymorphisms and functional activity with systemic oxidative stress and cardiovascular risk. JAMA 299:1265–1276
Blatter-Garin MC, James RW, Dussoix P, Blanché H, Passa P, Froguel P, Ruiz J (1997) Paraoxonase polymorphism Met-Leu54 is associated with modified serum concentrations of the enzyme: a possible link between the paraoxonase gene and increased risk of cardiovascular disease in diabetes. J Clin Invest 99:62–66
Brophy VH, Jarvik GP, Richter RJ, Rozek LS, Schellenberg GD, Furlong CE (2000) Analysis of paraoxonase (PON1) L55M status requires both genotype and phenotype. Pharmacogenetics 10:453–460
Camps J, Marsillach J, Joven J (2009) Measurement of serum paraoxonase-1 activity in the evaluation of liver function. World J Gastroenterol 28:1929–1933
Can Demirdöğen B, Türkanoğlu A, Bek S, Sanisoğlu Y, Demirkaya S, Vural O, Arinç E, Adali O (2008) Paraoxonase/arylesterase ratio, PON1 192Q/R polymorphism and PON1 status are associated with increased risk of ischemic stroke. Clin Biochem 41:1–9
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, Jones DW, Materson BJ, Oparil S, Wright JT Jr, Roccella EJ (2003) Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. JAMA 289:2560–2572
Church DF, Pryor WA (1985) The free radical chemistry of cigarette smoke and its toxicological implications. Environ Health Perspect 64:111–126
Durrington PN, Mackness B, Mackness MI (2001) Paraoxonase and atherosclerosis. Arterioscler Thromb Vasc Biol 21:473–480
Efrat M, Aviram M (2010) Paraoxonase 1 interactions with HDL, antioxidants and macrophages regulate atherogenesis: a protective role for HDL phospholipids. Adv Exp Med Biol 660:153–166
Ergun MA, Yurtcu E, Demirci H, Ilhan MN, Barkar V, Yetkin I, Menevse A (2011) PON1 55 and 192 gene polymorphisms in type 2 diabetes mellitus patients in a Turkish population. Biochem Genet 49:1–8
Farmer JA, Liao J (2011) Evolving concepts of the role of high-density lipoprotein in protection from atherosclerosis. Curr Atheroscler Rep 13:107–114
Friedewald WT, Levy RI, Fredrickson DS (1972) Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 18:499–502
Gluba A, Pietrucha T, Banach M, Piotrowski G, Rysz J (2010) The role of polymorphisms within paraoxonases (192 Gln/Arg in PON1 and 311Ser/Cys in PON2) in the modulation of cardiovascular risk: a pilot study. Angiology 61:157–165
Gupta N, Gill K, Singh S (2009) Paraoxonases: structure, gene polymorphism and role in coronary artery disease. Indian J Med Res 130:361–368
Guxens M, Tomás M, Elosua R, Aldasoro E, Segura A, Fiol M, Sala J, Vila J, Fullana M, Sentí M, Vega G, de la Rica M, Marrugat J (2008) Association between paraoxonase-1 and paraoxonase-2 polymorphisms and the risk of acute myocardial infarction. Investigadores del estudio Iberica. Rev Esp Cardiol 61:269–275
Humbert R, Adler DA, Disteche CK, Hassett C, Omiecinski CJ, Furlong CE (1993) The molecular basis of the human serum paraoxonase activity polymorphism. Nat Genet 3:73–76
Jalilian A, Javadi E, Akrami M, Fakhrzadeh H, Heshmat R, Rahmani M, Bandarian F (2008) Association of cys 311 ser polymorphism of paraoxonase-2 gene with the risk of coronary artery disease. Arch Iran Med 11:544–549
Kallel A, Sediri Y, Sbaï MH, Mourali MS, Feki M, Elasmi M, Taieb SH, Sanhaji H, Souheil O, Mechmeche R, Jemaa R, Kaabachi N (2010) The paraoxonase L55M and Q192R gene polymorphisms and myocardial infarction in a Tunisian population. Clin Biochem 43:1461–1463
Kaman D, Ilhan N, Metin K, Akbulut M, Ustündağ B (2009) A preliminary study of human paraoxonase and PON 1 L/M 55–PON 1 Q/R 192 polymorphisms in Turkish patients with coronary artery disease. Cell Biochem Funct 27:88–92
Kuo CL, La Du BN (1995) Comparison of purified human and rabbit serum paraoxonases. Drug Metab Dispos 23:935–944
Mackness MI, Arrol S, Mackness B, Durrington PN (1997) Alloenzymes of paraoxonase and effectiveness of high-density lipoproteins in protecting low-density lipoprotein against lipid peroxidation. Lancet 349:851–852
Mackness B, Durrington PN, Abuashia B, Boulton AJM, Mackness MI (2000) Low paraoxonase activity in type II diabetes mellitus complicated by retinopathy. Clin Sci 98:355–363
Mackness B, Davies GK, Turkie W, Lee E, Roberts DH, Hill E, Roberts C, Durrington PN, Mackness MI (2001) Paraoxonase status in coronary heart disease: are activity and concentration more important than genotype? Arterioscler Thromb Vasc Biol 21:1451–1457
Mackness B, Durrington PN, Mackness MI (2002) The paraoxonase gene family and coronary heart disease. Curr Opin Lipidol 13:357–362
Mackness B, Durrington P, McElduff P, Yarnell J, Azam N, Watt M, Mackness M (2003) Low paraoxonase activity predicts coronary events in the Caerphilly Prospective Study. Circulation 107:2775–2779
Mackness B, McElduff P, Mackness MI (2005) The paraoxonase-2-310 polymorphism is associated with the presence of microvascular complications in diabetes mellitus. J Intern Med 258:363–368
Martinelli N, Girelli D, Olivieri O, Stranieri C, Trabetti E, Pizzolo F, Friso S, Tenuti I, Cheng S, Grow MA, Pignatti PF, Corrocher R (2004) Interaction between smoking and PON2 Ser311Cys polymorphism as a determinant of the risk of myocardial infarction. Eur J Clin Invest 34:14–20
Martinelli N, Girelli D, Olivieri O, Cavallari U, Biscuola M, Trabetti E, Friso S, Pizzolo F, Tenuti I, Bozzini C, Villa G, Ceradini B, Sandri M, Cheng S, Grow MA, Pignatti PF, Corrocher R (2005) Interaction between metabolic syndrome and PON1 polymorphisms as a determinant of the risk of coronary artery disease. Clin Exp Med 5:20–30
Miller SA, Dykes DD, Polesky HF (1988) A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res 16:1215
Motti C, Dessì M, Gnasso A, Irace C, Indigeno P, Angelucci CB, Bernardini S, Fucci G, Federici G, Cortese C (2001) A multiplex PCR-based DNA assay for the detection of paraoxonase gene cluster polymorphisms. Atherosclerosis 158:35–40
Ng CJ, Bourquard N, Grijalva V, Hama S, Shih DM, Navab M, Fogelman AM, Lusis AJ, Young S, Reddy ST (2006) Paraoxonase-2 deficiency aggravates atherosclerosis in mice despite lower apolipoprotein-B-containing lipoproteins: anti-atherogenic role for paraoxonase-2. J Biol Chem 281:29491–29500
Nishio E, Watanabe Y (1997) Cigarette smoke extract inhibits plasma paraoxonase activity by modification of the enzyme’s free thiols. Biochem Biophys Res Commun 236:289–293
Oliveira SA, Mansur AP, Ribeiro CC, José Ramires AF, Annichino-Bizzacchi JM (2004) PON1M/L55 mutation protects high-risk patients against coronary artery disease. Int J Cardiol 94:73–77
Osei-Hyiaman D, Hou L, Mengbai F, Zhiyin R, Zhiming Z, Kano K (2001) Coronary artery disease risk in Chinese type 2 diabetics: is there a role for paraxonase 1 gene (Q192R) polymorphism? Eur J Endocrinol 144:639–644
Pasdar A, Ross-Adams H, Cumming A, Cheung J, Whalley L, St Clair D, MacLeod MJ (2006) Paraoxonase gene polymorphisms and haplotype analysis in a stroke population. BMC Med Genet 7:28
Précourt LP, Amre D, Denis MC, Lavoie JC, Delvin E, Seidman E, Levy E (2011) The three-gene paraoxonase family: physiologic roles, actions and regulation. Atherosclerosis 214:20–36
Princen HMG, van Poppel G, Vogelezang C, Buytenhek R, Kok FJ (1992) Supplementation with vitamin E but not b-carotene in vivo protects low density lipoprotein from lipid peroxidation in vitro: effect of cigarette smoking. Arterioscler Thromb 12:554–562
Qu Y, Yang Z, Jin F, Sun L, Zhang C, Ji L, Sun H, Wang B, Wang L (2008) The Ser311Cys variation in the paraoxonase 2 gene increases the risk of type 2 diabetes in northern Chinese. J Genet 87:165–169
Ranade K, Kirchgessner TG, Iakoubova OA, Devlin JJ, DelMonte T, Vishnupad P, Hui L, Tsuchihashi Z, Sacks FM, Sabatine MS, Braunwald E, White TJ, Shaw PM, Dracopoli NC (2005) Evaluation of the paraoxonases as candidate genes for stroke: Gln192Arg polymorphism in the paraoxonase 1 gene is associated with increased risk of stroke. Stroke 36:2346–2350
Regieli JJ, Jukema JW, Doevendans PA, Zwinderman AH, Kastelein JJ, Grobbee DE, van der Graaf Y (2009) Paraoxonase variants relate to 10-year risk in coronary artery disease impact of a high-density lipoprotein-bound antioxidant in secondary prevention. J Am Coll Cardiol 54:1238–1245
Rejeb J, Omezzine A, Rebhi L, Naffeti I, Kchok K, Belkahla R, Bel Hadjmbarek I, Ben Rejeb N, Nabli N, Boujelbene A, Ben Abdelaziz A, Boughzala E, Bouslama A (2008) Association of the cholesteryl ester transfer protein Taq1 B2B2 genotype with higher high-density lipoprotein cholesterol concentrations and lower risk of coronary artery disease in a Tunisian population. Arch Cardiovasc Dis 101:629–636
Rejeb J, Omezzine A, Boumaiza I, Rebhi L, Kalboussi N, Laouini A, Rejeb NB, Nabli N, Abdelaziz AB, Boughzala E, Bouslama A (2010) Metabolic syndrome is a risk factor for coronary artery disease in a Tunisian population. Metab Syndr Relat Disord 8:105–112
Rios DL, D’Onofrio LO, Cerqueira CC, Bonfim-Silva R, Carvalho HG, Santos-Filho A, Galvão-Castro B (2007) Paraoxonase 1 gene polymorphisms in angiographically assessed coronary artery disease: evidence for gender interaction among Brazilians. Clin Chem Lab Med 45:874–878
Santanam N, Parthasarathy S (2007) Aspirin is a substrate for paraoxonase-like activity: implications in atherosclerosis. Atherosclerosis 191:272–275
Scheffler E, Wiest E, Woehrle J, Otto I, Schulz I, Huber L, Ziegler R, Dresel HA (1992) Smoking influences the atherogenic potential of low-density lipoprotein. Clin Invest Med 70:263–268
Sen-Banerjee S, Siles X, Campos H (2000) Tobacco smoking modifies association between Gln-Arg192 polymorphism of human paraoxonase gene and risk of myocardial infarction. Arterioscler Thromb Vasc Biol 20:2120–2126
Sentí M, Tomás M, Fitó M, Weinbrenner T, Covas MI, Sala J, Masiá R, Marrugat J (2003) Antioxidant paraoxonase 1 activity in the metabolic syndrome. J Clin Endocrinol Metab 88:5422–5426
Shin BS (2009) Paraoxonase gene polymorphism in southwestern Korean population. J Korean Med Sci 24:561–566
Shin BS, Oh SY, Kim YS, Kim KW (2008) The paraoxonase gene polymorphism in stroke patients and lipid profile. Acta Neurol Scand 117:237–243
Tsompanidi EM, Brinkmeier MS, Fotiadou EH, Giakoumi SM, Kypreos KE (2010) HDL biogenesis and functions: role of HDL quality and quantity in atherosclerosis. Atherosclerosis 208:3–9
Wang M, Lang X, Zou L, Huang S, Xu Z (2011) Four genetic polymorphisms of paraoxonase gene and risk of coronary heart disease: a meta-analysis based on 88 case–control studies. Atherosclerosis 214:377–385
Watzinger N, Schmidt H, Schumacher M, Schmidt R, Eber B, Fruhwald FM, Zweiker R, Kostner GM, Klein W (2002) Human paraoxonase 1 gene polymorphisms and the risk of coronary heart disease: a community-based study. Cardiology 98:116–122
Yang X, Gao Y, Zhou J, Zhen Y, Yang Y, Wang J, Song L, Liu Y, Xu H, Chen Z, Hui R (2006) Plasma homocysteine thiolactone adducts associated with risk of coronary heart disease. Clin Chim Acta 364:230–234
Yoo J, Seo B, Kim Y (2005) SNPAnalyzer: a web-based integrated work-bench for single-nucleotide polymorphism analysis. Nucleic Acids Res 33:483–488
Acknowledgments
This study was supported by grants from the Tunisian Ministry of Higher Education, Scientific Research, and Technology and the Tunisian Ministry of Health (UR 28/04); without their extremely generous and strong support, this study could not have been undertaken. We are especially grateful to the study participants. We acknowledge the excellent technical assistance of members of the Biochemistry and Cardiology Departments of Sahloul University Hospital.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rejeb, J., Omezzine, A., Rebhi, L. et al. Association of PON1 and PON2 Polymorphisms with PON1 Activity and Significant Coronary Stenosis in a Tunisian Population. Biochem Genet 51, 76–91 (2013). https://doi.org/10.1007/s10528-012-9544-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10528-012-9544-y