
Abstract
To determine the relationship between the genetic and environmental risk factors for common internalizing psychopathology (IP) and mental well-being (MWB), we examined detailed measures of emotional, social and psychological well-being, and a history of major depression (MD), generalized anxiety disorder (GAD) and panic attacks in the last year, in 1,386 twins from same-sex pairs from the MIDUS national USA sample assessed in 1995 and then again in 2005. Statistical analyses were performed with the Mx program. In the 1995 data, the best fit model contained one substantially heritable common factor for MD, GAD and panic attacks, and one strongly heritable common factor for the three well-being measures. Genetic and environmental risk factors for IP accounted for, respectively, 50 and 5%, of the genetic and environmental influences on MWB. We then constructed, using 1995 and 2005 data, two common factors that reflected temporally stable influences on (i) MD and GAD, and (ii) on emotional and psychological well-being. Genetic and environmental risk factors for the stable liability to IP accounted for 41 and 29% of the stable genetic and environmental influences, respectively, on MWB. This study suggests that genetic risk factors for IP make up 41–50% of the genetic influences on MWB. The overlap of environmental risk factors is more modest. Although low levels of IP on average reflect a high genetic propensity for MWB, other independent genetic influences play an important role in producing good mental health.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
A wide range of family, twin and adoption studies support an important role for genetic factors in the etiology of the common internalizing psychiatric syndromes of major depression (Kendler et al. 2006; Sullivan et al. 2000) and the anxiety disorders (Hettema et al. 2001), and suggest that these genetic risk factors are closely inter-related (Kendler et al. 2003; Kendler et al. 2010). For convenience, we will here consider these disorders as manifestations of “Internalizing Psychopathology” (IP). Many studies have examined the role of genetic influences on various measures of well-being (e.g., happiness or life satisfaction) generally, and mental well-being (MWB) in particular (Lykken and Tellegen 1996; Nes et al. 2006; Roysamb et al. 2003; Stubbe et al. 2005), and have consistently found modest to moderate levels of heritability. These two sets of findings lead to an obvious question: What is the relationship between the genetic influences on IP and on MWB? This question is of interest because it sheds light on the degree to which, from a genetic perspective, mental health reflects something positive in its own right versus simply the absence of high risk for mental illness.
Prior studies have, in the general population, consistently found that measures of IP and MWB are moderately and inversely inter-related with correlations typically in the range of −0.40 to −0.60, suggesting that measures of positive mental health and psychiatric disorders belong to separable but correlated dimensions (Keyes 2002; Keyes 2005). This moderate phenotypic association of IP and MWB indicates that the absence of symptoms of IP does not imply the presence of good mental health for many individuals in the population. This article attempts to understand the causes of this phenotypic relationship between IP and MWB. Specifically, we evaluate three hypotheses for the inter-relationship of genetic influences on IP and MWB.
First, the inter-relationship could be very modest. Genetic influences on IP could have little or no impact on MWB. Second, consistent with the phenotypic results, this relationship could be moderate. High levels of MWB could, on average, reflect both low genetic risk for IP and a substantial contribution of other independent genetic influences that predispose to healthy psychological functioning. Third, the inter-relationship could be very strong so that from a genetic perspective, high levels of MWB would simply reflect low levels of liability to IP.
Twin studies of both IP and MWB have also demonstrated the importance of environment influences. A parallel set of questions could therefore be asked about the relationship between environmental risk factors for IP and MWB. Are the two sets of environmental exposures largely unrelated (as would occur if most depressogenic or anxiogenic environments did not strongly impact on MWB) or are they strongly and negative correlated (as would be expected if environmental experiences that predisposed to high levels of MWB were also strongly protective against IP)?
We address these questions, for the first time to our knowledge, in a nationally representative USA twin sample that includes a comprehensive assessment of MWB which measures both happiness (e.g., positive affect or emotional well-being) and the Aristotelian concept of eudaimonia (i.e., doing well or flourishing in terms of psychological and social well-being (Keyes 2002; Keyes 2005; Keyes 2007)). Our assessment of IP consists of DSM-IV major depression (MD), generalized anxiety disorder (GAD), and panic attacks (PA) in the last year. Furthermore, this twin sample was assessed twice over a 10 year period, permitting us to examine the inter-relationship between the temporally stable components of the vulnerability to IP and MWB.
Methods
Sample
About 50,000 households that were representative of the USA population were screened by telephone to determine if they knew of immediate relatives who were members of twin pairs. Inclusion criteria included being first-degree relatives of the original contact or the contact’s partner, being between 25 and 74 years old at the time of recruitment, living in the continental USA, being reachable by telephone, and being fluent in English. A total of 14.8% of screened households had twin pairs, of which 60% gave permission for the twins to be contacted for study recruitment. Zygosity was determined using self-report questions shown to give greater than 90% accuracy in zygosity diagnosis (Lykken et al. 1990). The racial, ethnic composition of the same-sex twin sample was 84.7% White (non-Hispanic) in 1995 and 89.7% in 2005, 4.4% Black in 1995 and 2.7% in 2005, 1.8% “other” minority in 1995, and 1.6% in 2005 (the remaining percent are refusals to answer).
A longitudinal follow-up of this sample was conducted in 2005–2006. Because most of the field procedures took place in 2005, we refer to wave two as “2005”. Respondents were offered $20 for completion of MIDUS 1 surveys and up to $60 for completion of MIDUS 2 surveys as incentives for participation.
Of those who participated in wave one, the final retention rate for the longitudinal cohort of twins was 78%. Among those who did not participate in 2005, 130 (9.4%) refused, and 95 (6.8%) were no longer working telephone numbers, 57 (4.1%) were deceased (as confirmed by the National Death Index), and 8 (0.6%) were too ill to be interviewed. The MIDUS survey complied with Institutional Review Board standards of the University of Wisconsin and of the Harvard Medical School, and interviewers read to the interviewees a standard informed consent protocol at the beginning of the telephone interview.
The 1995 twin sample examined in this report included a total of 1,386 twins from same-sex twin pairs. Given the low power to detect qualitative sex effects (Prescott and Gottesman 1993), we excluded opposite-sex dizygotic twins from this analysis. The resulting sample contained 670 complete pairs (46 individual twins without their co-twin). The 49 same-sex twin pairs (or 98 individual twins from a same-sex pair) that are missing from the present analyses come from 23 twin pairs (or 46 individual twins) without their co-twin and 26 twin pairs (or 52 individual twins) with missing data on one of the measures of mental illness or mental well-being.
The complete same-sex twin pairs were divided into the following groups: 186 female monozygotic (MZ), 198 female dizygotic (DZ), 163 male MZ, and 123 male DZ, and had a mean age of 44.6 (SD = 12.2). The 2005 follow-up sample included 1,079 twins from same-sex twin pairs, including 453 complete pairs and 173 individual twins without their co-twin. The complete same-sex twin pairs were divided into the following groups: 128 female MZ, 134 female DZ, 112 male MZ, and 79 male DZ, and had a mean age of 53.9 (SD = 11.8).
Measures
We utilized three measures of MWB, employing the terminology developed by Keyes (Keyes 1998; Keyes 2002; Keyes 2005; Robitschek and Keyes 2009) based on his and other’s (Gallagher et al. 2009) studies of the structure of well-being: emotional, psychological, and social well-being.Footnote 1 As outlined in Table 1, emotional well-being was assessed by a six-item scale of positive affect and an item measuring overall life satisfaction (Andrews and Withey 1976; Bradburn 1969; Cantril 1965; Gurin et al. 1960; Mroczek and Kolarz 1998). The Cronbach alpha reliability of this seven item emotional well-being scale was +0.88. Psychological well-being was assessed by six scales of three items each (Table 1; Ryff and Keyes 1995). The Cronbach alpha reliability of the psychological well-being scale was +0.76. Social well-being was assessed with five scales of three items each (Table 1). The Cronbach alpha reliability of the social well-being scale was +0.72 (Keyes 1998).
In both the 1995 and 2005 waves, a history of (1) major depression (MD), (2) generalized anxiety disorder (GAD), and (3) panic attacks (PA) in the last year was assessed by phone interview using the highly structured Composite International Diagnostic Interview Short Form (CIDI-SF) (Kessler et al. 1998). Studies have shown that this instrument has excellent diagnostic sensitivity and diagnostic specificity as compared with the DSM-IV diagnoses based on the full CIDI in the National Comorbidity Study (Kessler et al. 1999).
Statistical methods
Last year MD, GAD, and PA were treated as dichotomous threshold traits and the three dimensions of MWB were treated as five category polychotomies. We examined the relationship between the genetic and environmental influences on IP and MWB in two ways. First, we focused on the 1995 data using last year prevalences of MD, GAD and PA, and the three measures of MWB.
We began with an atheoretical saturated Cholesky model with the hope of being able to show that a simple two common factor model would well describe the data. We present in Fig. 1 such a two common factor model with shared environmental effects eliminated for simplicity. The common factor of IP is indexed by the three individual disorders (via paths IPM, IPG, and IPP); and the common factor of MWB is indexed by the three individual forms of well-being (via paths MWBE, MWBS, and MWBP). All three forms of MWB also have specific genetic and environmental factors unique to each of them via paths A3 through A8, and E3 through E8, respectively. The genetic influences on the IP and MWB common factors result from a factor (A1) that is shared between both factors (via paths A1I and A1M, respectively) and a factor (A2) that is unique to the MWB factor via path A2M. (Note: The environmental influences are modeled analogously.) In this model, the proportion of genetic influences on MWB that results from genetic risk factors for IP is easily calculated as A 21M /(A 21M + A 22M ).

The structure of a simple two common factor model for Internalizing Psychopathology and Mental Well-Being in the 1995 MIDUS survey. See the text for further details. Shared environmental effects have been omitted from this figure for the sake of simplicity. A refers to additive genetic effects and E to individual specific environmental effects. Other abbreviations are: MD major depression disorder, GAD generalized anxiety disorder, Panic panic attacks, EWB emotional well-being, SWB social well-being, and PWB psychological well-being
Our second model incorporates both the 1995 and 2005 data. However, to model all of our IP and MWB variables assessed on both occasions would have required a model with 12 di- or polychotomous variables. Because of the demands of multi-dimensional integration, the run times for such a model in Mx would have been prohibitive. So, we restricted, for these computational reasons, our longitudinal analysis to two internalizing disorders and two of the measures of MWB producing a total of eight variables.
The details of this model, based on the best fitting model in our first set of analyses, are depicted in Fig. 2. It is broadly similar to the model used to examine the 1995 data with two important differences. First, it included general factors (Internalizing Psychopathology 1 and Mental Well-being 1) that reflected responses obtained on the measures at both the 1995 and 2005 assessments. Thus, these factors reflected the temporally stable propensities to IP and MWB, respectively. Second, this model contains two additional factors (Internalizing Psychopathology 2 and Mental Well-being 2) that reflect new influences on IP and MWB which arose between the 1995 and 2005 assessments. As with our earlier model, this model contains genetic and environmental influences shared between IP and MWB (A1 for the temporally stable factors and A2 for the new influences arising at 2005), and such influences specific for MWB (A3 for the temporally stable factors and A4 for the new influences arising at 2005).

The full model for the analysis of Internalizing Psychopathology and Mental Well-Being in both the 1995 and 2005 MIDUS surveys. See the text for further details and the legend for Fig. 1 for abbreviations
In studying both same-sex male and female twins, we can test for quantitative sex effects, allowing us to determine if the magnitude of the genetic and environmental parameters in our structural model differ between sexes. Twin model fitting of the raw data was performed using the Mx software package (Neale et al. 2003). The goal of model fitting is to achieve a balance between explanatory power and simplicity. This goal is operationalized by the use of Bayesian information criterion (BIC) that has been shown to perform particularly well with complex models as we have used here (Markon and Krueger 2004). We seek to minimize the BIC value.
Results
1995 Assessment
Our first set of twin models examined the inter-relationship between our three measures of MWB and our three measures of IP in the 1995 MIDUS survey data. Our full or baseline model I was a saturated ACE Cholesky decomposition which included separate parameter estimates for males and females (Table 1). Model II dropped all shared environmental pathways and resulted in a large improvement in the BIC (−130.7). Model III dropped all genetic pathways and also resulted in an improvement in fit over model I, but was inferior to the fit provided by model II. In model IV, we then constrained all the parameters in model II to equality across the sexes, producing a large further improvement in fit (BIC = −229.6). In model V, we attempted to substantially simplify these analyses by applying the model depicted in Fig. 1 and outlined in detail above. This much simpler model fit well with a large improvement over model IV (BIC = −341.2). This was our best fit model and the parameter estimates are given in Fig. 3.

Of the many results in this model, six are particularly noteworthy. First, the heritability of the latent factors for IP and MWB (reflecting paths A1I, A1M, and A2M, respectively, as seen in Fig. 1) were both quite high (61 and 72%, respectively). Second, the IP factor was well indexed by all three disorders, most strongly by GAD, followed by MD and PA (reflecting paths IPM, IPG, and IPP, respectively). Third, the general MWB factor was well indexed by all three of our specific measures, most strongly by psychological MWB (path MWBP), next by emotional MWB (path MWBE), and least strongly by social MWB (path MWBS). Fourth, the common factors did not capture all of the genetic influences on the internalizing disorders and forms of MWB, with some of them, particularly social and emotional well-being (paths A7 and A6, respectively), having modest to moderate trait specific genetic effects. Fifth, we can calculate from this model that the estimated phenotypic correlation between IP and MWB factors is −0.54 of which 86% is mediated by genetic and 14% by individual specific environmental factors. (These results are reassuringly similar to the −0.53 correlation observed between the IP and MWB factors observed in the entire MIDUS sample (n = 3,032; Keyes 2005). Sixth, and most importantly, the model permitted us to estimate the proportion of genetic and environmental influences of general MWB that were shared with IP. These figures were respectively, 50 and 5%.
1995 and 2005 Assessments
Analysis of the longitudinal two-wave data on IP and MWB began with the model depicted in Fig. 2 which, constituted the full model for these analyses. This model assumed the common factor structure that provided the best explanation for the 1995 data. Because of computational limitations, we had to use only two measures of each construct, taking those that loaded most strongly on the common factor in our best fit prior model: MD and GAD for IP, and emotional and psychological well-being for MWB.
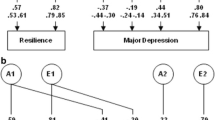
Model I for these analyses is depicted in Fig. 2. In models II and III, we dropped, respectively, all shared environmental and all additive genetic effects. While the fit improved for both models, model II had the lowest BIC (−88.3). Model IV constrained all the parameters to equality in males and females with a large improvement in the BIC (−168.6). Finally, in model V, we attempted to simplify this model by dropping the factors (Internalizing Psychopathology Two and General Well-Being Two) that reflected specific effects for the 2005 assessment. This produced a further substantial improvement in fit (BIC = −181.7) and model V constituted the best fit model. The parameter estimates for this model are shown in Fig. 4.

Six points are worth emphasizing about the results of this model. First, the heritability of the common factor to IP (61%) and MWB (69%) are reassuringly similar to that seen when examining only the 1995 data. Second, the common IP factor is well indexed by past year MD and GAD as assessed in both 1995 and 2005 with loadings in the narrow range from +0.70 to +0.83. Third, as with the 1995 data, the MWB factor is moderately better indexed by psychological (loading +0.81 and 0.82 in 1995 and 2005, respectively) than by emotional well-being (loading +0.69 and +0.68 in 1995 and 2005, respectively). Fourth, as with the 1995 data, the common factors did not capture all of the genetic influences on the specific measures of IP and MWB. While most of the specific genetic loadings were low, some—in particular on MD in 2005 and emotional MWB in 1995—were substantial. Fifth, we can calculate, from this model, that the estimated phenotypic correlation between our IP and MWB factors is −0.60 of which 69% is mediated by genetic, and 31% by individual specific environmental, factors. Sixth, and most importantly, this model permitted us to obtain a second estimate of the proportion of genetic and environmental influences of MWB that were shared with IP. These figures for our longitudinal data were, respectively, 41 and 29%.
Discussion
The goal of this article was to evaluate three hypotheses about the nature of the relationship between the genetic and environmental influences on IP and MWB. We evaluated this question using two inter-related sets of data from the national MIDUS twin study. Our first approach utilized only the 1995 data and examined all three measures of IP (i.e., past year diagnosis of MD, GAD, and PA) and the three measures of MWB (i.e., the scales assessing emotional, social, and psychological well-being). The best fit model was a simple one in which both IP and MWB were identified as common factors, each indexed by the three relevant measures. Exactly half of the genetic influences of the common factor of MWB were shared with the IP common factor and 50% were independent.
These results are inconsistent with both the first and third hypothesis: that genes for MWB were either unrelated or very closely related to those for IP. Rather, these findings were as predicted by the second hypothesis: that genetic influences on MWB can be meaningfully divided into two groups—those that convey a low risk for IP and those which impact more directly on the positive features of MWB. This hypothesis has been previously referred to by Keyes as the “dual continua model” (Keyes 2005). By contrast, we found a much lower sharing of environmental risk factors. Environmental influences on MWB were, in this model, largely independent of those that impact on IP.
Our second approach to this question utilized both the 1995 and 2005 data from the MIDUS, permitting us to look at the temporally stable influences on IP and MWB. Because of computational limitations, these analyses were restricted to two measures each of IP and MWB. Our analyses again produced a simple best fit model with one common IP factor that loaded substantially on measures of past year MD and GAD obtained 10 years apart, and one common MWB factor that loaded strongly on the measures of emotional and psychological MWB obtained in 1995 and 2005. This model estimated that genetic risk factors for the temporally stable component of IP were responsible for 41% of the genetic influences on the temporally stable measures of MWB. These results are reassuringly similar to those obtained from our first design and further support the second hypothesis articulated above—that important components of the genetic influences on MWB are partially shared with, and another portion is largely independent from, the risk to IP. However, in the model with longitudinal data, we found a level of sharing of environmental risk factors that, while still modest (29%), was substantially higher than that estimated with our first cross-sectional design (5%). These results suggest, consistent with clinical experience, that environmental events able to produce an enduring effect on liability to IP have more of an impact on MWB than events that have a more transient impact on risk for IP.
Our best fit twin models permit us to examine the degree to which genetic and environmental factors are responsible for the observed inverse relationship between IP and MWB. Examining our cross-sectional measures of MWB and one-year prevalence of IP, a very high proportion (86%) of the IP-MWB phenotypic correlation resulted from gene factors. When we modeled our two measures of MWB and IP assessed a decade apart, the picture differed somewhat. Now, genetic factors accounted for about two-thirds and stable environmental influences one-third of the phenotypic relationship between IP and MWB.
We found no evidence for quantitative sex effects in our model fitting. These findings suggest that, despite the consistent evidence for higher rates of IP in women, the underlying pattern of the association between IP and MWB are stable across the sexes.
These results can be usefully interpreted in the context of two prior reports. First, the factor structure we obtained for our measures of MWB which were examined jointly with IP in our analyses with the 1995 data are nearly identical to those found when we examined these MWB measures in this sample on their own (Keyes et al. 2010). Second, Nes et al. (Nes et al. 2008) recently examined, in young adult Norwegian twins, the inter-relationship between current symptoms of anxiety and depression and a single-item assessment of life satisfaction. While using a different approach to twin modeling, and finding sex differences (which we did not), their qualitative conclusions were similar to ours in that they found substantial but far from complete overlap in the genetic risk factors for anxiety/depression and life satisfaction.
Limitations
First, the sample size of twins is modest, so we have limited power to detect subtle effects (Neale et al. 1994). Second, the twins were ascertained indirectly via relatives so we cannot be certain that biases did not creep into this process. We can explore whether cooperation in our 2005 sample was representative of the 1995 sample with respect to the key variables in our analysis. We examined whether age, sex, a history of MD, GAD, and PA in the last year or levels of emotional, psychological, and social well-being predicted cooperation in our 2005 survey. Of the eight variables examined, two were significant at marginal levels of significance (P = 0.04) that would not withstand multiple test corrections. Higher levels of social well-being and a history of PA both modestly predicted increased cooperation. These results do not suggest that our follow-up sample was markedly biased with respect to our key variables of interest. Third, the MIDUS sample has a wide age range and our twin modeling did not formally correct for age effects. Regression analysis indicated that the associations between the well-being and psychopathology variables we examined and age were quite modest with the exception of emotional well-being measured in 1995, where age accounted for 3.1% of the variance. We therefore examined our best fit model regressing age effects out of all three of our well-being measures. The results were very similar to those seen in Fig. 3, suggesting that age effects minimally contributed to our reported parameter estimates.
Conclusions
These analyses shed light on an important aspect of the human condition—how risk factors for common psychiatric illness impact on human flourishing. We found that the preponderance of the inverse relationship between IP and MWB resulted from the impact of genetic factors. However, only about half of the genetic influences on a highly heritable and comprehensive measure of MWB derive from genetic risk factors for IP. That is, the dual continua observed at the phenotypic level in the general population (Keyes 2005) reflect a dual continua at the genetic level.
In common sense language, this means that while it is more difficult to reach high levels of well-being if you inherit strong genetic risk factors for depressive and anxiety disorders, this can be achieved. A strong dose of genetic liability to psychiatric illness does not ordain low levels of well-being. Furthermore, low levels of genetic risk for IP by no means guarantee a life well-lived. Rather than being an artifact, the dual continua arises, in large measure, because the genetic propensity for positive mental health is in part independent of the genetic liability for common internalizing disorders. From a genetic as well as a phenotypic perspective, mental health is both influenced by, but considerably more than, the absence of mental illness.
Notes
The well-being literature does not have a common set of terms for describing these dimensions. While many psychologist tend to refer to emotional well-being as “subjective well-being,” Keyes argues that all three dimensions of MWB are subjective assessments of well-being that are more clearly identified by whether the measures focus on feeling states (i.e., hedonia) toward one’s life or how well individuals see themselves functioning in their lives (i.e., eudaimonia), with the latter being distinguished in terms of whether the functioning is psychological (i.e., more private and personal) or social (i.e., more public and communal). For consistency with the past research, which involves the same model in this article, we employ Keyes’ terminology.
References
Andrews FM, Withey SB (1976) Social indicators of well-being: Americans’ perceptions of life quality. Plenum, New York
Bradburn NM (1969) The structure of psychological well-being. Aldine, Chicago
Cantril H (1965) The pattern of human concerns. Rutgers University Press, New Brunswick
Gallagher MW, Lopez SJ, Preacher KJ (2009) The hierarchical structure of well-being. J Pers 77(4):1025–1050
Gurin G, Veroff J, Feld S (1960) Americans view their mental health. Basic Books, New York
Hettema JM, Neale MC, Kendler KS (2001) A review and meta-analysis of the genetic epidemiology of anxiety disorders. Am J Psychother 158(10):1568–1578
Kendler KS, Prescott CA, Myers J, Neale MC (2003) The structure of genetic and environmental risk factors for common psychiatric and substance use disorders in men and women. Arch Gen Psychiatry 60(9):929–937
Kendler KS, Gatz M, Gardner C, Pedersen N (2006) A Swedish national twin study of lifetime major depression. Am J Psychother 163(1):109–114
Kendler KS, Aggen S, Knudsen GP, Roysamb E, Neale M, Reichborn-Kjennerud T (2010) The structure of genetic and environmental risk factors for syndromal and subsyndromal common DSM-IV axis I and all axis II personality disorders. Am J Psych 168(1):29–39
Kessler RC, Andrews G, Mroczek DK, Ustun B, Wittchen H-U (1998) The world health organization composite international diagnostic interview short form (CIDI-SF). Int J Meth Psych Res 7(4):171–185
Kessler RC, DuPont RL, Berglund P, Wittchen HU (1999) Impairment in pure and comorbid generalized anxiety disorder and major depression at 12 months in two national surveys. Am J Psychother 156(12):1915–1923
Keyes CLM (1998) Social well-being. Soc Psychol Quart 61(2):121–140
Keyes CLM (2002) The mental health continuum: From languishing to flourishing in life. J Health Soc Behav 43(2):207–222
Keyes CLM (2005) Mental illness and/or mental health? Investigating axioms of the complete state model of health. J Consult Clin Psychol 73(3):539–548
Keyes CLM (2007) Promoting and protecting mental health as flourishing—A complementary strategy for improving national mental health. Am Psychol 62(2):95–108
Keyes CLM, Myers JM, Kendler KS (2010) The structure of the genetic and environmental influences on mental well-being. Am J Public Health 100(12):2379–2384
Lykken D, Tellegen A (1996) Happiness is a stochastic phenomenon. Psychol Sci 7(3):186–189
Lykken DT, Bouchard TJ Jr, McGue M, Tellegen A (1990) The Minnesota twin family registry: some initial findings. Acta Genet Med Gemellol (Roma) 39(1):35–70
Markon KE, Krueger RF (2004) An empirical comparison of information-theoretic selection criteria for multivariate behavior genetic models. Behav Genet 34(6):593–610
Mroczek DK, Kolarz CM (1998) The effect of age on positive and negative affect: a developmental perspective on happiness. J Person Soc Psychol 75(5):1333–1349
Neale MC, Eaves LJ, Kendler KS (1994) The power of the classical twin study to resolve variation in threshold traits. Behav Genet 24(3):239–258
Neale MC, Boker SM, Xie G, Maes HH (2003) Mx: Statistical Modeling. Dept. of Psychiatry, Virginia Commonwealth University Medical School, Richmond
Nes RB, Roysamb E, Tambs K, Harris JR, Reichborn-Kjennerud T (2006) Subjective well-being: genetic and environmental contributions to stability and change. Psychol Med 36(7):1033–1042
Nes RB, Czajkowski N, Roysamb E, Reichborn-Kjennerud T, Tambs K (2008) Well-being and ill-being: shared environments, shared genes? J Posit Psychol 3(4):253–265
Prescott CA, Gottesman I (1993) Power limitations in detecting heterogeneity of genetic effects: the case of sex differences in alcoholism. Presented at the annual meeting of the society for research on psychopathology, Chicago, 23–26 October 1993
Robitschek C, Keyes CLM (2009) Keyes’s model of mental health with personal growth initiative as a parsimonious predictor. J Couns Psychol 56(2):321–329
Roysamb E, Tambs K, Reichborn-Kjennerud T, Neale MC, Harris JR (2003) Happiness and health: environmental and genetic contributions to the relationship between subjective well-being, perceived health, and somatic illness. J Person Soc Psychol 85(6):1136–1146
Ryff CD, Keyes CL (1995) The structure of psychological well-being revisited. J Person Soc Psychol 69(4):719–727
Stubbe JH, Posthuma D, Boomsma DI, de Geus EJ (2005) Heritability of life satisfaction in adults: a twin-family study. Psychol Med 35(11):1581–1588
Sullivan PF, Neale MC, Kendler KS (2000) Genetic epidemiology of major depression: review and meta-analysis. Am J Psychother 157(10):1552–1562
Acknowledgments
Supported in part by NIH grant MH068643. The 1995 phase of the study was supported by the John D. and Catherine T. MacArthur Foundation Research Network on Successful Midlife Development. The 2005 phase was supported by a grant from the National Institute on Aging (P01-AG020166) to conduct a longitudinal follow-up of the MIDUS (Midlife in the USA) investigation.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Edited by Michael Lyons.
Rights and permissions
About this article
Cite this article
Kendler, K.S., Myers, J.M., Maes, H.H. et al. The Relationship Between the Genetic and Environmental Influences on Common Internalizing Psychiatric Disorders and Mental Well-Being. Behav Genet 41, 641–650 (2011). https://doi.org/10.1007/s10519-011-9466-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10519-011-9466-1