
Abstract
Compared to the booming industry of AIMDSS, the usage of AIMDSS among healthcare professionals is relatively low in the hospital. Thus, a research on the acceptance and adoption intention of AIMDSS by health professionals is imperative. In this study, an integration of Unified theory of user acceptance of technology and trust theory is proposed for exploring the adoption of AIMDSS. Besides, two groups of additional factors, related to AIMDSS (task complexity, technology characteristics, and perceived substitution crisis) and health professionals’ characteristics (propensity to trust and personal innovativeness in IT) are considered in the integrated model. The data set of proposed research model is collected through paper survey and Internet survey in China. The empirical examination demonstrates a high predictive power of this proposed model in explaining AIMDSS adoption. Finally, the theoretical contribution and practical implications of this research are discussed.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
In China, misdiagnosis and low efficiency in medical diagnosis are the main trigger factors of the contradiction between patients and doctors. In most cases, health professionals have to make their decision based on various medical examination data generated by kinds of technical means, such as the X ray film, endoscopic image, etc. However, it is not a simple job to identify the lesion position, and besides, the efficiency and accuracy may decrease largely after the doctors have read too many images. The complexity and workload of diagnosis have created pressure on health professionals for a long time. There are no authoritative statistics of the clinical misdiagnosis rate. However, it is a consensus that the average clinical misdiagnosis rate is about 30%, and for malignant cancers (Leukemia, pancreatic, etc.) is even up to 40%.Footnote 1 Therefore, it creates a great demand and significance in improving the accuracy of medical diagnosis. At present, some artificial intelligence products have aroused lot of attention in the medical field, which are mainly developed for disease detection and diagnosis on basis of patients’ examination data, including the forms of image and text. Applying the artificial intelligence technology in the problem of medical diagnosis is expected to assist physicians in their routine work to improve the diagnostic level and alleviate their work pressure significantly. Many technology companies, such as Baylabs, Enitic and Freenome, have developed AIMDSS for assisting healthcare professionals in the early detection of cancers and quick diagnosis of common disease (Terry et al. 2016). This kind of system is aimed to serve as an artificial robot that provides detection results and treatments as a “second opinion” to healthcare professionals, and helps them complete their work more precisely and efficiently. Many AIMDSS have been validated relatively satisfactory diagnosis accuracy results compared to human doctors. For example, according to Enitic, the accuracy of malignant tumors detection system they developed is higher than radiologic technologists. Enlitic used lung cancer related image databases, “LIDC (Lung Image Database Consortium)” and “NLST (National Lung Screening Trial)”, for a verification. Results showed that the accuracy of malignant tumors detection system was 50% more higher than radiologic technologists.Footnote 2 Recently, the research Esteva’s team have done on artificial intelligence medical diagnosis was introduced on the cover of the journal Nature. Esteva’s team employed convolutional neural network to analyze nearly 130 thousand clinical pictures of cutaneous carcinoma, and finally this neural network rapidly became a real cutaneous carcinoma expert (Esteva et al. 2017). With the development of AIMDSS, an increasing number of studies and reports about AIMDSS have emerged in recent years. Some aimed to propose a high performance diagnosis system based on various AI techniques (Er et al. 2015; Cimperman et al. 2016). Some discussed the impact it brings on healthcare industries and the comparison between AIMDSS and healthcare professionals.Footnote 3,Footnote 4,Footnote 5 In fact, AIMDSS has already proved useful in the healthcare industry. For example, at Xiangya hospital in China, a AIMDSS for skin disease is on the line, open to clinicians. The system can make rapid response to different skin photos, giving directions for possible diseases and their probability. At present, the diagnosis accuracy of this system on Biett’s disease exceeds 85%.Footnote 6 At Shanghai Changzheng Hospital in China, radiologists are using a AIMDSS to enhance medical diagnosis in reading CT scans and X-rays of lung cancer patients. The AIMDSS can learn the core characteristics of lung cancer and identify the suspicious lesions and nodules through different CT image sequences and make earlier diagnosis of lung cancer more available.Footnote 7
While many reports and studies represented a bright prospect of AIMDSS, AIMDSS is still in the fairly early stage of it’s widely implementation in the healthcare sector. A recent survey by the Healthcare Information and Management Systems Society in American in 2017 indicated a lower utilization of AI technologies that only 4.7% of the survey respondents were already using AI technologies in hospitals.Footnote 8 In fact, as early as 1972, the world’s first computerized diagnosis support system, an early precursor to AIMDSS of today, was developed in the UK. The system used naive Bayesian algorithm to recognize the possible cause of acute abdominal pain and was trained to the point where it was as accurate as senior doctors. However, the system with good performance on diagnosis is still not in routine use so far.Footnote 9 This indicates that the routine usage of AIMDSS is not just depends on technologies, but also people’s attitude. A lack of trust in new technologies, a generalized conflict of computers, etc. are all the possible barriers to routine use of a new IT in a certain industry. Especially for healthcare professionals, it always takes a long time to actually use a new healthcare system in daily clinical works after it is developed. Medical diagnosis impacts significantly to peoples’ health and life and health professionals have to take responsible for their patients. Thus, health professionals may be more cautious than professionals in other fields when considering whether to adopt a new product or service to assist their works. In addition, health professionals are always strongly proud of their expertise that more psychological conflict might be caused for them to accept such a computerized assistant which claims to be better than themselves at diagnosing. That is to say, a technical victory may not be enough for AIMDSS to be successfully used in daily work. Therefore, it is quite essential to explore the critical factors in several aspects that influence health professionals’ adopting behavior towards AIMDSS. This could have important implications not only for the AIMDSS promotion, but also for the improvement of healthcare industry. However, compared to the booming industry of AIMDSS, there is lack of research on the acceptance and adoption intention of AIMDSS by health professionals, which has caused a gap between the rapid development of AIMDSS and small-scale usage by health professionals in daily work. To the best of our knowledge, our study is the first attempt to investigate the intrinsic motivation of the adoption behavior on AIMDSS so as to greatly promote the pervasion of such systems in hospitals.
For the problem of user acceptance of information technology (IT) in various fields, the unified theory of user acceptance of technology (UTAUT) has been widely used (Dulle and Minishi-Majanja 2011; Venkatesh et al. 2011). It has been applied to explain the individuals’ adoption behavior by integrating the elements from eight prominent models, which reflects both the aspects of technology and organization and has been verified higher explanatory power than other IT adoption models (Venkatesh et al. 2003). For a more accurate understanding of healthcare professionals’ acceptance of AIMDSS, we add initial trust as a behavioral intention determinant into UTAUT, and thus divide the formation process of usage behavioral intention into three stages. Two groups of additional factors are considered in the extended model. The first group is related to AIMDSS used by healthcare professionals, and the other one is health professionals’ characteristics factors. We assume that the factors related to AIMDSS, including task complexity, technology characteristics, and perceived substitution crisis are three significant factors that affect health professionals’ acceptance behavior. Apart from product itself and organizational factors, the personality trait and individuality of health professionals, such as propensity to trust and personal innovativeness in IT, also influence the adoption behaviors towards the AIMDSS, and these factors are also included in our study. In view of this, we propose some hypotheses based on the integration of three components discussed above, and test all the hypotheses by conducting a survey to study the acceptance and usage intention of AIMDSS by health professionals.
The organization of this paper is as follows. In Sect. 2, we review the healthcare service adoption, IT acceptance and use models. Section 3 describes our proposed research model, including the AIMDSS adoption factors and hypotheses. The methodology is introduced in Sect. 4, followed by a survey and analysis results in Sect. 5. Sections 6 and 7 respectively describes the discussions, implications, conclusion and limitations of our study.
2 Literature review
In this part, we seek to summarize the theoretical models in healthcare service adoption studies in different fields as a solid theoretical foundation of our research on health professionals’ adoption towards AIMDSS.
2.1 Review on healthcare service adoption studies
In this part, we review the related research on healthcare service adoption from two perspectives, adoption subjects and adoption objects. Adoption subjects refer to those individuals or organizations considering whether to adopt any new healthcare services. In this paper, we divide the adoption subjects generally into three categories, i.e., healthcare recipients (e.g., patients, or individuals who’d like to receive healthcare services), healthcare professionals (e.g., doctors, medical technicians, etc.) and healthcare organizations (e.g., hospitals, clinics, etc.). The factors which influence adoption behavior can be differentiated for different types of adoption subjects. For example, considering different adoption subjects confronted with a new healthcare service who all need going through a decision process, healthcare recipients may pay more attention on the benefits in improving their health condition while professionals focus on the benefits in promoting their job efficiency and performance. For example, Yang et al. (2015) proved that patients’ health condition significantly moderated the relationship between their satisfaction and online health consulting services quality provided by physicians. According to the literature review on health professionals’ adoption towards mobile-health (m-health) services provided by Gagnon et al. (2015), factors related to work environment and workload remarkably facilitate or block physicians’ adoption towards m-health services. From health organizations’ perspective, they may take more consideration on the characteristics of hospitals, top management support and government privacies and so on. Furthermore, in healthcare service adoption studies toward specific adoption subjects, lots of researchers tend to classify the respondents based on certain characteristics so as to enable a more accurate knowledge of adoption behaviors. For instance, Zhang et al. (2014) took the gender as a moderating variable to investigate the gender differences of healthcare recipients on m-health adoption, and the study showed male appears more active on adopting m-health services.
Adoption objects refer to those emerging electronic/mobile/smart healthcare services oriented to healthcare recipients or healthcare professionals. Healthcare services can be divided into three categories by technical carriers, including the mobile devices (e.g., smartphone, tablet computer, PDA), medical related applications (e.g., drug reference app, clinical score app) and medical related information systems (e.g., PACS, HIS, EMR, EHR). According to the main contributions offered by different kinds of healthcare services to different adoption subjects, they can be classified into the categories as shown in Table 1. Healthcare services can be categorized into the following groups: remote consulting, healthcare management, and disease management. In most cases, one healthcare service probably has several functions. For instance, in Hilliard et al.’s study (2014), the studied adoption object, an m-heath app not only provided cystic Fibrosis Self- Management services (disease management) but also common health information (healthcare management) to healthcare recipients, but only the cystic Fibrosis Self- Management service was the research topic in their paper. For healthcare professionals, healthcare services include but not limited to medical assistant, remote diagnose, medical education, medical reference and medical data management. By and large, researches on medical data management service adoption have become dominant in this area. For healthcare organizations, the adoption objects are basically the same as healthcare professionals.
2.2 Review on service adoption models
The adaptation and integration of theories on technology adoption in different fields of applications helps us generate a more accurate and comprehensive understanding to the users’ adoption behavior and the related processed. In healthcare adoption fields, technology acceptance theories that have been widely used include technology acceptance model (TAM), theory of planned behavior (TPB), unified theory of user acceptance of technology (UTAUT), the technology–organization–environment (TOE), theory of diffusion of innovations (DOI), task-technology fit (TTF). TAM is usually used in exploring individuals (e.g., patients, healthcare professionals, et al.) behavior in healthcare services adoption. The basic postulate in TAM is that perceived usefulness and perceived ease of use are two core constructs which determine the intention-to-use which in turn influences the actual usage behavior. The adoption studies following TAM all apply this postulate. Hung and Jen (2012) used an original TAM to study people’s adoption of mobile health management services, where all variables in TAM were proved to be significant. In addition, they considered age as a moderating factor and finally found that the intention to use varied with age. Another example was provided by Hoque (2016) who investigated the younger citizens’ adoption towards m-health services on the basis of TAM. The researcher extended the original TAM with two additional constructs, subjective norm and personal innovativeness in IT, and considered gender as a moderating factor in the proposed model. The study found that constructs from the original TAM model and these two additional constructs all played a highly significant role in influencing m-health adoption and the gender also made a difference toward technology adoption.
TPB is an extension of theory of reasoned action (TRA) in the field of individual adoption behavior. TPB posits that attitude toward behavior, subjective norm and perceived behavioral control all have impact on users’ intention to use (Ajzen 1991). In healthcare adoption studies, TPB is usually applied together with other theories. For example, Deng et al. (2014) compared users’ adoption towards mobile health services between middle-aged and old groups based on a combined model incorporating constructs from TPB and VAB (value-attitude-behavior). Another example was provided by Wu et al. (2011) where TAM and TPB were integrated to explore hospital’s professionals’ adoption towards mobile health services.
In recent years, UTAUT, which was proposed as a unified theory integrating eight prominent technology acceptance theories (TAM, DOI, TPB et al.) by Venkatesh et al. (2003) has become dominant in the healthcare service adoption literature. Although it was presented relatively late, it shows more abundant compared to other theories. A good example of the application of UTAUT in the area of IT acceptance research was provided by Kijsanayotin et al. (2009) who used it to understand factors influencing Thailand’s community health centers’ (CHCs) IT adoption across a sample of 1607 CHCs in Thailand. The researchers improved the original UTAUT model by adding voluntariness, experience and IT knowledge as three new concepts to explain the intrinsic motivation of IT adoption. Based on the results of the investigation study, they found that past IT experience and facilitating conditions were the most important predicting factor of the IT use followed by intention to use which was prominently impacted by performance expectancy. Another good example was provided by Cimperman et al. (2016) who studied elderly users’ acceptance of Home Telehealth Services (HTS) based on an extended UTAUT model. They extended the original model by adding three additional constructs including doctor’s opinion, computer anxiety, and perceived security into the context of elderly adults’ health technology acceptance. Finally, they found that social influence which existed in the original UTAUT model appeared an insignificant role in predicting behavioral intention to use in this particular context.
TOE is one of the famous theories used to explore the organizations behavior in the process of healthcare services adoption. TOE is focused on technological, organizational and environmental to explore the technology adoption of organizations (Tornatzky and Fleischer 1990; Chang et al. 2007). Yang et al. (2013) analyzed the factors influencing hospital’s adoption decision towards healthcare information systems through these three dimensions. And finally, the researchers developed a framework of these significant influencing factors.
DOI is a theory that explains the events of the innovation adoption process to a process that a new thing gradually been comprehended and adopted by specific group by means of certain channels over time. Unlike other theories, DOI pay more attention on information necessarily at every stage of innovation adoption (Rogers 2003). Theoretically speaking, DOI can be used to understand both individuals and organizations adoption behavior towards innovation. However, in healthcare service adoption studies, DOI has been used in individuals (patients, healthcare professionals) adoption more frequently. For example, Chew et al. (2004) applied DOI to investigate strategies for increasing the usage of Internet by family physicians. In this study, the researchers found the critical information that push forward physicians start and keep to learn the internet use on the basis of DOI.
Another adoption theory TTF argues the significance of fit between IT and IT-supported users’ tasks in explaining user adoption behavior (Goodhue and Thompson 1995). Compared with the individual TTF model, TTF is more likely to be combined with other models such as TAM and UATUT to explain individual behavior to use an IT. For example, Zhou et al.’s (2010) study, an integrated model of TTF and UATUT were applied to explain mobile banking user adoption. Results showed that the interaction between technology and tasks has a significant effect on user adoption of mobile banking.
2.3 Trust-based theoretical framework of individual technology acceptance
Trust in technology refers to the “beliefs about a technology’s capability rather than its will or its motives” (Mcknight 2005). Extensive studies discussed individual technology acceptance process from a perspective of trust formation, where the trustee was a technology such as an information system or a recommendation agent. For example, Lu et al. (2016) studied an adoption problem of online microsourcing through uncovering the trust-formation logic in online microsourcing market places. Wang and Benbasat (2005) applied a model of trust and technology acceptance to explore individual technology acceptance in a context of online recommendation agents. Those indicated that trust in technology played a significant role in technology acceptance. Thus, we outline a trust-based theoretical framework of individual technology acceptance based on those prior researches on trust and technology adoption for a better understanding of AIMDSS adoption among healthcare professionals. As shown in Fig. 1, trusting bases are the determinants of trust in technology, which in turn lead to trust-related behaviors. Trusting bases show different in various contexts. For instance, in a study on mobile payment user adoption from a trust perspective (Yan and Pan 2015), four trusting bases were proposed in the research model: perceived ease of use, perceived usefulness, structural assurance and ubiquity. These are the critical factors that lead to users’ trust in mobile payment, which then positively affects usage intention. Through a literature review of research on technology trust (Chaouali et al. 2016; Lai et al. 2011; Gefen et al. 2008), we draw three categories of trusting bases which jointly lead to trust formation in technology. The three categories are individual traits, perceptions of the attributes of technology and organization environment, which respectively reflects the differences of trustors in trusting a certain technology from the perspectives of individual, technology and organization state. Finally, a trustor with higher trust degree in technology is more likely to adopt, or intend to adopt the target technology.

A trust-based theoretical framework of individual technology acceptance
3 Research model and hypotheses
In this part, we seek to propose our research model, including the AIMDSS adoption factors and hypotheses.
3.1 UTAUT and AIMDSS adoption
UTAUT is a well-established model that has been widely applied to predict and explain individuals’ behavior during the process of adopting a technology. According to UTAUT, an individual’s adoption behavior is determined by behavior intention and facilitating conditions, and behavior intention is jointly determined by performance expectancy, effort expectancy and social influence. Venkatesh et al. (2003) verified that UTAUT performed a substantial improvement compared to other user acceptance models and explained up to 69 percent of the variance in behavioral intention, which is the most recognized determinant of actual use. However, considering the reality that AIMDSS is still an emerging thing in China, and most healthcare professionals have no access to AIMDSS in their routine work currently, using the measurement of actual usage may lead to an inaccurate conclusion about healthcare professionals adoption of AIMDSS. Therefore, we chose behavior intention rather than actual use as the dependent variable in our model. Behavior intention in this study refers to the strength and extent of healthcare professional’s willingness to adopt an AIMDSS. In this particular section, we discuss the potential factors included in original UTAUT.
3.1.1 Performance expectancy
Performance expectancy is defined as “the degree to which a person believes that using a particular system would enhance his or her job performance”, which is derived from perceived usefulness proposed in the original TAM. Venkatesh et al. (2003) demonstrated that performance expectancy had a direct influence on behavioral intention towards adopting a target technology. Further studies on UTAUT supported the significant relationship between performance expectance and behavioral intention in various IT settings (Abushanab and Pearson 2007). Based on the discussions above, we argue that the mechanisms related to performance expectance and behavior intention is also true in the context of AIMDSS. Consequently, the following hypothesis H1 is suggested:
H1
Performance expectancy has a positive influence on behavioral intention to use AIMDSS.
3.1.2 Effort expectancy
Effort expectancy is defined as “the degree of ease associated with the use of the system”, which is derived from perceived ease of use proposed in the original TAM (Venkatesh et al. 2003). Many existing studies demonstrated that effort expectancy positively influences behavioral intention to use a new IT such as internet banking (Abushanab and Pearson 2007), mobile learning (Wang et al. 2009), EMR system (Kim et al. 2016) etc. The easier to operate a new IT, the more active they are to use it. Therefore, we expect that it is important for the doctors to perceive ease of use when using AIMDSS, otherwise there would be less incentive to use them. Consequently, the following hypothesis H2 is suggested:
H2
Effort expectancy has a positive influence on behavioral intention to use AIMDSS.
In addition to the direct influence of performance expectancy and effort expectancy on behavioral intention, previous studies argue that a potential linkage also exists between effort expectancy and performance expectancy. The easier individuals feel to operate with a technology, the more likely they are to perceive a higher “usefulness” of that technology (Cimperman et al. 2016). It is consistent with TAM theory which argues that “perceived ease of use has a direct influence on perceived usefulness.” (Davis 1989). Based on the above theories, we assume that the potential linkage also exists in an AIMDSS adoption context, that is, the higher effort expectancy leads to higher performance expectancy for healthcare professionals. Consequently, the following hypothesis H3 is suggested:
H3
Effort expectancy has a positive influence on performance expectancy for using AIMDSS.
3.1.3 Social influence
Social influence is defined as “the degree to which an individual perceives that important others believe he or she should use the new system”. Individuals are more or less influenced by others, especially those who are closer and important to them, such as relatives, friends, superiors, etc. (Venkatesh et al. 2003). These persons’ positive or negative opinions and behavior will influence us more when considering whether to use it. Some studies already found social influence a major contribution to adopt m-health, such as cloud comoputing (Alharbi 2014), and E-government services (Alshehri et al. 2013) etc. Thus, there’s reason to believe that doctors’ intention to use AIMDSS would be impacted by important persons in their social circles. Consequently, the following hypothesis H4 is suggested:
H4
Social Influence has a positive influence on behavioral intention to use AIMDSS.
3.2 Initial trust and AIMDSS adoption
Trust refers to a degree to which an individual believes in, and is willing to depend on, another party. According to McKnight’s trust theory, trust formulation at different stages is based on different factors and processes (Mcknight 2005). Considering that most healthcare professionals in China now basically have no prior experiences with AIMDSS, in this research, we focus on the initial stage of trust formulation, which refers to trust in an unfamiliar party or with no prior use, that how it may influence healthcare professionals’ behavior during the process of adopting an AIMDSS.
According to Luhmann’s theory, trust helps in reducing complexity through excluding those undesirable and adverse actions that other people or organizations are likely to do in the future (Luhmann 1982). In the case of AIMDSS adoption for healthcare professionals, with the unique relevance of using AIMDSS in the patient’ health and life, healthcare professionals tend to be more cautious than other technology adopters when deciding whether or not to adopt target technologies for protecting the quality of healthcare services for patients. With trusting, healthcare professionals would exclude adverse consequences when using AIMDSS as a diagnosis assistant in daily work, like misdiagnosis and information leakage, which finally influence their intention to use AIMDSS. Previous studies demonstrated a significant influence of trust on usage behavior of information technologies, which further supports the argument (Bansal et al. 2010; Chiu et al. 2012; Ke et al. 2009). Consequently, it is hypothesized that initial trust positively influences healthcare professionals’ intention to use AIMDSS in their daily work as proposed in H5.
H5
Initial trust has a positive influence on behavioral intention to use AIMDSS.
3.3 Antecedents of initial trust
In order to accurately understand the role of trust in the context of AIMDSS adoption, we now turn to an exploration of its antecedents. Previous researches have discussed potential factors that may be predictive of trust in individual technology acceptance settings. As discussed before, these potential factors can be classified roughly into three main categories: individual trials, perceptions of the attributes of technology and organizational environment. According to the trust-based theoretical framework outlined before and the specific research context, we identified performance expectancy, effort expectancy, social influence and initial trust as four potential antecedents of trust in an AIMDSS. The following chapter states the reasons for adopting these four constructs.
3.3.1 Performance expectancy, effort expectancy and initial trust
Li et al. (2008) posited that user’s general expectations of a specific, novel technology would ultimately impact their trust opinions in this technology. As mentioned above, performance expectancy and effort expectancy are two kinds of general expectations of a specific technology. The former specifically refers to the expectation of necessary effort on using such a technology and the latter specifically refers to an expectation of improvement in performance. Those are two concrete reflection of the perceptions on the attributes of technology, which are discussed before that can lead to trust formation in technology.
Many studies discussed the relationship between effort expectancy and trust formation. One study investigated the online purchase intentions based on an integrated model of trust and TAM, and confirmed a linkage between perceived ease of use (which corresponds to the construct of effort expectancy in UTAUT) and trust in e-vendor (Gefen et al. 2003). Another study on the enabling factors for electronic logistics information system acceptance demonstrated that perceived ease of use positively influences trust in electronic logistics information system (Tung and Chou 2008). In the context of AIMDSS, a perception of hard to use AIMDSS might decrease the healthcare professionals’ confidence in the reliability of AIMDSS, which implicitly indicates that the product cannot be trusted. Therefore, we have the following hypothesis H6 which considers the relationship between effort expectancy and initial trust.
H6
Effort expectancy has a positive influence on initial trust in AIMDSS.
Previous studies also argued that performance expectancy has a significant influence on trust formation. In the study by Gu et al. (2015), in terms of the consumers’ adoption of wearable commerce, performance expectancy was posted as a direct factor of initial trust in wearable commerce. Additional study indicated that performance expectancy was a significant antecedent of initial trust in mobile banking among 194 voluntary participators (Oliveira et al. 2014). In the context of AIMDSS, when healthcare professionals have a high expectation toward having an expected performance, they are likely to build a solid confidence in AIMDSS. Accordingly, we posit a potential linkage between performance expectancy and initial trust in AIMDSS. Therefore, the following hypothesis H7 is thus proposed.
H7
Performance expectancy has a positive influence on initial trust in AIMDSS.
3.3.2 Social influence and initial trust
Kelman’s (1958) attitude change theory proposes that individuals tend to be fully motivated to comply with people who are important to him, which implies a direct linkage between social influence and behavior intention. Li et al. (2008) argued that such linkage also plays a significant role in the impact of social influence on trusting intention. Besides, other studies also strongly support the view. Li et al. (2006) demonstrated a direct relationship between social influence and trusting beliefs in IS settings. When individuals have not enough knowledge and actual operation experiences on a technology, they are more likely to rely on the important people’s opinions and incorporate them into trust formation Li et al. (2008). For healthcare professionals, we study in this study, who have no direct experiences with AIMDSS, their perception that important people, such as patients, colleagues, or leaders et al. think that he should or should not perform the AIMDSS will have a significant impact on their initial trust in AIMDSS. The following hypothesis H8 is thus proposed.
H8
Social influence has a positive influence on initial trust in AIMDSS.
3.3.3 Propensity to trust and initial trust
Some individuals are more likely to trust than others, while some not and even more skeptical. Many researchers have considered this different trust propensity from the perspective of an individual’s generalized trust in others, something acts as a personal trait that is stable across different situations and may influence the likelihood that the individual will trust others. This kind of personal trait is referred as the propensity to trust (Rotter 1971). In this study, we define Propensity to trust as “a stable within-party factor that will affect the likelihood the party will trust.” (Mayer et al. 1995). Propensity to trust varies among individuals with different living experiences, cultural backgrounds and personality types. Mayer’s (1995) trust theory argues that propensity to trust plays an important role as an antecedent in individuals’ trust formation, in particularly, when there is no prior interaction between trustor and trustee. Accordingly, while AIMDSS is an emerging technology that most healthcare professionals have no prior interaction with an AIMDSS, they cannot develop trust based on prior experiences or acquire adequate information of AIMDSS. Under such circumstances propensity to trust is argued to be an important determinant of initial trust in AIMDSS, as described in H9.
H9
Propensity to trust has a positive influence on initial trust in AIMDSS.
3.4 Personal innovativeness in IT and AIMDSS adoption
Personal innovativeness refers to the willingness of an individual trying out a new innovation (Agarwal and Prasad 1998). According to DOI, people react differently due to their inherent propensity to adopt a new innovation. Innovative adopters are classified into five categories in this theory: innovators, early adopters, early majority, late majority, and laggards (Rogers 2003). Based on this classification, we propose a concept personal innovativeness in IT which describes the extent to which an individual would like to try out a new IT (Agarwal and Prasad 1998).
People with high innovativeness in IT are more likely to be capable of controlling a new technology than others, and they usually consider using a new technology less complex and difficult. Considering that effort expectancy refers to the degree of difficulty that individuals perceive when using a technology, many studies have explored the relationship between personal innovativeness in IT and effort expectancy. Wu et al. (2011) demonstrated that personal innovativeness in IT significantly affected perceived ease of use, an equivalent construct of effort expectancy, in terms of healthcare professionals in their use of mobile healthcare. Besides, Yi et al. (2006) indicated the positively influence of personal innovativeness on perceived ease of use in the context of PDA acceptance by healthcare professionals. Accordingly, we assume that healthcare professional’s innovativeness in IT positively influences effort expectancy for AIMAD as described in H10.
H10
Personal innovativeness in IT has a positive influence on effort expectancy for AIMDSS.
3.5 Task complexity and AIMDSS adoption
Task complexity refers to the degree of perceived difficulty and load required to accomplish a given task (Gallupe et al. 1988). It may involve high uncertainty and difficulty since there is a lack of understanding or necessary information (Daft et al. 1987). An information system designed for target tasks is required to reduce the uncertainty and difficulty by filling the understanding gab and providing necessary information. In technology acceptance research, task complexity has drawn attention as an important factor to explain individuals’ technology acceptance. The value of a task support technology varies since the technology may play different roles for tasks with different degrees of complexity. In the study of Lee and Rao (2009), in terms of e-government compliance services acceptance by citizens, task complexity was posited as a direct antecedent of relative usefulness on intention to use website for information. In the case of AIMDSS adoption, healthcare professionals confront with simple or complex tasks. For more complex diagnosis tasks, i.e., the diseases are hard to recognize but threaten patients’ life, they may perceive a higher value of AIMDSS than those simple ones. Accordingly, we argue that there is a potential linkage between task complexity and performance expectancy considering the problem of AIMDSS adoption.
H11
Task complexity has a positive influence on effort expectancy for AIMDSS.
3.6 Technology characteristic and AIMDSS adoption
In the context of IS research, technology refers to computer systems, such as hardware, software et al. and user support services designed for supporting users’ tasks (Goodhue and Thompson 1995). Some researchers have discussed the potential linkage between technology characteristic and effort expectancy in the problem of technology adoption. Technology with clearer interfaces and using process may simplify user operation and make the usage less complex. Davis (1993) verified that technology characteristic, specifically, the system design features, had a significant effect on perceived usefulness. In other study of Zhou et al. (2010), technology characteristic was posited as a direct antecedent of effort expectancy toward the behavior of using mobile banking. Accordingly, we argue that there exists a potential relationship between technology characteristic and effort expectancy for AIMDSS.
H12
Technology characteristics have a positive influence on effort expectancy for AIMDSS.
3.7 Perceived substitution crisis and AIMDSS adoption
Individuals’ perceptions of crisis have been studied for many years and regarded as a prominent barrier of IT adoption and usage (Featherman and Pavlou 2003). Now in the context of AIMDSS adoption by healthcare professionals, we specifically consider a new construct, i.e., the substitution crisis triggered by AIMDSS, which refers to concerns of being replaced by the target AIMDSS. With the rapid development of the artificial intelligence applications in medical diagnosis, some concerns have recently been floated that doctors’ authority would be challenged by artificial intelligence products and someday doctors would even be replaced by those products. It is obvious to us that such concerns are one of the most possible barriers of AIMDSS adoption for the protection of their benefits. The following hypothesis H13 is suggested:
H13
Perceived substitution crisis has a negative influence on behavior intention to use AIMDSS.
Figure 2 presents our research model which incorporates the UTUAT, trust theory and other related theories. Specifically, we argue that trust-based factors also play a great role in the formation of AIMDSS adoption by healthcare professionals, besides the general components including performance expectancy, effort expectancy and social influence, proposed in original UTAUT. In addition, four contextual factors, task complexity, technology characteristics, personal innovativeness in IT and perceived substitution crisis, have been placed as potential antecedents of individual adoption in this research model.

AIMDSS adoption model for healthcare professionals
4 Method
4.1 Questionnaire design
Structured questionnaire is one of the most important methods of capturing key factors and their logical relationships in complicated phenomena. We design a structured questionnaire to validate the AIMDSS adoption model for healthcare professionals proposed above.It consists of two parts: the demographic information (e.g., gender, age, professional ranks etc.), and 10 latent constructs in our proposed model. All items except that for perceived substitution crisis (PSC) are adapted from previous studies with proven good validity and reliability. Items for performance expectancy (PE), effort expectancy (EE), social influence (SI), and behavioral intention (BI) are adapted from Venkatesh et al. (2003). Items for initial trust (IT) are adapted from Li et al. (2008). Measurement items for task complexity (TAC) and technology characteristics (TEC) are adapted from Zhou et al. (2010). These items are adjusted in our questionnaire to match the context of AIMDSS adoption among healthcare professionals. Measurement items extracted from personal innovativeness in IT (PIIT) and are propensity to trust (PT) are suggested by Wu et al. (2011) and Li et al. (2008). Since PIIT and PT are personal traits which are relatively invariant across situations, items have remained largely unchanged in our questionnaire. Besides, perceived substitution crisis (PSC) is a relatively new concept in IT adoption studies and there are little literatures about it, we attempt to design items for PSC to capture the essential aspects of the perceived crisis of target AIMDSS. Specifically, four items are designed in consider of possibly crisis in being replaced, independent, unemployment and negatively impacted in diagnosis capacity by using AIMDSS.
Table 2 shows adoption factors proposed in the research model and their measurement items. Each item was measured using five-point Likert scales, with answer choices ranging from “strongly disagree” (1) to “strongly agree” (5).
4.2 Data collection
A survey study including paper survey and Internet survey was conducted to examine the acceptance of AMIAD systems by healthcare professionals. Online survey was posted for a month in sojump.com, a special questionnaire online platform in China. The questionnaire links are only accessible to healthcare professionals. At the same time, paper surveys were sent out to healthcare professionals in Huainan First People’s Hospital and Anhui Chinese medicine hospital. In total, we received 202 questionnaires feedback. Finally, 191 questionnaires were remained for this study by excluding invalid ones, and the valid response rate was 94.5%.
Table 3 shows the demographic profile of the survey respondents. Among the respondents, granted the blank exceptions, 62.83% of the respondents are female, and 36.65% are male. The demographic profile shows that respondents are relatively young since about 76% are under 40 years old.
5 Data analysis and results
Partial least squares (PLS) is a second-generation structural equation modeling (SEM) technique that is used to evaluate causal relationship between latent constructs. Compared to other structural equation modeling (SEM) techniques, like AMOS and LISREL, PLS has advantages when analyzing sample of small size (Wu et al. 2011). In this study, 191 residents are examined, the size of which may not be large enough for AMOS or LISREL technique. Therefore, PLS (Smart-PLS V 3.2.6) is applied for testing the proposed research model in this study.
5.1 Measurement model evaluation
Measurement model evaluation is the first stage in PLS analysis which is used to examine the reliability and validity of each construct (Anderson and Gerbing 1988), which reveals whether the items developed in questionnaire are able to comprehensively and validly measure constructs in AIMDSS adoption model for healthcare professionals. This is the essential prerequisite to validate the model based on questionnaire designed above. Table 4 exhibits the indexes of reliability and convergent validity for the scale. Table 5 exhibits the correlation analysis between each two constructs. The reliability of each construct is discriminated by cronbach’s α values (Lee and Kim 1999). Cronbach’s α values higher than 0.7 indicates good reliability (Hair et al. 2013). Table 4 shows that cronbach’s α value of all constructs exceed 0.7, which indicates a high degree of reliability.
Construct validity include convergent validity and discriminant validity. With regard to convergent validity, it is commonly assessed by three criteria. Firstly, item loadings of all standardized items are supposed to be higher than 0.70 and statistically significant. Thus, TC4 (item loading = 0.570) and TC5 (item loading = 0.606) are deleted. Secondly, composite reliability (CR) for each construct should be higher than 0.8. Thirdly, average variance extracted (AVE) for each construct should be higher than 0.5 (Wu et al. 2011). As shown in Table 4, with TC4 and TC5 removed, all item loadings remained range from 0.724 to 0.928 and all show significant with 0.001 level. CR of each construct is above the suggested value 0.8, and AVE of each construct is above the suggested value 0.5. These criteria jointly demonstrate a high level of convergent validity. Next, with regard to discriminant validity, it is assessed by a rule of thumb that the square root of AVE for each construct is supposed to be higher than its correlations with other constructs (Fornell 1982; Fornell and Larcker 1981). As shown in Table 5, in this study, each square root of AVE for a construct is above its correlation coefficient with other constructs. However, some correlation coefficients between variables seem relatively high, such as correlations between BI and IT (0.836) and correlations between TAC and BI (0.831). Therefore, we conducted a further test for multicollinearity by examining the variance inflation factor (VIF) and tolerance. The criterion is that if the VIF of a construct is higher than 10, then the construct is highly collinear and is inappropriate for regression analysis (Asher 1983). In this study, the VIF ranges from 1.000 to 2.501, far less than the unacceptable value of 10, demonstrating an absence of multicollinearity.
5.2 Structural model evaluation
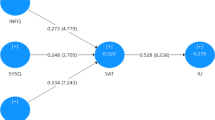
Structural model evaluation is the second stage in PLS analysis for testing hypothesis. Figure 3 shows the PLS results for the proposed structural model, with path coefficients and t-values. First, Initial trust (β = 0.590, p < 0.001), and performance expectancy (β = 0.191, p < 0.01) both all significantly predictive of behavioral intention. Therefore, Hypothesis 5 and 1 are all supported. In contrast, social influence (β = 0.163, p > 0.05), effort expectancy (β = 0.078, p > 0.05), perceived substitution crisis (β = 0.064, p > 0.05) reveals no significance in influencing behavioral intention. Hypothesis 4, 2, and 13 are not supported. In brief, the five constructs, initial trust, performance expectancy, effort expectancy, social influence, and perceived substitution crisis, jointly explain 68.9% of variance in behavioral intention (R2 = 0.689). Next, performance expectancy (β = 0.162, p < 0.05), effort expectancy (β = 0.243, p < 0.01) propensity to trust (β = 0.307, p < 0.001) and social influence (β = 0.307 p < 0.001) all show influence on initial trust (R2 = 0.597), and thus hypothesis 7, 6, 9 and 8 are all supported. In summary, the four constructs, performance expectancy, effort expectancy, propensity to trust and social influence, jointly explain 55.9% of initial trust (R2 = 0.559). The antecedences of performance expectancy (R2 = 0.27) are task characteristics (β = 0.302, p < 0.001) and effort expectancy (β = 0.277, p < 0.01). The two constructs together explain 22.7% of variance in performance expectancy (R2 = 0.227). Hypothesis 11 and 3 are both supported. The antecedences of effort expectancy (R2 = 0.475) are technology characteristics (β = 0.379, p < 0.001) and personal innovativeness in IT (β = 0.379, p < 0.001). The two constructs together explain 48.4% of variance in effort expectancy. Therefore, hypothesis 12 and 10 are supported.

Structure model and path coefficients
6 Discussions
This study aims to explore the behavior intention towards AMIADS by healthcare professionals based upon UTAUT and other related theories. Most of the casual hypotheses of proposed model are supported while there are also a few unexpected results contradicting what we assumed. The following chapter discusses some valuable findings and implications based upon our research results above.
Firstly, the results indicate that initial trust and performance expectancy both have significant effects on behavioral intention of using AMIADS (H5, H1). Moreover, initial trust shows a stronger impact on behavioral intention than performance expectancy (β = 0.563 vs 0.172), which is not consistent with some previous findings that performance expectancy has the greatest impact on behavioral intention. The reason behind this may be the special context of healthcare since it is closely related to peoples’ health. Compared to other IT adopters, healthcare professionals tend to bear more burdens in lives and health issues. Instead of the pursuit of increase in job performance, potential risks on patient’s lives and health may be the most concerns among healthcare professionals about adopting a new product to assist them in medical diagnosis. Therefore, before adopting a new product, healthcare professionals should trust the target products with a higher level compared to other individuals. Trust refers to a degree to what an individual are willingness to assume risks (Mayer et al. 1995). Only when the level of confidence is higher than the perceived risks, individuals will trust in the target object. Therefore, healthcare professionals’ initial trust acts as the key determinants of behavioral intention towards using AMIADS.
Secondly, another interesting finding is the non-significant influence of effort expectancy and social influence on behavioral intention in this study (H2, H4), which are contrary to what was posited in the original UTAUT. However, in an additional experiment, in which the trust-based factors were all excluded from our proposed model, Performance expectancy (β = 0.317, p < 0.001), effort expectancy (β = 0.263, p < 0.01) and social influence (β = 0.263, p < 0.001) all have been well indicated as direct antecedents of behavioral intention toward using AMIADS. The results are basically consistent with the logic in UTAUT. Besides, the model without trust-based factors could only explain 54.8% in the behavioral intention, which are lower than our proposed model including trust-based factors (R2 = 0.548 vs 0.691). The finding reveals a reasonability and necessity to add trust-based factors into original UTAUT framework for a more accurate understanding of healthcare professionals’ acceptance of AMIADS Compared to effort expectancy and social influence, initial trust of AMIAD systems is the determinant factor in formulating the willingness to adopting AMIADS.
Thirdly, the findings show that initial trust towards AMIAD systems rely on four determinants, that is, propensity to trust, performance expectancy, social influence, and effort expectancy (H9, H7, H8, H6). Moreover, initial trust is the most significant determinant that directly affects initial trust compared to other three constructs (β = 0.307 vs 0.243 vs 0.228 vs 0.162). The reason behind this may be healthcare professionals are mainly unfamiliar of AMIAD systems, since AMIAD system now is still an emerging technology and have not been used widely in actual operation. Thus, it is hard for healthcare professionals to build trust through direct experiences or enough knowledge on AMIADS. In such a situation, healthcare professionals with high initial trust are more likely to form trust beliefs towards AMIADS.
Fourthly, the results indicate that task complexity and technology characteristics are two determinants that respectively influence performance expectancy and effort expectancy for using AMIADS (H11, H12). For healthcare professionals with higher task complexity, they have more demands on related instruments or services to help them improve diagnosis accuracy and ease their heavy load of jobs. Besides, the technology characteristics related to diagnosis capacity, interpretability of diagnosis results and interoperability between systems and healthcare professionals (see Table 2) both reveal a high influence on effort expectancy for using AMIADS.
Finally, the results indicate that perceived substitution crisis reveals no significant impact in influencing healthcare professionals’ behavioral adoption towards using AMIAD systems (H13), which is inconsistent with our proposed hypothesis. This unexpected finding can be explained reasonably. The results of the experiment for examining the extent of perceived substitution crisis show that its average value is relatively lower than other factors. It is mainly because that artificial intelligence applications in medical diagnosis just have started and there are few mature products which can be actually applied to practical usage in China. Healthcare professionals have not felt much crisis that they would be totally replaced by those artificial intelligence products someday. Therefore, perceived substitution crisis is not an important determinant of behavioral intention toward AMIAD systems under these circumstances.
7 Implications
7.1 Contributions to theory
Firstly, we conduct a comprehensive study on healthcare professional’s behavioral intention to adopt AMIADS, which focuses on the unique features in healthcare context and looks deep into the decision process of an individual to adopt a new technology. While extensive studies have discussed healthcare professional adoption of various applications, none of them have focused on the application of artificial intelligence in medical diagnosis, which is expected to have a wide application prospect in future medical field (Wu et al. 2011; Yang et al. 2015). This study attempts to explain the healthcare professionals’ behavior to apply AMIADS in their daily work. Thus, our research extends the research by introducing a new adoption object.
Secondly, this study integrates UTAUT with trust theory to explain the adoption behavior in an IS context. In particular, our study makes a clear distinction for different stages of trust, which is largely be overlooked by previous researchers on novel technology acceptance. In a context of AMIADS acceptance, we emphasize the initial stage of trust in AMIADS, where healthcare professionals have no prior interaction with AMIADS in reality. Besides, we firstly introduce initial trust as a mediator between existing constructs in the original UTAUT and behavioral intention. While UTAUT has been widely used for analyzing human adoption behavior in various domains, those studies mainly focused on adding determinant factors which influence the behavior into the original UTAUT (Or et al. 2011; Zhou et al. 2010; Kijsanayotin et al. 2009). However, there is inadequate research considering a potential mediator between existing factors and behavior intention. This study is the first attempt to expand the UTAUT theory with a potential mediator to explore individual adoption behavior for a novel technology. At first, we present a trust-based theoretical framework to understand individual decision process of adopting a technology. The framework origins from varies IS trust researches and adapted to the healthcare service adoption domain. According to the logic of trust-based theoretical framework, we integrate UTAUT with trust-based factors. The initial trust is presented and tested as a mediator between existing constructs (effort expectancy, social influence and performance expectancy) in the original UTAUT and behavioral intention. We consider it since healthcare professionals tend to be conservative about adopting a new technology because their work closely related to patients’ lives and health. Thus, this study extends both existing UTAUT research and technology adoption research in a context of healthcare.
Thirdly, this study has considered several dimensions of personal traits in the individual technology acceptance analysis. However, unlike most other studies that simply considered innovation-based factors (e.g., personal innovativeness in IT or computer anxiety) from the perspective of psychological state, our study also considers a trust-based factors, initial trust, to accurately identify individual differences in the adoption of a new technology. Results show that initial trust plays a significant role in increasing the willingness of healthcare professionals to adopt AMIADS. This indicates the need to consider personality differences from the perspective of initial trust in the technology acceptance analysis.
Fourthly, few researchers have considered the role of task complexity and technology characteristics in the context of healthcare professional adoption of a novel technology. We consider this respectively from two perspectives: individual and technology states. Individuals who perceive different degrees of complexity for a given task have different degrees of perceived usefulness (Lee and Rao 2009). From the perspective of technology, we mainly consider interactivity and interpretability of AMIADS based on the preliminary findings of healthcare professionals’ preferences on an assistant diagnosis tool. Our study demonstrates the significant impact of the two predictors on the behavioral intention of AMIADS acceptance. This presents a broader view of potential antecedents of behavioral intention for healthcare professional.
7.2 Implications for practice
From a practice perspective, several implications can be drawn from this study. First, this study demonstrates initial trust as the most significant predictor of AMIADS adoption among healthcare professionals, which suggests AMIADS manufactures how to attract potential customers: they need to enhance healthcare professional’ trust in AMIADS. Our study reveals several ways to improve healthcare professionals initial trust in AMIADS. To begin with, the AMIADS manufactures should consider both two factors when develop their products, i.e., ease of use and usefulness. In order to enhance ease of use, two types of technology characteristics, interpretability of diagnosis results and interoperability between systems and healthcare professionals should be considered in the product development. If AMIADS can offer a detailed explanation of how they accomplish the diagnosis, or give healthcare professionals a certain leading role during the process of assistant diagnosis, the degree to which healthcare professionals trust in AMIADS would be largely increased.
From the perspective of usefulness, apart from the improvement of accuracy and efficiency of diagnosis, our study also indicates that task complexity largely influences performance expectancy for using AMIADS. For healthcare professionals who need to diagnose relatively more complex diseases, they have more demands for related instruments or services to help them improve diagnosis performance and ease their heavy load of jobs. This group of healthcare professionals shows a larger behavioral intention towards using AMIAD systems compared to those with easier tasks. This may have an indication that AMIAD system developers should continuously pay attention to researches on complex and high-risk diseases diagnosis, and develop more high-quality products oriented to such diseases.
8 Conclusions
To promote the behavioral intention of AMIADS adoption by healthcare professionals, we propose an integrated model based on UATUT, trust theory and other related factors to understand AMIADS acceptance behavior among healthcare professionals, and conducted an empirical study to examine our proposal. Except perceived substitution risks, the other eight factors all are indicated as significant predictors of healthcare professionals acceptance of AMIADS. Besides, there is an important find that initial trust is a significant predictor of healthcare professionals AMIADS adoption and a mediator between existing factors in the original UTAUT and behavioral intention of using AMIADS. In view of this, our study extends the healthcare professional adoption research and proposes a new way to improve the original UTAUT for a better understanding of healthcare professionals adoption of AMIADS. Furthermore, we provide a development insight for AMIADS manufacturers to make their products more acceptable.
There are some limitations in our study. Firstly, our research didn’t measure actual usage of AMIADS adoption. Subsequent research should address the issue of measuring the actual usage of AMIADS to analyze the conversion rate between behavioral intention and actual acceptance of technology. Secondly, in this paper, data collection was geographically limited to China. As AMIADS adoption is a worldwide phenomenon, replication of the findings across different geographical contexts is necessary. Future studies should be cross-region. Thirdly, we did not consider potential moderators of the relationships between key factors while many studies have indicated the age and gender have moderate effects on technology acceptance behavior. This may cause a deviation against the current findings. Future research can take potential moderators, e.g., gender, age, professional ranks etc. into consideration. Fourthly, the size of residents is lower than desirable for all of our efforts. Future research should overcome those difficulties to obtain a desirable size of residents for a more appropriate result.
Notes
References
Abushanab, E., & Pearson, J. M. (2007). Internet banking in Jordan: The unified theory of acceptance and use of technology (UTAUT) perspective. Journal of Systems & Information Technology, 9(1), 78–97.
Agarwal, R., & Prasad, J. (1998). A conceptual and operational definition of personal innovativeness in the domain of information technology. Information Systems Research, 9(2), 204–215.
Ajzen, I. (1991). The theory of planned behavior. Research in Nursing & Health, 14(2), 137–144.
Alharbi, S. T. (2014). Trust and acceptance of cloud computing: A revised UTAUT model. In International conference on computational science and computational intelligence (Vol.2, pp. 131–134). IEEE.
Alshehri, M., Drew, S., & Alghamdi, R. (2013). Analysis of citizens acceptance for e-government services: Applying the UTAUT model.
Anderson, J. C., & Gerbing, D. W. (1988). Structural equation modeling in practice: A review and recommended two-step approach. Psychological Bulletin, 103(3), 411–423.
Asher, H. B. (1983). Causal modeling (2nd ed.). Thousand Oaks: Sage Publications.
Bansal, G., Zahedi, F. M., & Gefen, D. (2010). The impact of personal dispositions on information sensitivity, privacy concern and trust in disclosing health information online. Decision Support Systems, 49(2), 138–150.
Chang, I. C., Hwang, H. G., Hung, M. C., Lin, M. H., & Yen, D. C. (2007). Factors affecting the adoption of electronic signature: executives’ perspective of hospital information department. Decision Support Systems, 44(1), 350–359.
Chaouali, W., Yahia, I. B., & Souiden, N. (2016). The interplay of counter-conformity motivation, social influence, and trust in customers’ intention to adopt internet banking services: the case of an emerging country. Journal of Retailing & Consumer Services, 28, 209–218.
Chew, F., Grant, W., & Tote, R. (2004). Doctors on-line: using diffusion of innovations theory to understand internet use. Family Medicine, 36(9), 645.
Chiu, C. M., Hsu, M. H., Lai, H., & Chang, C. M. (2012). Re-examining the influence of trust on online repeat purchase intention: The moderating role of habit and its antecedents. Decision Support Systems, 53(4), 835–845.
Cimperman, M., Makovec, B. M., & Trkman, P. (2016). Analyzing older users’ home telehealth services acceptance behavior-applying an extended utaut model. International Journal of Medical Informatics, 90, 22–31.
Daft, R. L., Lengel, R. H., & Trevino, L. K. (1987). Message equivocality, media selection, and manager performance: implications for information systems. MIS Quarterly, 11(3), 355–366.
Davis, F. D. (1989). Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Quarterly, 13(3), 319–340.
Davis, F. D. (1993). User acceptance of information technology: System characteristics, user perceptions and behavioral impacts. International Journal of Man–Machine Studies, 38(3), 475–487.
Deng, Z., Mo, X., & Liu, S. (2014). Comparison of the middle-aged and older users’ adoption of mobile health services in China. International Journal of Medical Informatics, 83(3), 210.
Dulle, F. W., & Minishi-Majanja, M. K. (2011). The suitability of the unified theory of acceptance and use of technology (UTAUT) model in open access adoption studies. Information Development, 27(1), 32–45.
Er, O., Tanrikulu, A. Ç., & Abakay, A. (2015). Use of artificial intelligence techniques for diagnosis of malignant pleural mesothelioma. Dicle Medical Journal, 42(1), 5–11.
Esteva, A., Kuprel, B., Novoa, R. A., Ko, J., Swetter, S. M., Blau, H. M., & Thrun, S. (2017). Dermatologist-level classification of skin cancer with deep neural networks. Nature, 542(7639), 115.
Featherman, M. S., & Pavlou, P. A. (2003). Predicting e-services adoption: A perceived risk facets perspective. Cambridge: Academic Press, Inc.
Fornell, C. (1982). A second generation of multivariate analysis. Santa Barbara: Praeger.
Fornell, C., & Larcker, D. F. (1981). Evaluating structural equation models with unobservable variables and measurement error. Journal of Marketing Research, 18(1), 39–50.
Gagnon, M. P., Ngangue, P., Paynegagnon, J., & Desmartis, M. (2015). M-health adoption by healthcare professionals: a systematic review. Journal of the American Medical Informatics Association Jamia, 54(1), 334–336.
Gallupe, R. B., Desanctis, G., & Dickson, G. W. (1988). Computer-based support for group problem-finding: An experimental investigation. MIS Quarterly, 12(2), 277–296.
Gefen, D., Karahanna, E., & Straub, D. W. (2003). Trust and tam in online shopping: an integrated model. MIS Quarterly, 27(1), 51–90.
Gefen, D., Rose, G. M., Warkentin, M., & Pavlou, P. A. (2008). Cultural diversity and trust in it adoption: A comparison of potential e-voters in the USA and South Africa. Journal of Global Information Management, 13(1), 54–78.
Goodhue, D. L., & Thompson, R. L. (1995). Task-technology fit and individual performance. MIS Quarterly, 19(2), 213–236.
Gu, Z., Wei, J., & Xu, F. (2015). An empirical study on factors influencing consumers’’ initial trust in wearable commerce. Data Processor for Better Business Education, 56(1), 79–85.
Hair, J. F., Black, W. C., Babin, B. J., Anderson, R. E., & Tatham, R. L. (2013). Multivariate data analysis. Technometrics, 30(1), 130–131.
Hilliard, M. E., Hahn, A., Ridge, A. K., Eakin, M. N., & Riekert, K. A. (2014). User preferences and design recommendations for an mhealth app to promote cystic fibrosis self-management. JMIR mHealth & uHealth, 2(4), e44.
Hoque, M. R. (2016). An empirical study of mhealth adoption in a developing country: The moderating effect of gender concern. BMC Medical Informatics and Decision Making, 16(1), 51.
Hung, M. C., & Jen, W. Y. (2012). The adoption of mobile health management services: An empirical study. Journal of Medical Systems, 36(3), 1381.
Ke, W., Liu, H., Wei, K. K., Gu, J., & Chen, H. (2009). How do mediated and non-mediated power affect electronic supply chain management system adoption? The mediating effects of trust and institutional pressures. Decision Support Systems, 46(4), 839–851.
Kelman, H. C. (1958). Compliance, identification, and internalization: three processes of attitude change. Journal of Conflict Resolution, 2(1), 51–60.
Kijsanayotin, B., Pannarunothai, S., & Speedie, S. M. (2009). Factors influencing health information technology adoption in Thailand’s community health centers: Applying the UTAUT model. International Journal of Medical Informatics, 78(6), 404–416.
Kim, S., Lee, K. H., Hwang, H., & Yoo, S. (2016). Analysis of the factors influencing healthcare professionals’ adoption of mobile electronic medical record (EMR) using the unified theory of acceptance and use of technology (UTAUT) in a tertiary hospital. BMC Medical Informatics and Decision Making, 16(1), 1–12.
Lai, I. K. W., Tong, V. W. L., & Lai, D. C. F. (2011). Trust factors influencing the adoption of internet-based interorganizational systems. Electronic Commerce Research and Applications, 10(1), 85–93.
Lee, J. N., & Kim, Y. G. (1999). Effect of partnership quality on is outsourcing success: conceptual framework and empirical validation. Journal of Management Information Systems, 15(4), 29–61.
Lee, J. K., & Rao, H. R. (2009). Task complexity and different decision criteria for online service acceptance: A comparison of two e-government compliance service domains. Decision Support Systems, 47(4), 424–435.
Li, X., Hess, T. J., & Valacich, J. S. (2006). Using attitude and social influence to develop an extended trust model for information systems. ACM Sigmis Database, 37(2–3), 108–124.
Li, X., Hess, T. J., & Valacich, J. S. (2008). Why do we trust new technology? A study of initial trust formation with organizational information systems. Journal of Strategic Information Systems, 17(1), 39–71.
Lu, B., Zhang, T., Wang, L., & Keller, L. R. (2016). Trust antecedents, trust and online microsourcing adoption. Decision Support Systems, 85(C), 104–114.
Luhmann, N. (1982). Trust and power. Chichester: Wiley.
Maguire, R., Mccann, L., Miller, M., & Kearney, N. (2009). Nurse’s perceptions and experiences of using of a mobile-phone-based advanced symptom management system (ASYMS) to monitor and manage chemotherapy-related toxicity. European Journal of Cancer Care, 18(2), 156–164.
Mayer, R. C., Davis, J. H. F., & Schoorman, F. D. (1995). An integrative model of organizational trust. Academy of Management Review, 20(3), 709–734.
Mcknight, D. H. (2005). Trust in information technology. The Blackwell encyclopedia of management. Vol. 7 management information systems. Malden: Blackwell Publications.
Oliveira, T., Faria, M., & Thomas, M. A. (2014). Extending the understanding of mobile banking adoption: When UTAUT meets TTF and ITM. International Journal of Information Management the Journal for Information Professionals, 34(5), 689–703.
Or, C.K.L., Karsh, B. T., Severtson, D. J., Burke, L. J., Brown, R. L., & Brennan, P. F. (2011). Factors affecting home care patients’ acceptance of a web-based interactive self-management technology. Journal of the American Medical Informatics Association Jamia, 18(1), 51–59.
Rogers, E. M. (2003). Diffusion of Innovations, (5th ed.). New York: Free Press Edition.
Rotter, J. B. (1971). Generalized expectancies for interpersonal trust. American Psychologist, 26(5), 443–452.
Terry, H.P., Hulsing, J., Grant, M., Powell, D., Mubayi, P., & Syed, W. (2016). AI, Machine learning and data Fuel the future of productivity. The Golden Sachs Group, Inc. November 14.
Toth-pal, E., Wårdh, I., Strender, L. E., & Nilsson, G. (2008). Implementing a clinical decision-support system in practice: A qualitative analysis of influencing attitudes and characteristics among general practitioners. Medical Informatics, 33(1), 39–54.
Tornatzky, L. G., & Fleischer, M. (1990). Processes of technological innovation. Lexington, KY: Lexington Books.
Tung, F. C., & Chou, C. C. M. (2008). An extension of trust and tam model with IDT in the adoption of the electronic logistics information system in his in the medical industry. International Journal of Medical Informatics, 77(5), 324.
Venkatesh, V., Moris, M. G., Davis, G. B., & Davis, F. D. (2003). User acceptance of information technology: Toward a unified view. MIS Quarterly, 27(3), 425–478.
Venkatesh, V., Thong, J. Y. L., Chan, F. K. Y., Hu, J. H., & Brown, S. A. (2011). Extending the two-stage information systems continuance model: Incorporating UTAUT predictors and the role of context. Information Systems Journal, 21(6), 527–555.
Wallace, S., Clark, M., & White, J. (2012). ‘It’s on my iphone’: Attitudes to the use of mobile computing devices in medical education, a mixed-methods study. BMJ Open, 2(4), e001099.
Wang, W., & Benbasat, I. (2005). Trust in and adoption of online recommendation agents. Journal of the Association for Information Systems, 6(3), 4.
Wang, Y. S., Wu, M. C., & Wang, H. Y. (2009). Investigating the determinants and age and gender differences in the acceptance of mobile learning. British Journal of Educational Technology, 40(1), 92–118.
Wiggins, C., Trimmer, K., Beachboard, J., & Peterson, T. (2009). Prior experience and physicians’ intentions to adopt EMR. In Hawaii international conference on system sciences (pp. 1–9). IEEE Computer Society.
Wu, I. L., Li, J. Y., & Fu, C. Y. (2011). The adoption of mobile healthcare by hospital’s professionals: An integrative perspective. Decision Support Systems, 51(3), 587–596.
Xue, L., Yen, C. C., Chang, L., Chan, H. C., Tai, B. C., Tan, S. B., Duh H. B. L., & Choolani, M. (2012). An exploratory study of ageing women’s perception on access to health informatics via a mobile phone-based intervention. International Journal of Medical Informatics, 81(9), 637–648.
Yan, H., & Pan, K. (2015). Examining mobile payment user adoption from the perspective of trust transfer. International Journal of Networking and Virtual Organisations, 8(1), 117–130.
Yang, H., Guo, X., & Wu, T. (2015). Exploring the influence of the online physician service delivery process on patient satisfaction. Decision Support Systems, 78(1), 113–121.
Yang, Z., Kankanhalli, A., Ng, B. Y., & Lim, J. T. Y. (2013). Analyzing the enabling factors for the organizational decision to adopt healthcare information systems. Decision Support Systems, 55(3), 764–776.
Yi, M. Y., Jackson, J. D., Park, J. S., & Probst, J. C. (2006). Understanding information technology acceptance by individual professionals: Toward an integrative view. Information & Management, 43(3), 350–363.
Zhang, X., Guo, X., Lai, K. H., Guo, F., & Li, C. (2014). Understanding gender differences in m-health adoption: A modified theory of reasoned action model. Telemedicine Journal and e-Health: The Official Journal of the American Telemedicine Association, 20(1), 39–46.
Zhou, T., Lu, Y., & Wang, B. (2010). Integrating TTF and UTAUT to explain mobile banking user adoption. Computers in Human Behavior, 26(4), 760–767.
Acknowledgements
This work is supported by the National Natural Science Foundation of China (Nos. 71501058, 71601065, 71690235 and 71690230), and Innovative Research Groups of the National Natural Science Foundation of China (71521001). Panos M. Pardalos is partially supported by the project of “Distinguished International Professor by the Chinese Ministry of Education” (MS2014HFGY026).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Fan, W., Liu, J., Zhu, S. et al. Investigating the impacting factors for the healthcare professionals to adopt artificial intelligence-based medical diagnosis support system (AIMDSS). Ann Oper Res 294, 567–592 (2020). https://doi.org/10.1007/s10479-018-2818-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10479-018-2818-y