
Abstract
Access to safe and effective sexual healthcare services for transgender and male sex workers (TMSW) is a human right. Globally, TMSW experience a higher prevalence of human immunodeficiency virus (HIV) and sexually transmitted infections than the general population or other sex workers, suggesting the existence of unique challenges for this group when accessing healthcare. A systematic database search identified 22 qualitative papers addressing barriers to accessing sexual healthcare services for TMSW. These papers were critically evaluated for adherence to best practice standards for qualitative research and research with sex workers. A coding process identified five themes. Stigma was the predominant barrier, and was divided into stigma related to sexuality, gender identity, HIV status, sex worker status, and internalised stigma. Other barriers were confidentiality concerns, sexual health literacy, fatalism, and structural barriers. Each of these themes were informed by the wider context of stigma. The literature presents a complex syndemic of social disadvantage and exclusion acting to produce and reinforce health disparities related to sexual health and access to screening and treatment for TMSW.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Accessing safe and effective sexual healthcare services for transgender and male sex workers (TMSW) is a human right [1, 2]. However, TMSW experience disproportionately high prevalence of human immunodeficiency virus (HIV) and sexually transmitted infections (STI) in low, middle, and high-income countries [3,4,5]. This disease burden has made TMSW a priority population within the worldwide HIV response [6].
Epidemiological evidence regarding the sexual health of TMSW is limited. Few countries provide HIV/STI prevalence data for TMSW as a population [6, 7]. The available evidence, however, does indicate higher prevalence of HIV among male sex workers (MSW) in comparison to female sex workers (FSW), and in comparison to men who have sex with men (MSM) not engaged in sex work [8, 9]. This difference is more acute in Latin America and Sub-Saharan Africa [10]. In many parts of the world transgender sex workers (TSW) also experience a larger HIV burden than MSW or FSW [4].
The greater burden of HIV/STIs within this population suggests that TMSW may face unique barriers to accessing healthcare. The accessibility of sexual health screening, counselling, and treatment can be restricted in settings pervaded by stigma, marginalisation, and resource constraints [11, 12], thereby contributing towards serious disparities in health [11,12,13]. TMSW can experience discrimination related to sexual identity, gender identity, or sex work-related stigma [14,15,16]. Stigma related to HIV can also discourage sex workers from accessing testing, delaying diagnosis and treatment [17]. Multiple co-existing forms of stigma have been implicated in reduced service access and HIV disparities between ethnic groups [18] and for MSM [19] and FSW [20,21,22]. However, limited research has addressed the social and cultural contexts that produce these access barriers for TMSW.
Understanding the complex process of healthcare access for TMSW requires research approaches that move beyond a focus on measuring individual HIV-related ‘risk’ [23]. TMSW encompass a diversity of experiences, strengths, and needs which necessitate a research methodology that can capture these realities [24]. Quantitative research can be prone to under-reporting or misclassification of TMSW in contexts where transgender identities are not acknowledged, or same-sex relationships are criminalised [25]. Divergent research methods, and varied definitions of sex work also complicate sample comparisons, and challenge generalised understandings of TMSW as a population [7]. Sex workers are considered a ‘hard to reach’ group due to structural factors such as stigma and criminalisation [26]. Hard to reach populations can be more difficult for quantitative researchers to access due to inflexible research protocols and resource limitations [27]. Survey or questionnaire formats can also potentially efface some of the complex local nuances of hard to reach groups in dynamic environments [28, 29]. Qualitative approaches such as semi-structured interviews, focus groups, and ethnographic fieldwork have been effectively utilised to explore the social reality of service barriers for this population [30,31,32,33,34,35]. Qualitative data can depict the individual and their environment with the depth and specificity necessary to understand complex social and biomedical processes such as the accessing of sexual healthcare by marginalised groups [29]. This paper reviews and summarises qualitative research addressing TMSW access to sexual healthcare.
In addition to identifying sexual healthcare access barriers for TMSW, this review also aimed to examine validity and ethics in qualitative sex worker research. Despite the significant complexities and methodological challenges when engaging in research with TMSW [36], and calls for more research into sex worker health [37], there is to date no set of principles to guide ‘best practice’ research in this area. Some of the ethical and methodological issues encountered in research with marginalised groups are addressed by community based participatory research (CBPR), which has been described as ‘best practise’ in this area [38,39,40]. CBPR foregrounds equitable partnerships and tangible community benefits, by developing research practices that empower sex workers as drivers of research priorities and protect sex worker participants from exploitation [36, 40, 41]. As part of the review process for this paper, a set of guiding principles were developed based on literature regarding ethics and standards for research with sex workers, with an emphasis on the CBPR model [36, 41,42,43]. These principles enabled the authors to explore how TMSW have been engaged and empowered by research conducted around their community.
Methods
Search Strategy
The review was conducted as per the PRISMA guidelines [44]. Systematic database searches were conducted of Cochrane Library, PsycINFO, PubMed, Scopus, and Sociological Abstracts. The search was restricted to research published since 2000 to focus on contemporary literature. Medical subject heading (MeSH) terms and plain text words were used. These databases were searched using the following terms: ‘sex work’, ‘male sex work’, transgender, prostitut*, and HIV. The intention was to use a high sensitivity, low specificity search strategy to collect all research related to TMSW. Given the limitations of database indexing, these searches were supplemented by a hand search of titles and abstracts in the following journals: AIDS and Behavior, Transgender Health, International Journal of Transgenderism, The Lancet HIV, HIV and AIDS Review, Culture, Health and Sexuality, and Journal of HIV/AIDS and Social Services. These journals were selected based on their scope and history of publishing research relevant to the research question. Grey literature such as government reports, case reports, reviews, and opinion pieces, and unpublished university theses were excluded. Results were imported into bibliographic management software Endnote.
Papers selected for inclusion were original qualitative research articles published in a peer reviewed journal after the year 2000. Additional criteria were that all or part of the sample were specified to be TMSW, and that barriers to accessing sexual healthcare services experienced whilst engaging in sex work were either discussed by participants or by the authors in their findings or discussion.
The initial database search results were subject to a title and abstract review, which selected original peer reviewed articles, published since 2000 and with an appropriate sample. During the full manuscript review papers were evaluated for discussion by participants or authors of barriers to accessing sexual healthcare services. A large body of research has focused on factors experienced by TMSW which are also known to be barriers to healthcare access, such as criminalisation, marginalisation, and mental health concerns. Papers were only included if participants or the author discussed these issues explicitly in the context of healthcare access. The original database search included both quantitative and qualitative research, as it was unknown whether enough qualitative research addressing the research question was available to permit a meaningful review and meta-summary. Once it was established a significant number of papers remaining after full manuscript review used qualitative methods, studies that utilised only quantitative measures were excluded. Manual inspection was then conducted of the reference lists in the final sample of qualitative papers.
Study Quality Assessment
The basic details and quality scores of each study are reported in Table 1. Two authors independently reviewed the final sample and assigned quality scores using the standardised 14 item quality appraisal checklist developed by the National Institute for Health and Care Excellence (NICE) [45]. One of three quality scores could be applied (++, +, or −), indicating whether the article fulfilled nearly all the criteria, some criteria, or very few of the criteria. The purpose of this review was to appraise the methodological rigor and theoretical consistency of the sample [46]. This framework was selected due to its utilisation in multiple reviews of similarly marginalised populations [47, 48]. This appraisal did not influence whether studies were included in the review.
The articles were then evaluated for adherence to best practise standards in the field of sex worker research. In the absence of established criteria, a set of general principles were developed for best practise research with sex workers based on a review of the literature regarding sex worker research methodologies [36, 40, 41, 43] and with an emphasis on the principles of CBPR [38, 42]. These guiding principles are detailed in Table 2 and were endorsed by a steering committee of sex worker representatives who were also advising on a qualitative research project that was informed by this review at the University of Queensland. These principles were translated into a ranking system mirroring that used by NICE [45] and employed for the critical appraisal process in this review. Articles were awarded one of three quality scores (++, +, or −), based on whether they demonstrated adherence to all, some, or none of these guiding principles.
Data Extraction
Descriptive details of the sample were extracted into a standardised tool. These details included the authors, year of publication, aims of the study, country in which the study was conducted, sample characteristics, method of data collection and analysis, and limitations. The results and discussion sections of each study were then read multiple times to identify mentions of perceived and experienced barriers to service access for TMSW. Findings and conclusions relevant to the research question were then extracted to identify first order constructs within participant quotes, and second order constructs in the author’s discussions [49]. In two studies which included cis-gendered FSW [50, 51], when authors made comments regarding the experiences of their sample without specifying the gender of particular participants, these were not included in the data analysis.
Data Synthesis
Thematic anlaysis was the primary method of analysis used by the articles included in this review, providing descriptive summaries of the data. Therefore a ‘qualitative meta-summary’ approach was utilised as the most appropriate method of synthesis [52]. An open coding process was used to categorise barriers into distinct and separable themes. In cases where very few papers identified a certain barrier, this was incorporated under another heading where appropriate. After this coding process, the results were entered into a table to assess the prevalence of each identified barrier. These themes are summarised in Table 3.
Results
Sample Selection
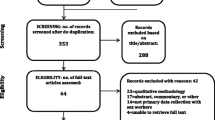
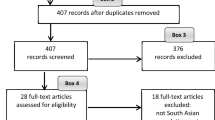
The literature search process is summarised in Fig. 1. The database search and hand search of relevant journals identified 1236 different articles and reports, 394 of which were found to be published original research related directly to TMSW, based on title and abstract screening. After full manuscript review, 19 qualitative articles were selected. This sample included two papers derived from the same research study as they addressed different elements of service access [53, 54]. Two articles included in this sample were the result of hand searches [55, 56]. Reference list searches of this final sample of 19 identified three additional articles for inclusion [17, 30, 57].

Flowchart of literature search and identification process
Study Characteristics and Methodology
The most common geographic locations of the selected studies were North America (n = 6), Asia (n = 6), and Africa (n = 5). The studies were published between 2008 and 2017. Eighteen papers included MSW in their sample, nine of which focused on MSW alone. Six papers reported on the sexual identities of the MSW participants and included heterosexual, bisexual, and gay-identifying men. Twelve studies included transgender participants, and seven involved both male and transgender sex workers. Only one paper specified including female-to-male transgender participants [58]. This paper described female-to-male transgender sex workers with male clients, whereas all other papers with transgender participants focused on transgender women with male clients and who engaged in personal relationships with men. Other studies examined a combination of male and female sex workers [50, 57], or female, male, and transgender sex workers [51, 59]. Five papers were not intentionally focusing on sex work but had sex workers included in their sample as an incidental result of their sampling methods [17, 30, 35, 55, 58].
The majority of the papers included in this review used qualitative in-depth interviews as their research method. Two studies used focus group discussions [31, 60]. Six papers used both in-depth interviews and focus groups [35, 51, 53, 57, 58, 61]. Three papers used mixed methods, including qualitative in-depth interviews and cross-sectional quantitative surveys [59, 62, 63]. Three papers combined ethnographic fieldwork with qualitative interviews [57, 64, 65].
Seven papers included in the sample used thematic analysis as an analytic approach [31, 34, 50, 51, 53, 56, 59]. Another eight papers did not report a specific method for analysing data, however most described an inductive process of coding transcripts and identification of themes [32, 54, 57, 58, 60, 61, 64, 65]. The remaining papers ascribed to framework analysis [33], cross-case analysis [55], the constant comparative method [17, 30], descriptive content analysis [62], grounded theory approach [63], and concept analysis [35].
Results of the critical appraisal process using the NICE [45] guidelines are included in Table 1. Seven papers achieved a (++) rating, 12 were rated (+) and 4 were rated (−). The most common limitation observed when applying the NICE guidelines was a lack of methodological transparency, such as discussion of recruitment, researcher characteristics or training, and ethical considerations. Papers were also evaluated according to the five best practise principles for research with sex workers developed for this review. Overall, this sample exhibited few features of best practise sex worker research. Only one study described a process of involving sex worker representatives in the research process [34]. Reza-Paul et al. [57] frame their research as a staged evaluation of a community-based intervention, and therefore also describe examples of empowering their respondents through a participatory action research process. The use of peer-researchers has been increasingly recognised as an effective approach to overcome power differences and increase qualitative data validity [66], however this sample rarely engaged peer-researchers at any stage. The limited use of empowerment-focused research methods is a critical limitation of some articles in this review.
Clear descriptions of author’s theoretical positioning is necessary to determine the orientation of a research project towards key issues in sex work research such as human rights, harm reduction, and strengths-based intervention [36]. Adequate explanations and justifications for the use of conceptual frameworks are also of particular importance in the context of qualitative research with marginalised populations, and are another component of the NICE guidelines [45]. The orientation of the researcher’s conducting the studies in this review towards gender, sexuality, or sex work theory, and the subsequent theoretical and conceptual frameworks for their research were often unclearly reported. Several studies in this review did refer conceptually to the influence of stigma across multiple levels of social organisation [30, 55, 63]. Others provided insightful and nuanced thematic descriptions [32, 56, 62]. In each of these cases, however, these allusions and descriptions did not extend to interpretive or theoretical analysis of results in the context of sex work theory. Xavier et al. [58] provided a rich introductory account of stigma concepts and their potential application to transgender healthcare, however this framework was not brought to bear on their findings. The strongest application of interpretive theory in this sample was by Samudzi and Mannell [31] in their use of hegemonic masculinity concepts [67] to understand gender identity and exclusion in South Africa. There is a need for engagement in more theoretically engaged research with TMSW to further develop the valuable findings of these studies.
Themes
The themes identified via the meta-summary process are presented in Table 3. Stigma was reported as the most significant barrier. Five forms of stigma were identified: that relating to sexuality, gender identity, sex work history, HIV, and also internalised stigma. Four other barriers to accessing sexual healthcare services for TMSW were identified: confidentiality concerns, fatalism, sexual health literacy, and structural barriers.
Stigma
The predominant barrier to accessing sexual healthcare services identified in this review was a multi-dimensional experience of stigma, which emerged as a theme in all but one study [53]. These experiences of stigma included stigma related to HIV [62, 63], MSM status [32, 56], gender identity [33, 35], sex work [51, 56], and internalised stigma. The concept of internalised stigma refers to occasions where individuals may endorse stereotypes about themselves, or anticipate social rejection [68], and was observed by eight studies in this review [31, 32, 34, 35, 54, 60, 63, 64]. Multiple mental health concerns were incorporated under this theme, including substance use, depression, and low self-efficacy. Whilst there are many factors that can cause or exacerbate these issues, the participants and researchers in these studies interpreted, and understood them to be a result of, internalised stigma, and a barrier to effectively accessing sexual healthcare services. Most authors did not identify particular overriding forms of stigma for TMSW, instead citing the interactive and compounding nature of these various forms of marginalisation.
Enacted and perceived stigma was experienced frequently from healthcare workers. This occurred along a broad spectrum, from the US where participants reported a lack of competency in transgender healthcare and undue focus on the patient’s sex work history [58], to blatant disregard for patient confidentiality [51], ridicule [31], or complete refusal of care in some contexts in Sub-Saharan Africa [56]. Cultural conservatism in Malaysia and Lebanon also exacerbated cultural taboos related to MSM or gender diversity within the healthcare system and was a further impediment to HIV education and prevention efforts [32, 33].
The consequences of stigma were wide-ranging and interacted in complex ways. Some MSW avoided HIV testing, due to fear of their sexual behaviour becoming known to partners, family, or their community [31, 32, 55, 62]. One study in Puerto Rico investigated attitudes towards HIV self-tests, and found that TMSW would not use a self-test with clients in case a positive test caused the client to become aggressive or violent [59]. Some transgender participants in the US were concerned that a HIV diagnosis could exacerbate the stigma they already experience and result in further marginalisation from their community [58]. Stigma also operated within TMSW networks. MSW working in a Lebanese brothel avoided testing because they knew they would lose their employment if the proprietor discovered they were HIV-positive [32]. Some TSW in Guatemala feared that a HIV diagnosis would alienate them among their peers, endangering the fragile social sphere in which they had found security and acceptance [55]. Stigma can also limit the care that TMSW receive when they do access health services. In addition to the examples of direct discrimination highlighted above, the fear of stigma caused some TMSW participants in Sub-Saharan Africa to not disclose the actual reason for their presentation if it was related to their sexual behaviour or sex work [51, 61]. This could result in the provision of incorrect health advice, insufficient risk counselling or disease screening, and inappropriate medication prescriptions.
Confidentiality
Eleven studies in the sample identified concerns over confidentiality to be a barrier to access [30, 31, 34, 50, 51, 53, 55, 58, 62, 63, 65]. This included concerns about being seen attending a HIV testing service, or the staff breaching their confidentiality to co-workers or other people outside the clinic [34, 55]. These concerns were more pronounced in less metropolitan areas where privacy was more difficult to maintain [58]. Some respondents travelled long distances to access clinics unconnected to their local communities to ensure confidentiality [55]. In some resource poor contexts such as Sub-Saharan Africa, lack of confidentiality was related to the practical restrictions of the service [30], however in the majority of cases it was driven by stigma from healthcare workers who disclosed TMSW health information to friends and co-workers [31, 51].
Sexual Health Literacy
Many authors also identified that the level of knowledge possessed by some TMSW with regards to sexual health and STI transmission affected their risk perception and subsequent intention to access sexual healthcare services [32, 50, 51, 53, 59, 61, 63,64,65]. Some MSW in Vietnam perceived that they could minimise their HIV risk by carefully selecting clients that seem clean and well dressed and were unaware that infections could be contracted from asymptomatic clients [62]. Underhill et al. [53] also found some MSW participants believed they did not need HIV testing because their partner had recently tested negative.
A range of broader structural factors also contributed to the variable levels of knowledge with regards to sexual healthcare. The effects of criminalisation were observed more acutely in regions such as Kenya and Malaysia where sexual intercourse between men is illegal, hampering attempts to provide HIV targeted education [33, 61]. Levels of sexual health knowledge were also mediated by professional isolation. Networks of sex workers in Germany were able to support and mentor younger workers, whereas isolated newcomers were less aware of their level of sexual health risk [64]. Findings from a study with Lebanese MSW suggested, however, that the influence of peers could also sometimes inhibit access to services [32], due to group perceptions such as HIV testing being unimportant.
Fatalism
Participants reported fatalistic attitudes towards their sexual health in five studies, including contexts with highly resourced health systems [30, 32, 53, 62, 63]. Fatalism is a belief in one’s own lack of agency, and has been associated with environments in which social alienation and fragmentation inhibits long-term, goal directed behaviour [69]. Some participants claimed they did not seek out sexual healthcare due to a lack of concern over their HIV status or other potential conditions. In two studies from the US, participants explained this perspective by arguing that contracting HIV was inevitable, or that HIV is a terminal disease with a poor prognosis, and so formal diagnosis would not change their behaviour or cause them to seek treatment [53, 63]. Other participants in Lebanon and Vietnam also expressed that the inevitability of HIV/STI infection made testing irrelevant [32, 62]. Transgender participants in India reported fatalism with regards to accessing HIV treatment, even after a positive diagnosis [30]. They explained this perspective with reference to their belief that they could never have a family, leading them to expect a low quality of life, and so accept a shorter life expectancy due to HIV.
Structural Barriers
Structural barriers to access were most prevalent in studies conducted in Sub-Saharan Africa. Participants were sometimes unable to travel to the service, either because transport was unavailable or because the required time would significantly disrupt their workday [51]. The quality and organisation of the service was also an obstacle. These included issues such as long waiting times, lack of coordination, and inability to ensure privacy and confidentiality [31, 50, 51]. Studies in multiple regions found the cost of services was also an obstacle [31, 51, 55]. Two studies in South America reported that participants’ preferred private clinics to the public system, due to there being less discrimination and more discretion, but often were unable to afford these services [55, 65]. Researchers from Germany [64] and Lebanon [32] also noted that the migrant status of some TMSW in some cases made them ineligible for health insurance, further reducing their ability to pay for healthcare.
Discussion
TMSW are considered a priority population within the international HIV response, due to higher prevalence of HIV/STIs [6], and the presence of unique impediments to accessing healthcare. The purpose of this review was to appraise and summarise the qualitative literature regarding these barriers. The findings demonstrate the diversity and complexity of the challenges faced by TMSW in different regions and contexts, underlined by the near universality of stigma and marginalisation.
This review clearly highlights stigma as the primary barrier to accessing sexual healthcare for TMSW. The significance of stigma has been reflected in other research with sex workers [20, 70]. A recent systematic review of healthcare accessibility for TMSW and FSW also found stigma to be the most significant barrier [70]. Lazarus et al. [20] surveyed 252 FSW and also found occupational stigma experienced in healthcare settings to be the primary access barrier even after controlling for individual demographics, and social and work environments. The relationship between stigma and health outcomes has also been established for the general population of MSM [14, 71] and transgender people [15].
Stigma is described by Goffman [72] as a product of society’s attitudes towards attributes considered ‘significantly discrediting.’ In the context of TMSW, the enactment of stigma produces and reinforces economic, cultural, and social inequalities relating to these stigmatised attributes, such as gender, sexuality, and occupation [73]. This process can be clearly observed within this sample. In terms of the TMSW in these studies, multiple stigmatised social categories, such as MSM, sex worker, or being transgender, are concentrated in a single population with higher HIV/STI prevalence and restricted access to healthcare services. This symbiotic relationship between biological pathology and social conditions has been understood in terms of syndemic theory [74, 75]. Syndemics refers to how biomedical and social processes can combine to cause the progressive reproduction of marginal health and living conditions, particularly for transgender women [76]. Rather than a linear accumulation of stigmatised identities, these social categorisations are interactive and mutually reinforcing. Diverse gender or sexual identities, for example, can sometimes contribute to social marginalisation which can promote participation in unsafe forms of sex work, thereby increasing the individual’s risk for HIV or other sexual health conditions. This dynamic and synergistic process of disadvantage can become a major access barrier for TMSW, by exacerbating fatalism, inhibiting sexual health literacy, and limiting individual’s resources with which to manage their health [75].
Goffman’s [72] formulation of stigma also included a separation between those who are discredited, and those who are only potentially ‘discreditable,’ in the eyes of society. The findings summarised in this review highlighted a similar dichotomy in the experience of stigma for MSM compared to people who are transgender. Many MSM participants had the option of concealing their sexual behaviour from friends, family, and other intimate partners [32, 54, 62]. Sex work could therefore be a sustainable way to achieve financial independence for them and their family, whilst minimising the associated stigma, and allowing them to also engage in other forms of work. Transgender individuals, however, often reported stigma in all spheres of life, as their gender identity could be a more visible social marker [34, 73]. Some transgender women in South Africa reported maintaining a masculine appearance in order to reduce the possibility of discrimination or violence [31]. Stigma could also be experienced by MSM who were more overt in the expression of their sexual identity [55]. This difference between public versus private identities could influence what kind of services people access. Boyce et al. [55] found that heterosexual-identifying MSM preferred clinics that would not identify them as members of this group, whereas transgender participants preferred a sense of belonging and community related to sexual health services.
Finally, the other barriers to healthcare access identified in this review that were not explicitly produced by stigma were still informed by it. The widespread concerns regarding confidentiality were often related to anticipated stigma from healthcare workers. Service providers broke confidentiality out of an apparent lack of respect for their patient’s identity or privacy [31, 55]. Stigma also limited sexual health literacy for TMSW. In contexts where same-sex relationships or transgender identities were not recognised, the social exclusion of these populations made education more difficult and exacerbated this barrier [33, 61]. There is also a close relationship between fatalism and internalised stigma. Participant’s expressions of fatalism were often driven by misperceptions of HIV risk or treatment, or by their expectations of life in an environment where options such as marriage, family, and social acceptance were unavailable [30, 62]. These common and consistent experiences of stigma can translate into an internalisation of deviance narratives and perceptions of natural or even deserved isolation, exclusion, and pathological abnormality among sexual minorities and gender diverse individuals [34]. The impact of this on the mental and physical health and social functioning of a group such as TMSW is wide ranging and complex, sometimes manifesting as the fatalism expressed by some participants in these studies. Feelings of shame and guilt for perceived transgressions combined with an apparently irremediably low social status may contribute to this harmful passivity towards sexual health, as well as exacerbating associated issues such as mental health concerns and harmful substance use. Therefore, both enacted and perceived stigma fostered these fatalistic attitudes towards sexual health, discouraged service access, impaired health literacy, and made many services an unsafe place to disclose personal information. Goffman’s [72] original formulation of stigma is clearly expressed by this syndemic of social exclusion and poor sexual health. For participants in these studies, therefore, stigma was the most significant factor in producing and reinforcing barriers to accessing sexual healthcare.
Recommendations
Participants across multiple papers recommended two ways in which barriers to sexual healthcare for TMSW could be addressed. First was the need for multi-dimensional services that integrated sexual health, mental health, and alcohol and other drug services [60, 63]. This would enable the service to reflect in its structure the prevalence and intersection of these factors experienced by TMSW. The second recommendation was that multi-disciplinary services be provided by staff trained in managing issues specific to this population [31, 35, 50, 51, 56, 58]. There have been examples of sensitivity training in Sub-Saharan African countries improving health professional’s knowledge of health issues affecting MSM and reducing homophobia [77, 78]. Clinics have also been developed that specialise in holistic transgender health and have observed significant improvements in access and health outcomes [79]. The development of national policies to support clinics that are sensitive to the needs of TMSW is the foremost recommendation made by the WHO [80]. Tools and best-practise standards do exist, therefore, to enable healthcare services to transition to the kind of model recommended almost unanimously by these studies’ participants.
Limitations
Limitations of this review include the translation services employed by multiple studies when coding transcripts, which may have obscured some nuances of participant responses. All of the studies were also addressing sensitive and personal issues, and it is difficult to evaluate the degree to which recall bias or social desirability bias [81, 82] may have influenced responses. Several studies also accessed their participants via community support or advocacy organisations, therefore their available sample may have been more engaged with healthcare services than the general population of TMSW.
Previous researchers have also expressed concerns that the conflation of cisgender male and transgender sex workers in health research implies a homogeneity between these groups that is not reflected in the experiences of TMSW [83]. Limiting the review to peer-reviewed publications may also have exposed the sampling process to publication bias. Three studies explicitly aimed to explore experiences of stigma [31, 34, 54], which may have inflated the significance of this factor in relation to the other barriers that were identified.
Further research in this area should include a systematic meta-analysis of the quantitative literature regarding TMSW healthcare access. Papers were excluded from this review that addressed additional factors known to affect individual’s capacity to access healthcare, but which were not identified as such by authors or participants. These include structural and interpersonal factors such as criminalisation [2, 20] social capital [75], and violence [84], each of which can be viewed as structural manifestations of stigma, whilst also acting to produce and reinforce marginalisation. The relationship between criminalisation and HIV prevalence has been recently reaffirmed by Shannon et al. [85], and a decriminalisation process grounded in human rights has been promoted as a key component of public health efforts aimed at reducing HIV/STIs among sex workers [1, 2]. Future qualitative reviews should incorporate these broader factors that contribute to the syndemic of health disparities experienced by TMSW.
Conclusions
The research papers summarised in this review describe TMSW’s experience of a complex syndemic, dominated by the experience of stigma and marginalisation and resulting in an increased prevalence of HIV/STIs in many contexts. The evaluation of these articles in the context of best practise sex worker research indicates that there is still progress to be made regarding the implementation of action-oriented research that empowers sex workers throughout the research process. However, the qualitative evidence reported in these studies provides essential context for the epidemiology of HIV/STI within this population worldwide. Emphasis in the wider literature on prevalence of HIV/STI and risk behaviours among TMSW should be tempered by the detailed descriptions in this sample of the wider context of inequity and disadvantage in which this population is so often situated. Finally, this review highlights the consistent request from TMSW across multiple settings for integrated sexual healthcare services, with appropriately trained staff, that respect the dignity of all clients.
References
Kerrigan D, Kennedy CE, Morgan-Thomas R, Reza-Paul S, Mwangi P, Win KT, et al. A community empowerment approach to the HIV response among sex workers: effectiveness, challenges, and considerations for implementation and scale-up. Lancet. 2015;385(9963):172–85.
Decker MR, Crago A, Chu SKH, Sherman SG, Seshu MS, Buthelezi K, et al. Human rights violations against sex workers: burden and effect on HIV. Lancet. 2015;385(9963):186–99.
Clements-Nolle K, Marx R, Guzman R, Katz M. HIV prevalence, risk behaviours, healthcare use, and mental health status of transgender persons: implications for public health intervention. Am J Public Health. 2001;91:915–21.
Operario D, Soma T, Underhill K. Sex work and HIV status among transgender women: systematic review and meta-analysis. J Acquir Immune Defic Syndr. 2008;48(1):97–103.
Tang W, Mahapatra T, Liu F, Fu G, Yang B, Tucker JD, et al. Burden of HIV and syphilis: a comparative evaluation between male sex workers and non-sex-worker men who have sex with men in urban China. PLoS ONE. 2015;10(5):e0126604.
UNAIDS. Global report 2012: UNAIDS report of the global AIDS epidemic. Joint United Nations Programme on HIV/AIDS. UNAIDS; 2012.
Poteat T, Wirtz AL, Radix A, Borquez A, Silva-Santisteban A, Deutsch MB, et al. HIV risk and preventive interventions in transgender women sex workers. Lancet. 2015;385(9964):274–86.
Myers T, Allman D, Xu K, Remis RS, Aguinaldo J, Burchell A, et al. The prevalence and correlates of hepatitis C virus (HCV) infection and HCV-HIV co-infection in a community sample of gay and bisexual men. Int J Infect Dis. 2009;13(6):730–9.
Nguyen TA, Nguyen HT, Le GT, Detels R. Prevalence and risk factors associated with HIV infection among men having sex with men in Ho Chi Minh City, Vietnam. AIDS Behav. 2008;12(3):476–82.
Oldenburg CE, Perez-Brumer AG, Reisner SL, Mimiaga MJ. Transactional sex and the HIV epidemic among men who have sex with men (MSM): results from a systematic review and meta-analysis. AIDS Behav. 2015;19(12):2177–83.
Baral SD, Friedman MR, Geibel S, Rebe K, Bozhinov B, Diouf D, et al. Male sex workers: practices, contexts, and vulnerabilities for HIV acquisition and transmission. Lancet (Lond Engl). 2015;385(9964):260–73.
Sperber J, Landers S, Lawrence S. Access to health care for transgendered persons: results of a needs assessment in Boston. Int J Transgend. 2005;8(2–3):75–91.
Singh GK, Azuine RE, Siahpush M. Widening socioeconomic, racial, and geographic disparities in HIV/AIDS mortality in the United States, 1987–2011. Adv Prev Med. 2013;2013:657961.
Newman PA, Philbin MM, Hirsch JS, Wilson PA, Ly AT, Giang LM, et al. Structural barriers to HIV prevention among men who have sex with men (MSM) in Vietnam: diversity, stigma, and healthcare access. PLoS ONE. 2018. https://doi.org/10.1371/journal.pone.0195000.
White Hughto JM, Reisner SL, Pachankis JE. Transgender stigma and health: a critical review of stigma determinants, mechanisms, and interventions. Soc Sci Med. 2015;147:222–31.
Beattie TSH, Bhattacharjee P, Suresh M, Isac S, Ramesh BM, Moses S. Personal, interpersonal and structural challenges to accessing HIV testing, treatment and care services among female sex workers, men who have sex with men and transgenders in Karnataka State, South India. J Epidemiol Community Health. 2012;66(Suppl 2):42–8.
Chakrapani V, Newman PA, Shunmugam M, McLuckie A, Melwin F. Structural violence against Kothi-identified men who have sex with men in Chennai, India: a qualitative investigation. AIDS Educ Prev. 2007;19(4):346–64.
Earnshaw VA, Bogart LM, Dovidio JF, Williams DR. Stigma and racial/ethnic HIV disparities: moving toward resilience. Am Psychol. 2013;68(4):225–36.
Arnold EA, Rebchook GM, Kegeles SM. ‘Triply cursed’: racism, homophobia and HIV-related stigma are barriers to regular HIV testing, treatment adherence and disclosure among young Black gay men. Cult Health Sex. 2014;16(6):710–22.
Lazarus L, Deering KN, Nabess R, Gibson K, Tyndall MW, Shannon K. Occupational stigma as a primary barrier to health care for street-based sex workers in Canada. Cult Health Sex. 2012;14(2):139–50.
Logie CH, James L, Tharao W, Loutfy MR. HIV, gender, race, sexual orientation, and sex work: a qualitative study of intersectional stigma experienced by HIV-positive women in Ontario, Canada. PLoS Med. 2011;8(11):e1001124.
Ngo AD, Ratliff EA, McCurdy SA, Ross MW, Markham C, Pham HT. Health-seeking behaviour for sexually transmitted infections and HIV testing among female sex workers in Vietnam. AIDS Care. 2007;19(7):878–87.
Levesque J, Harris MF, Russell G. Patient-centred access to health care: conceptualising access at the interface of health systems and populations. Int J Equity Health. 2013;12(18):18.
Harcourt C, Donovan B. The many faces of sex work. Sex Transm Infect. 2005;81(3):201–6.
Jobson GA, Theron LB, Kaggwa JK, Kim HJ. Transgender in Africa: invisible, inaccessible, or ignored? SAHARA-J J Soc Asp HIV/AIDS. 2012;9(3):160–3.
Bungay V, Oliffe J, Atchison C. Addressing underrepresentation in sex work research: reflections on designing a purposeful sampling strategy. Qual Health Res. 2016;26(7):966–78.
Bonevski B, Randell M, Paul C, Chapman K, Twyman L, Bryant J, et al. Reaching the hard-to-reach: a systematic review of strategies for improving health and medical research with socially disadvantaged groups. BMC Med Res Methodol. 2014;14(1):42.
Dudwick N, Kuehnast K, Jones VN, Woolcock M. Analyzing social capital in context: a guide to using qualitative methods and data. Washington, DC: World Bank Institute; 2006.
Choy LT. The strengths and weaknesses of research methodology: comparison and complimentary between qualitative and quantitative approaches. IOSR J Humanit Soc Sci. 2014;19(4):99–104.
Chakrapani V, Newman PA, Shunmugam M, Dubrow R. Barriers to free antiretroviral treatment access among Kothi-identified men who have sex with men and Aravanis (transgender women) in Chennai, India. AIDS Care. 2011;23(12):1687–94.
Samudzi Z, Mannell J. Cisgender male and transgender female sex workers in South Africa: gender variant identities and narratives of exclusion. Cult Health Sex. 2016;18(1):1–14.
Aunon FM, Wagner GJ, Maher R, Khouri D, Kaplan RL, Mokhbat J. An exploratory study of HIV risk behaviors and testing among male sex workers in Beirut, Lebanon. Soc Work Public Health. 2015;30(4):373–84.
Barmania S, Aljunid SM. Navigating HIV prevention policy and Islam in Malaysia: contention, compatibility or reconciliation? Findings from in-depth interviews among key stakeholders. BMC Public Health. 2016;16:524.
Ganju D, Saggurti N. Stigma, violence and HIV vulnerability among transgender persons in sex work in Maharashtra, India. Cult Health Sex. 2017;19(8):903–17.
Sevelius JM, Keatley J, Calma N, Arnold E. ‘I am not a man’: trans-specific barriers and facilitators to PrEP acceptability among transgender women. Glob Public Health. 2016;11(7–8):1060–75.
Shaver FM. Sex work research: methodological and ethical challenges. J Interpers Violence. 2005;20(3):296–319.
Beyrer C, Crago A, Bekker L, Butler J, Shannon K, Kerrigan D, et al. An action agenda for HIV and sex workers. Lancet. 2015;385(9964):287–301.
Abel G, Fitzgerald L, Brunton C. Christchurch School of Medicine study: methodology and methods. In: Abel G, Fitzgerald L, Healy C, Taylor A, editors. Taking the crime out of sex work: New Zealand sex workers’ fight for decriminalisation. Bristol: The Policy Press; 2010. p. 159–62.
Graça M, Gonçalves M, Martins A. Participatory action research with sex workers and an outreach team: a co-authored case study. Action Res. 2017. https://doi.org/10.13140/RG.2.1.3688.4080..
Singh AA, Richmond K, Burnes TR. Feminist participatory action research with transgender communities: fostering the practice of ethical and empowering research designs. Int J Transgend. 2013;14(3):93–104.
Jeffreys E. Sex worker-driven research: best practice ethics. Dialogue e-J. 2010;8.
Baum F, MacDougall C, Smith D. Participatory action research. J Epidemiol Community Health. 2006;60(10):854–7.
van der Meulen E. Action research with sex workers: dismantling barriers and building bridges. Action Res. 2011;9(4):370–84.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7).
National Institute for Health and Care Excellence. Methods for the development of NICE public health guidance. London: National Institute for Health and Clinical Excellence; 2012.
Noyes J, Hannes K, Booth A, Harris J, Harden A, Popay J, et al. Qualitative research and Cochrane review. 2008. In: Cochrane handbook for systematic review of interventions (Internet). Cochrane Qualitative and Implementation Methods Group; p. 571.
Lui CW, Dean J, Mutch A, Mao L, Debattista J, Lemoire J, et al. HIV testing in men who have sex with men: a follow-up review of the qualitative literature since 2010. AIDS Behav. 2017. https://doi.org/10.1007/s10461-017-1752-3.
Lorenc T, Marrero-Guillamon I, Llewellyn A, Aggleton P, Cooper C, Lehmann A, et al. HIV testing among men who have sex with men (MSM): systematic review of qualitative evidence. Health Educ Res. 2011;26(5):834–46.
Toye F, Seers K, Allcock N, Briggs M, Carr E, Barker K. Meta-ethnography 25 years on: challenges and insights for synthesising a large number of qualitative studies. BMC Med Res Methodol. 2014;14:80.
Restar AJ, Tocco JU, Mantell JE, Lafort Y, Gichangi P, Masvawure TB, et al. Perspectives on HIV pre- and post-exposure prophylaxes (PrEP and PEP) among female and male sex workers in Mombasa, Kenya: implications for integrating biomedical prevention into sexual health services. AIDS Educ Prev. 2017;29(2):141–53.
Scorgie F, Nakato D, Harper E, Richter M, Maseko S, Nare P, et al. ‘We are despised in the hospitals’: sex workers’ experiences of accessing health care in four African countries. Cult Health Sex. 2013;15(4):450–65.
Sandelowski M, Barroso J, Voils CI. Using qualitative metasummary to synthesize qualitative and quantitative descriptive findings. Res Nurs Health. 2007;30(1):99–111.
Underhill K, Morrow KM, Colleran CM, Holcomb R, Operario D, Calabrese SK, et al. Access to healthcare, HIV/STI testing, and preferred pre-exposure prophylaxis providers among men who have sex with men and men who engage in street-based sex work in the US. PLoS ONE. 2014;9(11):e112425.
Underhill K, Morrow KM, Colleran C, Holcomb R, Calabrese SK, Operario D, et al. A qualitative study of medical mistrust, perceived discrimination, and risk behavior disclosure to clinicians by U.S. male sex workers and other men who have sex with men: implications for biomedical HIV prevention. J Urban Health. 2015;92(4):667–86.
Boyce S, Barrington C, Bolanos H, Arandi CG, Paz-Bailey G. Facilitating access to sexual health services for men who have sex with men and male-to-female transgender persons in Guatemala City. Cult Health Sex. 2012;14(3):313–27.
Okanlawon K, Adebowale AS, Titilayo A. Sexual hazards, life experiences and social circumstances among male sex workers in Nigeria. Cult Health Sex. 2013;15(Suppl 1):S22–33.
Reza-Paul S, Lorway R, O’Brien N, Lazarus L, Jain J, Bhagya M, et al. Sex worker-led structural interventions in India: a case study on addressing violence in HIV prevention through the Ashodaya Samithi Collective in Mysore. Indian J Med Res. 2012;135(1):98–106.
Xavier J, Bradford J, Hendricks M, Safford L, McKee R, Martin E, et al. Transgender health care access in Virginia: a qualitative study. Int J Transgend. 2013;14(1):3–17.
Giguere R, Frasca T, Dolezal C, Febo I, Cranston RD, Mayer K, et al. Acceptability of three novel HIV prevention methods among young male and transgender female sex workers in Puerto Rico. AIDS Behav. 2016;20(10):2192–202.
Jones JL, Rasch RFR, MacMaster S, Adams SM, Cooper RL. The experiences of African American male commercial sex workers at-risk for HIV: accessing outreach services. J Gay Lesbian Soc Serv. 2009;21(2–3):282–93.
Okal J, Luchters S, Geibel S, Chersich MF, Lango D, Temmerman M. Social context, sexual risk perceptions and stigma: HIV vulnerability among male sex workers in Mombasa, Kenya. Cult Health Sex. 2009;11(8):811–26.
Mimiaga MJ, Reisner SL, Closson EF, Perry N, Perkovich B, Nguyen T, et al. Self-perceived HIV risk and the use of risk reduction strategies among men who engage in transactional sex with other men in Ho Chi Minh City, Vietnam. AIDS Care. 2013;25(8):1039–44.
Reisner SL, Mimiaga MJ, Mayer KH, Tinsley JP, Safren SA. Tricks of the trade: sexual health behaviors, the context of HIV risk, and potential prevention intervention strategies for male sex workers. J LGBT Health Res. 2008;4(4):195–209.
Castaneda H. Structural vulnerability and access to medical care among migrant street-based male sex workers in Germany. Soc Sci Med. 2013;84:94–101.
Infante C, Sosa-Rubi SG, Cuadra SM. Sex work in Mexico: vulnerability of male, travesti, transgender and transsexual sex workers. Cult Health Sex. 2009;11(2):125–37.
Collumbien M, Qureshi AA, Mayhew SH, Rizvi N, Rabbani A, Rolfe B, et al. Understanding the context of male and transgender sex work using peer ethnography. Sex Transm Infect. 2009;85(Suppl 2):ii3–7.
Morrell R, Jewkes R, Lindegger G. Hegemonic masculinity/masculinities in South Africa. Men Masc. 2012;15(1):11–30.
Livingston JD, Boyd JE. Correlates and consequences of internalized stigma for people living with mental illness: a systematic review and meta-analysis. Soc Sci Med. 2010;71(12):2150–61.
Meyer-Weitz A. Understanding fatalism in HIV/AIDS protection: the individual in dialogue with contextual factors. Afr J AIDS Res. 2005;4(2):75–82.
Ma PHX, Chan ZCY, Loke AY. The socio-ecological model approach to understanding barriers and facilitators to the accessing of health services by sex workers: a systematic review. AIDS Behav. 2017;21(8):2412–38.
Stahlman S, Grosso A, Ketende S, Sweitzer S, Mothopeng T, Taruberekera N, et al. Depression and social stigma among MSM in Lesotho: implications for HIV and sexually transmitted infection prevention. AIDS Behav. 2015;19(8):1460–9.
Goffman E. Stigma: notes on the management of a spoiled identity. New York: Simon and Schuster; 1963.
Lacombe-Duncan A. An intersectional perspective on access to HIV-related healthcare for transgender women. Transgend Health. 2016;1(1):137–41.
Singer M, Bulled N, Ostrach B, Mendenhall E. Syndemics and the biosocial conception of health. Lancet. 2017;389(10072):941–50.
Biello KB, Colby D, Closson E, Mimiaga MJ. The syndemic condition of psychosocial problems and HIV risk among male sex workers in Ho Chi Minh City, Vietnam. AIDS Behav. 2014;18(7):1264–71.
Brennan J, Kuhns LM, Johnson AK, Belzer M, Wilson EC, Garofalo R. Syndemic theory and HIV-related risk among young transgender women: the role of multiple, co-occurring health problems and social marginalization. Am J Public Health. 2012;102(9):1751–7.
Dijkstra M, van der Elst EM, Micheni M, Gichuru E, Musyoki H, Duby Z, et al. Emerging themes for sensitivity training modules of African healthcare workers attending to men who have sex with men: a systematic review. Int Health. 2015;7(3):151–62.
van der Elst EM, Smith AD, Gichuru E, Wahome E, Musyoki H, Muraguri N, et al. Men who have sex with men sensitivity training reduces homoprejudice and increases knowledge among Kenyan healthcare providers in coastal Kenya. J Int AIDS Soc. 2013;16(Suppl 3):18748.
Reisner SL, Bradford J, Hopwood R, Gonzalez A, Makadon H, Todisco D, et al. Comprehensive transgender healthcare: the gender affirming clinical and public health model of Fenway Health. J Urban Health. 2015;92(3):584–92.
WHO. Guidelines: prevention and treatment of HIV and other sexually transmitted infections among men who have sex with men and transgender people: recommendations for a public health approach. Geneva: World Health Organisation; 2011.
Chillag K, Guest G, Bunce A, Johnson L, Kilmarx PH, Smith DK. Talking about sex in Botswana: social desirability bias and possible implications for HIV-prevention research. Afr J AIDS Res. 2006;5(2):123–31.
Kelly CA, Soler-Hampejsek E, Mensch BS, Hewett PC. Social desirability bias in sexual behavior reporting: evidence from an interview mode experiment in rural Malawi. Int Perspect Sex Reprod Health. 2013;39(1):14–21.
Perez-Brumer AG, Oldenburg CE, Reisner SL, Clark JL, Parker RG. Towards ‘reflexive epidemiology’: conflation of cisgender male and transgender women sex workers and implications for global understandings of HIV prevalence. Glob Public Health. 2016;11(7–8):849–65.
Dunkle KL, Wong FY, Nehl EJ, Lin L, He N, Huang J, et al. Male-on-male intimate partner violence and sexual risk behaviors among money boys and other men who have sex with men in Shanghai, China. Sex Transm Dis. 2013;40(5):362–5.
Shannon K, Crago A-L, Baral SD, Bekker L-G, Kerrigan D, Decker MR, et al. The global response and unmet actions for HIV and sex workers. Lancet. 2018;392(10148):698–710.
Funding
All funding for this review was provided by the HIV Foundation, Queensland.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
This research received ethical approval under the University of Queensland Human Research Ethics Committee (Approval Number #2016001287).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Brookfield, S., Dean, J., Forrest, C. et al. Barriers to Accessing Sexual Health Services for Transgender and Male Sex Workers: A Systematic Qualitative Meta-summary. AIDS Behav 24, 682–696 (2020). https://doi.org/10.1007/s10461-019-02453-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-019-02453-4