
Abstract
Currently, the Centers for Disease Control and Prevention recommends that persons between 15 and 64 years get tested for human immunodeficiency virus (HIV) at least once in their lifetime and persons with HIV risk factors get tested more frequently. There is limited research examining factors associated with never testing for HIV among non-Hispanic Black men in the United States. The purpose of this study was to examine the prevalence of never testing for HIV, reasons for never testing for HIV, and correlates of never testing for HIV. We analyzed 2011–2013 National Survey of Family Growth data and restricted analyses to male respondents aged 15–44 years who self-identified as being non-Hispanic Black. Logistic regression models estimated adjusted prevalence ratios (APR) assessing the association between socio-demographic and behavioral factors and never testing for HIV. An estimated 31.2 % of non-Hispanic Black males aged 15–44 years have never been tested for HIV. Non-Hispanic Black men aged 15–17 years (APR 4.45; 95 % CI 2.88–6.87) or 18–24 years (APR 1.94; 95 % CI 1.21–3.13), who did not visit a doctor or healthcare provider (APR 1.43; 95 % CI 1.10–1.86), or did not report any sexual risk behaviors in the past 12 months (APR 1.83; 95 % CI 1.34–2.51) were more likely to never test for HIV compared to their respective counterparts. Continued expansion of HIV testing initiatives and prevention programs that focus on non-Hispanic Black men is critical to addressing HIV-related health disparities and the public health burden of HIV in this population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Non-Hispanic Blacks in the United States (US) are most affected by the human immunodeficiency virus (HIV) [1]. While they make up approximately 13 % of the US population, they accounted for an estimated 44 % of all new HIV infections among adults and adolescents in 2014 [1]. Among all non-Hispanic Blacks, approximately 74 % of all infections in 2014 occurred in men [1]. The rate of HIV diagnoses among non-Hispanic Black men was more than seven and two times the rates of HIV diagnoses among White and Hispanic men in 2014, respectively [1]. Non-Hispanic Black men are also more likely to die from HIV than men of any other race [2]. Since 2004, HIV has consistently ranked among the top ten leading causes of death among this population [2]. Given these figures, existing literature has focused on identifying factors that contribute to the disproportionate impact of HIV on non-Hispanic Black men. Structural, social, and sexual network factors have been implicated as significant contributors to these disparities [3–6]. Lack of HIV testing has also been associated with the high rates of HIV infection among this population [7].
HIV testing is the cornerstone of HIV prevention and care and is essential to achieving the objectives of the National HIV/AIDS strategy of reducing new HIV infections, optimizing health outcomes among people living with HIV and reducing HIV-related health disparities [8]. Currently, the Centers for Disease Control and Prevention (CDC) recommends that persons between 15 and 64 years get tested for HIV at least once in their lifetime and persons with HIV risk factors get tested more frequently [9]. HIV testing rates are higher for non-Hispanic Blacks than other racial/ethnic groups [10, 11]. However, despite public health efforts to expand opportunities for HIV testing among this population, they are more likely to get tested and diagnosed with HIV late in the course of their infection [1]. Among men in particular, the rate of late HIV diagnosis is significantly higher for non-Hispanic Blacks than the rates among White and Hispanic men [1].
Given that there is still no cure for HIV, prevention continues to be a main component of HIV control efforts, and testing is central to these efforts [12, 13]. HIV testing presents valuable opportunities to identify new infections, increase awareness of HIV status, and address the HIV-related health disparities borne by non-Hispanic Black men. While previous studies have examined the prevalence of and factors associated with recent HIV testing among non-Hispanic Black men [14–16], few studies have examined the correlates of never testing for HIV among this group. To inform targeted programs and policies, it is critical to understand the correlates of never testing for HIV among this population. Using a nationally representative sample of non-Hispanic Black men in the US, we examined (1) the prevalence of never testing for HIV, (2) specific reasons offered by respondents for never testing for HIV, and (3) the socio-demographic and behavioral correlates of never testing for HIV.
Methods
Data Source and Sample
The National Survey for Family Growth (NSFG) is an in-person cross-sectional health survey conducted by the CDC that is representative of the civilian, non-institutionalized population of the US aged 15–44 years [17, 18]. Respondents of Hispanic/Latino and Black race/ethnicity and adolescents were oversampled to produce reliable estimates for these groups. One randomly-selected resident from each household was interviewed. Information on sensitive issues, including sexual identity and behavior with the same and opposite sex were collected using Audio Computer-Assisted Self-Interviewing. Minors were required to have consent from a parent or guardian and provide their own assent [17, 18]. The study sample was weighted to produce national US estimates using methods and procedures proposed by the National Center for Health Statistics to account for weighting based on selection probability, nonresponse and sampling differences between regions. The procedures of the NSFG recruitment protocol were reviewed and approved by Institutional Review Board of the National Center for Health Statistics [19]. Additional details regarding the NSFG sample design, weighting methodology, and variance estimation are described elsewhere [19]. A total of 4815 men completed the interview in the 2011–2013 NSFG continuous cycle with a response rate of 72.1 %. We restricted the analyses to non-Hispanic Black men aged 15–44 years for a final analytical sample of 933, representing a weighted national estimate of 7,787,657.
Outcome Variables
The outcome for this analysis was never tested for HIV and was measured by the question, “Excluding blood donations, have you ever been tested for HIV? (yes/no).” Respondents who answered “no” were classified as having never tested for HIV. Those who answered “no” were then asked “Which one of these would you say is the MAIN reason why you have not been tested for HIV?” We classified these reasons into three categories: unlikely exposed, fear or HIV-related stigma, and access-related or other reasons. Respondents categorized as mainly never testing because “they were unlikely exposed” responded that they were: 1) unlikely exposed to HIV; 2) reported spouse or partner tested negative; or 3) never had sexual intercourse. Respondents categorized as mainly never testing due to “fear or HIV-related stigma” responded that they were: 1) worried about what other people would think if they got tested for HIV; 2) afraid to find out if they were HIV positive; 3) or did not like needles. Respondents categorized as mainly never testing for “access-related or other reasons” stated they were: 1) never offered an HIV test; 2) did not have health insurance and could not afford an HIV test; or 3) some other reason.
Independent variables
Additional socio-demographic, healthcare access-related, and behavioral variables (correlates) were included in the analysis based upon availability in the NSFG and association with HIV testing. Demographic variables included: age in years (15–17, 18–24, 25–34, 35–44); income classified according to the Federal Poverty Guidelines (below poverty level, or above poverty level); and relationship status (married/cohabitating, unmarried/not cohabitating). Healthcare access-related variables included: health insurance coverage in the past 12 months (yes, no); visited the doctor or healthcare provider in past 12 months (yes, no); and usual place of health care (yes, no). Sexual risk behaviors that confer a high risk for HIV infection, indicating the need for annual HIV testing, were selected and included [20]: sexual orientation (heterosexual, homosexual/bisexual); and HIV-related sexual risk behaviors in the past 12 months (i.e. four or more opposite sex partners, sex with an injection drug user, sex with an HIV-positive person, exchanged sex for money or drugs, any anal or oral sex with a male, or sex with a partner who had sex with other partners).
Data Analysis
All analyses were performed on weighted data using SUDAAN version 10.0.1 (Research Triangle Institute), a software package that accounts for the complex sampling design of the NSFG. Chi square statistics were calculated to determine statistically significant differences (p < 0.05) in the distribution of the study variables. Logistic regression analyses were used to calculate prevalence ratios (PRs) and 95 % confidence intervals (95 % CIs) for each independent variable to assess the association with never testing for HIV. Adjusted prevalence ratios (APRs) were calculated by controlling for specific demographic, healthcare access-related, and behavioral covariates significant in the bivariate analyses at p < 0.05.
Results
A sample distribution of study variables is presented in Table 1. Over half (58.5 %) of the sample of non-Hispanic Black men reported being unmarried or not cohabitating. Approximately one-third of the sample reported living below the poverty level (29.4 %), having health insurance coverage in the past 12 months (35.6 %), visited a doctor or healthcare provider in the past 12 months (38.5 %), and did not have a usual place of healthcare (31.3 %). Only 2.8 % reported being either homosexual or bisexual and 23.6 % reported any sexual risk behaviors in the past 12 months. Nearly a third (31.2 %) of non-Hispanic Black men aged 15–44 years have never tested for HIV.
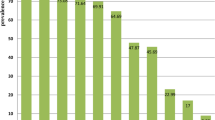
Testing history varied significantly (p < 0.05) by age, income, relationship status, health insurance coverage in the past 12 months, doctor or healthcare provider visit in the past 12 months, and HIV-related sexual risk behaviors (Table 2). The proportion of never testing was highest among non-Hispanic Black men who were 15–24 years of age (66.3 %), living above the poverty level (63.7 %), unmarried/not cohabitating (76 %), did not have health insurance coverage or visit a doctor or healthcare provider in past 12 months (71.1 and 73.8 %, respectively), and did not report any HIV-related risk behaviors (85.1 %). Table 3 presents weighted estimates of specific reasons for never testing for HIV. Among non-Hispanic Black men who reported never testing for HIV, the most common reason for never testing was unlikely exposure (63.4 %) followed by healthcare access-related or other reasons (31.7 %) and fear or HIV-related stigma (4.9 %).
Table 4 shows unadjusted and adjusted prevalence ratios for never testing for HIV among non-Hispanic Black men. In the unadjusted model, non-Hispanic Black men aged 15–17 years and 18–24 years were 5.88 (95 % CI 3.61–9.58) and 2.53 (95 % CI 1.45–4.40) times more likely to never test for HIV as compared to those aged 35–44 years (Table 4). Likewise, non-Hispanic Black men who were below the poverty level (1.37; 95 % CI 1.08–1.74), were not married or cohabitating (2.26; 95 % CI 1.43–3.55), did not visit a doctor or healthcare provider (1.77; 95 % CI 1.26–2.48), did not report any HIV-related risk behaviors (1.74; 95 % CI 1.12–2.70) were more likely to never test for HIV compared to non-Hispanic Black men living above the poverty level, married/cohabitating, visited a doctor or healthcare provider, or reported at least one HIV-related risk behavior respectively.
In the adjusted model, after controlling for all study variables, non-Hispanic Black men aged 15–17 years (4.45; 95 % CI 2.88–6.87) or 18–24 years (1.94; 95 % CI 1.21–3.13), who did not visit a doctor or healthcare provider in the past 12 months (1.43; 95 % CI 1.10–1.86), or did not report any HIV-related risk behaviors (1.83; 95 % CI 1.34–2.51) were still more likely to never test for HIV compared to those between 35–44 years, who visited a doctor or healthcare provider in the past 12 months, and who reported any HIV-related risk behaviors in the past 12 months.
Discussion
Although non-Hispanic Blacks are more likely to report a history of HIV testing than other ethnic groups, the findings of this study suggest that a significant proportion of non-Hispanic Black men do not adhere to the CDC recommendation of getting tested for HIV at least once in their lifetime [9]. Of concern, approximately 31.2 % of non-Hispanic Black men between 15 and 44 years in this study have never been tested for HIV despite the fact that non-Hispanic Black men in this age group have higher rates of HIV infection than men of any other race/ethnicity [1]. The prevalence of respondents who have never been tested for HIV has public health implications for the prevention, transmission, and control of HIV among non-Hispanic Black men, especially among younger study respondents as younger persons are more likely to be sexually active than older respondents [10, 11, 13]. About 30 % of new HIV infections can be attributed to persons who do not know that they have HIV [13]. Additionally, people who are not aware of their HIV infection/status are not able to access medications that can delay disease progression and reduce transmission risk [13].
The high prevalence of never testing for HIV among young men in this study could be attributed to a number of factors. Many young men do not seek any form of preventative healthcare [21] except for mandatory college or sports physical examinations. Majority of HIV testing in the US is done in clinical settings, [22, 23] however clinic-based HIV testing presents challenges to younger persons [23]. Young non-Hispanic Black men may not have health care coverage that can cover the costs of obtaining an HIV test. Furthermore, many younger persons may still be covered by their parents’ health insurance coverage and may be less inclined to get tested for HIV out of fear that their parents may become aware of the test itself or the results. Fear and stigma surrounding HIV and HIV testing in healthcare facilities in the non-Hispanic Black community may also preclude young people from getting tested for HIV in these locations [15, 16]. Young non-Hispanic Black men are more influenced by normative attitudes of their peers and are more susceptible to social marginalization than older men [24]. Studies have shown that HIV-related stigma and the fear of social marginalization play a role in the reluctance of young non-Hispanic Black men to get tested at healthcare centers and become aware of their HIV status [24]. Prior research has also shown that complacency and beliefs about HIV and HIV risk can affect HIV testing among young non-Hispanic Black men [25, 26]. Young persons are less likely than older persons to perceive HIV as a severe medical condition and this can affect the healthcare behaviors, such as HIV testing, that they take to prevent and mitigate HIV risk and transmission [25, 26].
HIV testing has also been associated with frequency of clinical encounters [26]. Persons who report routine out-patient visits are more likely to report HIV test than those who do not. Non-Hispanic Blacks, especially young non-Hispanic Blacks are less likely to report routine clinical encounters and outpatient visits than older and White men, [27] and may be more likely to report never testing for HIV. In the multivariable analysis, persons with no sexual risk behaviors were more likely to have never tested for HIV. The lack of testing among persons with no sexual risk behaviors may be due to the fact that HIV prevention programs and interventions primarily target persons with risk factors for HIV which include persons who report risky sexual behavior. Alternatively, persons who report risky sexual behavior may also be more cognizant of their risk of HIV than persons who do not engage in risky sexual behavior, and thus may be more likely to get tested for HIV. However, there are other non-sexual risks factors for HIV acquisition, hence the importance of getting tested for HIV at least once even if a person is not engaging in risky sexual behaviors cannot be overstated.
Married/cohabitating respondents were less likely to have never been tested for HIV than unmarried/not cohabitating respondents. Married/co-habiting relationships are presumably more serious and of a longer duration than other types of relationships and these characteristics may provide greater opportunities for communication and comfort about HIV testing. The greater prevalence of HIV testing among married/co-habiting respondents may also be indicative of their intention to discontinue condom use [28]. However, the finding that unmarried/not co-habiting were more likely to have never tested for HIV is worrisome as these persons are unaware of their HIV status and may be at risk for HIV [29]. The most common reason for never testing for HIV was “unlikely exposure to HIV”. Findings from a recent study showed that many individuals are likely to underestimate their personal risk for HIV acquisition [30]. In this study, two-thirds of newly-diagnosed respondents assessed their HIV risk as low or none [30]. Furthermore, due to the higher prevalence of HIV among non-Hispanic Blacks, the risk of HIV acquisition with each HIV risk behavior is high, hence the need to get tested for HIV. Programs that promote HIV testing among black men must address perception of risk.
HIV testing in this population has significant public health benefits as it facilitates the identification and linkage of HIV infected persons into care which in turn can reduce the risk of HIV transmission among non-Hispanic Blacks. The continued expansion of HIV testing programs and social media campaigns, especially those that target young non-Hispanic Black men, are required. Expanding free HIV testing programs to include non-traditional locations like AIDS-service organizations and pharmacies as well as partnering with community centers and faith-based organizations can be beneficial as it will reach persons that may be missed during regular healthcare visits, facilitate normative HIV testing, and mitigate fear and stigma associated with HIV testing [31, 32]. These programs can also eliminate some of the structural barriers to HIV testing in this population and increase the accessibility and availability of HIV testing services. Providing resources about the availability of home-based testing kits has also shown promise in increasing the frequency of HIV tests and addressing concerns about anonymity, confidentiality, and stigma [33]. HIV testing social media campaigns that target non-Hispanic Black men can also increase awareness about the importance of HIV testing, emphasize the benefits of HIV testing, address HIV testing misconceptions and stigma, provide information on HIV testing locations, and facilitate normative HIV testing in this population. Cultural competence is also important in increasing HIV testing as it can serve to allay the fears of HIV testing stigma among non-Hispanic black men [26].
Healthcare providers, especially those that serve predominantly non-Hispanic Black men, have a role to play in increasing HIV testing in this population as research has shown that people are more likely to get tested for HIV when a healthcare provider recommends it [26]. Current prevention guidelines call for routine HIV testing as part of medical care for all adolescents and adults in the US [34]. The US Preventive Services Task Force also assigned a “grade A” designation for routine HIV testing for all adolescents and adults aged 15–65 years, indicating with a high certainty that the net benefits of HIV testing are substantial [34]. Increased awareness of this recommendation and its acceptance by healthcare providers may increase HIV testing rates among non-Hispanic Black men and aid in the prompt identification of HIV-infected persons.
HIV testing also offers opportunities to provide comprehensive sexual education. Adapting opt-out HIV testing in clinical settings can be particularly beneficial to young persons, whether they are sexually active or not, as it can create an environment that facilitates HIV risk education, disclosure of their risk behaviors, and behavioral risk counseling. Finally, the Affordable Care Act (ACA) is another opportunity to expand HIV testing among non-Hispanic Black men [35]. Under the ACA, HIV testing is considered an essential health benefit, meaning that all persons can obtain an HIV test without cost-sharing, therefore eliminating cost as a limitation to HIV testing [35].
This study is not without limitations. First, the NSFG is not administered to homeless or institutionalized persons, therefore excluding those who are hospitalized and incarcerated. Second, no causal associations can be inferred given the cross-sectional design of the NSFG survey. Third, measures used in the analysis like HIV testing and reasons for HIV testing are self-reported by the participants, and are therefore subject to recall and social desirability bias. Fourth, we did not include any substance use variables. Future research should explore whether cigarette and alcohol use influence HIV testing behaviors among non-Hispanic Black men as previous findings have shown that African American adults who use these two substances are more likely to perceive themselves to be at risk for HIV and test for HIV [36].
Conclusions
To achieve the goals of the National HIV/AIDS strategy, HIV testing must continue to be a core component of HIV prevention and care efforts among non-Hispanic Black men. Continued expansion of HIV testing initiatives and prevention programs that focus on non-Hispanic Black men is critical to addressing health disparities and the public health burden of HIV in this population.
References
Centers for Disease Control and Prevention. Diagnoses of HIV infection in the United States and dependent areas, 2014, vol. 26. Available at http://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-report-us.pdf Accessed 10 Feb 2016.
Centers for Disease Control and Prevention. Leading causes of death in Males, United States Available at http://www.cdc.gov/men/lcod/ Accessed 24 June 2015.
Maulsby C, Millett G, Lindsey K, et al. HIV among black men who have sex with men (MSM) in the United States: a review of the literature. AIDS Behav. 2014;18(1):10–25.
Bowleg L, Raj A. Shared communities, structural contexts, and HIV risk: prioritizing the HIV risk, and prevention needs of Black heterosexual men. Am J Public Health. 2012;102(S2):S173–7.
Bowleg L, Burkholder GJ, Massie JS, et al. Racial discrimination, social support, and sexual HIV risk among Black heterosexual men. AIDS Behav. 2013;17(1):407–18.
Reed E, Santana MC, Bowleg L, et al. Experiences of racial discrimination and relation to sexual risk for HIV among a sample of urban black and African American men. J Urban Health. 2013;90(2):314–22.
Wejnert C, Le B, Rose CE, et al. HIV infection and awareness among men who have sex with men–20 cities, United States, 2008 and 2011. PLoS One. 2013;8(10):e76878.
National HIV/AIDS Strategy. July 2010. Available at https://www.whitehouse.gov/sites/default/files/uploads/NHAS.pdf Accessed 10 May 2015.
Centers for Disease Control and Prevention. HIV testing in clinical settings. Available at http://www.cdc.gov/hiv/testing/clinical/ Accessed 24 June 2015.
Ebrahim SH, Anderson JE, Weidle P, et al. Race/ethnic disparities in HIV testing and knowledge about treatment for HIV/AIDS: United States, 2001. AIDS Patient Care STDs. 2004;18(1):27–33.
Murray K, Oraka E. Racial and ethnic disparities in future testing intentions for HIV: US, 2007–2010: results from the National Health Interview Survey. AIDS Behav. 2014;18(7):1247–55.
Gardner EM, McLees MP, Steiner JF, et al. The spectrum of engagement in HIV care and its relevance to test-and-treat strategies for prevention of HIV infection. Clin Infect Dis. 2011;52(6):793–800.
Skarbinski J, Rosenberg E, Paz-Bailey G, et al. Human immunodeficiency virus transmission at each step of the care continuum in the US. JAMA Intern Med. 2015;175(4):588–96.
Ojikutu B, Nnaji C, Sithole J, et al. All black people are not alike: differences in HIV testing patterns, knowledge, and experience of stigma between US-born and non–US-born blacks in Massachusetts. AIDS Patient Care STDs. 2013;27(1):45–54.
Bogart LM, Derose KP, Kanouse DE, et al. Correlates of HIV testing among African American and Latino church congregants: the role of HIV stigmatizing attitudes and discussions about HIV. J Urban Health. 2015;92(1):93–107.
Doshi RK, Malebranche D, Bowleg L, et al. Health care and HIV testing experiences among Black men in the South: implications for “Seek, Test, Treat, and Retain” HIV prevention strategies. AIDS Patient Care STDs. 2013;27(2):123–33.
Lepkowski JM, Mosher WD, Davis KE, et al. National Survey of Family Growth, Cycle 6: sample design, weighting, imputation, and variance estimation. Vital Health Stat. 2006;2(142):1–82.
National Center for Health Statistics (U.S.). Responsive design, weighting, and variance estimation in the 2006–2010 National Survey of Family Growth. Hyattsville: U.S. Dept. of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics; 2013.
Lepkowski JM, Mosher WD, Groves RM, et al. Responsive design, weighting, and variance estimation in the 2006–2010 National Survey of Family Growth. Vital Health Stat. 2013;2(158):1–52.
Branson BM, Handsfield HH, Lampe MA, et al. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. J Natl Med Assoc. 2008;100(1):131–47.
Lau JS, Adams SH, Irwin CE, Ozer EM. Receipt of preventive health services in young adults. J Adolesc Health. 2013;52(1):42–9.
Robinson KT, Sanders SA, Boyd JL. High-risk HIV minorities in the United States: Who gets tested and where? Am J Health Behav. 2012;36(3):348–59.
Talib HJ, Silver EJ, Coupey SM, et al. The influence of individual, partner, and relationship factors on HIV testing in adolescents. AIDS Patient Care STDs. 2013;27(11):637–45.
Arnold EA, Rebchook GM, Kegeles SM. ‘Triply cursed’: racism, homophobia and HIV-related stigma are barriers to regular HIV testing, treatment adherence and disclosure among young Black gay men. Cult Health Sex. 2014;16(6):710–22.
Valdiserri RO. Mapping the roots of HIV/AIDS complacency: implications for program and policy development. AIDS Educ Prev. 2004;16(5):426–39.
Petroll AE, DiFranceisco W, McAuliffe TL, et al. HIV testing rates, testing locations, and healthcare utilization among urban African-American men. J Urban Health. 2009;86(1):119–31.
Swenson RR, Rizzo CJ, Brown LK, et al. Prevalence and correlates of HIV testing among sexually active African American adolescents in four US cities. Sex Transm Dis. 2009;36(9):584.
Carter MW, Kraft JM, Hatfield‐Timajchy K, et al. STD and HIV testing behaviors among black and Puerto Rican young adults. Perspect Sex Reprod Health. 2011;201143(4):238–46.
Marks G, Crepaz N, Senterfitt JW, et al. Meta-analysis of high-risk sexual behavior in persons aware and unaware they are infected with HIV in the United States: implications for HIV prevention programs. JAIDS J Acquir Immune Defic Syndr. 2005;39(4):446–53.
Nunn A, Zaller N, Cornwall A, et al. Low perceived risk and high HIV prevalence among a predominantly African American population participating in Philadelphia’s rapid HIV testing program. AIDS patient care STDs. 2011;25(4):229–35.
Nyblade L, Stangl A, Weiss E, Ashburn K. Combating HIV stigma in health care settings: what works? J Intern AIDS Soc. 2009;12(1):15.
Abara W, Coleman JD, Fairchild A, et al. A faith-based community partnership to address HIV/AIDS in the southern United States: implementation, challenges, and lessons learned. J Relig Health. 2015;54(1):122–33.
Obermeyer CM, Osborn M. The utilization of testing and counseling for HIV: a review of the social and behavioral evidence. Am J Public Health. 2007;97(10):1762.
United States Preventive Services Task Force. Human Immunodeficiency Virus (HIV) Infection: Screening. Available at http://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/human-immunodeficiency-virus-hiv-infection-screening?ds=1&s=HIV. Accessed 21 Feb 2016.
Abara W, Heiman HJ. The Affordable Care Act and low-income people living with HIV: looking forward in 2014 and beyond. J Assoc Nurses AIDS Care. 2014;25(6):476–82.
Conserve D, King G, Turo A, Wafula E. Cigarette smoking and alcohol use as predictors of HIV testing in the United States: Results from the 2010 National Health Interview Survey. AIDS Care. 2014;26(7):842–9.
Acknowledgments
This study was supported by a training grant from the National Institute of Health, National Institute of Allergy and Infectious Diseases (T32 AI007001).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Donaldson F. Conserve has received training grant support from the National Institute of Health, National Institute of Allergy and Infectious Diseases and has no conflict of interest. Emeka Oraka declares that he has no conflict of interest. Winston E. Abara declares that he has no conflict of interest. Edith Wafula declares that she has no conflict of interest. Angela Turo declares that she has no conflict of interest.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Conserve, D.F., Oraka, E., Abara, W.E. et al. Correlates of Never Testing for HIV Among Non-Hispanic Black Men in the United States: National Survey of Family Growth, 2011–2013. AIDS Behav 21, 492–500 (2017). https://doi.org/10.1007/s10461-016-1452-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-016-1452-4