
Abstract
Adaptive expertise has been promoted as an emerging model of expertise in health professions education in response to the inherent complexities of patient care; however, as the concept increasingly influences the structure of professional training and practice, it creates the potential for misunderstandings of the definition and implications of adaptive expertise. To foster a common understanding of the concept, we conducted a scoping review to explore how adaptive expertise has been discussed within health professions education literature. Five databases—MedLine, PubMed, ERIC, CINAHL, and PsycINFO—were searched using the exact term “adaptive expertise”, producing 212 unique articles. Fifty-eight articles met inclusion criteria. In the included articles, authors discussed the conceptual implications of adaptive expertise for health professions education, strategies for training for adaptive expertise, and research findings aimed at supporting the development of adaptive expertise or utilizing adaptive expertise as a theoretical framework. The goal of this scoping review is to establish a resource for frontline educators tasked with fostering the development of adaptive expertise in learners through education initiatives. A common understanding of adaptive expertise is essential to ensuring effective implementation in training programs.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Taking care of the health of human beings and communities is complex and often unpredictable. Not only are physicians required to respond to the inherently complex needs of individual patients, but physicians also work and learn within dynamic networks of healthcare workers and interprofessional communities. Further, the astonishing speed of societal transformation resulting from technological advances and the information revolution (Thimbleby, 2013) has had a profound impact on how patients interact with their healthcare providers. Clinical research regularly results in the need to adjust previously standard ways of practice, and often produces new knowledge that must be mastered—which may also entail “unlearning” what was previously accepted as truth. All of these factors and more contribute to the need for healthcare practitioners to be able to be flexible and adaptable. So how can healthcare providers be prepared to effectively meet this challenge? How can training programs prepare their graduates with the tools and skills to be able to adapt as needed when faced with unfamiliar or new situations? A potential solution is to explicitly incorporate the concept of adaptive expertise into healthcare professions education (HPE).
Initially proposed by Hatano and Inagaki (1984) to explain differences in the development of skills in solving math problems, the concept of adaptive expertise proposes that there are two kinds of expertise: routine expertise, and adaptive expertise. As originally conceptualized, routine expertise requires mastery of skills, knowledge, and procedures so that carrying out the processes or actions (problem-solving) associated with those skills and knowledge is highly efficient and accurate. Adaptive expertise requires similar levels of mastery, but also incorporates deeper conceptual understanding and insight, so that the adaptive expert can solve new problems that are outside those assumed by routine expertise, or even develop new processes or procedures for problem-solving that differ from those learned/mastered in developing routine expertise (Fig. 1). It is important to note that this conceptualization of expertise does not assume that routine and adaptive expertise are two sides of a dichotomy – routine experts can demonstrate adaptive expertise, and adaptive expertise still requires the foundation of mastery needed for routine expertise.

The relationship between routine expertise and adaptive expertise is not a dichotomy. Rather, adaptive expertise is an extension of routine expertise characterized by a deeper conceptual understanding that facilitates innovation and creativity in problem-solving, balanced by efficiency and good judgement about when and when not to innovate. Both types of expertise are essential to health professionals
Much of the initial research and instructional interventions about adaptive expertise took place in the context of mathematics education, with a focus on understanding differences in how novices and experts approach arithmetical problem-solving (Baroody et al., 2013; Hatano & Oura, 2003; McMullen et al., 2020; Verschaffel et al., 2009). The applicability of the adaptive expertise concept applied to all areas of education — students often learn through problem-solving — which resulted in a sustained interest in adaptive expertise among researchers in teacher education (Crawford et al., 2005; Janssen et al., 2008; McDiarmid and Clevenger-Bright, 2008; Metz et al., 2020; Soslau, 2012; Tynjälä et al., 2006). Beyond the classroom, adaptive expertise research rapidly expanded as researchers explored the ways that experts approach problem-solving in challenging, novel, unfamiliar, or complex situations (Bransford et al., 2000; Carbonell et al., 2014; Schwartz et al., 2005; Wineburg, 1998). Other researchers wanted to examine and understand why some people were flexible in how they used their existing knowledge and skills, while others were unable to solve non-routine problems or adapt to changes in circumstances (Hutton et al., 2017; Newton et al., 2010; Spiro, 1988).
Understanding what processes underlie the ability to be flexible in response to challenge and to demonstrate appropriate application of knowledge in non-routine situations is the essential first step in developing educational interventions and strategies to support the development of adaptive expertise. Research into adaptive expertise has identified some of the key characteristics of people who demonstrate adaptive expertise (Carbonell et al., 2014): well-developed metacognitive skills such as monitoring one’s own performance and learning, and assessing one’s own level of knowledge (Bransford, 2007; Crawford et al., 2005; Lin et al., 2005; Janssen et al., 2008; Mees et al., 2020); flexibility (Baroody, 2003; Mees et al., 2020); and creativity (Gube & Lajoie, 2020). Given how closely these characteristics mirror many of the elements of self-regulated learning (SRL), it is not surprising that many authors have made the connection between fostering SRL behaviours and the development of adaptive expertise (Anthony et al., 2015; Lajoie & Gube, 2018; Vanasupa et al., 2010). As will be seen in the Results and Discussion, the connection between SRL and adaptive expertise is of interest in the HPE literature (e.g., Lajoie & Gube, 2018), where SRL serves as the basis for the Master Adaptive Learner model (Cutrer et al., 2018).
Adaptive expertise is particularly important for those working in professions or environments where complexity, challenge, and novelty occur regularly (Carbonell et al., 2014; Grenier, 2021). Researchers in professions that are characterized by the need to adapt in complex circumstances, such as engineering (Harris et al., 2002) and the military (Hutton et al., 2017), have embraced adaptive expertise as a useful way to frame the skills necessary for training professionals who are well-suited for challenging work. Findings from adaptive expertise research in other contexts have begun to inform the development of educational interventions that are intended to support the development of adaptive expertise, such as the “Coaching for Improved Ability to Handle Unforeseen Events” (CIAU) program for nuclear power plant operators in Norway (Skjerve and Holmgren 2018). Nuclear power plants are high-risk environments that have multiple levels of safety measures which include strict operational and procedural routines. Licensed operators must have high procedural fluency for carrying out these routines. However, it is possible for serious accidents to arise from unforeseen circumstances or series of events (David et al., 1996). The CIAU program leverages what is known about the metacognitive processes that underpin adaptive expertise in order to promote flexible thinking and adaptivity in nuclear power plan workers so that they can perform a high-risk profession safely, even when faced with challenge and non-routine circumstances.
Given the relevance of adaptive expertise to effective performance of high-risk tasks in challenging, unpredictable, or complex circumstances (Feltovich et al., 1997), it is not surprising that there has been intense interest in how the concept of adaptive expertise may apply in the health professions. Healthcare professionals and learners face complexity daily, both in navigating the healthcare system and in caring for patients (Woodruff, 2019). While HPE programs try to design instruction to prepare graduates for the complexity of healthcare, it is impossible to train for every eventuality. This is particularly true for clinical situations that are high in acuity but low in frequency, which often need to be taught using simulation scenarios (Brown & Mackinnon, 2016; Wheeler et al., 2013). Unfortunately, teaching specific high acuity/low frequency scenarios is generally not effective, as skills are lost without opportunities to practice (Hatchimonji et al., 2020). Incorporating adaptive expertise into HPE programs may provide a solution, by targeting how healthcare practitioners approach challenge and novelty in the clinical context, rather than training for specific scenarios (Mylopoulos et al., 2018a).
Adaptive expertise as a concept first appeared in the HPE literature when Mylopoulos and Regehr proposed adaptive expertise as an alternative or complement to some of the more traditional cognitive paradigms for thinking about expertise (Mylopoulos & Regehr, 2007). Mylopoulos and Regehr made the argument that a potential reason for some of the challenges inherent in researching the development of expertise may have been the result of limitations of the cognitive paradigms being used. Specifically, the authors argued that most research in medical expertise at the time focused on outputs from tasks (real or artificial) as proxies for how experts versus novices used knowledge, rather than on the creative processes that experts used to solve the task. In introducing the concept of adaptive expertise into HPE, Mylopoulos and Regehr contributed to a shift in thinking about expertise from comparing novice versus expert to considering how expertise continuously develops and how different experts solve problems or enact their expertise (Mylopoulos & Scardamalia, 2008; Mylopoulos & Woods, 2009; Sockalingam et al., 2016).
While the introduction of the concept of routine and adaptive expertise has opened up new ways of thinking about expertise, the rapidity with which this model has been embraced comes with some potential risks. As is the case any time that a construct, concept, theory, or model from one context is introduced into a novel context — especially a context as specialized as healthcare — it is essential to ensure there is consistency in how those ideas are understood as they are taken up by scholars in the new context. It is important to keep in mind that the concepts of routine and adaptive expertise were initially theorized in the context of math education and child development to explain differences in approaches to solving math problems. In this context, there are clear routines and sub-routines associated with mathematical functions and strategies for mathematical problem-solving (Carbonell & Dailey-Hebert, 2021), allowing for relative ease in identifying novel approaches in strategy use. Contrast this with the context of healthcare practice, where routines and sub-routines are not as distinct, nor even uniformly common across specialties and sub-specialties. Given the differences between the contexts of mathematical problem-solving and clinical care, it is not surprising that some of the nuances of the concepts of routine and adaptive expertise may be lost in translation. This issue may be further exacerbated by the rise in popularity of guidelines and the call for more standardization implicit in ‘best practices’ and quality improvement, which can make the case that healthcare is on the path of establishing what ‘routine care’ looks like. It is important to ensure that both learners and practitioners understand that adaptive expertise does not mean dispensing with or rejecting routine expertise and guidelines; rather, adaptive expertise is needed for recognizing when a guideline does not apply, or when the guideline needs to be applied for a specific patient in a specific way.
The potential for differing understandings of routine and adaptive expertise becomes concerning when considering the increasing call for incorporating adaptive expertise into HPE (Edje & Price, 2021; Lajoie & Gube, 2018; Mylopoulos et al., 2018a; Steinert et al., 2021; Woods et al., 2021). While the scholars immersed in writing about adaptive expertise possess in-depth knowledge, those are not the frontline educators who will be tasked with implementing initiatives to support and foster the development of adaptive expertise in learners in HPE programs. Further, as more authors begin to contribute to the adaptive expertise literature, there is a concurrent increase in the potential for misunderstandings and differing conceptualizations in both academic and clinical audiences.
As health professions educators find themselves faced with expectations of teaching and assessing adaptive expertise, it is crucial to examine the ways in which adaptive expertise is defined and described in the HPE literature. Through exploring different authors’ definitions and descriptions of adaptive expertise, we aimed to identify opportunities to foster a common understanding among frontline educators. Further, we sought out examples of recommendations for how training programs could support the development of adaptive expertise. Our overall goal was to consolidate information from disparate sources to provide frontline educators with a primer for understanding what adaptive expertise is and how development of adaptive expertise can be supported through teaching and assessment.
Methods
This scoping review follows the framework developed by Arksey and O’Malley (2005). Our goal in this study was not to appraise the quality of included studies, and so a systematic review approach was not appropriate. Rather, we were interested in creating a general overview of available knowledge about how adaptive expertise is defined in the HPE literature, and the ways in which authors have proposed or implemented interventions to support the development of adaptive expertise in health professions learners. Given this purpose, we determined that a scoping review would be appropriate as we were interested in rapidly examining the extent, range, and nature of research activity and available evidence underpinning the research area (Daudt et al., 2013; Levac et al., 2010; Peterson et al., 2017). The Arksey and O’Malley (2005) framework identifies five stages: (1) identifying the research question; (2) identifying relevant studies; (3) study selection; (4) charting the data; (5) collating, summarizing, and reporting the results. Following these stages, an optional consultation exercise to inform and validate findings is identified as an opportunity to enhance results. The use of this framework promotes transparency and replicability of study findings.
Stage 1 Identifying the research question
The research questions guiding this review were:
-
1.How is adaptive expertise defined within HPE literature?
-
2.How can HPE programs support the development of adaptive expertise?
Stage 2 Identifying relevant studies
The primary goal of this scoping review is to explore how the concept of adaptive expertise is defined and applied in HPE in order to consolidate this information for frontline health professions educators. We focused on published literature in HPE. In June 2021, we searched the following databases using the exact term “adaptive expertise” for the years 1984–2021: MedLine, PubMed, ERIC, CINAHL, and PsycINFO. Our start year reflects the year that the term adaptive expertise was first introduced by Hatano and Inagaki. We intentionally used the databases above to capture a broad range of education literature, which we would then further narrow to HPE literature in the ensuing stages of the study, as described in the following section. Additionally, we reviewed references lists of included articles for any additional literature not captured in the initial search. However, as the purpose of this study was to provide a general overview of adaptive expertise in HPE, our secondary searching was not exhaustive, and was limited to publications in peer-reviewed journals. This was a deliberate decision made by the team, in recognition of the trade-off between breadth, comprehensiveness, and feasibility in conducting scoping reviews (Daudt et al., 2013; Levac et al., 2010), and we found that our initial search provided a comprehensive database of articles suitable for the purpose of this study.
Stage 3 Study selection
Inclusion criteria for this study included articles which discussed adaptive expertise with specific reference to its role in HPE (Table 1). This included articles both discussing theoretical considerations of adaptive expertise, and research aimed at supporting the development of adaptive expertise in training. Although a previous scoping review explored adaptive expertise within education (Kua et al., 2020), we specifically limited our focus to HPE literature to ensure that any theoretical considerations or research that we identified were in our context of interest. Our context of interest included all populations of HPE learners and all levels (i.e. undergraduate, postgraduate, continuing profession development, etc.) of HPE in order to capture a breadth of available literature. One reviewer (NC) determined initial eligibility of articles, with frequent consultation with the full research team to verify appropriate inclusion or exclusion of articles.
Stage 4 Charting the data
For each article, data extraction included descriptive information such as authorship, year of publication, geographic location, and discipline. As inclusion criteria included non-research studies, specific data extracted from articles included definitions of adaptive expertise and strategies to promote its inclusion in HPE training and practice.
Stage 5 Collating, summarizing, and reporting the results
Summarizing and synthesizing the extracted data was done initially by NC, in consultation with SR and BH. The team adopted a subjectivist epistemology (Thomas et al., 2020) because the goal of this scoping review was to examine and summarize theoretical descriptions of the construct of adaptive expertise, as well as to describe strategies and interventions to support learners in developing adaptive expertise in the context of HPE, and all team members are HPE scholars. In examining the data each team member brought pre-existing knowledge of and experience with HPE, and interpretation of the data would be filtered through the team members’ existing expertise (Brannick & Coghlan, 2007; Guba & Lincoln, 1994). In particular, the team members approached the data from a generalist physician perspective (i.e., family medicine), with experience across the continuum of education (undergraduate, postgraduate, and continuing professional education) (Thomas et al., 2020). In discussing the initial synthesis of data, NC, SR, and BH acknowledged the prior knowledge and theoretical perspectives that they were bringing to interpretation of the data, as well as the specific generalism context in which SR and BH conduct their scholarly work (Feast & Melles, 2010). This process of acknowledging and reflecting on existing knowledge and expertise, including the generalist contextual lens which each team member was bringing to the interpretation and analysis of the data, was also followed in the Consultation exercise in Stage 6.
Stage 6 Consultation exercise
As synthesis progressed, two consultation sessions were held with the Certification Process and Assessment Committee (CPAC) of the College of Family Physicians of Canada. Previous CPAC work has considered the role of adaptability in family medicine practice and training. CPAC members reviewed the synthesis, and offered suggestions and comments on the relationship between adaptive expertise and HPE. Final synthesis was determined through agreement between CPAC and the research team.
In keeping with the subjective epistemology approach, the research team explicitly acknowledged that the synthesis and interpretation of the findings of this scoping review would be influenced by the subjective judgement of the research team (Brannick & Coghlan, 2007; Thomas et al., 2020). The research team brought a generalist, education-focused perspective to the synthesis and interpretation of the data, with additional contextual lens of summarizing the adaptive expertise literature for frontline clinical educators. As a result, the reporting of extracted data in the Results section attempts to position findings both with respect to the research questions guiding this review, as well as within historical conceptualizations of adaptive expertise. This latter consideration can help deepen our understanding of how adaptive expertise has been adopted within HPE, and further acknowledge strategies to support the development of adaptive expertise in education programs.
Results
Across the five databases, the search resulted in 212 unique articles. Upon abstract and full-text review of these articles, 58 met inclusion criteria (Fig. 2). The earliest included article is from 2007 — suggesting the influence of the aforementioned Mylopoulos and Regher article to the field of health profession education. Thirty articles were commentary-type articles that discussed the theoretical implications of adaptive expertise or its relationship to HPE; the remaining 28 articles reported research aimed at supporting the development of adaptive expertise or utilizing adaptive expertise as a theoretical framework (Table 2). The data extraction table is included as an Appendix.

PRISMA diagram for the scoping review search
How is adaptive expertise defined within HPE literature?
Definitions and descriptions of adaptive expertise in HPE are generally aligned with Hatano and Inagaki’s (1984) original conceptualization, albeit with added dimensions of patient care and patient safety. Most authors define adaptive expertise as a model of expert development and performance that emphasizes a balance between efficiency and innovation (Cutrer et al., 2017; Lake et al., 2019; Mylopoulos & Woods, 2009, 2017; Pusic et al., 2018a, 2018b; Sockalingam et al., 2016, 2020).
Most authors describe adaptive expertise in the context of how adaptive experts respond to problems or challenges. Rather than viewing problems solely as an avenue to apply previous knowledge, adaptive experts approach problems as opportunities to create new knowledge, for innovation and creativity, and to learn and improve practice (Mylopoulos & Scardamalia, 2008). Potential challenges identified in the examined articles include working with complex patient populations (Biro et al., 2021; Grossnickle et al., 2019; Kawamura et al., 2016), within dynamic team-based systems of care (Orsino & Ng, 2019; Salas et al., 2008) and interactions with novel healthcare technologies (Gegenfurtner et al., 2017; Guo et al., 2013; Varpio et al., 2009). Most articles described adaptive expertise as the capacity to recognize when a routine approach to problem solving is insufficient, and the ability to reframe the problem in order to invent new solutions and learn new knowledge (Bleakley, 2021; Cutrer & Ehrenfeld, 2017; Mylopoulos & Woods, 2014; Mylopoulos et al., 2018a).
In describing adaptive expertise, all authors also describe routine expertise; however, the ways in which authors describe the relationship between routine and adaptive expertise can appear contradictory. For example, consider this statement from Kawamura et al., (2020):
“Adaptive experts are characterized by the procedural fluency of knowing how to complete tasks, as seen in routine experts, complemented by an understanding of why an approach works within a specific context. This explicit conceptual understanding is what sets adaptive experts apart from routine experts as it permits adaptation to variability.”
The notion of setting adaptive experts apart from routine experts might be inferred to suggest a dichotomy with routine expertise, but it is important to remember that adaptive experts still utilize routine expertise. Efficiency in practice — or routine expertise — is complemented by problem solving in novel, complex, or ambiguous situations. Rather, the key distinction emphasized in the above quotation is that routine expertise lacks the innovative capacity observed in adaptive expertise.
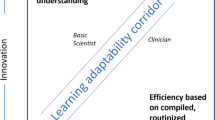
In one of the earliest publications introducing the concept of adaptive expertise to HPE, Mylopoulos and Regehr (2009) described the “optimal adaptability corridor” (OAC) (Schwartz et al., 2005). The OAC represents the balance between the efficiency and innovative dimensions of problem solving (Mylopoulos & Regehr, 2009; Mylopoulos & Woods, 2009). In more recent publications in the HPE literature (i.e., since 2017), there has been an increase in the number of authors who describe adaptive expertise as it relates to the OAC, likely due to a publication in Academic Medicine by Cutrer and colleagues in 2017 that included a figure of the OAC adapted from the original from Schwartz et al., (2005).
Most authors also describe the metacognitive processes, professional dispositions, and habits of inquiry that are incorporated into adaptive expertise (Mylopoulos & Woods, 2009; Valbuena et al., 2019) (Table 3). These factors are incorporated into the recommendations for how training programs can support the development of adaptive expertise that are described in the final section of the Results.
How can HPE programs support the development of adaptive expertise?
In almost all of the included papers, authors either explicitly or implicitly addressed the need to design training to support the development of adaptive expertise. A number of papers offered specific recommendations for training curriculum to support the development of adaptive expertise (Croskerry, 2018; Edje & Price, 2021; Fu, 2019; Hutchinson et al., 2019; Mylopoulos et al., 2018b; Quirk & Chumley, 2018; Valbuena et al., 2019). Many authors, especially in commentary or perspective articles, contrasted traditional educational approaches or strategies that emphasized solely routine expertise with the need for alternative approaches that emphasize adaptive expertise (Cutrer et al., 2017; Mylopoulos & Regehr, 2009; Mylopoulos & Woods, 2009; Rose, 2007). These authors point out that curricula and instructional approaches that focus on maximizing short-term performance through the acquisition and application of previous knowledge — as traditionally emphasized in training curriculum — is insufficient for long-term learning, and does not prepare learners to solve problems in novel situations (Mylopoulos et al., 2018b; Sockalingam et al., 2016). The recommendations for educational approaches or strategies described by authors of the included papers all shared the aim of preparing learners to practice within the OAC, by moving beyond the acquisition and application of knowledge to demonstrating the capacity to learn and/or create new knowledge in order to adjust performance appropriately in the face of novel situations (Cutrer et al., 2017; Mylopoulos & Regehr, 2009). The recommendations are grouped under two prevalent conceptualizations: preparation for future learning and the Master Adaptive Learner model.
Preparation for future learning (PFL) is described as “the capacity to learn new information, to use resources effectively and innovatively, and to invent new strategies for learning and problem solving in practice” (Mylopoulos et al., 2016). Mylopoulos and colleagues (2018a) present three approaches to education that support PFL and, subsequently, adaptive expertise: emphasizing understanding rather than performance, emphasizing struggle and risk taking, and supporting meaningful variation. The integration of biomedical or basic science knowledge with clinical knowledge (Dickinson et al., 2020; Martimianakis et al., 2020; Mema et al., 2020; Mylopoulos et al., 2018b; Mylopoulos & Woods, 2014; Ravitz, et al., 2019; Sockalingam et al., 2020) and the use of contrasting cases in training has been promoted as a strategy to build conceptual understandings of knowledge (Mema et al., 2020; Mylopoulos & Woods, 2017; Mylopoulos et al., 2018b). Meanwhile, active learning strategies — and, more generally, learning environments in which risk-taking, creativity, and innovation are encouraged — can also support the development of PFL (Biro et al., 2021; Guo et al., 2013; Sockalingam et al., 2021; Steenhof et al., 2020; Steenhof et al., 2019). Finally, clinical educators can instil the belief that innovative problem solving is a core competency for healthcare professionals by role modeling and by making explicit efforts to provide learners with legitimate experiences in which they can meaningfully engage in innovative problem-solving during training (Mylopoulos & Regehr, 2009; Mylopoulos & Scardamalia, 2008).
Similar recommendations were found in articles that cited the Master Adaptive Learner (MAL) model recently proposed by Cutrer and colleagues (Cutrer et al., 2017, 2018). The MAL combines aspects of the Plan-Do-Study-Act cycle of quality improvement with metacognitive aspects of the theory of self-regulated learning (SRL) (Butler & Brydges, 2013; Zimmerman, 2002). In the MAL model, there are four stages for effective learning: identify gaps in knowledge, engage in learning, evaluate what was learned, and incorporate this learning into practice. These stages do not occur in isolation: curiosity, motivation, mindset, and resilience promote and sustain the learner’s ability to engage in the learning cycle, with support and guidance from coaching and the learning environment (Cutrer et al., 2018). The model stresses the importance of cognitive skills — specifically, critical thinking and reflection — as essential to learning (Cutrer et al., 2017). Several authors of the included studies referred to the MAL framework to help understand the development of adaptive expertise (Dickinson et al., 2020; Edje & Price, 2021; Gisondi et al., 2021; Regan et al., 2019).
Some authors report on qualitative research studies, including interviews, focus groups, or observational research to understand how students or teachers understand or define expertise, adaptiveness, or innovation in practice, and portfolios, journals, or similar assessments intended to stimulate critical reflection (Bradfield et al., 2019; Dickinson et al., 2020; Grossnickle et al., 2019; Kawamura et al., 2020; Kawamura et al., 2016; Mylopoulos et al., 2017; Mylopoulos & Woods, 2014; Mylopoulos & Farhat, 2015; Mylopoulos & Regehr, 2009; Mylopoulos & Scardamalia, 2008; Reed, 2018; Regan et al., 2019; Sockalingam et al., 2020; Sockalingam et al., 2021; Varpio et al., 2009). The findings from these studies provide insight into how clinical educators, practitioners, and learners think about expertise, and about how experiences in training and practice contribute to development of expertise. This information adds to understanding how PFL or MAL instructional recommendations may contribute to development of adaptive expertise.
While there was consistency among authors in the recommendations for instructional strategies or approaches to support development of adaptive expertise, few authors provided evaluation evidence. For PFL, research has focused on evidence of transfer: the extent to which students are able to transfer their knowledge from one problem-solving situation to a different, yet related, context (Croskerry, 2018; Gegenfurtner et al., 2017; Martin & Schwartz, 2009; Pusic et al., 2018a, 2018b). Case-based simulations provide some evidence (Guo et al., 2013; Mema et al., 2020). However, many transfer protocols, especially those that address future learning, have fairly effortful designs that are not easily or feasibly implemented in HPE programs, such as eye-tracking studies (Gegenfurtner et al., 2017) and double transfer protocols that endeavour to determine whether a PFL assessment can reveal differences in performance that would otherwise be undetected by traditional assessment methods (Mylopoulos & Woods, 2014; Steenhof, 2020; Steenhoff et al., 2019, 2020).
Discussion
The goal of this scoping review was to consolidate published information about what adaptive expertise is, and how educators can support development of adaptive expertise in their learners, specifically in the context of HPE. While there is a growing body of literature to support the adoption of adaptive expertise into HPE (Kua et al., 2021), much of that literature is more conceptual than applied, and many busy frontline educators may not have the capacity to engage with that conversation. We wanted to provide a resource to promote a common understanding among frontline healthcare professions educators of how adaptive expertise is defined and can be applied in the HPE context. Holding a common understanding of the ‘what’ and ‘how’ of adaptive expertise will facilitate more effective uptake and implementation of strategies in clinical training programs and environments (Lane et al., 2015).
Our findings suggest that there is a fairly consistent description of adaptive expertise both within HPE as well as with respect to the conceptualization originally proposed by Hatano and Inagaki (1984). Adaptive expertise provides a model of expert development that incorporates both efficiency and innovation. Innovation is necessary to respond to the inherent complexity of healthcare; however, this is not to suggest that innovation replaces the necessity for efficiency in healthcare (Pusic et al., 2018a, 2018b). Just as an inability to be adaptive in a complex situation may result in poor patient care (Woodruff, 2019), being overly innovative in a situation which has a known solution may also result in poor patient care (Earl, 2019; Mylopoulos & Woods, 2017; Soni et al., 2016). While much of a healthcare provider’s practice includes consistency in what clinical presentations are seen, alongside the expected can be the unexpected — the novelty, uncertainty, and ambiguity which can arise in many areas of clinical practice (Woodruff, 2019).
Both within and outside the HPE literature, adaptive expertise is often graphically depicted in the form of a simple four quadrant grid. The y-axis represents increasing innovation, while the x-axis depicts increasing efficiency (Cutrer et al., 2017; Schwartz et al., 2005). Routine expertise is thus high in efficiency and low in innovation; adaptive expertise is high in both efficiency and innovation. While this commonly repeated depiction is a useful visual to communicate a more complex concept, it can lead to misinterpretation of the relationship of routine and adaptive expertise, with routine expertise being “less than” adaptive expertise. This potential misinterpretation runs counter to what was originally proposed by Hatano and Inagaki (1984), and built upon by other scholars who discussed the interrelationship of routine and adaptive expertise. Routine expertise is both a necessary precursor to adaptive expertise and is often employed at the same time as adaptive expertise: adaptive expertise is not free of content knowledge, and rather builds off extensive domain-specific knowledge or else risks innovation without the necessary sufficient judgement (Martimianakis et al., 2020; Mylopoulos et al., 2018a, 2018b). Further, routine expertise can be seen as a way to maximize an individual’s ability to be creative and innovate – the procedural fluency of routine expertise means that some of the routine subtasks of care can happen on “autopilot”, freeing up cognitive capacity for innovative problem-solving in the face of challenge or novelty (Carbonell & Dailey-Hebert, 2021; Gube & Lajoie, 2020; Schneider & Stern, 2010).
In the Introduction to this paper, we present a figure that offers a different way of visualizing the relationship between routine and adaptive expertise (Fig. 1). In the health professions in particular, routine expertise is essential for many aspects of patient care. Adaptive expertise builds upon that routine expertise, and enables clinicians to adeptly respond to challenges, or problem-solve in the face of situations that are not routine or do not follow established patterns. In Fig. 3, we build upon this visualization of the continuum of expertise to depict the OAC in the context of HPE. This Figure explicitly shows how the recommendations for teaching strategies to support development of adaptive expertise fit into the conceptual model, which can be useful for faculty development as training programs implement those strategies. Moreover, Fig. 3 reflects how routine expertise can lead to the development of adaptive expertise through certain enabling factors presented in Table 3, further highlighting the relationship between adaptive and routine expertise. Importantly, evidence across the continuum of education has demonstrated that students who receive forms of instruction that have been shown to support the development of adaptive expertise perform significantly better on PFL assessments with no detriment to knowledge acquisition and application — in other words, an explicit emphasis on innovation in training does not come at the cost of routine expertise (Mylopoulos & Woods, 2014; Mylopoulos et al., 2016; Steenhof et al., 2019).

The optimal adaptability corridor in health professions education (HPE) expanding on Bransford’s original proposition in 2005. Routine expertise is appropriate in most clinical situations, and is characterized by high efficiency and accuracy. However, when novel or challenging situations are encountered, innovation and creativity are needed to problem-solve — i.e., adaptive expertise. The arrow between routine expertise and adaptive expertise captures the key elements necessary to go from routine expertise to adaptive expertise. HPE programs can implement strategies to target the “optimal adaptability corridor” — the balance between being efficient and being innovative — to help learners to the necessary knowledge, skills, and procedures of routine expertise, while providing safe challenges to facilitate innovation and creativity in problem-solving, and the skill to balance efficiency and innovation appropriately (i.e., judgement to know when and when not to innovate) to support development of adaptive expertise
In working with frontline educators, a useful approach could be to present adaptive expertise as a marker of competence (Edie & Price, 2021). As noted by Regehr (1994), true competence manifests in unfamiliar situations, and it is inevitable that physicians will encounter novel problems in practice. Emerging work suggests that adaptive expertise may be a mindset that is stimulated by the realities of the complexity of authentic clinical practice, where the limits of routine expertise become evident (Betinol et al., 2022). Programs can create situations that allow learners to try out and reflect upon adaptive expertise strategies during training. Assessment of both the reflections and the strategies used could then become part of programmatic assessment of competence. This integrates adaptive expertise into expectations of competence, preparing learners to work with and learn from novel problems in the future (Gisondi et al., 2021). Further, an explicit focus on PFL in training promotes expertise as a process of lifelong learning rather than an endpoint (Alderson, 2010; Brehaut & Eva, 2012; Mukherjee et al., 2019), and embeds knowledge production in daily practice (Mylopoulos & Scardamalia, 2008). Similarly, the SRL concepts that were adapted for the MAL model have strong research evidence from the non-HPE literature to support their effectiveness and importance to lifelong learning (Winne, 2017; Zimmerman, 2002) and adaptive expertise (Anthony et al., 2015; Vanasupa et al., 2010), which is highly suggestive that using the MAL model in training will have similar benefits.
Given the emphasis on novelty, challenge, and uncertainty that are core to adaptive expertise, it is not surprising that this concept has rapidly gained traction among generalists. Kelly et al., (2021) identify six key concepts to inform the praxis of generalist care: comprehensive care, complexity, context, continuity of care, communication, and collaboration. The authors identify adaptive expertise as integral to the response to variability of context in practice; however, through this model, we can see the potential for adaptive expertise to further underpin some of the core components of generalism: managing complexity, uncertainty, and ambiguity in practice, responding to the needs of individual patients while negotiating personal and professional and even cultural boundaries, and participating within complex networks of care. Kvern (2021) also defines generalism both in relation to commitment to patients and the implied capability for problem solving in unexpected situations. Within the context of family medicine, Woods et al., (2021) propose adaptive expertise as a theoretical framework to support the practice and training of the “specialist generalist”, enabling resourcefulness when faced with ambiguity, the ability to balance innovation and efficiency, and acknowledges the different ways family physicians may conceptualize practice.
Medical education often teaches through ideal cases in order to present concepts with clarity and build procedural fluency (Bekdache et al., 2019). Acknowledging the different settings and populations in which generalists provide care, it is important to consider how uncertainty and complexity might be incorporated into workplace-based learning environments; moreover, it is essential that a greater emphasis on uncertainty and ambiguity in training does not come at the cost of comprehensive, patient-centered care. While certain strategies have been presented in this review that support the development of adaptive expertise in training, careful consideration must be given to how they may be implemented judiciously within a training program.
This last point relates to the two gaps we identified in this scoping review that must be addressed as programs begin to implement strategies to support development of adaptive expertise. First, evaluation evidence is sparse for many of the recommended teaching strategies — particularly evidence from HPE contexts, although this need for more evaluation evidence has also been noted in the non-HPE literature (Axelsson & Jansson, 2018; Carbonell et al., 2016). As described in the Results, evaluation of adaptive expertise tends to focus on evidence of transfer which often requires onerous designs (Mylopoulos et al., 2016). Evaluation approaches that are better suited to the unique contexts in which healthcare professions education takes place will need to be developed. Collecting evaluation evidence can occur in conjunction with implementation, as long as deliberate planning is done to pair implementation and evaluation (Hamza et al., 2020).
The second gap identified is the challenge of assessment of adaptive expertise in HPE programs. Workplace-based assessment of adaptive expertise requires prolonged engagement with students through frequent, formative, dynamic assessment (Orsino & Ng, 2019; Quirk & Chumley, 2018). Such an assessment system requires extensive data collection and analysis, and proper alignment with training curriculum (Sachdeva, 2020). Most healthcare education programs are not internally structured to allow for the prolonged and continuous relationships needed, and/or they are situated within healthcare system contexts that create potentially insurmountable barriers to such time-intensive assessment. Moreover, an increased appreciation of the contextual nature of problem solving potentially requires greater attention to the integration of competencies and context in learner assessment (Mylopoulos & Farhat, 2015; Mylopoulos & Woods, 2014; Orsino & Ng, 2019). Given that both learners and practitioners provide care in dynamic, team-based environments, Orsino and Ng (2019) advocate for the importance of collective competence and social awareness in assessments, and to not just think of assessment on the level of the individual.
This review has limitations. Due to the inclusion criteria and scope of the study, our findings only reflect literature exploring adaptive expertise specifically within HPE. While this strategy was essential for the goal of this review to establish a common understanding of adaptive expertise for frontline healthcare educators, it represents a subset of potential theorizations, applications, and strategies for the development of adaptive expertise in the wider education literature. Additionally, the search strategies for this scoping review were intentionally restrictive as far as the type of literature included. Our goal in carrying out this review was to develop a resource for frontline clinical educators that summarizes the primary literature about adaptive expertise, specifically how adaptive expertise is defined and how it may apply in the context of HPE contexts. As such, we included only publications in indexed peer-reviewed journals in English, which is a notable limitation to our data. Finally, reflecting the adoption of a subjectivist epistemology (Thomas et al., 2020), it is important to recognize the research team’s affiliation with family medicine and the influence this perspective may have had on the interpretation of results.
While this review is intended to serve as a general overview of definitions and applications of adaptive expertise in the HPE literature, it may also prompt thinking and discussion of potential future directions for research. An important next step in this research would be to examine adaptive expertise from a systems thinking approach, and expand the current analysis of the literature to consider the individual, organizational, and systems-level factors that influence or affect adaptive expertise. Another direction for future research would be to examine adaptive expertise through a specialist discipline lens; as mentioned in the Limitations section, all of the authors of this manuscript come from a generalist discipline background, which the authors acknowledge may have influenced the interpretation of the literature. Future research could also build upon this general overview by analyzing the adaptive expertise literature with a more critical lens, as this review reports on what has been published about adaptive expertise, but does not offer judgement of the approaches and assumptions within the individual publications that were included. Additionally, given the acknowledged narrowness of the search strategies for this study, future research should include an examination of the literature that includes a broader range of articles and more exhaustive search strategies.
Conclusions
Despite the challenges and limitations discussed above, the results of this scoping review highlight the potential for adaptive expertise as a guiding concept in HPE. Our goal was to consolidate information from across the HPE literature to help define adaptive expertise for frontline educators and present how the development of adaptive expertise can be supported through teaching and assessment. Although uncertainty is inevitable in the context of healthcare, it should not result in a diminished quality of patient care. Adaptive expertise can enable future healthcare professionals to continue to work and learn in these unfamiliar situations, while also promoting the efficient and effective response to well-established problems. As adaptive expertise continues to be adopted in HPE, this review will hopefully play a role in the deliberate pedagogical considerations towards training the next generation of expert healthcare professionals.
References
Alderson, D. (2010). Developing expertise in surgery. Medical Teacher, 32, 830–836.
Anthony, G., Hunter, J., & Hunter, R. (2015). Prospective teachers development of adaptive expertise. Teaching and Teacher Education, 49, 108–117.
Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8, 19–32.
Axelsson, A., & Jansson, A. A. (2018). On the Importance of Mental Time Frames. Journal of Applied Research in Memory and Cognition, 7(1), 51–59. https://doi.org/10.1016/j.jarmac.2017.12.004
Baroody, A. J. (2003). The development of adaptive expertise and flexibility: The integration of conceptual and procedural knowledge. The Development of Arithmetic Concepts and Skills: Constructive Adaptive Expertise, 1, 33.
Baroody, A. J., & Dowker, A. (2013). The development of arithmetic concepts and skills: Constructive adaptive expertise. Routledge.
Bekdache, G. N., Mylopoulos, M., Kulasegaram, K. M., & Windrim, R. (2019). Pedagogical strategies in teaching invasive prenatal procedures: A scoping review protocol. British Medical Journal Open, 9, e024629.
Bell, E., Horton, G., Blashki, G., & Seidel, B. M. (2012). Climate change: Could it help develop “adaptive expertise”? Advances in Health Sciences Education, 17, 211–224.
Betinol, E., Murphy, S., & Regehr, G. (2022). Exploring the development of adaptive expertise through the lens of threshold concepts. Medical Education. https://doi.org/10.1111/medu.14887
Biro, L., Song, K., & Nyhof-Young, J. (2021). First year medical student experiences with a clinical skills seminar emphasizing sexual and gender minority population complexity. Canadian Medical Education Journal, 12, e11–e20.
Bleakley, A. (2021). Re-visioning clinical reasoning, or stepping out from the skull. Medical Teacher, 43, 456–462.
Bradfield, Z., Hauck, Y., Kelly, M., & Duggan, R. (2019). Urgency to build a connection: Midwives’ experiences of being ‘with woman’ in a model where midwives are unknown. Midwifery, 69, 150–157.
Brannick, T., & Coghlan, D. (2007). In defense of being “native”: The case for insider academic research. Organizational Research Methods, 10(1), 59–74.
Bransford, J. (2007). Preparing people for rapidly changing environments. Journal of Engineering Education, 96(1), 1–3.
Bransford, J. D., Brown, A. L., & Cocking, R. R. (2000). How people learn (Vol. 11). National academy press.
Brehaut, J. C., & Eva, K. W. (2012). Building theories of knowledge translation interventions: Use the entire menu of constructs. Implementation Science, 7, 1–10.
Brown, L.L., & MacKinnon, R.J. (2016). Simulation for Rural Communities. In Comprehensive Healthcare Simulation: Pediatrics (pp. 299-313). Cham: Springer.
Butler, D. L., & Brydges, R. (2013). Learning in the health professions: What does self-regulation have to do with it? Medical Education, 47, 1057–1059.
Carbonell, K. & Dailey-Hebert, A. (2021). Routine expertise, adaptive expertise, and task and environmental influences. In M.L. Germain & R.S. Grenier (Eds.), Expertise at Work (pp. 39–56). Switzerland: Palgrave Macmillan.
Carbonell, K. B., Könings, K. D., Segers, M., & van Merriënboer, J. J. (2016). Measuring adaptive expertise: Development and validation of an instrument. European Journal of Work and Organizational Psychology, 25(2), 167–180.
Carbonell, K. B., Stalmeijer, R. E., Könings, K. D., Segers, M., & van Merriënboer, J. J. (2014). How experts deal with novel situations: A review of adaptive expertise. Educational Research Review, 12, 14–29.
Crawford, V.M., Schlager, M., Toyama, Y., Riel, M., & Vahey, P. (2005). Characterizing adaptive expertise in science teaching. In Annual meeting of the american educational research association, Montreal, Quebec, Canada (pp. 1–26).
Croskerry, P. (2018). Adaptive expertise in medical decision making. Medical Teacher, 40, 803–808.
Cutrer, W. B., Atkinson, H. G., Friedman, E., Deiorio, N., Gruppen, L. D., Dekhtyar, M., & Pusic, M. (2018). Exploring the characteristics and context that allow master adaptive learners to thrive. Medical Teacher, 40, 791–796.
Cutrer, W. B., & Ehrenfeld, J. M. (2017). Protocolization, standardization and the need for adaptive expertise in our medical systems. Journal of Medical Systems, 41, 1–2.
Cutrer, W. B., Miller, B., Pusic, M. V., Mejicano, G., Mangrulkar, R. S., Gruppen, L. D., Hawkins, R. E., Skochelak, S. E., & Moore, D. E., Jr. (2017). Fostering the development of master adaptive learners: A conceptual model to guide skill acquisition in medical education. Academic Medicine, 92, 70–75.
Daudt, H. M., van Mossel, C., & Scott, S. J. (2013). Enhancing the scoping study methodology: A large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Medical Research Methodology, 13, 1–9.
David, P. A., Maude-Griffin, R., & Rothwell, G. (1996). Learning by accident? Reductions in the risk of unplanned outages in US nuclear power plants after Three Mile Island. Journal of Risk and Uncertainty, 13(2), 175–198.
Dickinson, B. L., Gibson, K., VanDerKolk, K., Greene, J., Rosu, C. A., Navedo, D. D., Porter-Stransky, K. A., & Graves, L. E. (2020). “It is this very knowledge that makes us doctors”: An applied thematic analysis of how medical students perceive the relevance of biomedical science knowledge to clinical medicine. BMC Medical Education, 20, 1–11.
Earl, J. (2019). Innovative practice, clinical research, and the ethical advancement of medicine. The American Journal of Bioethics, 19(6), 7–18.
Edje, L., & Price, D. (2021). Training future family physicians to become Master Adaptive Learners. Family Medicine, 53, 559–566.
Feast, L., & Melles, G. (2010). Epistemological positions in design research: A brief review of the literature. In 2nd international conference on design education, University of New South Wales, Sydney, Australia.
Feltovich, P. J., Spiro, R. J., & Coulson, R. L. (1997). Issues of expert flexibility in contexts characterized by complexity and change. In P.J. Feltovich, K.M. Ford, & R.R. Hoffman (Eds.), Expertise in context: Human and machine (pp. 125–146). Menlo Park, USA: MIT Press.
Fu, B. (2019). Common ground: Frameworks for teaching improvisational ability in medical education. Teaching and Learning in Medicine, 31, 342–355.
Gegenfurtner, A., Lehtinen, E., Jarodzka, H., & Säljö, R. (2017). Effects of eye movement modeling examples on adaptive expertise in medical image diagnosis. Computers & Education, 113, 212–225.
Gisondi, M. A., Branzetti, J., Hopson, L. R., & Regan, L. (2021). Sustainable engaged accountable learners. AEM Education and Training, 5, 1–5.
Grenier, R. S. (2021). Identifying and Measuring Expertise in Organizations. In Expertise at Work (pp. 57–69). Cham: Palgrave Macmillan.
Grossnickle, K. E., Wiley, S., Zipple, J. T., & Kegerreis, S. (2019). Experiences of physical therapists working with women with chronic pelvic pain: A phenomenological qualitative study. Journal of Women’s Health Physical Therapy, 43, 61–72.
Guba, E. G., & Lincoln, Y. S. (1994). Competing paradigms in qualitative research. Handbook of Qualitative Research, 2(163–194), 105.
Gube, M., & Lajoie, S. (2020). Adaptive expertise and creative thinking: A synthetic review and implications for practice. Thinking Skills and Creativity, 35, 100630.
Guo, Y., Zhang, S., Ritter, A., & Man, H. (2013). A case study on a capsule robot in the gastrointestinal tract to teach robot programming and navigation. IEEE Transactions on Education, 57, 112–121.
Hamza, D. M., Ross, S., & Oandasan, I. (2020). Process and outcome evaluation of a CBME intervention guided by program theory. Journal of Evaluation in Clinical Practice, 26, 1096–1104.
Harris, T. R., Bransford, J. D., & Brophy, S. P. (2002). Roles for learning sciences and learning technologies in biomedical engineering education: A review of recent advances. Annual Review of Biomedical Engineering, 4(1), 29–48.
Hatano, G., & Inagaki, K. (1984). Two courses of expertise. Child Development and Education in Japan, 6, 27–36.
Hatano, G., & Oura, Y. (2003). Commentary: Reconceptualizing school learning using insight from expertise research. Educational Researcher, 32(8), 26–29.
Hatchimonji, J. S., Sikoutris, J., Smith, B. P., Vella, M. A., Dumas, R. P., Qasim, Z. A., Gallagher, J. J., Reilly, P. M., Raza, S. S., & Cannon, J. W. (2020). The REBOA dissipation curve: Training starts to wane at 6 months in the absence of clinical REBOA cases. Journal of Surgical Education, 77(6), 1598–1604.
Hutchinson, T., Snell, L. S., Wiseman, J., & Lubarksy, S. (2019). Applying adaptive expertise for students’ clinical decision making. Medical Education, 53, 1141–1142.
Hutton, R., Ward, P., Gore, J., Turner, P., Hoffman, R., Leggatt, A., & Conway, G. (2017). Developing adaptive expertise: A synthesis of literature and implications for training. In Proceedings of 13th International Conference on Naturalistic Decision Making (pp. 81–86).
Janssen, F., de Hullu, E., & Tigelaar, D. (2008). Positive experiences as input for reflection by student teachers. Teachers and Teaching: Theory and Practice, 14(2), 115–127.
Kawamura, A., Harris, I., Thomas, K., Mema, B., & Mylopoulos, M. (2020). Exploring how pediatric residents develop adaptive expertise in communication: The importance of “shifts” in understanding patient and family perspectives. Academic Medicine, 95, 1066–1072.
Kawamura, A., Mylopoulos, M., Orsino, A., Jimenez, E., & McNaughton, N. (2016). Promoting the development of adaptive expertise: Exploring a simulation model for sharing a diagnosis of autism with parents. Academic Medicine, 91, 1576–1581.
Kelly, M. A., Wicklum, S., Hubinette, M., & Power, L. (2021). The praxis of generalism in family medicine: Six concepts (6 C s) to inform teaching. Canadian Family Physician, 67, 786–788.
Kua, J., Lim, W. S., Teo, W., & Edwards, R. A. (2021). A scoping review of adaptive expertise in education. Medical Teacher, 43, 347–355.
Kvern, B. (2021). Generalism and the Medical Council of Canada’s licentiate decision: a white paper. Medical Council of Canada’s Assessment Innovation Taskforce
Lajoie, S. P., & Gube, M. (2018). Adaptive expertise in medical education: Accelerating learning trajectories by fostering self-regulated learning. Medical Teacher, 40, 809–812.
Lake, J. C., Tsui, E., Wu, J., Baker, M., & Kieffer, K. (2019). Case reports of diagnostic error: Liposarcoma mistaken for hematoma in an obese female with concurrent ipsilateral thrombosis on rivaroxaban. Diagnosis, 6, 301–305.
Lane, M. R., Lane, P. L., Rich, J., & Wheeling, B. (2015). Improving assessment: Creating a culture of assessment with a change management approach. Journal of Case Studies in Accreditation and Assessment, 4, 4–15.
Levac, D., Colquhoun, H., & O’Brien, K. K. (2010). Scoping studies: Advancing the methodology. Implementation Science, 5, 1–9.
Lin, X., Schwartz, D. L., & Hatano, G. (2005). Toward Teachers’ Adaptive Metacognition. Educational Psychologist, 40(4), 245–255. https://doi.org/10.1207/s15326985ep4004_6
Martimianakis, M. A., Mylopoulos, M., & Woods, N. N. (2020). Developing experts in health professions education research: Knowledge politics and adaptive expertise. Advances in Health Sciences Education, 25, 1127–1138.
Martin, L., & Schwartz, D. L. (2009). Prospective adaptation in the use of external representations. Cognition and Instruction, 27, 370–400.
McDiarmid, G. W., & Clevenger-Bright, M. (2008). Rethinking teacher capacity. Handbook of research on teacher education (pp. 134–156). Routledge.
McMullen, J., Hannula-Sormunen, M. M., Lehtinen, E., & Siegler, R. S. (2020). Distinguishing adaptive from routine expertise with rational number arithmetic. Learning and Instruction, 68, 101347.
Mees, A., Sinfield, D., Collins, D., & Collins, L. (2020). Adaptive expertise—a characteristic of expertise in outdoor instructors? Physical Education and Sport Pedagogy, 25(4), 423–438.
Mema, B., Mylopoulos, M., Tekian, A., & Park, Y. S. (2020). Using learning curves to identify and explain growth patterns of learners in bronchoscopy simulation: A mixed-methods study. Academic Medicine, 95, 1921–1928.
Metz, M., Kavanaugh, S. S., & Hauser, M. (2020). Developing adaptive expertise in facilitating text-based discussions: Attending to generalities and novelty. English Education, 52(4), 310–334.
Mukherjee, S., Meacock, J., & Chumas, P. (2019). Is surgery more about doing than thinking? British Journal of Hospital Medicine, 80, 605–608.
Mylopoulos, M., Borschel, D. T., O’Brien, T., Martimianakis, S., & Woods, N. N. (2017). Exploring integration in action: Competencies as building blocks of expertise. Academic Medicine, 92, 1794–1799.
Mylopoulos, M., Brydges, R., Woods, N. N., Manzone, J., & Schwartz, D. L. (2016). Preparation for future learning: A missing competency in health professions education? Medical Education, 50, 115–123.
Mylopoulos, M., & Farhat, W. (2015). “I can do better”: Exploring purposeful improvement in daily clinical work. Advances in Health Sciences Education, 20, 371–383.
Mylopoulos, M., Kulasegaram, K., & Woods, N. N. (2018). Developing the experts we need: Fostering adaptive expertise through education. Journal of Evaluation in Clinical Practice, 24, 674–677.
Mylopoulos, M., & Regehr, G. (2007). Cognitive metaphors of expertise and knowledge: Prospects and limitations for medical education. Medical Education, 41, 1159–1165.
Mylopoulos, M., & Regehr, G. (2009). How student models of expertise and innovation impact the development of adaptive expertise in medicine. Medical Education, 43, 127–132.
Mylopoulos, M., & Scardamalia, M. (2008). Doctors’ perspectives on their innovations in daily practice: Implications for knowledge building in health care. Medical Education, 42, 975–981.
Mylopoulos, M., Steenhof, N., Kaushal, A., & Woods, N. N. (2018). Twelve tips for designing curricula that support the development of adaptive expertise. Medical Teacher, 40, 850–854.
Mylopoulos, M., & Woods, N. (2014). Preparing medical students for future learning using basic science instruction. Medical Education, 48, 667–673.
Mylopoulos, M., & Woods, N. N. (2009). Having our cake and eating it too: Seeking the best of both worlds in expertise research. Medical Education, 43, 406–413.
Mylopoulos, M., & Woods, N. N. (2017). When I say… adaptive expertise. Medical Education, 51, 685–686.
Newton, K. J., Star, J. R., & Lynch, K. (2010). Understanding the development of flexibility in struggling algebra students. Mathematical Thinking and Learning, 12(4), 282–305.
Orsino, A., & Ng, S. (2019). Can adaptive expertise, reflective practice, and activity theory help achieve systems-based practice and collective competence? Canadian Medical Education Journal, 10, e55–e60.
Peterson, J., Pearce, P. F., Ferguson, L. A., & Langford, C. A. (2017). Understanding scoping reviews: Definition, purpose, and process. Journal of the American Association of Nurse Practitioners, 29, 12–16.
Pusic, M. V., Santen, S. A., Dekhtyar, M., Poncelet, A. N., Roberts, N. K., Wilson-Delfosse, A. L., & Cutrer, W. B. (2018). Learning to balance efficiency and innovation for optimal adaptive expertise. Medical Teacher, 40, 820–827.
Pusic, M. V., Santen, S. A., Dekhtyar, M., Poncelet, A. N., Roberts, N. K., Wilson-Delfosse, A. L., & Cutrer, W. B. (2018). Learning to balance efficiency and innovation for optimal adaptive expertise. Medical Teacher, 40(8), 820–827.
Quirk, M., & Chumley, H. (2018). The adaptive medical curriculum: A model for continuous improvement. Medical Teacher, 40, 786–790.
Ravitz, P., Berkhout, S., Lawson, A., Kay, T., & Meikle, S. (2019). Integrating evidence-supported psychotherapy principles in mental health case management: A capacity-building pilot. The Canadian Journal of Psychiatry, 64, 855–862.
Reed, F. I. (2018). Exploring the relationship between innovation in nursing education and clinical practice. Dissertation, State University of New York at Albany
Regan, L., Hopson, L. R., Gisondi, M. A., & Branzetti, J. (2019). Learning to learn: A qualitative study to uncover strategies used by Master Adaptive Learners in the planning of learning. Medical Teacher, 41, 1252–1262.
Regehr, G. (1994). Chickens and children do not an expert make. Academic Medicine, 69, 970–971.
Rose, N. (2007). Review of the Cambridge handbook of science. The British Journal of Psychiatry, 190, 279.
Royce, C. S., Hayes, M. M., & Schwartzstein, R. M. (2019). Teaching critical thinking: A case for instruction in cognitive biases to reduce diagnostic errors and improve patient safety. Academic Medicine, 94, 187–194.
Sachdeva, A. K. (2020). Acquiring and maintaining lifelong expertise in surgery. Surgery, 167, 787–792.
Salas, E., Wilson, K. A., Murphy, C. E., King, H., & Salisbury, M. (2008). Communicating, coordinating, and cooperating when lives depend on it: Tips for teamwork. The Joint Commission Journal on Quality and Patient Safety, 34, 333–341.
Schneider, M. & Stern, E. (2010). The cognitive perspective on learning: Ten cornerstone findings. In Organisation for Economic Co-Operation and Development (OECD) (Eds.), The nature of learning: Using research to inspire practice (pp. 69–90), Paris: OECD.
Schwartz, D. L., Bransford, J. D., & Sears, D. (2005). Efficiency and innovation in transfer. Transfer of Learning from a Modern Multidisciplinary Perspective, 3, 1–51.
Skjerve, A. B., & Holmgren, L. (2018). Training licensed nuclear power plant operators for handling unforeseen accident events: Social awareness and development and assessment of a training approach based on adaptive expertise theory by social education purpose. Arts Social Sciences Journal, 9, 385. https://doi.org/10.4172/2151-6200.1000385
Sockalingam, S., Chaudhary, Z. K., Barnett, R., Lazor, J., & Mylopoulos, M. (2020). Developing a framework of integrated competencies for adaptive expertise in integrated physical and mental health care. Teaching and Learning in Medicine, 32, 159–167.
Sockalingam, S., Mulsant, B. H., & Mylopoulos, M. (2016). Beyond integrated care competencies: The imperative for adaptive expertise. General Hospital Psychiatry, 43, 30–31.
Sockalingam, S., Rajaratnam, T., Zhou, C., Serhal, E., Crawford, A., & Mylopoulos, M. (2021). Building mental health capacity: Exploring the role of adaptive expertise in the ECHO virtual learning model. Journal of Continuing Education in the Health Professions, 41, 104–110.
Soni, S. M., Giboney, P., & Yee, H. F. (2016). Development and implementation of expected practices to reduce inappropriate variations in clinical practice. JAMA, 315(20), 2163–2164.
Soslau, E. (2012). Opportunities to develop adaptive teaching expertise during supervisory conferences. Teaching and Teacher Education, 28(5), 768–779.
Spiro, R. J. (1988). Cognitive flexibility theory: Advanced knowledge acquisition in ill-structured domains. Center for the Study of Reading Technical Report; No. 441.
Steenhof, N. (2020). Adaptive expertise in continuing pharmacy professional development. Pharmacy, 8, 21.
Steenhof, N., Woods, N. N., & Mylopoulos, M. (2020). Exploring why we learn from productive failure: Insights from the cognitive and learning sciences. Advances in Health Sciences Education, 25, 1099–1106.
Steenhof, N., Woods, N. N., Van Gerven, P. W., & Mylopoulos, M. (2019). Productive failure as an instructional approach to promote future learning. Advances in Health Sciences Education, 24, 739–749.
Steinert, Y., Irby, D. M., & Dolmans, D. (2021). Reframing faculty development practice and research through the lens of adaptive expertise. Medical Teacher, 43, 1–3.
Thimbleby, H. (2013). Technology and the future of healthcare. Journal of Public Health Research, 2, e28.
Thomas, A., Lubarsky, S., Varpio, L., Durning, S. J., & Young, M. E. (2020). Scoping reviews in health professions education: Challenges, considerations and lessons learned about epistemology and methodology. Advances in Health Sciences Education, 25, 989–1002.
Tynjälä, P., Slotte, V., Nieminen, J., Lonka, K., & Olkinuora, E. (2006). From university to working life: Graduates’ workplace skills in practice. Higher Education and Working Life: Collaborations, Confrontations and Challenges, 73–88.
Valbuena, G., O’Brien, B., Ten Cate, O., & O’Sullivan, P. (2019). Inquiry in the medical curriculum: A pedagogical conundrum and a proposed solution. Academic Medicine, 94, 804–808.
Vanasupa, L., Stolk, J., & Harding, T. (2010). Application of self-determination and self-regulation theories to course design: Planting the seeds for adaptive expertise. International Journal of Engineering Education, 26(4), 914.
Varpio, L., Schryer, C. F., & Lingard, L. (2009). Routine and adaptive expert strategies for resolving ICT mediated communication problems in the team setting. Medical Education, 43, 680–687.
Verschaffel, L., Luwel, K., Torbeyns, J., & Van Dooren, W. (2009). Conceptualizing, investigating, and enhancing adaptive expertise in elementary mathematics education. European Journal of Psychology of Education., 24(3), 335–359.
Wheeler, D. S., Geis, G., Mack, E. H., LeMaster, T., & Patterson, M. D. (2013). High-reliability emergency response teams in the hospital: Improving quality and safety using in situ simulation training. BMJ Quality & Safety, 22(6), 507–514.
Wineburg, S. (1998). Reading Abraham Lincoln: An expert/expert study in the interpretation of historical texts. Cognitive Science, 22(3), 319–346.
Winne, P. H. (2017). Cognition and metacognition within self-regulated learning. In Handbook of self-regulation of learning and performance (pp. 36–48). Routledge.
Woodruff, J. N. (2019). Accounting for complexity in medical education: A model of adaptive behaviour in medicine. Medical Education, 53(9), 861–873.
Woods, N. N., Mylopoulos, M., Nutik, M., & Freeman, R. (2021). Defining the specialist generalist: The imperative for adaptive expertise in family medicine. Canadian Family Physician, 67, 321–322.
Zimmerman, B. J. (2002). Becoming a self-regulated learner: An overview. Theory into Practice, 41, 64–70.
Acknowledgements
Funding from the College of Family Physicians of Canada supported the development of the report that this review is based on. The authors would like to thank Tatjana Lozanovska for all her help and support.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix 1
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Cupido, N., Ross, S., Lawrence, K. et al. Making sense of adaptive expertise for frontline clinical educators: a scoping review of definitions and strategies. Adv in Health Sci Educ 27, 1213–1243 (2022). https://doi.org/10.1007/s10459-022-10176-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10459-022-10176-w