
Abstract
We tested the null hypotheses that neither age, gender nor muscle pre-cocontraction state affect the latencies of changes in upper extremity kinematics or elbow muscle activity following an impulsive force to the hand. Thirty-eight healthy young and older adult volunteers lay prone on an apparatus with shoulders flexed 75° and arms slightly flexed. The non-dominant hand was subjected to three trials of impulsive loading with arm muscles precontracted to 25, 50, or 75% of maximum pre-cocontraction levels. Limb kinematic data and upper extremity electromyographic (EMG) activity were acquired. The results showed that pre-cocontraction muscle level (p < 0.001) and gender (p < 0.05 for wrist and shoulder) affected joint displacement onset times and age affected EMG onset times (p < 0.05). The peak applied force (F 1) occurred a mean (± SD) 27 (± 2) ms after impact. The latencies for the wrist, elbow, and shoulder displacements were 21 ± 3, 29 ± 5, and 34 ± 7 ms, respectively. Because the latencies for elbow flexion and lateral triceps EMG were 23 ± 5 and 84 ± 8 ms, respectively, muscle pre-activation rather than stretch reflexes prevent arm buckling under impulsive end loads.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The upper extremities are typically the first line of defense to protect the head and torso while bracing for a frontal car crash14 or arresting a fall to the ground.10 To prevent a slightly flexed limb from buckling under an impulsive load applied to the hand,9,11,18 the arm muscles are usually precontracted to brace the arm for impact.10,19,20,29 Muscle pre-cocontraction may be required4 because the impulsive ground reaction force on the hand peaks rises so quickly: within a few tens of milliseconds at the hand, and within one hundred milliseconds for the proximal extremity.9,10,12,16 Impulsive loads can reach 2–3 times body weight (BW) for a fall from even half standing height9,20 and 1–4 kN for a fall from standing height,12 enough to cause wrist fracture on a hard surface.15
If muscle pre-cocontraction is not used, and one instead has to rely upon neuromuscular reflexes to increase muscular resistance to arm buckling after onset of the impulsive load to the hand, it is not known whether the muscle reflexes are sufficiently rapid that they can effectively increase muscle stiffness before the muscle is forcibly stretched by limb flexion under gravitational and inertial loading. Furthermore, it is not known how long it takes before the elbow begins to flex when an arm is end-loaded. Finally, it is not known whether, once the elbow flexion starts, the triceps muscle reflex is rapid enough to increase muscle resistance to stretch before the elbow flexion phase is complete. One of the goals of this study is to find answers to these questions.
It is known that maximally tensing a striated muscle can increase its stiffness and damping by 50%,2 so increasing triceps muscle tension to half maximal values should increase its tensile stiffness by about 25%. To voluntarily increase striated muscle force by half-maximal values “as fast as possible” took 74 ms in young females, 87 ms in older females, 92 ms in young males, and 95 ms in older males.28 So, it takes approximately 90 ms to increase muscle tension by half-maximal values, and muscle stiffness by 25%.
The age and sex of an individual can also affect the time for propagation of the impulsive force along a limb, because they affect the length and mass distribution of the upper extremity. For example, young women typically weigh 17% less than young men and have 8% shorter stature. In addition, young women and men weigh 9 and 5% less than older women and men, respectively.21 These systematic differences might affect propagation latencies since an impulsive force will take more time to propagate the length of a longer male limb segment than a shorter female limb segment. And larger segmental masses can affect the momentum transfers from one arm segment to the next. For example, Wong et al. found a positive relationship between the longitudinal stress wave velocity and higher mass per unit length of the human bones.32 Finally, in terms of reflex latencies, nerve conduction velocity is known to be affected by age; for example, above 60 years the conduction velocity decreases by 1.5% per decade.7,22,30
The speed of a compressive stress along a human long bone in vivo has been reported as 351 and 266 ms−1 for male and female tibia at the medial malleolus32; these value have been corroborated by others on the anteromedial aspect of the tibia.6,13 We might guess that the axial acceleration of the soft tissues (i.e., muscle, fat, and skin) overlying a bone would lag that of the bone because of their compliant coupling to the bone.25 Hence a compressive stress wave traveling 0.5 m from the hand to the triceps’ bony origin will take approximately 1.5 ms. Since, muscle spindles are exquisitely sensitive to stretch3 and vibration,5 it is therefore theoretically possible that a muscle spindle in the triceps muscle could begin to sense triceps muscle stretch 2 ms after the onset of the ground reaction force,22 even though no elbow flexion has yet occurred. The latency of the monosynaptic reflex is mainly governed by the maximum conduction velocity, 50 ms−1,22,26,30 of the largest nerve axons in the nerve to triceps. So, the monosynaptic reflex latency for triceps should take about 20 ms for a 1 m long reflex arc length. This type of non-traditional monosynaptic reflex, which could be initiated by the proximal axial acceleration of the bony origin of the triceps muscle in the direction of the applied end-load to the limb, could potentially be significantly more rapid than the onset of traditional mono- and polysynaptic reflexes related to elbow flexion. The latter have been measured by Dietz et al. in a fall arrest to be ~25 and ~50 ms, respectively.12
The goal of this paper, therefore, was to test the primary (null) hypotheses that neither gender, age, nor level of pre-cocontraction affect the time it takes an impulsive force to propagate proximally along the upper extremity in healthy adults. The secondary hypothesis was that this propagation time is always shorter than the latency of the triceps EMG response to elbow flexion caused by impulsive loading. To help interpret the results, a forward dynamics model was used to explore how the magnitude of hand preload affects impulse propagation times along the upper extremity.
Methods
Ten healthy young males of mean (± SD) age of 25.5 (± 2.7) years, eight healthy young females of 24.5 (± 3.1) years, 9 healthy old males of 69.4 (± 3.4) years, and 11 healthy old females of 67.7 (± 2.4) years gave written informed consent to participate in the study, which was approved by the institutional review board. Mean height and mass for the young males were 1.795 (± 0.077) m and 75.88 (± 6.74) kg, for the young females were 1.683 (± 0.060) m and 60.96 (± 7.67) kg, respectively, and for the old males were 1.734 (± 0.085) m and 74.73 (± 11.83) kg and for the old females were 1.623 (± 0.039) m and 59.20 (± 7.01) kg, respectively. Subjects were screened by telephone to exclude any chronic illnesses or upper extremity fractures or sprains within the previous year.
An Optotrak Certus camera (Northern Digital, Inc., Waterloo, Canada) was used to measure the displacements of 15 arm, shoulder, and neck optoelectronic markers taped to the skin over wrist, elbow, and shoulder joint bony landmarks (Fig. 1). We placed quadruple surface electromyographic (EMG) electrodes (Trigno™ Wireless System, Delsys, Inc., Boston, MA, USA) on the skin over the mid belly of selected arm muscles to measure non-dominant arm muscle activity. Each Trigno™ electrode also contained a triaxial accelerometer from which signals were recorded. Each subject was asked to warm up his/her arm muscles by doing various stretches and several push-ups. We then measured subject’s resting and maximum voluntary pre-cocontraction (MVC) EMG levels of the triceps brachii (lateral head) muscles during elbow and shoulder flexion, extension and ab- and adduction by pulling up or pushing down on an handle attached to a vertical cable in series with an uniaxial force transducer (TLL-500, Transducer Techniques, Temecula, CA, USA).

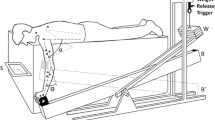
Apparatus for the impulsive end loading test of a human upper extremity. Each subject lay on a padded table with left hand positioned on a force transducer (F). The subject was asked to concentrate on monitoring EMG biofeedback from his/her elbow extensor muscle activity on a display screen (S) and maintaining it at a certain level of effort. A weight (W) of 23 kgf was released onto the end of the lever-arm (B) by a remote trigger, applying an impulsive force to the wrist (at the other end of lever arm) causing elbow flexion and shoulder adduction (the end of the lever-arm position being changed from B to B′). Alpha (α) and theta (θ) represent shoulder and elbow flexion angles, respectively
Next, each subject was asked to lie prone on a table with the base of the left hand “lightly touching” a 6-axis force transducer (MC3A-1000, AMTI, Newton, MA, USA) mounted at one end of a 76 mm × 152 mm × 2,032 mm hollow aluminum beam having a rectangular cross-sectional shape and wall thickness 6.35 mm (Fig. 1). The preload on the transducer was not controlled. The beam was pivoted at its midpoint about a fulcrum formed from a pair of collinear needle bearings and mounted on an axle in the horizontal plane.
The initial flexion angle of the elbow was adjusted to 25°. When ready, the subject was asked to hold his/her hand “lightly” in contact with the force transducer and to concentrate on monitoring EMG biofeedback from his/her lateral head of the triceps muscle activity on a display screen and maintaining triceps activity either at rest, or 25, 50, and 75% MVC values from the main agonist muscle. A weight of 23 kgf was released (see Fig. 1) from a fixed height of 720 mm to impact the top surface of the other end of the beam, thence applying an upward impulsive force to the wrist via the force transducer, thereby causing elbow flexion, and shoulder adduction and trunk extension. The subject was instructed “not to intervene” before, during and after the weight drop. For example, if the trial was conducted with 75% MVC, the subject was instructed to contract the target muscle steadily at 75% of MVC during the test. At least three trials were conducted at each of the three levels of muscle activation, and these were presented in randomized order.
3-D kinematics data were measured at 280 Hz from 15 infrared-emitting diodes adhered to the skin with double-sided tape. The kinematics and force data were digitally low-pass filtered (MATLAB, The MathWorks, 4th order Butterworth) with cutoff frequencies of 30 and 300 Hz.9,20 Surface electromyography (EMG) data were collected at 4 kHz. A band-pass 6th order filter with breakpoints at 40 Hz and 500 Hz was used to attenuate any movement artifacts in the EMG signal. Then, the EMG data were rectified and digitally low-pass 4th order Butterworth filtered with a cutoff frequency of 30 Hz.12,27 EMG data were normalized by maximum MVC values. The muscle pre-cocontraction state for each trial was determined as the mean value of a 100 ms time window 50 ms before the weight drop.
The onset time of displacement of each joint marker was calculated using MATLAB routines as the intersection of two linearly extrapolated lines: the baseline level line, defined from 100 ms before the impact, and the slope of the signal for 150 ms following the impact.27 Similarly, the rectified EMG onset time of the target agonist muscle (i.e., lateral triceps brachii) was determined by a MATLAB routine when it exceeded the threshold at the mean plus two standard deviation (SD) value. Peak force values were identified using a MATLAB moving window routine to find local maximum and minimum values.
Typical temporal measurements for each signal in a subject are shown in Fig. 2. The red circles in the plots (a), (b), (c), and (d) show the onset of each joint marker displacement: t a was defined as the onset of wrist marker displacement; t b, the onset of elbow rotation (θ elbow); t c, the onset of elbow linear displacement; and t d, the onset of the shoulder displacement. In the force graph (e), the red circles represent; t 0, the onset (0 ms) of the impulsive force (F 0); t 1, the latency of the first peak in that force signal (F 1); t 2, the latency of second peak force (F 2); t 3, the latency of the first minimum (F 3) in the force trace between F 1 and F 2. The bottom plot (f) shows raw (blue dotted line) and the filtered (magenta solid line) EMG data with the onset time indicated by the solid vertical red line, t e.

Temporal plots for one trial in Subject OFZC showing the onset times of landmark movement (a–d); measured impulsive force (e); and EMG in the lateral triceps brachii (f). t 0 represents the onset (0 ms) of the impulsive force (F 0); t 1, the latency of the first peak in that force signal (F 1, 27 ms); t 2, the latency of second peak force (F 2, 120 ms); t 3, the latency of the first minimum (F 3, 63 ms) in the force trace between F 1 and F 2; t a, the onset of wrist marker displacement (21 ms); t b, the onset of elbow rotation (θ elbow, 23 ms); t c, the onset of elbow linear displacement (29 ms); and t d, the onset of the shoulder displacement (34 ms). The bottom plot (f) shows raw (blue dotted line) and the filtered (magenta solid line) EMG data with the onset time indicated by the solid vertical red line, t e (84 ms)
Data Analyses
Descriptive statistics were calculated for peak force, joint marker and EMG onset times. A repeated measures analysis of variance (rm-ANOVA) was used to test the null hypothesis for age, gender, and three different muscle pre-cocontraction levels using SAS 9.3 software. An analysis of covariance (ANCOVA) was used to examine the relationship between preload and pre-cocontraction and their effects on results. A p value of less than 0.05 was considered statistically significant for the three main effects (primary hypothesis). A Bonferoni correction was used for the interactions.
Forward Dynamics Model
To examine the effect of hand preload on the results, forward dynamics calculations of upper limb segment kinetics were analyzed using MD Adams™ (MSC. Software Corporation, version 2010). A 3-D, sagittally symmetric, four-link (including hand, forearm, upper arm, and clavicle), lumped parameter, musculoskeletal representation of a 50th percentile male upper extremity was modeled. Arm segments were assumed to be connected by two frictionless revolute joints representing wrist and elbow joints and by two frictionless spherical joints at shoulder and sternoclavicular joints. Segment anthropometric, mass, and inertial properties were assigned based upon the literature.31 The model arm muscles were represented by a torsional spring and damper in parallel at the elbow, and again at the shoulder and sternoclavicular joints, with average tensile stiffness and damping coefficients for either 25, 50, or 75% MVC levels taken from the literature.18 The model hand-wrist was loaded in a proximal direction with a force time history and peak values equal to the average values measured in each of three blocks of impulsive loading tests. Model kinematic responses were simulated based on preloads of 0, 50, and 100 N, and pre-cocontraction levels of either 25, 50, and 75% MVC. For each test condition, the mean model-predicted onset times of the linear displacements at each joint and angular displacement at the elbow were calculated to examine the effect of hand preload on impulse transmission times along the extremity.
Results
A typical temporal history for each signal in a subject is shown in Fig. 2. Across all subjects, the peak applied force (F 1) occurred a mean (± SD) 27 (± 2) ms after the onset of the applied force (t 1 in Table 1). Similarly, the onset times for displacements of the wrist, elbow, and shoulder markers were 21 (± 3) ms, 29 (± 5) ms, and 34 (± 7) ms, respectively (t a, t c, and t d in Table 1). The corresponding onset times for elbow flexion and lateral triceps brachii muscle activity were 23 (± 5) and 84 (± 8) ms, respectively (t b and t e in Table 1). The second peak (F 2) was reached at 120 (± 9) ms and the minimum value (F 3) at 63 (± 5) ms, respectively (t 2 and t 3 in Table 1).
In terms of the hypothesis testing, Table 2 shows the main effect of age, gender, and pre-cocontraction level and the interaction of the onset times of each joint and the latencies of the force signals, and EMG onset time in the lateral triceps brachii. The ANOVA (Table 2) demonstrated a significant gender effect, age effect, and pre-cocontraction level effect on onset times. Age affected EMG onset time, gender affected wrist and shoulder displacement onset times, and pre-cocontraction level significantly affected all kinematic onset times, as well as the time to first and second peak applied force. While the higher pre-cocontraction level was associated with a more rapid onset time for each joint marker, the lower pre-cocontraction level was associated with a shorter time to reach the first peak force (F 1). Although the wrist marker in males started to displace earlier, the latencies of propagation proximal to the shoulder marker was longer than in the females. Young adults had significantly shorter EMG onset times than older adults (p < 0.05).
Average values of the initial force (F 0), the first peak force (F 1), and the second peak force (F 2) were higher in young and male subjects, as well as in higher pre-cocontraction level condition, than in old or female subjects, and in the lower pre-cocontraction level condition (Table 3). The muscle pre-cocontraction level was found to have a significant effect on the onset times of arm joint displacements in the current study. The relationship between the pre-cocontraction level and the preload, which was represented as F 0 (the initial force), is shown in Tables 3 and 4. The other two peak forces (F 1, F 2) including F 0 were significantly affected by the pre-cocontraction level (p < 0.0001).
Since subjects had some difficulty in maintaining steady cocontraction levels prior to loading, we analyzed the mean (± SD) RMS EMG activity at the 25, 50, and 75% cocontraction levels over the last 100 ms prior to impact. These values were 0.055 (± 0.015) mV, 0.077 (± 0.021) mV, and 0.101 (± 0.035) mV, respectively.
The increase in elbow flexion angle in the first 150 ms following impact averaged (± SD) 21.1 (± 5.4)° and 27.1 (± 6.4)° in the young and old, respectively; 20.1 (± 4.0)° and 28.1 (± 6.4)° in the males and females, respectively; and 25.1 (± 6.1), 24.1 (± 6.8), and 23.5 (± 7.0) for the 25, 50, and 75% MVC trials, respectively.
The forward dynamic upper extremity model predicted that increasing muscle stiffness had less of an effect on joint displacement onset times than increasing the preload on the hand. For example, the model joint displacement onset times (t a − t d) were shortened by 5% when the pre-cocontraction level was increased from 25 to 75%MVC, but shortened by an average of 15% when the preload was increased from 0 to 100 N (Table 5). Pre-cocontraction was predicted to have a larger effect on the increase in elbow angle than preload in this model.
Discussion
This study provides the first experimental evidence for the effect of age, sex, and muscle pre-cocontraction level on the kinematics of the upper extremity loaded under large impulsive end-loads. The main hypotheses were rejected in that the ANOVA (Table 2) demonstrated a significant gender effect, age effect, and pre-cocontraction level effect on onset times. The secondary hypothesis was supported in that even the longest latency to onset of the shoulder marker in any subject was approximately 40 ms, with the onsets of displacements at the wrist and elbow being shorter (Table 1), and all these latencies being substantially shorter than the mean EMG onset time of the lateral triceps brachii measured at 84 ms (Fig. 3).

Illustration of mean onset times of landmark movement and EMG onset time across all subjects. The red circles indicate the onset of linear displacements at the wrist, elbow, and shoulder joints. The green triangle represents the onset of rotation at the elbow joint. The blue rectangle denotes onset of lateral triceps brachii EMG signal. Measures of data variability are provided in Table 1
Although several significant interactions were found (i.e., age × gender, age × pre-cocontraction, or gender × pre-cocontraction, Table 2) they do not seriously affect the main conclusions that gender, age and precontraction level affect onset times.
As far as the secondary hypothesis is concerned, the results suggest that the elbow began to flex 6 ms before the origin of the triceps started to displace, so the triceps EMG response at 84 ms was most likely triggered by arm flexion rather than axial movement of the bony origin of the triceps muscle in the direction of the impulsive force, as discussed in “Introduction”. The results also suggest that there is not sufficient time for longer loop neural reflexes to modulate arm buckling resistance before the 84 ms onset of triceps stretch. This latter was either caused by induced elbow flexion (onset of 23 ms) or onset of the proximal displacement of the origin of the triceps muscle near the acromion marker (34 ms). Given the ~90 ms Thelen et al. 28 found it takes to increase tension, and therefore tensile stiffness, by half-maximal values (see “Introduction”), it is highly unlikely that any muscle reflex can significantly increase the tensile stiffness of the triceps before it is forcibly stretched at 23 ms. This is true even if the onset of the impulsive force was so rapid that it triggered a flexural stress wave along the bones of the upper arm to set up longitudinal vibrations that initiated a stretch reflex in the triceps muscle.
The 84 ms onset of lateral triceps brachii muscle activity after impact is consistent with empirical studies conducted over the past 60 years (for review, see Pruszynski and Scott).24 For example, typical elbow muscle responses following stretch yield an initial peak reflex response 20–50 ms after the perturbation (the ‘short-latency response’)23 based on a monosynaptic contribution. A second peak, occurring 50–100 ms after the perturbation, is termed the ‘long-latency stretch response’ based on polysynaptic contributions. Our 84 ms triceps response therefore belongs in this latter category. The final myoelectric burst, called the ‘voluntary response’, occurs after 100 ms and involves feedback control processes (‘relatively slow motor response’).17 These were not considered in the present study.
The forward dynamic simulation model predictions (Table 5) suggested that the preload applied by the hand to the force transducer before it started to accelerate likely affects the displacement onset times at each joint. The zero preload condition (0 N) approximated the in vivo situations of arresting a fall to the ground,10 while larger preloads represent bracing for a frontal car crash.14 The forward dynamic model predictions were verified by comparing the predicted joint displacement onset times for the range of hand preload conditions with the experimental results (c.f., Tables 1, 5). The experimental results showed that the preload (F 0) was significantly affected by the pre-cocontraction level and gender (Table 4) so one cannot separate the effects of the higher pre-cocontraction levels from those caused by the larger preloads. But the forward dynamics model allows one to separate those effects (Table 5). In addition, the ANCOVA results showed that the effect of a preload on arm kinematics during the 25% pre-cocontraction level was significantly greater than that at 50 and 70% levels.
In general, the higher the arm muscle pre-cocontraction level, the faster the stress wave can travel through the stiffer muscles overlying the bone,25 and this explains the shorter onset time of the wrist, elbow and shoulder joint displacements at higher pre-cocontraction levels. A confounder was that the higher pre-cocontraction levels were also associated with high preloads on the stationary hand/wrist of a subject. However in our experiment, the presence of that preload was a safety measure to prevent the beam and force transducer accelerating so as to cause an excessive, and therefore potentially unsafe,1 impact force on the stationary hand/wrist of an older subject.
Limitations of our methods include the possible presence of movement artifact in the triceps muscle activity responses. We noticed a large positive cross-correlation coefficient, ranging from 0.68 to 0.98, between the EMG signal and the measured linear accelerations of the wireless EMG electrode/amplifier over the first 84 ms post-impact. The linear accelerations were measured from the onboard 3-axis Trigno™ accelerometers during the 40 ms post-impact time frame (Fig. 4). The presence of motion artifact on the Trigno™ wireless system is surprising given the double differential design of the preamplifier which should have attenuated signals common to the two pairs of electrodes. We cannot exclude the possibility that a monosynaptic stretch reflex might have increased EMG signal in the 25 ms after impact, but given that a maximum EMG pre-cocontraction takes 88 ms27 to peak and that it takes 90 ms for muscle to reach 50% MVC,28 it is unlikely that monosynaptic reflexes could have had much mechanical effect prior to 80 ms.

Temporal plot for one trial in Subject OMYB showing the EMG signal (in red line) of the wireless EMG sensor and the acceleration (RMS in blue dashed line) of the 3-axis accelerometer built into the wireless EMG sensor. Correlation coefficient was calculated during the interval from 10 to 50 ms after the impact (F 0)
A second limitation was the fact that some subjects had difficulty using biofeedback to maintain a constant pre-cocontraction feedback level. This likely increased the variability observed in the pre-impact triceps pre-cocontraction level.
A third limitation was the lack of data on the onset of shoulder extension or abduction rotation which would have informed the question of whether shoulder flexor and/or adductor muscle reflexes are rapid enough to change shoulder muscle stiffness before those muscles are stretched. However, given the onset of shoulder motion at 34 ms, the present results suggest this is unlikely, even if the muscle reflex latencies for triceps have shorter reflex arcs.
A fourth limitation related to the relatively modest impulsive force induced by the drop-weight-and-rotating beam apparatus which amounted to approximately 0.25* BW (Table 3). While it sufficed to impart a realistic “jolt” to accelerate both arm segments and torso upwards by approximately 10 cm, it is certainly less than the more than 1*BW force that occurs during falls onto a hard surface (see review in “Introduction”). However, subject safety was paramount in these experiments involving older adults, especially since we did not inform subjects of the exact time of release; they could not anticipate the timing of the impact as in a real fall.9,11,18,29 This means that the neural ‘set’ and reticular activation of the motor control system might have been less in these subjects than during a real fall arrest. For example, the vestibular system was inactivated by the stimulus, there was no visual stimulus from an on-rushing surface to clue one into when impact would occur, and there was imprecise anticipation of when ‘ground contact’ would occur.
Our experiment helps one consider upper extremity responses in the act of bracing oneself against steering wheel or the dashboard of a car before a frontal crash whose exact timing is uncertain. Our results on the latencies of the kinematic movements are conservative since in real falls Dietz et al. 12 have shown latencies half (i.e., 10–20 ms) those measured in this experiment (i.e., 27 ms, Fig. 2e). Thus the longer latency to a lower peak loading we used in this paper is more reflective of landing on or striking a soft rather than a hard surface.8 Hence, in a real fall, there would be even less time for reflexes to increase muscle forces than in the present experiment.
The most important result from this study is the marked effect of pre-cocontraction level and gender on the propagation of an impulse along the upper extremity. Furthermore, the “preflex”,4 resulting from forced stretch of pre-activated muscle, with its increased stiffness and viscosity property states, is more important than reflexes in dictating the response of an arm to an impulsive end load. We conclude that there is insufficient time for muscle reflexes to significantly increase muscle resistance to arm buckling when using the arm to protect the torso and head from impact. The present results suggest that if this is true for a fall onto a soft surface, then it is most certainly true for a fall onto a hard surface because there is even less time for the reflexes to have any meaningful effect.
References
Augat, P., H. Iida, Y. Jiang, E. Diao, and H. K. Genant. Distal radius fractures: mechanisms of injury and strength prediction by bone mineral assessment. J. Orthop. Res. 16:629–635, 1998.
Blanpied, P., and G. L. Smidt. The difference in stiffness of the active plantarflexors between young and elderly human females. J. Gerontol. 48:M58–M63, 1993.
Brown, M., I. Engberg, and P. Matthews. The relative sensitivity to vibration of muscle receptors of the cat. J. Physiol. 192:773–800, 1967.
Brown, I. E., and G. E. Loeb. A reductionist approach to creating and using neuromusculoskeletal models. In: Biomechanics and Neural Control of Movement and Posture, edited by J. M. Winters, and P. E. Crago. New York: Springer, 2000, pp. 148–163.
Burke, D., K. Hagbarth, L. Löfstedt, and B. G. Wallin. The responses of human muscle spindle endings to vibration of non-contracting muscles. J. Physiol. 261:673–693, 1976.
Cheng, S., J. Timonen, and H. Suominen. Elastic wave propagation in bone in vivo: methodology. J. Biomech. 28:471–478, 1995.
Cuccurullo, S. Electrodiagnostic medicine and clinical neuromuscular physiology. In: Physical Medicine and Rehabilitation Board Review, edited by S. Cuccurullo. New York: Demos Medical Publishing, 2004, pp. 315–319.
Cummings, S., and M. Nevitt. Non-skeletal determinants of fractures: the potential importance of the mechanics of falls. Osteoporos. Int. 4:S67–S70, 1994.
DeGoede, K., and J. Ashton-Miller. Fall arrest strategy affects peak hand impact force in a forward fall. J. Biomech. 35:843–848, 2002.
DeGoede, K., J. Ashton-Miller, and A. Schultz. Fall-related upper body injuries in the older adult: a review of the biomechanical issues. J. Biomech. 36:1043–1053, 2003.
DeGoede, K. M., J. A. Ashton-Miller, A. B. Schultz, and N. B. Alexander. Biomechanical factors affecting the peak hand reaction force during the bimanual arrest of a moving mass. J. Biomech. Eng. 124:107, 2002.
Dietz, V., J. Noth, and D. Schmidtbleicher. Interaction between pre-activity and stretch reflex in human triceps brachii during landing from forward falls. J. Physiol. 311:113–125, 1981.
Flynn, T., P. Cavanagh, H. Sommer, and J. Derr. Tibial flexural wave propagation in vivo: potential for bone stress injury risk assessment. Work 18:151–160, 2002.
Frampton, R., A. Morris, P. Thomas, and G. Bodiwala. An overview of upper extremity injuries to car occupants in UK vehicle crashes. In: Proceedings of the International Research Council on the Biomechanics of Impact. Germany: Hannover, 1997.
Frykman, G. Fracture of the Distal Radius Including Sequelae—Shoulder–Hand–Finger Syndrome, Disturbance in the Distal Radio-Ulnar Joint and Impairment of Nerve Function: A Clinical and Experimental Study. Acta Orthopaedica Scandinavica Supplementum, Vol. 108. Copenhagen: Munksgaard, 1967.
Hsiao, E., and S. Robinovitch. Common protective movements govern unexpected falls from standing height. J. Biomech. 31:1–9, 1998.
Kurtzer, I., J. A. Pruszynski, and S. H. Scott. Long-latency and voluntary responses to an arm displacement can be rapidly attenuated by perturbation offset. J. Neurophysiol. 103:3195–3204, 2010.
Lee, Y., and J. A. Ashton-Miller. The effects of gender, level of co-contraction, and initial angle on elbow extensor muscle stiffness and damping under a step increase in elbow flexion moment. Ann. Biomed. Eng. 39:2542–2549, 2011.
Lo, J., and J. A. Ashton-Miller. Effect of upper and lower extremity control strategies on predicted injury risk during simulated forward falls: a study in healthy young adults. J. Biomech. Eng. 130:041015, 2008.
Lo, J., G. McCabe, K. DeGoede, H. Okuizumi, and J. Ashton-Miller. On reducing hand impact force in forward falls: results of a brief intervention in young males. Clin. Biomech. 18:730–736, 2003.
McDowell, M. A., C. D. Fryar, C. L. Ogden, and K. M. Flegal. Anthropometric reference data for children and adults: United States, 2003–2006: US Department of Health and Human Services. National Center for Health Statistics: Centers for Disease Control and Prevention, 2008.
Norris, A. H., N. W. Shock, and I. H. Wagman. Age changes in the maximum conduction velocity of motor fibers of human ulnar nerves. J. Appl. Physiol. 5:589–593, 1953.
Pierrot-Deseilligny, E., and D. Burke. The Circuitry of the Human Spinal Cord: Its Role in Motor Control and Movement Disorders. Cambridge: Cambridge University Press, pp. 63–112, 2005.
Pruszynski, J. A., and S. H. Scott. Optimal feedback control and the long-latency stretch response. Exp. Brain Res. 218:341–359, 2012.
Saha, S., and R. S. Lakes. The effect of soft tissue on wave-propagation and vibration tests for determining the in vivo properties of bone. J. Biomech. 10:393–401, 1977.
Taylor, P. K. Non-linear effects of age on nerve conduction in adults. J. Neurol. Sci. 66:223–234, 1984.
Thelen, D. G., J. A. Ashton-Miller, A. B. Schultz, and N. B. Alexander. Do neural factors underlie age differences in rapid ankle torque development? J. Am. Geriatr. Soc. 44:804–808, 1996.
Thelen, D. G., A. B. Schultz, N. B. Alexander, and J. A. Ashton-Miller. Effects of age on rapid ankle torque development. J. Gerontol. A-Biol. 51:M226–M232, 1996.
Troy, K. L., and M. D. Grabiner. Asymmetrical ground impact of the hands after a trip-induced fall: experimental kinematics and kinetics. Clin. Biomech. 22:1088–1095, 2007.
Tsuchikane, A., Y. Nakatsuchi, and A. Nomura. The influence of joints and soft tissue on the natural frequency of the human tibia using the impulse response method. Proc. Inst. Mech. Eng. H 209:149–155, 1995.
Winter, D. A. Biomechanics and Motor Control of Human Movement. New York: Wiley, pp. 59–85, 2005.
Wong, F. Y., S. Pal, and S. Saha. The assessment of in vivo bone condition in humans by impact response measurement. J. Biomech. 16:849–856, 1983.
Acknowledgments
The authors wish to thank Kurt M. DeGoede, Ph.D., for conducting pilot studies11 leading to this paper. We thank the subjects for their participation and the financial support of PHS Grant P30 AG 024824 is gratefully acknowledged.
Author information
Authors and Affiliations
Corresponding author
Additional information
Associate Editor Thurmon E. Lockhart oversaw the review of this article.
Rights and permissions
About this article
Cite this article
Lee, Y., Ashton-Miller, J.A. Age and Gender Effects on the Proximal Propagation of an Impulsive Force Along the Adult Human Upper Extremity. Ann Biomed Eng 42, 25–35 (2014). https://doi.org/10.1007/s10439-013-0900-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-013-0900-9