
Abstract
Background
Hemodialysis results in significant change in daily living, physical and psychological impairments, disruption of marital, family, and social life. Health-related quality of life (HRQOL) assessment helps to plan individual treatment strategies, and determine the efficacy, quality of medical and social care provided.
Aim
The focus of the study was to assess HRQOL of hemodialysis patients attending El-Minia University Hospital dialysis unit, determine the relation between HRQOL and some sociodemograghic factors and clinical disorders and also to compare HRQOL between patients performing hemodialysis for less than and more than 5 years.
Subjects and methods
The study is a cross-sectional hospital-based study that included 170 hemodialysis patients; 81 males and 89 females, mean age 46.6 ± 14.6 years. In all 59.4 % were rural residents. Data were collected by a questionnaire which included, demographic, social and medical data. Kidney Disease Quality of Life-36 (KDQOL-36) health survey was used for assessment of HRQOL.
Results
About two thirds (64 %) of the studied hemodialysis patients had physical and mental quality of life (QOL) scores below average level. HRQOL was lower in old, female, married, illiterate and non-worker hemodialysis patients. Hepatitis C positive (HCV), diabetic and anemic patients had decreased QOL scores. A longer duration of hemodialysis treatment was associated with reduced physical QOL.
Conclusion
The most important sociodemographic factors affecting HRQOL were age, sex, education, occupation and marital status. The most important clinical disorders affecting QOL were anemia, HCV infection, sleep disturbances and diabetes. Increase awareness of hemodialysis patients and their caregivers about disabilities associated with hemodialysis treatment and educational programs to decrease the problems which the patients face and to increase the QOL.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic kidney disease (CKD) is a world-wide public-health problem. According to the World Health Organization, diseases of the kidney and urinary tract contribute to global burden with approximately 850,000 deaths every year and more than 115 million disability-adjusted life years. CKD represents the 12th leading cause of death and 17th leading cause of disability (WHO 2008).
The prevalence of dialysis patients in Egypt have increased from 10 per million population (pmp) in 1974 to 225 pmp in 1996 (Barsoum et al. 1996), and then from 403 pmp in 2003 to 483 in 2004 (Afifi 2008). The prevalence rate of ESRD in the El-Minia Governorate increased from 250 pmp in 2002 (El-Minshawy et al. 2002) to 260 pmp in 2005 (El-Minshawy and Kamel 2010), and had become 367 pmp in 2007 (El-Minshawy 2011).
Hemodialysis therapy is time-intensive, expensive and requires fluid and dietary restrictions. Long-term dialysis therapy itself often results in loss of freedom, the burden of coping with an incurable disease, dependence on caregivers, disruption of marital, family, and social life and reduced or complete loss of financial income. Due to these reasons, physical, psychological, socioeconomic and environmental aspects of life are impaired (Sathvik et al. 2008). One of the main points when treating patients with end-stage renal disease (ESRD), whose cure is not a realistic goal, is maximizing functioning and well-being, which refers to the ability to perform various daily activities and functions, and to support the patient in finding enjoyment in life. Patient assessments of functioning and well-being, which is referred to as HRQOL, also includes general health perception in each of three domains: physical, psychological and social (Kutner 2007).
Previous studies from various countries have been performed to find factors that affect the HRQOL of patients with ESRD. Although there are some inconsistencies between their results—overall physical factors; psychosocial factors such as marital status, depression, and anxiety levels; sociodemographic and clinical factors such as age, gender, duration of renal disease and dialysis, comorbid physical illnesses (e.g. diabetes)—all seem to have a significant effect on HRQOL (Kimmel and Patel 2007). ‘Adding life to years and not just years to life’ is as true for ESRD patients as for anyone else; thus, attaining a good health-related quality of life (HRQOL) in these patients is a difficult task, requiring significant efforts from nephrologists and support from social workers and psychologists (Seica et al. 2009).
This study was conducted to assess the quality of life (QOL) of hemodialysis patients and to determine the relation between QOL and some medical disorders (such as anemia, hypertension, diabetes mellitus and being hepatitis C positive (HCV). It also includes a comparison between patients performing dialysis for less than and more than 5 years.
Subjects and methods
This is a cross-sectional hospital-based descriptive study conducted to assess the QOL of hemodialysis patients and was carried out in the dialysis unit of El-Minia University Hospital during the period from January to June 2011. The El Minia Governorate is one of the Upper Egypt governorates and is 240 km to the south of Cairo. Approval was granted by the director of the El-Minia University Hospital dialysis unit and from the Head of the Department of Internal Medicine to obtain data from the hemodialysis patients and the results of some investigations regarding the patients to be included in the study.
This study was conducted among 170 hemodialysis patients (all hemodialysis patients attending El-Minia University Hospital dialysis unit during the period from 1st January to 30th June 2011) who agreed to be interviewed and to participate in the study; the response rate was 98 %. Patients who have undergone renal dialysis for less than 3 months, and patients who were admitted to the hospital were excluded from the study. Data were collected by a well-structured questionnaire, every participant in the study was interviewed in the dialysis unit by the researchers who took their answers and explained the aim of the study. The questionnaire included demographic data, social data, history of medical disorders, duration of dialysis treatment, clinical and laboratory data.
Quality of life was assessed by using a kidney-disease-specific measure of HRQOL known as the Kidney Disease Quality of Life-36 (KDQOL-36) survey which includes the 12- Item Short Form (SF-12) health survey plus kidney-disease-specific scales (Stec et al. 2008). The first 12 items of the KDQOL-36 are the Medical Outcomes Survey (MOS) SF-12 survey, which measures patients’ perceptions of their own physical and mental functioning. In addition, there are 24 kidney-disease specific questions. The KDQOL-36 survey consists of five scales:
-
1.
SF-12: physical component summery (PCS) includes:
-
Physical function: the patient can perform moderate activities such as moving a table or climbing several floors of stairs
-
Physical role: refers to limitations due to physical health problems
-
Pain and questions as to what degree pain interferes with normal work
-
General health perception and how the patient thinks about his or her health
-
-
2.
SF-12: mental component summery (MCS) includes:
-
Emotional wellbeing
-
Emotional role: refers to the role of limitations due to emotional health problems
-
Social function: the extent that physical health or emotional problems interfere with normal social activities with family, friends, or groups of people
-
Energy and fatigue: whether the patient has a lot of energy or feels fatigued
-
-
3.
Burden of kidney disease (questions 13–16):
Includes items about how much kidney disease interferes with daily life, takes up time, causes frustration, or makes the respondent feel like a burden to his or her family.
-
4.
Symptoms and problems (questions 17–28):
Assesses the extent a patient has been bothered (not at all, somewhat, moderately, very much and extremely) by symptoms during the last 30 days and includes items relevant to patients with kidney disease such as how bothered a respondent feels by sore muscles, chest pain, cramps, itchy or dry skin, shortness of breath, faintness/dizziness, lack of appetite, feeling exhausted or drained, numbness in the hands or feet, nausea, upset stomach or problems with dialysis access.
-
5.
Effects of kidney disease on daily life (questions 29–36):
Includes items about how bothered the respondent feels by fluid limits, diet restrictions, ability to work around the house, ability to travel, feeling dependent on doctors and other medical staff, stress or worries caused by kidney disease, sex life and personal appearance.
Scores are reported separately for each of the five KDQOL-36 scales. Results are summarized into the MCS scale, the physical component summary PCS, and the kidney disease component summary KDCS scores; the latter being a simple sum of the scores for kidney-specific questions with higher scores showing better QOL. Patient subscale scores and their QOL are divided into three groups (thirds):
-
1.
More than 1 SD above the mean is “above average”
-
2.
The mean +/– 1 SD is “average”
-
3.
More than 1 SD below the mean is “below average” (Schatell and Witten 2008)
Statistical analysis
The statistical program SPSS for Windows, version 13, was used for data analysis. Quantitative data were presented by mean and standard deviation, while qualitative data were presented by frequency distribution, chi squared test, student t test, one-way ANOVA test. In addition, multiple regression analysis was used to show the combined effect of different independent variables on the target (dependant variable). The probability of less than 0.05 was used as a cut-off point for all significant tests
Ethical consideration
Following ethical guidelines of epidemiological research, a written informed consent was developed and attached to all questionnaires. An explanation regarding the objectives of the study and details of the collected data was given to each subject. Subjects were also assured confidentiality, which was maintained by removing the names of the subjects from data collection forms whereby only numbers were kept for identification. The study protocol was approved by the standard ethics of the El-Minia University ethics committee for human experimentation.
Results
There were 81 males (47.6 %) and 89 females (52.4 %) among the studied sample as shown in (Table 1). About a quarter of the sample (22.4 %) were in the age group ≥60 years and 76 (44.7 %) of the patients had ≥5 years duration of dialysis. About half (52.9 %) of hemodialysis patients were married, 68 % of males compared to 39.3 % of females, and 4.9 % of males compared to 34.8 % of females were widows. There was a highly significant difference between males and females regarding educational level (p = 0.0001).
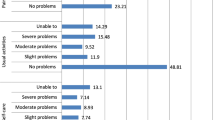
Table 2 shows mean and median scores of the components of the (KDQOL-36) survey. The physical component scale had the lowest score (27.67 ± 7.12) followed by the mental component (35.72 ± 7.07), while the kidney disease component had the highest score (41.99 ± 13.33). This means that physical QOL was more impaired than mental and kidney-disease related aspects of QOL in dialysis patients. Regarding the physical component, physical role, which refers to limitations due to physical health problems such as limitations in the kind of work that could performed or in other activities, scored the lowest (4.71 ± 26.23); conversely, physical function, which refers to the ability to perform moderate activities such as moving a table or climbing stairs, scored the highest. Regarding the mental component, emotional role, which refers to limitations due to emotional health problems such as the patient accomplished less than he or she would have liked and was not able to work or do other activities as carefully as usual, scored the lowest (15.88 ± 46.61); conversely, the highest score (93.29 ± 37.18) was attributed to emotional wellbeing, which includes feeling peaceful, calm, downhearted or depressed. Regarding the kidney disease component, the burden of kidney disease had the lowest score (10.96 ± 10.75). This component refers to the extent kidney disease interferes with daily life, takes up time, causes frustration, or makes the patient feel like a burden to his or her family; on the other hand, symptoms and problems, including sore muscles, chest pain, cramps, itchy skin, shortness of breath, faintness, lack of appetite, feeling exhausted, numbness in the hands or feet, nausea and problems with dialysis access, scored the highest (57.73 ± 15.08).
Male patients had higher physical QOL (29.3 ± 7.99) and kidney disease QOL scores (45.47 ± 14.46) than female patients (26.18 ± 5.88 and 38.82 ± 11.39 respectively), while there was no significant difference as regards mental QOL (Table 3). The duration of hemodialysis treatment negatively affected physical QOL as patients with a longer duration of hemodialysis treatment (>5 years) had a lower physical component score than those with a shorter duration of hemodialysis (26.08 ± 6.47 compared to 28.94 ± 7.39 respectively). Illiterate patients and those who can read and write had significantly lower scores regarding the physical, mental and kidney disease components than the more educated patients. Single patients had the highest score in physical (32.31 ± 5.66), mental (38.47 ± 8.48) and kidney disease components (47.55 ± 12.67). Unemployed patients had the lowest score in physical (26.65 ± 6.46) and kidney disease components (40.48 ± 12.82), while professional patients had the highest scores for each of the physical, mental and kidney disease component scores (43.29 ± 9.04, 52.7 ± 4.86 and 66.15 ± 24.3 respectively).
Medical diseases may affect HRQOF components in hemodialysis patients; Table 4 shows that diabetic patients (n = 36; 21.17 %) had significantly lower physical, mental and kidney disease component scores (21.67 ± 5.99, 33.35 ± 5.73 and 37.18 ± 9.38 respectively) than non-diabetic patients (28.2 ± 7.32, 36.36 ± 7.27 and 43.28 ± 13.96 respectively). Anemic patients (n = 136; 80 %) had lower scores as regards physical and kidney disease component scores (23.77 ± 3.76 and 37.99 ± 11.38 respectively) than non-anemic patients (31.74 ± 7.53 and 46.19 ± 13.99 respectively). In addition, hepatitis C positive patients (n = 103; 60.6 %) had significantly lower scores as regards the physical and kidney disease components (26.22 ± 6.47 and 40.52 ± 13.1 respectively) than hepatitis C negative patients (29.89 ± 7.54 and 44.25 ± 13.47 respectively; however, no significant difference as regarding mental component score (p = 0.6) was found. There was a significant relationship between sleep disturbances (n = 126; 74.1 %) and HRQOL including physical, mental and kidney disease component scores (p = 0.0001).
Multiple regression analysis showed that the most contributing socio-demographic and clinical factors affecting physical component scores among the studied hemodialysis patients were hemoglobin level, age and HCV, while the least contributing factors were education and residence (Table 5). Moreover, the most contributing socio-demographic and clinical factors affecting mental component scores among the studied hemodialysis patients were sleep disturbances and diabetes, while the least contributing factors were education and marital state (Table 6). In addition, the most contributing socio-demographic and clinical factors affecting the kidney disease component score among the studied hemodialysis patients were sleep disturbances and hemoglobin level, while the least contributing factors were education and occupation (Table 7).
Discussion
This cross-sectional hospital based study was conducted to assess the HRQOL and its relation to the socio-demographic characteristics and some clinical disorders among 170 hemodialysis patients attending El-Minia University Hospital dialysis. The age distribution of the studied patients ranged between 18 and 80 years old, 22.4 % of them were in the 60 years or more age group and 44.7 % had been on hemodialysis for 5 years or more. The mean age was 46.62 ± 14.59 and the study group consisted of (47.6 %) males and (52.4 %) females, which is similar to the mean age found by a previous study about hemodialysis patients carried out in the El Minia government which showed that the mean age was 46 ± 13 and males outnumber females (El-Minshawy 2011).
This study showed that ESRD patients on dialysis treatment had lower QOL scores; as PCS, MCS and KDCS scores were below the average values in 64 % of patients. This is in agreement with Amer et al. (2011) who studied QOL and functional-level assessment in Egyptian patients on chronic hemodialysis treatment and found that chronic hemodialysis significantly impaired physical and mental QOL. Our study demonstrated that PCS scores were lower than MCS scores and KDCS; in other words, despite the worsening of the physical health status, the mental health of dialysis patients is relatively preserved (Seica et al. 2009; Kim et al. 2012). This may be explained by the dynamic adaptation of patients’ expectations to their chronic illness (Brady et al. 2003).
This study showed that the subscale burden of kidney disease had the lowest score as compared with the other specific subscales of KDCS. This is can be explained in that the burden subscale assesses perceptions of frustration and interference of the disease in the life of every person, independent of symptoms or adaptation to the effects of the disease in their daily life (Fukuhara et al. 2003), which is consistent with another study by Unruh et al. (2005).
As regards the relation between QOL scores and sociodemographic and clinical factors, it was observed from this study that age had a significant influence on physical and mental QOL; as young patients had higher PCS, MCS and KDCS scores than old patients (≥60 years). This is in agreement with Lessan-Pezeshki and Rostami (2009) who studied contributing factors in HRQOL of ESRD patients in Iran using KDQOL-SF and found that there was a significant negative effect for old age on each of PCS, MCS and KDCS.
Duration of dialysis treatment plays an important role affecting the QOL of hemodialysis patients. This study found that longer duration on hemodialysis treatment (≥5 years) was associated more with lower physical QOL scores than shorter duration (>5 years) of treatment but had no significant effects on both mental and kidney-disease-related aspects of QOL, which is in agreement with Bohlke et al. (2008) who found that higher scores in the physical QOL occurred among patients who had been on dialysis for shorter lengths of time. Moreover, Pakpour et al. (2010) found that patients with a longer duration of hemodialysis suffered from poorer physical QOL but experienced no significant decrease in mental QOL.
A higher educational level was associated with higher PCS, MCS and KDCS scores, which is in agreement with a study in Egypt (Assal et al. 2006) and another study in Saudi Arabia (Bayoumi et al. 2009). These results are explained by the role of higher education in raising the awareness of the patients about the nature of chronic diseases and providing better coping ability regarding problems of hemodialysis treatment. On the other hand, AL-Jumaih et al. (2011) found that QOL scores were not significantly affected by level of education. Possibly, highly educated patients always hope for better QOL and state of health which makes them unsatisfied with their physical and mental health.
This study found that rural patients had lower PCS scores than urban patients. These results are in agreement with another study (Sathvik et al. 2008) and these results may be explained by the fact that rural residents in Egyptian community depend on their physical strength to do indoor and outdoor activities and hemodialysis markedly impairs their physical function.
Diabetic patients had lower MCS and KDCS than non-diabetic patients, which is in agreement with Seica et al. (2009) who found that the presence of diabetes was a significant factor for worsening the physical functioning. Furthermore, Anees et al. (2011) studied dialysis-related factors affecting QOL in hemodialysis patients in Pakistan and found that non-diabetic patients on hemodialysis had better QOL in physical health as compared to diabetic patients.
The current study found that anemic patients had lower scores as regards physical and kidney disease components than non-anemic patients, which is in agreement with Arogundade et al. (2005) who assessed QOL of hemodialysis patients in Egypt and found a positive correlation between HRQOL and hemoglobin concentration. Hepatitis C positive patients had significant difference in physical and kidney disease QOL but no significant difference regarding mental QOL. This can be explained by adaptation to chronic illness over time, which is in agreement with Afsar et al. 2009 who studied QOL of hemodialysis patients using SF-36 in Turkey and found that HCV positive patients had lower PCS and MCS scores than negative patients. There is significant effect of sleep disturbances on physical, mental and kidney-disease-related aspects of QOL and this is in agreement with Elder et al. 2008 who studied sleep quality that predicts QOL and mortality risk in hemodialysis patients and found that higher sleep quality scores were significantly associated with higher MCS and PCS scores.
Using multivariable regression analyses of sociodemographic and clinical factors affecting the PCS and MCS among hemodialysis patients, this study found that age, anemia and hepatitis C infection are negative predictors of physical QOL score, while sleep disturbances, diabetes and occupation are negative predictors of mental QOL. Multivariable regression analyses by Kao et al. (2009) showed that older age was significantly inversely associated with PCS but not with MCS. Moreover, in the study of predictors of QOL in hemodialysis patients by Bayoumi et al. (2009), multiple regression analysis demonstrated that age, dialysis duration, and male gender were negative predictors of QOL score.
According to Vasilieva (2006) who studied the QOL in chronic hemodialysis patients in Russia, linear regression analysis showed that duration of dialysis was a significant independent predictor of low PCS in hemodialysis patients. Chiang et al. (2004) studied the QOL on 497 Taiwanese hemodialysis patients in five hospitals using the SF-36 questionnaire. They found that male gender, age <50 years old, higher education level, marriage status, employment status and non-diabetic patients were all predictors of better PCS.
The limitations to this study include the cross-sectional design of the study which did not allow us to consider temporary trajectories of QOL, the small sample size and the use of only one clinical site. Replication using a larger sample from a number of sites with a longitudinal design and better control for extraneous variables is recommended. In conclusion HRQOL of hemodialysis patients is impaired. The most important sociodemographic factors affecting HRQOL were age, sex, education, occupation and marital status. The most important clinical disorders affecting QOL were anemia, HCV infection, sleep disturbances and diabetes.
References
Afifi A (2008) The Egyptian Renal Registry, The 9th annual report for the year 2008. Published on 29th Annual Congress of Nephrology of Egyptian Society of Nephrology and Transplantation (ESNT). Hurgada, Egypt. http://www.esnonline.net/content/downloads/registry/2008.pdf. Accessed on October 2011
Afsar B, Elsurer R, Sezer S, Ozdemir NF (2009) Quality of life in hemodialysis patients: hepatitis C virus infection makes sense. Int Urol Nephrol 41(4):1011–1019
Al-Jumaih A, Al-Onazi K, Binsalih S, Hejaili F, Al-Sayyari A (2011) A study of quality of life and its determinants among hemodialysis patients using the KDQOL-SF instrument in one center in Saudi Arabia. Arab J Nephrol Transplant 4(3):125–130
Amer M, Wahba H, Raafat V, Refaat H (2011) Study of QOL and functional level in Egyptian elderly on chronic hemodialysis treatment. Middle East J Age Aging 8(2):3–6
Anees M, Hameed F, Mumtaz A, Ibrahim M, Khan M (2011) Dialysis-related factors affecting quality of life in patients on hemodialysis. Iran J Kidney Dis 5(1):9–14
Arogundade FA, Abd-Essamie MA, Barsoum RS (2005) Health-related quality of life in emotionally related kidney transplantation: deductions from a comparative study. Saudi J Kidney Dis Transplant 16(3):311–320
Assal HS, Emam HM, Abdul Ghaffar N (2006) Health-related quality of life among Egyptian patients on hemodialysis. J Med Sci 6:314–320
Barsoum RS, Nabil M, Saady G (1996) Immunoglobulin A and the pathogenesis of schistosomal glomerulopathy. Kidney Int 50(3):920–928
Bayoumi M, Al Wakeel J, Al Harbi A, Al Suwaida A, Al Ghonaim M, Sulimani F, Mashraqy A (2009) Predictors of quality of life in hemodialysis patients. Self-learning package for hemodialysis patients, Saudi Arabia. Available at http://faculty.ksu.edu.sa/73577/Pages/PredictorsofQualityofLifeinHemodialysispatients.aspx. Accessed November 2011
Bohlke M, Nunes D, Marini S, Kitamura C, Andrade M (2008) Predictors of quality of life among patients on dialysis in southern Brazil. Sao Paulo Med J 126(5):252–256
Brady HD, Wilcox CS, Blake C, Plant WD (2003) Measures to improve quality of life in end-stage renal disease patients. In: Therapy in nephrology and hypertension. Saunders, Philadelphia, PA, pp 747–751
Chiang CK, Peng YS, Chiang SS, Yang CS, He YH, Hung KY, Wu KD, Wu MS, Fang CC, Tsai TJ, Chen WY (2004) Health-related quality of life of hemodialysis patients in Taiwan: a multicenter study. Blood Purif 22(6):490–498
Elder SG, Pisoni RL, Akizawa T, Fissell R, Andreucci VE, Fukuhara S, Kurokawa K, Rayner HC, Furniss AL, Port FK, Saran R (2008) Sleep quality predicts quality of life and mortality risk in haemodialysis patients: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol Dial Transplant 23(3):998–1004
El-Minshawy O (2011) End stage renal disease in El-Minia Governorate, Egypt: data of the year 2007. Nephro-Urol Mon 3(2):118–121
El-Minshawy O, Kamel EG (2010) Diabetics on hemodialysis in El-Minia Governorate, Upper Egypt: five-year study. Int Urol Nephrol 2:118–121
El-Minshawy O, El Sharqawy M, Ewis A (2002) End stage renal disease in El Minia Governorate (central Egypt): an epidemiological study. J Egypt Soc Nephrol 4:34–41
Fukuhara S, Lopes AA, Bragg-Gresham JL, Kurokawa K, Mapes DL, Akizawa T, Bommer J, Canaud BJ, Port FK, Philip J (2003) Health-related quality of life among dialysis patients on three continents: the Dialysis Outcomes and Practice Patterns Study. Kidney Int 64:1903–1910
Kao TW, Lai MS, Tsai TJ, Jan CF, Chie WC, Chen WY (2009) Economic, social, and psychological factors associated with health related quality of life of chronic hemodialysis patients in northern Taiwan. Artif Organs 33(1):61–68
Kim J, Kim B, Park K, Choi J, Seo J, Park S, Kim CH, Kim Y (2012) Health-related quality of life with KDQOL-36 and its association with self-efficacy and treatment satisfaction in Korean dialysis patients. Qual Life Res. doi:10.1007/s11136-012-0203-x
Kimmel PL, Patel SS (2007) Quality of life in patients with chronic kidney disease: focus on end-stage renal disease treated with hemodialysis. Semin Nephrol 26(1):68–79
Kutner N (2007) Quality of life assessment in a recent haemoglobin trial in CKD (CHOIR). Nephrol Dial Transplant 22(7):2099
Lessan-Pezeshki M, Rostami Z (2009) Contributing factors in health-related quality of life assessment of ESRD patients: a single center study. Int J Nephrol Urol 1(2):129–136
Pakpour A, Saffari M, Yekaninejad M, Panahi D, Harrison A, Molsted S (2010) Health-related quality of life in a sample of Iranian patients on hemodialysis. Iran J Kidney Dis 4(1):50–59
Sathvik BS, Parthasarathi G, Narahari MG, Gurudev KC (2008) An assessment of the quality of life in hemodialysis patients using the WHOQOL-BREF questionnaire. Indian J Nephrol 18(4):141–149
Seica A, Segall L, Verzan C, Vaduva N, Madincea M, Rusoiu S, Cristea S, Stefan M, Serbanescu D, Morosanu P, Grajdeanu L, Andronache R, Nechita M, Dragos D, Dronca A, Gusbeth-Tatomir P, Mircescu G, Covic A (2009) Factors affecting the quality of life of haemodialysis patients from Romania: a multicentric study. Nephrol Dial Transplant 24:626–629
Schatell D, Witten B (2008) Measuring dialysis patients’ health-related quality of life with the (KDQOL-36). Med Educ Inst 608:833–8033
Stec P, Schatell D, Witten B (2008) Why we need a health-related quality of life CPM. Nephrol News Issues 22(3):28–30, 35
Unruh ML, Weisbord SD, Kimmel PL (2005) Health-related quality of life in nephrology research and clinical practice. Semin Dial 18:82–90
Vasilieva IA (2006) Quality of life in chronic hemodialysis patients in Russia. Hemodial Int 10(3):274–278
World Health Organization (2008) The global burden of disease. World Health Organization, Geneva. Available at http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf. Accessed September 2011
Acknowledgments
The authors would like to offer their sincere thanks to all patients who participated in the study, and who gave of their time to answer our questions
Conflict of interest
No conflict of interest has been declared.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kamal, N.N., Kamel, E.G., Eldessouki, K.H. et al. Health-related quality of life among hemodialysis patients at El-Minia University Hospital, Egypt. J Public Health 21, 193–200 (2013). https://doi.org/10.1007/s10389-012-0538-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-012-0538-3