
Abstract
The aim of this study is to evaluate the effectiveness over application time of different formulations of a novel endodontic irrigant (QMix™ 2in1) composed of a polyaminocarboxylic acid chelating agent, a bisbiguanide antimicrobial agent, a surfactant and deionized water to remove the root canal smear layer and expose patent dentinal tubules compared to a standard solution of 17 % EDTA. Eighty human tooth roots from extracted, single-rooted teeth were instrumented (size 40.06) using 0.2 mL of sodium hypochlorite (6.15 %) between each file size with a 3 mL water rinse after final instrumentation. Eight groups of 10 roots were irrigated with 3 mL of different formulations of QMix: QMix A, QMix B, and QMix C, or 17 % EDTA for 60 and 90 s, respectively, then rinsed with 5 mL of sterile water. The roots were irrigated using a standard irrigation syringe and a 30 ga side-vent needle with an apical-coronal motion to within 1 mm of the working length. The coronal, middle and apical thirds of one canal surface of each root was evaluated at 1000× using scanning electron microscopy. The presence of smear layer was scored using a 5-point scale. Data were analyzed with the Kruskal–Wallis rank sums test, the Steel–Dwass, all-pairs comparison test, and the Steel method (with control) test. Irrigant type was highly significant (p < 0.007). Combined 60 and 90 s exposure data indicated QMix A (p = 0.014) and QMix C (p = 0.028) were superior to EDTA. While at the 90 s exposure time, smear layer removal by solutions QMix A (p = 0.043), QMix B (p = 0.018), and QMix C (p = 0.011) was superior to EDTA. All irrigants removed smear layer more effectively at the coronal and middle levels compared to the apical level (p < 0.001). Analysis showed all three QMix formulations were superior to EDTA in smear layer removal and exposure of dentinal tubules in the root canal system in single-rooted teeth.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Application of root canal instruments, in particular rotary instruments to the root canal wall during enlarging and shaping of the canal results in variable-thickness smear layer formation that covers the dentinal tubules and fills canal irregularities. This packed layer is composed of inorganic debris, dentin particles, and organic materials including pulp tissue remnants, bacteria (and their by-products) and blood cells, which has been described in depth by multiple authors [1, 2]. Furthermore, smear layers are usually packed into dentinal tubules at various depths up to 40 μm, which are known as smear plugs [3, 4]. The composition and morphology of the smear layer and smear plugs suggest that their removal during root canal procedures is necessary to achieve the desired outcomes of debris removal and disinfection [5, 6] although this recommendation has been controversial for many years [7]. If removed not only is the bacteria-laden dentinal and soft tissue debris removed, but also the dentinal tubules are exposed for further bacterial control through the use of disinfecting solutions [8].
Presently cleaning and disinfection of the root canal system requires the use of inorganic and organic solvent addition to an antimicrobial agent. However, no single solution is able to achieve these goals and the combined, concomitant or sequential use of two or more irrigating solutions is required. Currently, sodium hypochlorite (NaOCl) (0.5–6.15 %) and EDTA (15–17 %) are the two most commonly used intracanal irrigants [9–11]. NaOCl acts as a solvent of organic material and potent primary antimicrobial agent, while EDTA serves as the inorganic solvent or chelating agent. Using a combination of the two would represent the most optimal irrigation protocol. However, these agents cannot be combined directly prior to application or in situ because mixing results in an almost immediate complete loss of free chlorine, thus adversely affecting the antimicrobial properties of NaOCl [9, 12]. Furthermore, if the NaOCl is used as a final rinse or soak following the use of EDTA, the structural integrity of the dentin may be compromised [10, 13–15].
Elimination of an additional rinse or soak after smear layer removal with EDTA has been shown to preserve the integrity of the dentin [16]. However, disinfection of the dentin surface and dentin tubules may still be necessary. Subsequently following smear layer removal, soaking the root canal with chlorhexidine (2 %) has been advocated by many researchers and clinicians [17–19] due to its compatibility with dentin [20] and the potential for lasting residual antimicrobial effects [21]. However, it also may result in a precipitate of para-chloroaniline, which is potentially toxic, on contact with residual NaOCl [22–25]. Therefore, it is necessary to purge any remaining NaOCl from the root canal with copious quantities of sterile water, alcohol, or saline [24, 26] prior to the use of chlorhexidine.
To meet these challenges in the irrigation of the root canal system, a novel irrigating solution, QMix™ 2in1 (DENTSPLY Tulsa Dental Specialties, Tulsa, OK, USA) has been introduced to both remove smear layer and kill bacteria. This irrigant has a proprietary formulation and method of preparation, and has been shown to remove smear layer and kill recalcitrant bacteria, such as E. faecalis, in one application [8]. QMix™ is composed of a polyaminocarboxylic acid chelating agent, a bisbiguanide antimicrobial agent, a surfactant and deionized water [11]. Furthermore, QMix™ does not interact with remnant NaOCl to generate a precipitate if used as directed for the final rinse [Internal data on record with DENTSPLY Tulsa Dental Specialties, Tulsa, OK, USA] and its ability to penetrate into patent, smear-plug free dentin to kill bacteria present has been demonstrated using a novel model with potential significant clinical outcomes and implications [8].
Multiple variations of the QMix™ 2in1 irrigant have been compared to BioPure MTAD (DENTSPLY Tulsa Dental Specialties, Tulsa, OK, USA) and EDTA with regards to canal smear layer and debris removal [27]. According to the study, one version of the QMix™ solution evaluated was statistically comparable to BioPure MTAD following 60 s usage versus 5 min for BioPure MTAD, and the solution was more effective than 17 % EDTA at removing smear layer. Initial developmental research with QMix™ showed different levels of efficacy for smear layer removal when formulations were adjusted and time frames of usage were considered.
Therefore, the purpose of this study was to compare different formulations of QMix™ at two different application times with 17 % EDTA to evaluate these formulations for clinical use and to establish a protocol that facilitates the most efficacious removal of smear layer from the smear-laden root canal walls and canal irregularities. The three versions of QMix™ tested were identical in the ratios of active ingredients but varied slightly in pH, a secondary chemical property, as a means to identify a target formulation range for production. The solutions are principally composed of a polyaminocarboxylic acid chelating agent, a bisbiguanide antimicrobial agent, a surfactant and deionized water. The null hypothesis tested is that there is no statistical difference in smear layer removal performance between the various QMix™ solutions and EDTA.
Materials and methods
Preparation of tooth root model
Eighty single-rooted extracted human teeth (n = 20) were selected for this study. A diamond bur was used to remove the clinical crown of each tooth and to standardize the root length at 15 mm. Subsequently, a #10 K-file was inserted beyond the apex to confirm patency; 1 mm was subtracted from this length to establish the length to which the canals would be instrumented. The canals were enlarged and a glide path established with hand instruments to a size #20 K-file. In the presence of 6.15 % NaOCl (The Clorox Co., Oakland, CA, USA), ProTaper® Universal (DENTSPLY, Tulsa Dental Specialties, Tulsa, OK, USA) nickel-titanium rotary instruments were used to shape the canal to an apical size 40/0.06 (F4). Instruments were rotated at 300 rpm and allowed to progress without applying apical pressure to the established length, which was 1 mm short of the apex. Between each file the canals were rinsed with 0.2 mL 6.15 % sodium hypochlorite using a 30 ga side-vented needle (Max-i-Probe®, DENTSPLY RINN, Elgin, IL, USA).
Irrigation groups
Following final instrumentation and rinsing with NaOCl the canals were irrigated with 3 mL of sterile water. The specimens were divided into eight groups of ten teeth and irrigated with 3 formulations of QMix™ 2in1, designated QMix A, QMix B, and QMix C, and with EDTA as follows: (1) 3 mL of QMix A for 60 s; (2) 3 mL of QMix A for 90 s; (3) 3 mL of QMix B for 60 s; (4) 3 mL of QMix B for 90 s; (5) 3 mL of QMix C for 60 s; (6) 3 mL of QMix C for 90 s; (7) 3 mL of 17 % EDTA (Roydent Dental Products, Johnson City, TN, USA) for 60 s; (8) 3 mL of 17 % EDTA for 90 s.
To ensure adequate and even distribution of the solutions, the roots were irrigated using a standard irrigation syringe and a 30 ga side-vented needle with an apical-coronal motion to within 1 mm of the working length. Finally, the roots were rinsed thoroughly with 5 mL sterile water after the experimental exposure time to remove any excess solution and/or debris.
Scanning electron microscopy
For scanning electron microscopy (SEM) analysis, each specimen had their apical foramen and coronal opening sealed prior to longitudinal grooving and splitting into two halves using a hammer and chisel, along the coronal-apical axis. All specimens were washed briefly in cold 0.2 M potassium phosphate buffer, pH 7.2. The specimens were fixed in 2 % glutaraldehyde in 0.2 M potassium phosphate buffer, pH 7.2, at 4–6° C, for 18 h and then were washed gently in 0.2 M potassium phosphate buffer, pH 7.2, for 15 min. Dehydration of the specimens was completed using an acetone series as follows: 30 % acetone for 10 min, 60 % acetone for 10 min, 100 % acetone overnight (18 h). The specimens were taken from the 100 % acetone bath and critical point dried. Each specimen was examined grossly to determine the more appropriate half to be examined under SEM. The side of the specimen that appeared to have more canal space visible for examination was selected. The chosen specimens were mounted on SEM stubs and sputter-coated with gold then stored under vacuum.
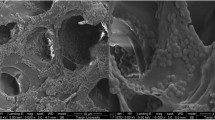
SEM was performed using a SU 6600 Hitachi Scanning Electron Microscope, (Hitachi High-Technologies Corporation, Japan). All specimens were examined at 1000× magnification to evaluate smear layer and debris in the coronal (10–12 mm from the apex), middle (6–7 mm from the apex), and apical (apical 1–2 mm from the apex) thirds. Fifteen microscopic fields per segment were viewed and photomicrographs were taken for a total of 45 fields per tooth. Viewing of the photomicrographs was blinded and scored for the presence of smear layer using the following ordinal criteria [28] (Fig. 1):

Scanning electron microscope photomicrographs of root canal walls (original magnification 1000×). a Representative specimen with a score of 1 = 100 % of the tubules in the sections examined are patent and there is no smear layer; b 2 ≥ 75 % < 100 % of the tubules in sections examined are patent and small area of smear layer are present; c 3 ≥ 50 % < 75 % of the tubules in sections examined are patent and larger areas of smear layer are present; d 4 ≥ 25 % < 50 % of the tubules in sections examined are patent and up to 50 % of the surfaces are covered with smear layer; e 5 ≤ 25 % to 0 % of the tubules in sections examined are patent and the majority of not all surfaces are covered with smear layer
-
1 = 100 % of the tubules in the sections examined were patent and there was no smear layer.
-
2 ≥ 75 % < 100 % of the tubules in sections examined were patent and small area of smear layer were present
-
3 ≥ 50 % < 75 % of the tubules in sections examined were patent and larger areas of smear layer were present
-
4 ≥ 25 % < 50 % of the tubules in sections examined were patent and up to 50 % of the surfaces were covered with smear layer
-
5 ≤ 25 % to 0 % of the tubules in sections examined were patent and the majority if not all surfaces were covered with smear layer
For the 60- and 90-second irrigations with the four treatments (QMix A, QMix B, QMix C, and EDTA), median smear layer scores were calculated from the raw data for the three tooth areas (apical, middle and coronal) and entered into statistical analyses (that is, for the 80 teeth, there were 80 median values for the apical areas, 80 median values for the middle areas, and 80 median values for the coronal areas.
Statistical analysis
For the four treatments (QMix A, QMix B, QMix C, and EDTA), and the three tooth areas (apical, middle and coronal) box plots were created and descriptive statistics (median, minimum, and maximum values) were calculated. To test for differences among groups, the Kruskal–Wallis rank sums test was used, and to test for differences between groups, the Steel–Dwass, all-pairs comparison test was used (this is a nonparametric version of the all pairs, Tukey honestly significant difference test). The Steel method was used to test for differences between QMix treatments and the control (EDTA). This test is a nonparametric version of the Dunnett’s test used to compare each level with a control. Alpha was set at 0.05. Statistical analyses were performed with JMP Statistical Software Release 10.0.0 (SAS Institute, Inc., Cary, NC).
Results
Statistical analysis, Fig. 2, contains box plots and summary statistics (medians, minimums, and maximums) for smear layer removal recorded in the apical, middle and coronal areas of the teeth. Figure 2 also contains box plots for median smear layer removal for the various treatments (QMix A, QMix B, QMix C, and EDTA). For these box pots, 60- and 90-second irrigations were combined. Median smear layer scores ranged from 1.0 to 5.0 in the middle and coronal areas and 2.0 to 5.0 in the apical areas. These combined data from all irrigants revealed significant differences among the smear layer scores in the three root areas (Kruskal–Wallis rank sums test, p < 0.001) and between tooth areas (Steel–Dwass, all-pairs comparison, p < 0.001) with smear layer levels in the apex > middle > coronal. There were significant differences among the treatments (Kruskal–Wallis rank sums test, p = 0.007). The Steel method used to test for differences with EDTA (control) demonstrated that QMix A and QMix C removed significantly more smear layer than EDTA (p = 0.014 and 0.028) but QMix B did not (p = 0.085). No significant difference in smear layer removal among the three QMix formulations was demonstrated (Kruskal–Wallis rank sums test, p = 0.283).

For 60- and 90-second irrigations combined, box plots of median values for coronal, middle, and apical areas of the teeth (a) and median values for treatments (b). To better illustrate the distribution of the data points; they are spread horizontally to minimize their overlapping one another. The ends of the boxes are the 25th and 75th quantiles (quartiles). The lines across the middles of the boxes are the medians. The interquartile range is the difference between the quartiles. The lines (whiskers) extend from the boxes to the outermost points that fall within the distance computed as 1.5 (interquartile range)
To determine the effects of a longer exposure time, the 90-second smear layer removal data was analyzed separately, Fig. 3. Significant differences were demonstrated among the irrigants (Kruskal–Wallis rank sums test, p = 0.005). While the Steel method used to test for differences with EDTA (control) demonstrated that QMix A, QMix B and QMix C removed significantly more smear layer than EDTA (p = 0.043, 0.018, and 0.011); no difference in smear layer removal among the three QMix formulations was demonstrated (Kruskal–Wallis rank sums test, p = 0.623). Altogether, these data indicate that, especially at the 90-s irrigation time, all of the QMix formulations are superior to EDTA.

For 90-second irrigations, box plots of median values for treatments. To better illustrate the distribution of the data points; they are spread horizontally to minimize their overlapping one another. The ends of the boxes are the 25th and 75th quantiles (quartiles). The lines across the middles of the boxes are the medians. The interquartile range is the difference between the quartiles. The lines (whiskers) extend from the boxes to the outermost points that fall within the distance computed as 1.5 (interquartile range)
Discussion
When compared to the positive EDTA control all of the QMix formulations were superior at removing smear layer in instrumented tooth roots. However, there was no definitive evidence that a single QMix formulation removed significantly more smear layer than the other two. It is possible that a larger sample size would reveal differences. Another limitation may be the use of nonparametric statistics for analysis of the data collected through this complex experimental design. Statisticians do not agree with regard to whether parametric or nonparametric procedures should be used with ordinal scale measurements [29, 30]. The main problem associated with using parametric procedures is the assumption that ordinal intervals are consistent. Advocates of using parametric procedures with ordinal data argue that parametric procedures are robust for even major violations of assumptions [31, 32]) and that parametric procedures are more powerful and versatile with complex designs. Although the ordinal rankings of this study appeared to fulfill the assumption that ordinal intervals are consistent and although our study had a fairly complex design, we elected to use conservative parametric procedures. Because of this, we limited the number of tests performed to lessen the likelihood of committing a type I error (declaring a difference when none exists). We acknowledge that using nonparametric procedures, we do increase the risk of a Type II error (declaring no difference when one exists). To balance risks of type I and II error rates, we used tests to adjust for multiple comparisons.
The results of this study demonstrate that QMix™ 2in1 has promise as a one-step irrigant for smear layer removal. This could be advantageous on two counts. Multiple studies have demonstrated the efficacy of using NaOCl and EDTA sequentially for smear layer removal, with NaOCl as the final antiseptic rinse [33–36]. Following canal enlarging and shaping, Goldman et al. [33] recommended 1 mL of 17 % EDTA followed by 10 mL of 5.25 % NaOCl. However, additional studies have questioned the combined use of NaOCl and EDTA in that their use may affect the mechanical properties of the remaining dentin [13, 37, 38]. Use of full strength NaOCl (5.25–6.15 %) appears to weaken dentin as evidenced by a significant increase in the surface strain of the remaining dentin. While this affect will plateau, indicating disintegration of the organic component, it could be hypothesized that the use of a chelating agent to remove the inorganic layer would expose additional organic components of the dentin, and a final rinse with NaOCl would further weaken the structure of the dentin. Furthermore, the combined use of NaOCl and EDTA almost immediately reduces the available chlorine in solution [12]. This has been confirmed previously, with negative impacts on both the tissue dissolution [39] and antimicrobial activity [9]. While the calcium-chelating ability of EDTA was not impacted, the combination of NaOCl and EDTA resulted in an almost complete loss of free chlorine in the form of OCl- and HOCl. As a result, Grawehr et al. [39] recommended that it may be clinically advantageous to rinse out any remaining EDTA with copious amounts of NaOCl. As mentioned previously, this step would adversely affect the mechanical properties of the remaining dentin.
Using a higher concentration (6.15 %) of NaOCl to counteract the loss of this irrigants’ properties leads to significantly more erosion of canal dentin [16]; 6.15 % is currently considered the most common concentration utilized by endodontists in the region in which this study was conducted. A 3 % solution of NaOCl was reported not to affect dentinal mechanical properties as compared to a 5 % solution [38]. However, samples were not tested with differing volumes of NaOCl and a reduced concentration of NaOCl would have less available chlorine. The use of a non-hypochlorite-based antimicrobial agent following smear layer removal may therefore be advantageous.
To prevent damage to the root dentin during disinfection, 2 % Chlorhexidine has been used in the clinical environment [20]. On the other hand, disinfection during the smear layer removal step, offers further advantages by reducing the number of post-NaOCl irrigation steps to achieve smear layer removal and disinfection to just one step.
Removal of the smear layer and debris in the apical third of the root canal remains challenging regardless of the solution used. In order to be effective in the instrumented root canal, the irrigant has to reach and be in contact with the entire root canal system for an adequate time. The instrumented shape of the root canal system makes this most problematic at the apex. Irrigant dynamics related to the canal shape, size, irrigant volume and pressure, irrigation needle design and size as well as depth of penetration are all significant variables [40, 41]. Three-dimensional computational fluid dynamics modeling of root canal irrigation demonstrates that the irrigant only rinses a limited distance beyond the tip of the needle where irrigant velocity (pressure) is significant [41]. However, these factors must be tailored at the apex to limit the possibility of apical extrusion into the periradicular tissues [42] or the nature of the irrigant must be altered to reduce or eliminate potential toxicity.
Comparing dentinal architecture from the coronal to apical, the dentin becomes less tubular with more intertubular dentin [42]. The action of any chelating agent may appear to be less effective in the apical third because intertubular dentin is less calcified than intratubular dentin that may reflect varying degrees of sclerosis, and may give the appearance that the agent is not effective in this area [42]. This may be more the case when using root samples from older individuals, which would indicate the research in this area should consider tooth age and the use of matched tooth pairs as factors in developing treatment protocols and determining outcomes. Paqué et al. [43] demonstrated that the dentin at the apical third of teeth was very sclerotic and impermeable, with increasing deposition of intertubular dentin, beginning in the third decade of life [44].
For this study, the selection of the specimens represented a wide range of sources with some teeth having readily visible dentinal tubules in all areas of the canal, while others had minimal to possibly no tubule visibility at the time of the initial survey. This latter finding is to be expected in elderly individuals and in cases where the pulp has undergone a long-term degenerative process with irritational dentin formation or the tubules have become sclerosed. This finding has been identified as being most pronounced in the apical area of canine teeth by Vasiliadis et al. [44], noting that their study, whilst there may appear to be complete mineralization, there were visible tubules remaining partly or completely open. While this type of tubule can and does occur and is often related just to advancing age, there are no definitive studies that have identified 100 % tubule occlusion through the formation of sclerotic dentine. Therefore, when viewing and evaluating all specimens, reasonable efforts were made to distinguish between loose and packed dentinal and between packed debris and solid dentinal structure in the scoring of each section, in addition to tubule patency or visibility. While the lack of tubule visibility may lead to misinterpretation in specimen evaluation; [45] if the evaluator only focused in one area, when this situation presented itself a wider field of dentine was viewed in an attempt to report findings as accurately as possible.
The problem of bacterial invasion into the dentinal tubules with or without the presence of smear layer, their viability, persistence, eradication and ability to cause further periradicular disease has been a controversial subject of many studies [46–52]. Within these studies, commonly used intracanal medicaments have been shown to have no effect on many of these microbial irritants, especially if they have migrated deeply in the dentinal tubules. Love and Jenkinson [52] indicated that a better understanding of the mechanisms of dentinal tubule penetration by bacteria is needed. Furthermore, the development of new control strategies that would both prevent their migration or kill them once they have penetrated the tubules is indicated.
The clinical use of techniques and materials that can both simplify irrigation protocols while achieving thorough removal of contaminated smear layer and disinfection of the dentinal tubules is ideal. At the same time, minimal to no impact on the integrity of the remaining dentin should be evident. Some studies have shown the variable erosive impact of specific acidic solutions (etidronic, EDTA and peracetic) on the microstructure of the dentin during smear layer removal when used in conjunction with NaOCl [45, 53]. Likewise, the outcome of these applications has varied based on location of the dentin and the extent of tubular sclerosis [45] although tubule orientation does not appear to impact on smear layer removal [54].
While there are no evidence-based studies that provide outcomes of treatment based solely on the removal of the smear layer, the literature supports the removal of this debris from the canal walls to enhance the elimination of necrotic tissue debris and irritants, bacterial kill in the dentinal tubules [8], and to encourage intimate adaptation of canal filling materials to both the dentin and into the tubules [55, 56]. However, with some of the newer obturation materials, such as calcium-silicate products, a deleterious outcome may occur due to the alteration in the integrity of dentinal collagen matrix and reduction in its flexural properties [57, 58].
In this study, the efficient and effective use of an irrigant that can remove the smear layer, open the dentinal tubules for disinfection and simplify the irrigation protocol has been demonstrated. Coupled with evidence that this irrigant, QMix™, can not only penetrate through and remove the debris that is formed on the root canal walls during enlargement and shaping, but also kill bacteria within the tubules [8], it is reasonable to consider adaptation of this new technology. However, it is recognized that further clinical studies would be warranted to demonstrate the long-term effect of this therapeutic and all-encompassing approach to root canal cleaning and disinfection. Moreover, it seems reasonable to ascertain this novel solution’s potential to demonstrate enhanced effectiveness when used in conjunction with sonic and ultrasonic agitation, in its ability to penetrate and destroy bacterial biofilms. While initial studies into this realm have been published [59], protocols within did not conform to the present directions for use by the manufacturer (http://www.tulsadentalspecialties.com/Libraries/Tab_Content_-_Irrigation_Activation/QMix_DFU.sflb.ashx accessed 1 September 2012), thereby opening the door to continued research in this field.
Conclusion
The null hypothesis in this study was rejected. All three of the modified QMix™ solutions removed significantly more smear layer when compared with EDTA. From a clinical perspective, QMix™ offers a reasonable and efficacious alternative to EDTA after primary irrigation with NaOCl .
References
McComb D, Smith DC. A preliminary scanning electron microscopic study of root canals after endodontic procedures. J Endod. 1975;1:238–42.
Peters O, Barbakow F. Effects of irrigation on debris and smear layer on canal walls prepared by two rotary techniques: a scanning electron microscopic study. J Endod. 2000;26:6–10.
Mader CL, Baumgartner JC, Peters DD. Scanning electron microscopic investigation of the smeared layer on root canal walls. J Endod. 1984;10:477–83.
Pashley D. Clinical considerations of microleakage. J Endod. 1990;16:70–7.
Torabinejad M, Handysides R, Khademi AA, Bakland LK. Clinical implications of the smear layer in endodontics: a review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94:658–66.
Volich DR, Chandler NP. The smear layer in endodontics—a review. Int Endod J. 2010;43:2–15.
Csonstkowsky M, Wilson EG, Holstein FA. The smear layer in endodontics. Dent Clin North Amer. 1990;34:13–25.
Ma J, Wang Z, Shen Y, Haapasalo M. A new noninvasive model to study the effectiveness of dentin disinfection by using confocal laser scanning microscopy. J Endod. 2011;37:1380–5.
Zehnder M, Schmidlin P, Sener B, Waltimo T. Chelation in root canal therapy reconsidered. J Endod. 2005;31:817–20.
Marending M, Paqué F, Fischer J, Zehnder M. Impact of irrigant sequence on mechanical properties of human root dentin. J Endod. 2007;33:1325–8.
Haapasalo M, Shen Y, Qian W, Gao Y. Irrigation in endodontics. Dent Clin North Amer. 2010;54:291–312.
Baumgartner JC, Ibay AC. The chemical reactions of irrigants used for root canal debridement. J Endod. 1987;13:47–51.
Sim TP, Knowles JC, Ng YL, Shelton J, Gulabivala K. Effect of sodium hypochlorite irrigant concentration on strain in teeth. Int Endod J. 2001;34:120–32.
Sum CP, Neo J, Kishen A. What we leave behind in root canals after endodontic treatment: some issues and concerns. Austr Endod J. 2005;31:94–100.
Qian W, Shen Y, Haapasalo M. Quantitative analysis of the effect of irrigant solution sequences on dentin erosion. J Endod. 2011;37:1437–41.
Niu W, Yoshioka T, Kobayashi C, Suda H. A scanning electron microscopic study of dentinal erosion by final irrigation with EDTA and NaOCl solutions. Int Endod J. 2002;35:934–9.
Basrani B, Santos JM, Tjäderhane L, Grad H, Gorduysus O, Huang J, Lawrence HP, Friedman S. Substantive antimicrobial activity in chlorhexidine-treated human root dentin. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94:240–5.
Basrani B, Tjäderhane L, Santos JM, Pascon E, Grad H, Lawrence HP, Friedman S. Efficacy of chlorhexidine- and calcium hydroxide-containing medicaments against Enterococcus faecalis in vitro. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:618–24.
Gomes BP, Souza SF, Ferraz CC, Teixeira FB, Zaia AA, Valdrighi L, Souza-Filho FJ. Effectiveness of 2 % chlorhexidine gel and calcium hydroxide against Enterococcus faecalis in bovine root dentine in vitro. Int Endod J. 2003;36:267–75.
Zamany A, Safavi K, Spangberg LS. The effect of chlorhexidine as an endodontic disinfectant. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:78–81.
Baca P, Junco P, Arias-Moliz MT, González-Rodríguez MP, Ferrer-Luque CM. Residual and antimicrobial activity of final irrigation regimens on Enterococcus faecalis-infected root canals. J Endod. 2011;37:1121–3.
Basrani BR, Manek S, Mathers D, Fillery E, Sodhi RNS. Determination of 4-chloroaniline and its derivatives formed in the interaction of sodium hypochlorite and chlorhexidine by using gas chromatography. J Endod. 2010;36:312–4.
Thomas JE, Sem DS. An in vitro spectroscopic analysis to determine whether para-chloroaniline is produced from mixing sodium hypochlorite and chlorhexidine. J Endod. 2010;36:315–7.
Krishnamurthy S, Sudhakaran S. Evaluation and prevention of the precipitate formed on interaction between sodium hypochlorite and chlorhexidine. J Endod. 2010;36:1154–7.
Nowicki JB, Sen DS. An in vitro spectroscopic analysis to determine the chemical composition of precipitate formed by mixing sodium hypochlorite and chlorhexidine. J Endod. 2011;37:983–8.
Basrani BR, Manek S, Sodhi RNS, Fillery E, Manzur A. Interaction between sodium hypochlorite and chlorhexidine gluconate. J Endod. 2007;33:966–9.
Dai L, Khechen K, Khan S, Gillen B, Loushine BA, Wimmer CE, et al. The effect of QMix, an experimental antibacterial root canal irrigant, on removal of canal wall smear layer and debris. J Endod. 2011;37:80–4.
Hülsmann M, Rümmelin C, Schäfers F. Root canal cleanliness after preparation with different endodontic handpieces and hand instruments: a comparative SEM investigation. J Endod. 1997;23:301–6.
Portney LG, Watkins MP. Foundations of Clinical Research. Nowak: Appleton and Lange. 1993; p. 357, 435–36.
Friedman M. A comparison of alternative tests of significance for the problem of rankings. Ann Math Stat. 1940;11:86–92.
Gaito J. Measurement scales and statistics: resurgence of an old misconception. Psycologic Bull. 1980;83:564–7.
Hasselkus BR, Safrit MJ. Measurement in occupational therapy. The Am J Occupat Therapy. 1976;30:429–36.
Goldman M, Goldman L, Cavaleri R, Bogis J, Lin P. The efficacy of several endodontic irrigating solutions: a scanning electron microscopic study: part 2. J Endod. 1982;8:487–92.
Yamada RS, Armas A, Goldman M, Lin PS. A scanning electron microscopic comparison of a high volume flush with several irrigating solutions: part 3. J Endod. 1983;9:137–42.
White RR, Goldman M, Lin PS. The influence of the smeared layer upon dentinal tubule penetration by plastic filling materials. J Endod. 1984;10:558–62.
Baumgartner JC, Mader CL. A scanning electron microscope evaluation of four root canal irrigation regimes. J Endod. 1987;13:147–57.
Sobhani OE, Gulabivala K, Knowles JC, Ng YL. The effect of irrigation time, root morphology and dentine thickness on tooth surface strain when using 5 % sodium hypochlorite and 17 % EDTA. Int Endod J. 2010;43:190–9.
Rajasingham R, Ng YL, Knowles JC, Gulabivala K. The effect of sodium hypochlorite and ethylenediaminetetraacetic acid irrigation, individually and in alternation, on tooth surface strain. Int Endod J. 2010;43:31–40.
Grawehr M, Sener B, Wltimo T, Zehnder M. Interactions of ethylenediaminetetraacetic acid with sodium hypochlorite in aqueous solutions. Int Endod J. 2003;36:411–5.
Gao Y, Haapasalo M, Shen Y, Gao Y. Development and validation of a three-dimensional fluid dynamics model of root canal irrigation. J Endod. 2010;35:1282–7.
Shen Y, Gao Y, Qian W, Ruse ND, Zhou X, Wu H, Haapasalo M. Three-dimensional numeric simulation of root canal irrigant flow with different irrigation needles. J Endod. 2010;36:884–9.
Pashley DH. Pulpodentin complex. In: Hargreaves KM, Goodis HE, editors. Seltzer and Bender’s Dental Pulp. Chicago, USA: Quintessence Publishing; 2002. pp. 63–94.
Paqué F, Luder HU, Sener B, et al. Tubular sclerosis rather than the smear layer impedes dye penetration into the dentin of endodontically instrumented root canals. Int Endod J. 2006;39:18–25.
Vasililadis L, Darling AI, Levers BG. The amount and distribution of sclerotic human root dentin. Arch Oral Biol. 1983;28:645–9.
Lottanti S, Gautschi H, Sener B, Zehnder M. Effects of ethylenediaminetetraacetic, etidronic, and peracetic acid irrigation on human root dentine and the smear layer. Int Endod J. 2009;42:335–43.
Safavi KE, Spångberg LS, Langeland K. Root canal dentinal tubule disinfection. J Endod. 1990;16:207–10.
Sen BH, Wesselink PR, Türkün M. The smear layer: a phenomenon in root canal therapy. Int Endod J. 1995;28:141–8.
Peters LB, Wesselink PR, Moorer WR. The fate and the role of bacteria left in root dentinal tubules. Int Endod J. 1995;28:95–9.
Peters LB, Wesselink PR, Buijs JF, van Winkelhoff AJ. Viable bacterial in root dentinal tubules of teeth with apical periodontitis. J Endod. 2001;27:76–81.
Buck RA, Eleazer PD, Staat RH, Sheetz JP. Effectiveness of three endodontic irrigants at various tubular depth in human dentin. J Endod. 2001;27:206–8.
Weiger R, de Lucena J, Decker HE, Löst C. Vitality status of microorganisms in infected human root dentine. Int Endod J. 2002;35:166–71.
Love RM, Jenkinson HF. Invasion of dentinal tubules by oral bacteria. Crit Rev Oral Biol Med. 2002;13:171–83.
Silva PV, Guedes DFC, Nakad FV, Pécora JD, Druz-Filho AM. Chitosan: a new solution for removal of smear layer after root canal instrumentation. Int Endod J. 2012;. doi:10.1111/j.1365-2591.2012.02119.x.
Cengiz T, Aktener BO, Pişkin B. The effect of dentinal tubule orientation on the removal of smear layer by root canal irrigants. A scanning electron microscopic study. Int Endod J. 1990;23:163–71.
Gutmann JL. Adaptation of injected thermoplasticized gutta-percha in the absence of the dentinal smear layer. Int Endod J. 1993;26:87–92.
Pallarés A, Faus V, Glickman GN. The adaptation of mechanically softened gutta-percha to the canal walls in the presence or absence of smear layer: a scanning electron microscopic study. Int Endod J. 1995;28:266–9.
Leiendecker AP, Qi YP, Sawyer AN, Niu LN, Agee KA, Loushine RJ, Weller RN, Pashley DH, Tay FR. Effects of calcium silicate-based materials on collagen matrix integrity of mineralized dentin. J Endod. 2012;38:829–33.
Sawyer AN, Nikonov SY, Pancio AK, Niu LN, Agee KA, Loushine RJ, Weller RN, Pashley DH, Tay FR. Effects of calcium silicate-based materials on the flexural properties of dentin. J Endod. 2012;38:680–3.
Ordinola-Zapata R, Bramante CM, Brandão Garcia R, Bombarda Andrade R, Bernardineli N, Gomes Moraes I, Duarte MAH. The antimicrobial effect of new and conventional endodontic irrigants on intra-orally infected dentin. Acta Odontol Scand. 2012;. doi:10.3109/00016357.2012.690531.
Acknowledgments
Dr. James L. Gutmann serves as a consultant for DENTSPLY Tulsa Dental Specialties and has no financial interest in the product or process addressed in the study. The other authors were not paid by DENTSPLY; research samples of QMix were provided by DENTSPLY for this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Eliot, C., Hatton, J.F., Stewart, G.P. et al. The effect of the irrigant QMix on removal of canal wall smear layer: an ex vivo study. Odontology 102, 232–240 (2014). https://doi.org/10.1007/s10266-012-0102-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10266-012-0102-1