
Abstract
Voriconazole (VRCZ) reportedly possesses a broad spectrum of antifungal activity against Aspergillus spp. and Candida spp., and the blood concentration of VRCZ is correlated with both the efficacy and the adverse effects of this drug. Monitoring of the blood concentration target level of VRCZ has not yet been widely adopted in the medical field, and no evidence concerning this target level has been reported. Accordingly, we used a meta-analysis to investigate the optimal blood concentration of VRCZ. Using data from 12 reports, we found that the success rate for fungal infection treatment increased significantly at VRCZ levels greater than 1.0 μg/ml when a graded cutoff value within the range of 1.0–3.0 μg/ml was used as the VRCZ trough blood concentration [odds ratio (OR) 7.23, 95% confidence interval (CI) 2.84–18.37, P < 0.0001]. Concerning the safety evaluation, the incidence of adverse neurological effects increased significantly at a cutoff value of 4.0 μg/ml when a graded cutoff value within the range of 3.0–6.0 μg/ml was used (OR 2.23, 95% CI 1.12–4.46, P = 0.02). However, in all 12 literature sources, an increasing incidence of liver dysfunction was reported at higher blood concentrations, and no accurate cutoff values were obtained. Consequently, a VRCZ trough blood concentration more than 1.0 μg/ml from the perspective of efficacy and less than 4.0 μg/ml from the perspective of safety is recommended.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Voriconazole (VRCZ) is a new triazole antifungal agent that was approved in Japan in April 2005. VRCZ addresses a broad spectrum of antifungal activity and also possesses superior antifungal effectiveness against Aspergillus spp., Candida spp., and Cryptococcus spp., as well as some other pathogenic fungi [1]. VRCZ is the first drug of choice for the treatment of invasive aspergillosis and chronic necrotizing pulmonary aspergillosis and is the second drug of choice for candidiasis and cryptococcosis, as mentioned in the guidelines for the diagnosis and treatment of deep mycosis (2007) [2]. Recently, the dosages and treatment methodologies for antifungal agents have been determined using pharmacokinetic/pharmacodynamic (PK/PD) theory. The efficacy of azole antifungal agents is reportedly correlated with the AUC/MIC [3, 4]. The metabolism of VRCZ is activated in the liver by CYP2C19, but the metabolic rate depends on genetic polymorphisms of CYP2C19. CYP2C19 polymorphisms are known to include a poor metabolizer (PM), a heterozygous extensive metabolizer (HEM), an extensive metabolizer (EM), and an ultrarapid metabolizer (URM). Reportedly, 19% of the Japanese population is considered to carry the PM polymorphism [5, 6]. As a result, the metabolism of VRCZ can be delayed, and the blood concentration can be higher than expected in some Japanese populations. In Japan in 2008, VRCZ became a target drug for therapeutic drug monitoring (TDM). Package inserts for the drug advise that blood concentration monitoring should be performed during the VRCZ administration period, but TDM for VRCZ has not yet become widespread in clinical settings. Recent literature has occasionally addressed the subject of VRCZ blood concentrations, but neither a definite opinion concerning blood concentrations and clinical efficacy nor a definite indicator concerning the target blood concentration has been mentioned. In the present study, we performed descriptive research using a meta-analysis method to examine the need for TDM during VRCZ therapy for deep mycosis.
Materials and methods
Database search and criteria for adopting data
To evaluate the relationship between VRCZ and its blood concentration as well as the efficacy and safety of the drug when administered to patients with deep mycosis, we searched medical databases for articles regarding the administration of VRCZ and blood concentrations of this drug. We searched for sources using the keywords ‘Voriconazole,’ ‘level,’ and ‘concentration’ using the MEDLINE (1966–April 2009) and Igakuchuozasshi, Ichushi-Web, Japan Medical Abstract Society (1983–April 2009) databases. We also manually conducted research to obtain further details using these databases. Afterward, we carefully examined the titles of the selected data as well as their synopses and contents. We finally selected all the reports from which data regarding the blood concentrations of VRCZ and its efficacy and safety could be extracted. For reports that did not contain extractable data, we sent a request to the authors of the reports that they disclose their data in detail.
Outcome setting
The primary emphasis of our study was to examine the efficacy and safety of VRCZ as well as its blood concentration. The method used to evaluate drug efficacy was defined based on the methods used in each of the extracted reports and included cases with clinical improvement. Liver dysfunction and neurological adverse effects were extracted from the data as indicators of the drug’s safety. As for the definition of liver dysfunction, we used the CTCAE criteria, version 3 [7], when no other definition was provided in the extracted study. Liver dysfunction was regarded as being present when the grade of a liver function test value (AST, ALT, ALP, γ-GTP, or Bil) increased beyond the values obtained before and after drug administration. Neurological adverse effects were defined as auditory and visual hallucinations and visual disorders. When treating the extracted data as a continuous variable, we calculated the weighted mean difference (WMD) of the outcome with a 95% confidence interval (CI). We also calculated the odds ratio (OR) and 95% CI when setting the cutoff value and treated both values as variable numbers.
Cutoff value setting
According to the most recent report, the minimum inhibitory concentration (MIC) of VRCZ against Aspergillus spp. and Candida spp. is between 0.5 and 1 μg/ml [2, 8]. Some studies have reported that drug efficacy increases when the trough concentration is more than 1.0 μg/ml, while others have reported that efficacy increases when the trough concentration is more than 2.0 μg/ml. Accordingly, we set the stepwise cutoff value for efficacy at between 1.0 and 3.0 μg/ml and examined the values. For drug efficacy, we set the cutoff value for safety at between 3.0 and 6.0 μg/ml and examined the safety in a stepwise manner, because some sources stated that the maximum value should be between 4.0 and 6.0 μg/ml. We extracted the blood concentrations for every 1.0 μg/ml and constructed a regression curve using blood concentration as an independent variable and the outcome incidence rate as a dependent variable.
Sensitivity analysis (examination of factors that could affect the outcome)
To examine factors that could affect blood concentration, we analyzed sensitivity relative to dosage, sex, age, and method of administration. For age, we divided the subjects into two groups: patients over 60 years and patients under 60 years of age. For dosage, we also divided the subjects into two groups: a high-dosage group and an ordinary dosage group. The former group consisted of patients with a dosage of more than 8 mg/kg/day. As an indicator of the blood concentration, we used the blood concentration (μg/ml) and the dosage (mg/day) to avoid a bias in the dosage amount. We also examined the relevance of sex, age, and dosage to the outcome incidence.
Statistical analysis
Statistical analysis was performed using the blood concentration, efficacy, and safety, which were extracted from each study. Review Manager 5.0 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration) was used to integrate the study results using a meta-analysis method. The Mantel–Heanzel method and the inverse variance method were used to calculate the OR, WMD, and 95% CI for each study. To examine the homogeneity of each study, a heterogeneity test was used; a value of P < 0.1 was considered to indicate statistical inhomogeneity. If homogeneity was identified, additional analyses using the fixed-effect model were performed. If inhomogeneity was identified, the random-effect model was used for the analysis. Furthermore, the regression analysis described by Egger et al. [9] was used against the disclosed bias. JMP 8 was used for the other analyses.
Results
Database search results
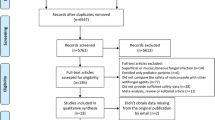
Having searched MEDLINE using the keywords ‘Voriconazole,’ ‘level,’ and ‘concentration,’ we obtained 196 data results. We also searched Igakuchuozasshi, Ichushi-Web, Japan Medical Abstract Society, and obtained 41 data results. We adopted 13 of these results, eliminating reports without blood concentration data, those reports in which the blood concentrations were not extractable, those containing general remarks or case reports only, and those without statements concerning efficacy or safety [10–21] (Table 1). Twelve of these 13 reports, consisting of nine original articles and three articles in abstract form, involved the treatment of deep mycosis, such as aspergillosis and candidiasis. The last of the 13 articles contained insufficient data for our analysis. Regarding the backgrounds of these 12 articles, 8 involved compromised hosts, such as posttransplantation patients and subjects with hemopathy. One of the 12 articles concerned with patients with respiratory disorders. The remaining 3 reports did not include such information. Ten articles included the trough blood concentration, but 1 article did not include such information (the 12th article). Two articles contained details regarding the combination of antifungal agents and antibacterial agents.
Evaluation of efficacy and safety outcome data according to VRCZ blood concentrations (continuous data)
To evaluate the blood concentration as well as the efficacy and safety of VRCZ, we examined the difference between blood concentrations with examination outcomes and blood concentrations without outcomes. Seven reports considered blood concentration as a continuous variable. We examined the relationship between the blood concentration and both the efficacy and safety of VRCZ using these seven reports. The difference between the VRCZ trough blood concentrations in the effectively treated group and the ineffectively treated group was not significant. However, the incidence of efficacy tended to increase at higher trough blood concentrations (WMD 1.95, 95% CI −2.18 to 1.84, P = 0.35) (Table 2). We also examined the relationship between the blood concentration and adverse drug effects in a similar manner. Higher incidences of liver dysfunction and neurological adverse effects tended to be seen at higher trough blood concentrations (liver dysfunction: WMD 1.73, 95% CI 0.33–3.79, P = 0.10; neurological adverse effects: WMD 0.26, 95% CI −0.40 to 0.93, P = 0.44) (Table 2).
Evaluation of VRCZ blood concentration cutoff values for outcome efficacy and safety (dichotomous data)
We set the stepwise cutoff values for the trough blood concentration within a range of 1.0 μg/ml and 3.0 μg/ml and compared the efficacy rates for values above and below the cutoff values. An analysis using four reports indicated that the efficacy against fungal infections increased significantly at a cutoff of 1.0 μg/ml (OR 7.23, 95% CI 2.84–18.37, P < 0.0001) (Table 3). Furthermore, we investigated the optimal blood concentration of VRCZ only against Aspergillus spp. in the present meta-analysis. The success rate for the eradication of fungal infections increased significantly at values greater than 1.0 μg/ml VRCZ (OR 8.62, 95% CI 1.98–37.50, P = 0.004) when graded cutoff values within the same range as already mentioned were used. To evaluate safety, we set the stepwise cutoff value within the range 3.0–6.0 μg/ml. Regarding safety, ten reports examining liver dysfunction and six reports mentioning adverse effects were found. Using these reports, we examined the incidence of adverse effects for values above and below the cutoff value. The incidence of liver dysfunction increased using cutoff rates (Table 4). For neurological adverse effects, the increase in incidence for values greater than 4.0 μg/ml was significant (OR 2.23, 95% CI 1.12–4.46, P = 0.02) (Table 5).
We plotted regression curves for liver dysfunction and neurological adverse effects using blood concentration as an independent variable and outcome incidence as a dependent variable (Fig. 1a, b). The regression curve for the incidence of liver dysfunction (y = 6.0628e0.2481x, P < 0.01, Fig. 1a) and the incidence of neurological adverse effects (y = 14.829e0.5863x, P = 0.054) are shown in Fig. 1b.

a Regression curve for the incidence of liver dysfunction and voriconazole (VRCZ) concentration. b Regression curve for the incidence of neurological adverse effects and VRCZ concentration. We extracted liver dysfunction and neurological adverse effect outcomes as a dependent variable and the blood concentration for every 0–10 μg/ml (see Table 5) and constructed regression curves with blood concentration as an independent variable. Statistical analysis was performed using the Spearman rank-order correlation coefficient
Sensitivity analysis of factors affecting outcome
A factor analysis revealed that the VRCZ blood concentration and dosage were significantly affected by the sex and age of the subjects. We compared the blood concentrations and dosages in both sexes and found that these factors were significantly higher in male patients (WMD 1.97, 95% CI 0.26–3.69, P = 0.02). We also found that these factors were significantly higher in patients over the age of 60 years (WMD 4.53, 95% CI 0.20–8.86, P = 0.04) (Table 6). No correlation between sex and age was found in any of the extracted reports or the present meta-analysis. We also examined the relationship between trough blood concentration and dosage among the collected samples. No significant correlation between these parameters was found (Spearman rank correlation) (data not shown). Furthermore, having examined the factors that could possibly affect the outcome, we obtained no significant variance in age, sex, or dosage (data not shown).
Examination of disclosed bias
We tested the disclosed bias (Tables 2, 3, 4, 5) using the regression analysis reported by Egger et al. The results did not support the hypothesis that Tables 2, 3, 4, and 5 reveal a disclosed bias.
Discussion
Many of the patients in the extracted reports were immunocompromised hosts with hematological or posttransplant disorders. The incidence of deep mycosis in compromised hosts has been increasing and is a serious matter. Therefore, the appropriate selection of antifungal agents and appropriate dosage settings are necessary. For example, compromised hosts are frequently treated with multiple drugs, immunosuppressive agents, or antibacterial agents. In such cases, topics such as drug-to-drug interactions and drug safety require discussion. The package inserts indicate that VRCZ interacts with various drugs, and these interactions may cause unexpected variations in blood concentrations of VRCZ.
According to Tan et al. [22], the incidence of adverse effects, such as liver dysfunction and abnormal vision, was dependent on the blood concentration. The present analysis indicated that the incidence of liver dysfunction increased at higher trough concentrations. Reportedly, not only the incidence of liver dysfunction, but also the incidence of neurological adverse effects, is correlated with the blood concentration. According to reports by Pascual et al. [15] and Imhof et al. [16], neurological adverse effects such as abnormal vision were detected in patients with a high trough concentration. The present analysis confirmed a significant incidence of adverse effects at concentrations greater than 4.0 μg/ml, and the incidence of neurological adverse effects tended to increase at higher trough concentrations. Because the data presently used did not adequately describe the neurological adverse effects, we did not examine levels greater than 7.0 μg/ml. Hallucinations are known to accompany visual agnosia (“abnormal vision”), so both blood concentration and patient monitoring are of importance.
According to a review performed by Niki et al. of patients treated for mycoses, no significant difference in trough concentrations was found between the effectively treated group and the ineffectively treated group. Furthermore, clinical efficacy for the treatment of deep mycoses was related not only to the blood concentrations of drugs, but also to various other factors including tissue transition, drug sensitivity of pathogenic fungi, and host immunity, as well as the underlying disease [23]. According to Ueda et al., no correlation between blood concentration and drug efficacy was found. However, a correlation between drug efficacy and the trough concentration was indicated when patients with intractable homeopathy were excluded [12]. These results showed that there was no difference in the blood concentration in the effectively treated group and the ineffectively treated group. A more detailed examination revealed the fact that trough concentrations greater than 1.0 μg/ml increased the drug efficacy rate. A further study of blood concentrations in patients infected with the pathogenic fungi Aspergillus spp. produced similar results, with a cutoff value of 1.0 μg/ml. For medical treatment, a standard value of 1.0 μg/ml has been established and was confirmed as our criterion. Under these circumstances, controlling blood concentration is essential.
VRCZ is metabolized primarily by liver CYP2C19, but the metabolic activity varies according to the CYP2C19 genotype [6]. The enzyme deficiency rate/partial deficiency rate of Japanese people is known to be higher than those of Europeans and Americans. Enzyme activity also reportedly varies according to sex [13, 24]. Therefore, the blood concentrations may be higher than expected in some populations [5]. Extensive metabolizers (EM) and poor metabolizers (PM) are known to have about a fourfold difference in their blood concentrations. Our analytical study indicated that the blood concentration/dosage among male patients was significantly higher than that among female patients. When the patients were divided into two groups according to age, the blood concentration/dosage in patients over 60 years old was higher than that in the younger group. Accordingly, not only the patients’ weight, as advised by the drug pamphlet, but also other patient characteristics should be considered when planning and adjusting dosages for individual patients.
A meta-analysis is an established quantitative approach to obtaining scientific evidence and is a respected epidemiological field of study. It is especially useful when effective results are not obtained or when research results differ. A limitation of meta-analyses is that they can result in a disclosed bias. Because of this, we conducted our research not only with the extracted reports but also using papers and abstracts from medical societies. We evaluated the closed documentary materials among the references used for our analysis using the regression analysis reported by Egger et al. [9]. The results did not support the hypothesis that Tables 2, 3, 4, and 5 indicated a disclosed bias, because the measurement of VRCZ blood concentrations is not yet widely performed, so the available information remains insufficient. However, no statistically significant differences were noted in more than half these analytical results. Therefore, the bias influence would be small if a disclosed bias does indeed exist in the other analytical results. When performing a meta-analysis, the general custom is to perform a sensitivity analysis for drugs, as research data can be difficult to analyze while considering effective factors and confounding factors. We examined the dosages, the methods of administration, sex, and age, regarding them as candidates for confounding factors, but data concerning preexisting diseases, racial classifications, concomitant drugs, or infectious pathogenic fungi were not possible to extract. Therefore, further examination of these points was not made. In addition, the outcome setting among each study was not standardized, limiting the present study.
Regarding VRCZ and its blood concentration, only a general review has so far been reported, and no integrated analyses have been performed. Using a meta-analysis in the present study, we obtained integrated evidence as well as more accurate indicators of the trough concentration. In conclusion, we believe that it may be desirable to set the blood concentration target level at more than 1.0 μg/ml to improve drug efficacy and at less than 4.0 μg/ml to ensure treatment safety when measuring VRCZ blood concentrations during treatment for deep mycosis. However, L-AMB may be preferable to TDM [25] because the VRCZ blood concentration may vary greatly among individuals.
Our investigation included an investigation of the optimum blood concentration using a meta-analysis, but a detailed analysis according to pathological condition or bacterial strain was not performed. These details are likely to be important, and future studies are needed.
References
Epinel-Ingroff A. In vitro activity of the new triazole voriconazole (UK-109, 494) against opportunistic filamentous and dimorphic fungi and common and emerging pathogens. J Clin Microbiol. 1998;36:198–202.
Deep-Seated Mycosis Guidelines Editorial Committee. Guidelines for management of deep-seated mycosis 2007. Tokyo: Kyowakikaku; 2007 (in Japanese).
Goodwin ML, Drew RH. Antifungal serum concentration monitoring: an update. J Antimicrob Chemother. 2008;61:17–25.
Andes D, Marchillo K, Stamstad T, Conklin R. In vivo pharmacokinetics and pharmacodynamics of a new triazole, voriconazole, in a murine candidiasis model. Antimicrob Agents Chemother. 2003;47:3165–9.
Wood N. Pharmacokinetics of Voriconazole. Jpn J Chemother. 2005;53:16–23.
Wang G, Lei HP, Li Z, Tan ZR, Guo D, Fan L, et al. The CYP2C19 ultra-rapid metabolizer genotype influences the pharmacokinetics of voriconazole in healthy male volunteers. Eur J Clin Pharmacol. 2009;65:281–5.
Common Terminology Criteria for Adverse Events (CTCAE) v3.0. http://www.jcog.jp/.
Yamaguchi H. Antifungal activity of voriconazole. Jpn J Chemother. 2005;53:8–15.
Egger M, Davey SG, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Matsumoto K, Ikawa K, Abematsu K, Fukunaga N, Nishida K, Fukumizu T, et al. Correlation between voriconazole trough plasma concentration and hepatotoxicity in patients with different CYP2C19 genotypes. Int J Antimicrob Agents. 2009;34:91–4.
Hagiwara E, Shiihara J, Matsushima A, Enomoto T, Tagawa A, Sekine A, et al. Usefulness of monitoring plasma voriconazole concentration in patients with chronic necrotizing pulmonary aspergillosis. Nihon Kokyuki Gakkai Zasshi. 2009;47:93–7.
Ueda K, Nannya Y, Kumano K, Hangaishi A, Takahashi T, Imai Y, et al. Monitoring trough concentration of voriconazole is important to ensure successful antifungal therapy and to avoid hepatic damage in patients with hematological disorders. Int J Hematol. 2009;89:592–9.
Shimoeda S, Nakazawa K, Kobayashi H, Nakagawa S, Yamato S, Sasaki M, et al. Clinical significance of measuring serum concentrations of voriconazole in the hematological field. Jpn J Pharm Health Care Sci. 2008;34:638–43.
Okuda T, Okuda A, Watanabe N, Takao M, Takayanagi K. Retrospective serological tests for determining the optimal blood concentration of voriconazole for treating fungal infection. Yakugaku Zasshi. 2008;128:1811–8.
Pascual A, Calandra T, Bolay S, Buclin T, Bille J, Marchetti O. Voriconazole therapeutic drug monitoring in patients with invasive mycoses improves efficacy and safety outcomes. Clin Infect Dis. 2008;46:201–11.
Imhof A, Schaer DJ, Schanz U, Schwarz U. Neurological adverse events to voriconazole: evidence for therapeutic drug monitoring. Swiss Med Wkly. 2006;136:739–42.
Obata Y, Takada T, Tamura K. Zoukishikkan wo Kisosikkan tosita Shinsyusei Aspergillus reiniokeru Voriconazole no Yakubutukettyuunoudo Monitoring to Rinsyokouka. Jpn J Chemother. 2008;56:172.
Yoshida H, Sawada K, Tuzuki K, Suzumura Y, Oohira Y, Yoneyama E, et al. Voriconazole no TDM. Zisshi No Igi (Jpn J Pharmacol Ther). 2007;38:S239.
Takakura S, Sawada K, Fujiwara N, Saitoh T, Itoh Y, Iiinuma Y, et al. Voriconazole Kettyuu Noudo Monitoring no Hituyousei. Jpn J Chemother. 2006;54:56.
Denning BW, Ribaud P, Milpied N, Caillot D, Herbrecht R, Thiel E, et al. Efficacy and safety of voriconazole in the treatment of acute invasive aspergillosis. Clin Infect Dis. 2002;34:563–71.
Smith J, Safdar N, Knasinski V, Simmons W, Bhavnani SM, Ambrose PG, et al. Voriconazole therapeutic drug monitoring. Antimicrob Agents Chemother. 2006;50:1570–2.
Tan K, Brayshaw N, Tomaszewski K, Troke P, Wood N. Investigation of the potential relationships between plasma voriconazole concentrations and visual adverse events or liver function test abnormalities. J Clin Pharmacol. 2006;46:235–43.
Niki Y, Yoshida M, Shimada K, Kohno S, Masaoka T, Yamaguchi H, et al. A clinical trial of voriconazole for deep-seated mycosis. An uncontrolled multicenter study. Jpn J Chemother. 2005;53:32–50.
Parkinson A, Mudra DR, Johnson C, Dwyer A, Carroll KM. The effects of gender, age, ethnicity, and liver cirrhosis on cytochrome P450 enzyme activity in human liver microsomes and inducibility in cultured human hepatocytes. Toxicol Appl Pharmacol. 2004;199:193–209.
Hamada Y, Komatsu T, Seto Y, Matsubara H, Kume H, Sunakawa K, et al. Liposomal-amphotericin B efficacy and safety. J Jpn Assoc Infect Dis. 2010;84:193–8.
Acknowledgments
We wish to express our deep gratitude to each of the authors who contributed their valuable time in providing the databases necessary for this study.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Hamada, Y., Seto, Y., Yago, K. et al. Investigation and threshold of optimum blood concentration of voriconazole: a descriptive statistical meta-analysis. J Infect Chemother 18, 501–507 (2012). https://doi.org/10.1007/s10156-011-0363-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10156-011-0363-6