
Abstract
Radiotherapy plays an important role in the treatment of various malignancies, and intensity-modulated radiotherapy (IMRT) is an attractive option because it can deliver precise conformal radiation doses to the target while minimizing the dose to adjacent normal tissues. IMRT provides a highly conformal dose distribution by modulating the intensity of the radiation beam. A number of malignancies have been targeted by IMRT; this work reviews published data on the major disease sites treated with IMRT. The dosimetric advantage of IMRT has resulted in the significant reduction of adverse effects in some tumors. However, there are few clinical trials comparing IMRT and three-dimensional conformal radiotherapy (3D-CRT), and no definite increase in survival or the loco-regional control rate by IMRT has been demonstrated in many malignancies. IMRT also requires greater time and resources to complete compared to 3D-CRT. In addition, the cost–effectiveness of IMRT versus 3D-CRT has not yet been established.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Precise radiotherapy techniques including three-dimensional conformal radiotherapy (3D-CRT), stereotactic radiotherapy, intensity-modulated radiotherapy (IMRT), and image-guided radiotherapy (IGRT) have been developed in recent decades with the rapid development of computer technology and radiation physics. Shinji Takahashi was one of the pioneers of this field, and conformal radiotherapy was achieved in Japan in the 1960s using rotating multileaf collimators (MLCs) [1]. In the 1990s, with the development of the more sophisticated IMRT, these conformal techniques were overtaken by inverse treatment-planning procedures.
IMRT provides highly conformal dose distribution by modulating the intensity of the radiation beam. IMRT can deliver precise radiation doses to the target while minimizing the dose to adjacent normal tissues. Typically, IMRT delivery is performed by conventional MLC-mounted linear accelerators. To create non-uniform dose intensity, there are three different types of IMRT delivery using conventional linear accelerators: step-and-shoot, sliding window, and volumetric modulated arc therapy (VMAT). In step-and-shoot IMRT, small MLC-generated segments are used for dose delivery, and radiation is not delivered while the leaves move to create the next segment. Sliding-window IMRT uses modulated MLC velocity to change the beam intensity in multiple static radiation fields, and the radiation is delivered as the leaves are moving. VMAT is one of the rotational forms of IMRT with moving MLC and changing dose rates during rotational dose delivery. In general, VMAT offers more conformal dose distributions and faster treatment times [2].
A helical tomotherapy unit is a completely dedicated rotational IMRT machine with a megavoltage computed tomography (CT) detection system. Tomotherapy delivers narrow intensity-modulated beams in a helical manner as they are rotated around the patient. The CyberKnife is a stereotactic radiation machine in principle, but the dose intensity for the target can be modulated. A CyberKnife can deliver multiple narrow beams from non-coplanar and non-isocentric angles, and the dose delivery has excellent dose conformality and steep dose gradients.
To deliver a highly conformal radiation dose by IMRT, it is necessary to secure geometrical precision. The administration of IMRT is often accomplished with an image-guidance-capable system using on-board cone-beam CT, in-room CT, ultrasonography, or other optical image techniques.
These sophisticated techniques have spread rapidly and widely around the world. IMRT has opened a new era in radiation oncology, and it will be one of the standard radiotherapy practices for many tumors in the near future [3].
This work reviews the published data with regard to the major malignancies treated with IMRT. Potential disadvantages of IMRT are also discussed.
Clinical perspective
Brain
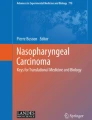
IMRT could be highly attractive for the treatment of brain tumors because brain tumors frequently occur in an area close to several radiosensitive normal tissues (Fig. 1). In particular, the simultaneous integrated boost (SIB) technique using IMRT, which delivers different doses to the gross tumor volume and sub-target surrounding the primary tumor, is promising in the treatment of glioblastomas (GBMs). GBMs are considered to have a low α/β ratio, and the potential benefit of administering hypofractionated regimens with the SIB technique has been explored [4, 5]. Amelio et al. [4] summarized in their review that IMRT is clearly better than 3D-CRT in terms of dose conformity and sparing of organs-at-risk (OARs), although 3D-CRT and IMRT provide similar dosimetric results in terms of target coverage. However, there are no definite data to suggest that this dosimetric benefit will translate into a clinical advantage. Amelio et al. [4] concluded that hypofractionated IMRT with temozolomide in GBM patients with a good prognosis may be somewhat beneficial, although this must be confirmed by properly designed trials.

Example of axial dose distribution by intensity-modulated radiotherapy for a patient with a postoperative anaplastic meningioma
Hippocampus sparing in whole-brain radiotherapy using IMRT is also challenging. The development of neurocognitive decline is observed in a portion of patients after whole-brain radiotherapy. Although techniques for hippocampus sparing have been demonstrated in some papers, there are limited available data showing the clinical benefits [6].
Head and neck
One of advantages of IMRT for head and neck lesions is that with IMRT clinicians can increase the therapeutic ratio in tumors close to the critical organs, such as the brain stem and optic nerves. IMRT also allows sparing of the anatomical structures involved in swallowing [7]. Xerostomia is not a critical symptom, but it can be very inconvenient for a long period. Retrospective and prospective studies have shown that IMRT resulted in a decrease in xerostomia compared to 3D-CRT [8, 9], with improved quality of life.
Classically, in the 3D-CRT treatment plans, patients with head and neck cancer are irradiated using sequential radiotherapy plans to treat smaller boost fields from larger fields to elective nodal areas, which is known as a “shrinking-field approach.” IMRT has opened a new window for the SIB technique, which enables the simultaneous delivery of individualized dose levels to the targets and elective nodal areas within a single treatment fraction [10]. This technique may have some advantages for head and neck cancer: the possibility of dose escalation to the targets, thus decreasing the overall time of the treatment by moderating treatment acceleration.
Dose painting or biologically conformal radiotherapy is also a promising technique, in which the dose is increased in the radioresistant parts of tumors and decreased in the radiosensitive parts, to improve tumor control [11]. However, there are no definite data on the superiority of IMRT for head and neck tumors from the point of disease control. In addition, the proper delivery of IMRT requires sufficient knowledge of the complex anatomy of the head and neck region. A thorough understanding of local and regional tumor spread is also required. Adaptive radiotherapy customizing the radiation plan in response to anatomical changes during treatment may be necessary to ensure that the prescribed dose is actually delivered to the targets. Large clinical trials are needed to clarify the effectiveness of IMRT over 3D-CRT in head and neck cancer treatment.
Breast
Postoperative radiotherapy has been a part of the standard process of breast-conserving therapy after lumpectomy for many years, supported by a large amount of evidence [12]. Standard radiotherapy provides two tangential opposed fields with wedges. However, conventional irradiation may produce hot areas in the dose distribution, because the shape of the breast is complex. IMRT for the breast can produce a more uniform dose distribution, resulting in a possible reduction of adverse effects. As for acute toxicity, Freedman et al. [13] reported that breast IMRT was associated with significant improvement in grade 2 and 3 dermatitis, a finding that is supported by another study [12]. However, only a few retrospective reports exist on the decrease in late toxicities with less follow-up for patients receiving IMRT [13]. Moreover, if breast cancer-related outcomes are the main outcome of interest, there seems to be no evidence of a difference in local recurrence rates between IMRT and conventional tangential radiotherapy. Further studies on late toxicities and disease control are needed, with longer follow-ups.
Lung
Conventional radiotherapy is frequently performed for lung cancer with a total dose of 60 Gy in 30 fractions in combination with chemotherapy, and excellent local control is not achieved in many cases. Although the higher radiation doses to the tumor lead to a better chance of local control, there may be difficulties due to the toxicities of the normal tissues. IMRT can deliver higher conformal doses to the target while sparing surrounding OARs. However, there are some potential problems with the use of IMRT for lung tumors: target motion and the potential toxicity of a lower dose to larger volumes of the lung.
In the reports of dosimetric comparisons between IMRT and 3D-CRT, standard toxicity parameters such as V20 (the percentage of lung volume receiving 20 Gy or more) are improved by IMRT [14]. However, greater lung volumes would receive a lower dose because IMRT needs larger monitor units and a larger number of beam directions. Several reports have mentioned the need for caution regarding these larger volumes of lower-dose irradiated lung, as critical radiation pneumonitis has been reported in conjunction with IMRT for lung cancer [15]. Thus, in addition to the standard lung toxicity parameters, other parameters such as V5 and V10, which are related to lower-dose irradiated lung volumes, may be more clinically relevant.
Respiratory motion is another issue for thoracic IMRT [16]. Typically, radiotherapy is delivered with the patient breathing normally. Although four-dimensional CT-based planning to incorporate the tumor motion within the target volume has been introduced in clinical practice, dose calculations are carried out on a static data set. In patients treated with IMRT, the effect of tumor motion may lead to a different dose actually being delivered in another phase. With greater target movement, the potential risk of a mismatch between the planned and delivered doses may become larger. For tumors with a greater amount of respiratory motion, a respiratory gating technique or abdominal compression is required to reduce this mismatch of dose delivery.
As for tumor control, there are no randomized trials comparing the tumor control provided by IMRT and 3D-CRT as radiotherapy for lung tumors, although Jiang et al. [17] reported in their retrospective analysis on the improvement of toxicities and favorable outcomes with IMRT. In a review Bezjak et al. [16] stated that the currently available data are insufficient to fully determine the clinical advantages of IMRT.
Prostate
It is well known that disease control in prostate cancer is dependent on the radiation dose [18, 19]. Randomized controlled trials and retrospective large series have confirmed the benefit of dose escalation, in particular, for the improvement of biochemical tumor control. IMRT provides concave dose distributions according to the shape of the prostate and seminal vesicles, and allows a safe dose escalation to the target while minimizing the dose to the bladder and the rectum. Therefore, even in the absence of definitive randomized control studies comparing IMRT with 3D-CRT, IMRT has increasingly been adopted as the standard radiotherapy technique for prostate cancer, with favorable results in large institutional series [18, 20, 21]. In guidelines, IMRT is recommended for the radical external radiotherapy of prostate cancer where an escalated radiation dose greater than 70 Gy dose is required [21].
The role of pelvic radiotherapy in the management of high-risk prostate cancer remains controversial [21]. The SIB technique, which simultaneously delivers a high dose to the prostate and a lower dose to the pelvic nodes, is promising [22]. The role of IMRT for pelvic nodes in the treatment of prostate cancer remains an area for continued investigation.
Hypofractionated IMRT is another challenge for prostate cancer. Since the α/β ratios for prostate cancer are much lower than those of other malignant tumors, prostate cancer may be highly sensitive to fraction size. Several large randomized trials comparing conventional fractionation to hypofractionation, typically using image-guided techniques, are ongoing [23]. However, it should be noted that at present hypofractionated IMRT should be used only in the context of clinical trials.
In the postoperative setting, some studies demonstrated that IMRT achieved decreased late toxicity rates [24], but there were insufficient data to indicate that IMRT is superior to 3D-CRT [21, 25].
Uterus
In radiotherapy for gynecological cancers, there are four main OARs: the small bowel, bladder, rectum, and bone marrow [26]. The dosimetric benefits of IMRT have resulted in the reduction of both gastrointestinal (GI) and genitourinary (GU) toxicities [26]. Gandhi et al. [27] also reported that IMRT decreased the incidence rate of acute and late GI toxicities compared to 3D-CRT, with comparable clinical outcomes. IMRT may also be beneficial for the reduction of hematological toxicities due to the decrease in the irradiated volume of bone marrow, which was shown by the results of the Radiation Therapy Oncology Group (RTOG) 0418 trial [28]. Regarding treatment outcomes in the postoperative setting, disease-related outcomes appear to be similar for IMRT and 3D-CRT [29], although no randomized comparisons of IMRT to 3D-CRT techniques in this context are available.
One of the promising areas for gynecological IMRT is the boost approach for nodal disease [26]. An additional 10–15 Gy to involved nodes may be achieved safely, with the dose to the small bowel limited to 45–50 Gy.
An issue in the use of IMRT for gynecological cancers is the effect of inter- and intra-fraction motion on targets and OARs. Organ motion patterns are reported to be patient-specific, with some having large shifts (~40 mm) of the target volume [30]. In cases without surgery, the significant tumor regression during radiotherapy may be also a problem linked to IMRT delivery. These possibilities may present the risk of tumor underdosing or increased dose to normal tissues.
Spinal metastasis
Advanced cancer patients frequently develop spinal bone metastases. Conventional radiotherapy with total doses of 8–30 Gy in 1–10 fractions is the current standard for spinal metastases; however, the dose escalation is limited because of the tolerance of the spinal cord. IMRT generates highly conformal dose distributions, and image guidance enables a precise treatment delivery. This treatment for spinal metastases is preferably called “stereotactic body radiosurgery/radiotherapy,” because total doses ranging from 20 to 30 Gy are fractionated into fewer fractions and rigid spine immobilization is required. Stereotactic body radiotherapy has proven to be an efficient alternative to conventional radiotherapy, in particular for patients with restricted spinal metastasis [31], although a higher risk of vertebral compression fractures was reported [32].
Potential disadvantages
As noted above, there are several disadvantages of IMRT that should be considered. First, the complexity of IMRT delivery results in a greater consumption of resources compared to 3D-CRT techniques. Much more time is required for the radiation physicist and oncologist to contour the targets and OARs and to make an appropriate treatment plan. Multiple iterations are often required before an optimal plan is achieved. The radiation beam delivery is also more complex, requiring more time for quality control and assurance protocols to confirm the quality of the treatment. IMRT also needs more expensive and sophisticated treatment-planning software and related systems. This increased complexity has strained the resources of radiation departments.
Second, inter-observer variability regarding the contouring is an issue, because IMRT generates a highly conformal dose distribution to the targets. It is well known that there is significant inter-observer variability in the contouring at various disease sites. Consensus guidelines must be published and practice is required for the appropriate contouring of the targets.
Third, with the increased accuracy of radiation delivery, a greater incorporation of motion is necessary to prevent marginal misses. Immobilization must be certain and precise to minimize positioning errors. In most cases, expensive image-guidance-capable systems are required to confirm the position of the target in daily setups and/or during irradiation. IMRT treatments are thus more costly to provide.
There are many analyses of cost–effectiveness comparing IMRT with 3D-CRT, some favorable to IMRT [33] and others unfavorable [34]. Variations exist between countries in the determination of cost estimates, depending in part on healthcare billing practices. The cost–effectiveness of IMRT versus 3D-CRT should be properly evaluated.
Finally, because of the greater leakage and scattered radiation in IMRT compared to 3D-CRT, there are theoretical concerns about an increased risk of radiation-induced secondary primary cancer. It has been estimated that the incidence of secondary malignancies by IMRT compared with 3D-CRT may increase from 1 to 1.75 % for patients surviving for 10 years [35]. In particular, there are special concerns in patients with pediatric cancer. Although the actual increase in the incidence of secondary primary cancer by IMRT is not well demonstrated, it should be noted that a small increased risk of secondary primary cancer has been observed in irradiated prostate cancer patients compared to a non-irradiated population in several studies [36].
Conclusion
IMRT requires greater time and resources to complete than 3D-CRT. For planners, treatment planning has become a more time-consuming process with IMRT. IMRT also requires more quality assurance steps to maintain the performance of the radiotherapy delivery system. The dosimetric advantage of IMRT has resulted in the reduction of adverse effects in some tumors. However, no increase in survival or the loco-regional control rate has been clearly demonstrated in many malignancies. Although there is a definite dosimetric advantage of IMRT, clinicians should be aware of these uncertainties and use caution when choosing IMRT.
References
Fraass BA (1995) The development of conformal radiation therapy. Med Phys 22:1911–1921
Teoh M, Clark CH, Wood K et al (2011) Volumetric modulated arc therapy: a review of current literature and clinical use in practice. Br J Radiol 84:967–996
Tomita N, Kodaira T, Teshima T et al (2014) Japanese structure survey of high-precision radiotherapy in 2012 based on institutional questionnaire about the patterns of care. Jpn J Clin Oncol. doi:10.1093/jjco/hyu041
Amelio D, Lorentini S, Schwarz M et al (2010) Intensity-modulated radiation therapy in newly diagnosed glioblastoma: a systematic review on clinical and technical issues. Radiother Oncol 97:361–369
Iuchi T, Hatano K, Kodama T et al (2014) Phase 2 trial of hypofractionated high-dose intensity modulated radiation therapy with concurrent and adjuvant temozolomide for newly diagnosed glioblastoma. Int J Radiat Oncol Biol Phys 88:793–800
Oskan F, Ganswindt U, Schwarz SB et al (2014) Hippocampus sparing in whole-brain radiotherapy. A review. Strahlenther Onkol 190:337–341
van der Laan HP, Gawryszuk A, Christianen ME et al (2013) Swallowing-sparing intensity-modulated radiotherapy for head and neck cancer patients: treatment planning optimization and clinical introduction. Radiother Oncol 107:282–287
Gomez-Millan J, Fernandez JR, Medina Carmona JA (2013) Current status of IMRT in head and neck cancer. Rep Pract Oncol Radiother 18:371–375
Nutting CM, Morden JP, Harrington KJ et al (2011) Parotid-sparing intensity modulated versus conventional radiotherapy in head and neck cancer (PARSPORT): a phase 3 multicentre randomised controlled trial. Lancet Oncol 12:127–136
Spiotto MT, Weichselbaum RR (2014) Comparison of 3D conformal radiotherapy and intensity modulated radiotherapy with or without simultaneous integrated boost during concurrent chemoradiation for locally advanced head and neck cancers. PLoS One 9:e94456
Gregoire V, Jeraj R, Lee JA et al (2012) Radiotherapy for head and neck tumours in 2012 and beyond: conformal, tailored, and adaptive? Lancet Oncol 13:e292–e300
Dayes I, Rumble RB, Bowen J et al (2012) Intensity-modulated radiotherapy in the treatment of breast cancer. Clin Oncol 24:488–498
Freedman GM, Li T, Nicolaou N et al (2009) Breast intensity-modulated radiation therapy reduces time spent with acute dermatitis for women of all breast sizes during radiation. Int J Radiat Oncol Biol Phys 74:689–694
Manon RR, Jaradat H, Patel R et al (2005) Potential for radiation therapy technology innovations to permit dose escalation for non-small-cell lung cancer. Clin Lung Cancer 7:107–113
Aibe N, Yamazaki H, Nakamura S et al (2014) Outcome and toxicity of stereotactic body radiotherapy with helical tomotherapy for inoperable lung tumor: analysis of grade 5 radiation pneumonitis. J Radiat Res 55(3):575–582.
Bezjak A, Rumble RB, Rodrigues G et al (2012) Intensity-modulated radiotherapy in the treatment of lung cancer. Clin Oncol 24:508–520
Jiang ZQ, Yang K, Komaki R et al (2012) Long-term clinical outcome of intensity-modulated radiotherapy for inoperable non-small cell lung cancer: the MD Anderson experience. Int J Radiat Oncol Biol Phys 83:332–339
Zelefsky MJ, Yamada Y, Fuks Z et al (2008) Long-term results of conformal radiotherapy for prostate cancer: impact of dose escalation on biochemical tumor control and distant metastases-free survival outcomes. Int J Radiat Oncol Biol Phys 71:1028–1033
Hatano K, Araki H, Sakai M et al (2007) Current status of intensity-modulated radiation therapy (IMRT). Int J Clin Oncol 12:408–415
Cahlon O, Hunt M, Zelefsky MJ (2008) Intensity-modulated radiation therapy: supportive data for prostate cancer. Semin Radiat Oncol 18:48–57
Bauman G, Rumble RB, Chen J et al (2012) Intensity-modulated radiotherapy in the treatment of prostate cancer. Clin Oncol 24:461–473
Li XA, Wang JZ, Jursinic PA et al (2005) Dosimetric advantages of IMRT simultaneous integrated boost for high-risk prostate cancer. Int J Radiat Oncol Biol Phys 61:1251–1257
Zaorsky NG, Ohri N, Showalter TN et al (2013) Systematic review of hypofractionated radiation therapy for prostate cancer. Cancer Treat Rev 39:728–736
Nath SK, Sandhu AP, Rose BS et al (2010) Toxicity analysis of postoperative image-guided intensity-modulated radiotherapy for prostate cancer. Int J Radiat Oncol Biol Phys 78:435–441
Thompson IM, Valicenti RK, Albertsen P et al (2013) Adjuvant and salvage radiotherapy after prostatectomy: AUA/ASTRO guideline. J Urol 190:441–449
Wagner A, Jhingran A, Gaffney D (2013) Intensity modulated radiotherapy in gynecologic cancers: hope, hype or hyperbole? Gynecol Oncol 130:229–236
Gandhi AK, Sharma DN, Rath GK et al (2013) Early clinical outcomes and toxicity of intensity modulated versus conventional pelvic radiation therapy for locally advanced cervix carcinoma: a prospective randomized study. Int J Radiat Oncol Biol Phys 87:542–548
Klopp AH, Moughan J, Portelance L et al (2013) Hematologic toxicity in RTOG 0418: a phase 2 study of postoperative IMRT for gynecologic cancer. Int J Radiat Oncol Biol Phys 86:83–90
Fernandez-Ots A, Crook J (2013) The role of intensity modulated radiotherapy in gynecological radiotherapy: present and future. Rep Pract Oncol Radiother 18:363–370
Jadon R, Pembroke CA, Hanna CL et al (2014) A systematic review of organ motion and image-guided strategies in external beam radiotherapy for cervical cancer. Clin Oncol 26:185–196
Joaquim AF, Ghizoni E, Tedeschi H et al (2013) Stereotactic radiosurgery for spinal metastases: a literature review. Einstein (Sao Paulo, Brazil) 11:247–255
Sahgal A, Whyne CM, Ma L et al (2013) Vertebral compression fracture after stereotactic body radiotherapy for spinal metastases. Lancet Oncol 14:e310–e320
Yong JH, Beca J, McGowan T et al (2012) Cost-effectiveness of intensity-modulated radiotherapy in prostate cancer. Clin Oncol 24:521–531
Goldin GH, Sheets NC, Meyer AM et al (2013) Comparative effectiveness of intensity-modulated radiotherapy and conventional conformal radiotherapy in the treatment of prostate cancer after radical prostatectomy. JAMA Intern Med 173:1136–1143
Hall EJ, Wuu CS (2003) Radiation-induced second cancers: the impact of 3D-CRT and IMRT. Int J Radiat Oncol Biol Phys 56:83–88
Murray L, Henry A, Hoskin P et al (2014) Second primary cancers after radiation for prostate cancer: a systematic review of the clinical data and impact of treatment technique. Radiother Oncol 110:213–228
Acknowledgments
This study was supported in part by KAKENHI (No. 26670563) and a Health Labor Sciences Research Grant (H23-Sanjigan-Ippan-007) from the Japanese Ministry of Health, Labor and Welfare.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Nakamura, K., Sasaki, T., Ohga, S. et al. Recent advances in radiation oncology: intensity-modulated radiotherapy, a clinical perspective. Int J Clin Oncol 19, 564–569 (2014). https://doi.org/10.1007/s10147-014-0718-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10147-014-0718-y