
Abstract
Natural history of idiopathic normal-pressure hydrocephalus (INPH) is not clear. We performed a literature search for studies that looked into the outcome of unshunted INPH patients trying to answer the following questions: Do all INPH patients deteriorate without shunt? If yes, at what rate? Do some NPH patients improve without shunt? If yes, to what extent? Six studies objectively described the outcome of 102 INPH patients. Result shows that without surgery, most INPH patients had measurable deterioration as early as 3 months following initial assessment. A small number of patients might improve without shunt, however the extent of improvement is not clear. The homogeneity of the findings of the cohort studies provided high evidence supporting the rule of shunt surgery in INPH patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cerebrospinal fluid shunt insertion is the most widely practiced method of treatment of idiopathic normal-pressure hydrocephalus (INPH) [2, 3] since its description by Hakim and Adams in 1965 [1, 6]. However, no study has compared surgical versus conservative treatment in this population, hence the natural history of this condition is not clear and the evidence supporting shunt insertion is not of high quality [3].
INPH diagnosis is difficult since the presenting symptoms are often attributed to aging or more common differential diagnosis. Furthermore associated comorbidities can affect shunt response negatively [13, 16]. There is no gold standard test for diagnosis and many think that the sole practical test for definitive NPH is the patient’s response to shunt insertion [9, 19].
If shunt placement was offered solely on the basis of patient history, examination and presence of ventriculomegaly on neuroimaging, only 46–61% of patients would benefit from surgery [2]. Early surgical series of shunt insertion in idiopathic normal-pressure hydrocephalus have shown low improvement and high complication rates [3, 7]; subsequently, shunt insertion has been advised to be reserved for patients in whom there is a favourable risk-to-benefit ratio [3]. Additional selection criteria based on physiological or functional testing are used in different centres to predict shunt responsiveness, with variable outcome results [2, 13]. The purpose of this review is to try to provide clearer understanding of the outcome of INPH patients without shunt surgery.
Methods
The following research questions were formulated:
-
Do all INPH patients deteriorate without shunt? If yes, at what rate?
-
Do some NPH patients improve without shunt? If yes, to what extent?
Medline was searched in May 2010 for articles discussing the outcome of unshunted INPH patients, using a combination of medical subject headings and free text key words; the search strategy is presented in Table 1.
The results were combined, and abstracts were reviewed for studies of unshunted normal-pressure hydrocephalus patients that satisfied the following inclusion and exclusion criteria:
-
The study should be of idiopathic normal-pressure hydrocephalus patients.
-
The study should clarify the criteria of inclusion of INPH patients.
-
The study should have an objective method of outcome assessment.
The following variables were extracted from included papers formulating the review tables (Tables 2, 3, and 4): study type and level of evidence provided [according to March 2009 Oxford Centre for Evidence-based Medicine (CEBM)—levels of evidence document], number of patients per study, mean age of patients per study, mean follow-up time, diagnostic criteria, outcome assessment method and number of deaths.
Results
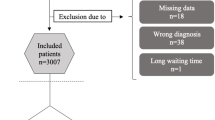
Seven studies were found of which six satisfied the inclusion criteria and objectively described the outcome of 102 patients with provisional diagnosis of INPH and no shunt insertion surgery (Table 2). Follow-up period was 3 months to 7.2 years. There was one case series of patients who refused shunt surgery and five cohort studies comparing the outcome of unshunted patients with shunted patients. Only one cohort study compared two groups without applying any further factors while the other four cohort studies compared two groups depending on results of prognostic tests (Tables 3 and 4).
Scollato et al. [18] published a case series of nine patients with probable INPH, who refused shunt surgery. Clinical evaluation and CSF aqueductal dynamic MRI study was repeated every 6 months for a total of 2 years; all nine patients demonstrated worsening of at least one of the components of the triad by 24 months. Clinical progression was related to changes in aqueductal stroke volume.
Razay et al. [15] prospectively studied a cohort of 33 probable INPH patients. The 3–4 months’ outcome of 19 shunted patients was compared with that of 14 unshunted patients (ten patients declined surgery and four patients were still on the waiting list). While in the shunted group, most patients showed moderate or marked improvement on global ratings, balance and urinary functioning, in the unshunted group, most patients showed moderate or marked worsening (nine patients on global ratings, eight on dementia functioning, and nine on balance and gait functioning). It is not clear whether the remaining patients improved or remained stable, the median change at follow-up figures for the timed up and go and 10-m walking tests do show that some unshunted patients might have improved. However, the results were presented for the group as a whole.
Eide and Brean [5] followed up 37 probable INPH patients for 12 months. Selection for shunt insertion was based on intracranial pulse pressure amplitude based on which patients were divided into two groups: 14 patients with non-elevated pulse pressure amplitudes (group A) and 23 patients with elevated pulse pressure amplitudes (group B). Shunt was advised for group B. However, two patients refused surgery and furthermore one patient in group A had shunt insertion. The 12-month outcome of the 22 shunted patients was compared with that of the 15 unshunted patients. Unshunted patients had median reduction in NPH score of −1 and median reduction in Stein–Langfitt score of −1, compared with shunted patients where a median increase in NPH score was +4 and the median increase of Stein–Langfitt score was +1.
Savolainen et al. [17] prospectively studied a group of INPH patients where the decision of shunt insertion was based on intraventricular overnight ICP recording. The ICP was considered abnormally high if it was continuously above 10 mmHg, or if the basal pressure was between 5 and 10 mmHg and there were any A waves or more than 30% B waves. Twenty-six patients did not fulfil shunt insertion criteria and were followed up. All patients had cortical biopsy as well as lumbar infusion test. After 5 years, none of the unshunted patients had improved in activity of daily living (47% unchanged and 53% worse), while 72% of shunted patients improved postoperatively.
Brean and Eide [4] studied a group of INPH patients with infusion tests results of outflow resistance (Rout) >10 mmHg/ml/min. ICP monitoring was used as a prognostic test, where CSF pressure pulsatility was used as a measure of intracranial compliance. Twenty patients had shunt insertion and were compared with 12 with no shunt. At 12 months follow-up, 16 of 18 shunted patients (89%) had improved neurologically. Those not receiving a shunt remained unchanged or worsened.
Pfisterer et al. [14] compared the outcome of 26 patients with probable INPH that were excluded from shunt surgery based on continuous intraventricular pressure monitoring and intraventricular infusion test. Patients with basal pressure above 10 mmHg and/or A waves and/or B waves of more than 10% of the recorded period were selected for shunt insertion. While 96% of shunted patients improved from gait disturbance, 77% from cognitive impairment and 75.7% from urinary dysfunction, only 15% of the unshunted patients improved from gait disturbance, 9% from cognitive impairment and 18% from urinary dysfunction.
In an early surgical series, Hughes et al. [8] retrospectively compared the outcome of 12 unshunted INPH patients with that of 27 shunted patients. In the unshunted patients group, 50% worsened, 42% were unchanged and one patient improved, compared with shunted group: 41% worsened, 26% were unchanged and 33% improved. No objective outcome assessment method was used, and thus this study has been excluded from further analysis.
Discussion
The “natural history” of untreated INPH has not been studied well and long-term outcome of untreated patients is not clear. The international guidelines for diagnosis and management of idiopathic normal-pressure hydrocephalus advise shunt insertion as a guideline rather than a standard since no trial has yet compared the placement of a shunt versus conservative management in a randomized controlled manner [3].
Study types and quality
Of the six studies included in this review, only one study was done aiming to compare outcome of shunt versus no shunt in an INPH population (Razay et al.), the remaining five articles were mainly concerned with studying the effect of prognostic test or imaging findings. Follow-up period varied between different studies, and outcome assessment method varied. Each study presented data in different way: either as improvement of each patient per symptom or improvement of the whole group per symptom or global improvement of patient or total group.
Outcome
Giving the different inclusion and assessment criteria and small numbers of patients, meta-analysis of the provided data was not possible. Studies were divided into two groups depending on the studied population.
In Table 3 we included the two studies that looked into the outcome of the unshunted probable INPH patients with no added confounding factor (Razay et al. and Scollato et al.). Both studies showed that unshunted patients progressively worsened overtime. This worsening was measurable in more than half of the patients as early as 3 months following the initial assessment.
Table 4 shows the results from the remaining four cohort studies. These are studies that compared the outcome of the shunted INPH patients who where thought likely to benefit from shunt with those unshunted because they were thought to be unlikely to benefit from shunt based on results of prognostic tests.
Since none of the prognostic tests used are 100% specific or sensitive [13], the unshunted patients group might include some true INPH patients, the rest might represent patients with other diagnoses or advanced INPH patient. The natural history of patients thought to be unlikely to benefit from shunt surgery is again unknown. The majority of patients deteriorated as early as 1 year following initial assessment. Interestingly, some patients improved in at least one of the symptoms of the triad on follow-up; i.e., INPH might not be an invariably progressive disorder as previously thought. This improvement might be related to use of lumbar infusion and resulting CSF drainage through dural hole. It is known that non-shunted patients may improve weeks or months after a CSF tap [11, 12]. All the five cohort studies agreed that shunted patients have significantly better outcome than that of unshunted patients.
Level of evidence
All these studies provided class 4 evidence according to the CEBM level of evidence document [case series and a poor cohort either due to failure to carry out a sufficiently long follow-up of patients or the presence of additional confounder in the cohort (prognostic tests)]. However, collectively, the homogeneity of the conclusions of the five cohort studies in this review does provide relatively high-ranking evidence (2a according to CEBM level of evidence document) that the majority of unshunted patients do deteriorate without shunt surgery and that shunt insertion results in better outcome compared with conservative management. It is not possible to draw any conclusion from the mortality figures provided in the six studies given the small number of patients, variable follow-up time and absence of normal controls.
Controlled randomized trial comparing shunted versus unshunted patients would provide an accurate estimate of long-term natural history of INPH as well as providing the evidence to support or dismiss surgical management of INPH. However, recruitment of a suspected INPH patient into a conservative arm might be difficult, even if we consider it acceptable from an ethical point of view [3]. On the other hand, well-designed cohort studies could provide high-quality evidence of the existence as well as natural history of this condition. Comparison with normal controls is needed to estimate the extent of improvement induced by shunt or deterioration without shunt and the effect of such change on patient independence and on society. Since normal-pressure hydrocephalus is a rare condition, there is a need for collaboration between different centres, and this fact has already been recognized by the international hydrocephalus research society [10].
Conclusions
Although quality of studies was poor and numbers were small, this review has shown that without surgery, most INPH patients had measurable deterioration as early as 3 months following initial assessment. This would probably indicate the need for an early intervention as well as need for early diagnosis. A small number of patients might improve without shunt; however, the extent of improvement is not clear. The homogeneity of the findings of the cohort studies provided high evidence supporting the rule of shunt surgery in INPH patients.
References
Adams R, Fisher C, Hakim S, Ojemann R, Sweet W (1965) Symptomatic occult hydrocephalus with“normal” cerebrospinal-fluid pressure. A treatable syndrome. N Engl J Med 273:117
Batra S, Rigamonti D (2009) Idiopathic normal pressure hydrocephalus: the benefits and problems of shunting. Nat Clin Pract Neurol 5:80–81
Bergsneider M, Black PML, Klinge P, Marmarou A, Relkin N (2005) Surgical management of idiopathic normal-pressure hydrocephalus. Neurosurgery 57:S2
Brean A, Eide PK (2008) Assessment of idiopathic normal pressure patients in neurological practice: the role of lumbar infusion testing for referral of patients to neurosurgery. Eur J Neurol 15:605–612
Eide PK, Brean A (2006) Intracranial pulse pressure amplitude levels determined during preoperative assessment of subjects with possible idiopathic normal pressure hydrocephalus. Acta Neurochir 148:1151–1156
Hakim S, Adams R (1965) The special clinical problem of symptomatic hydrocephalus with normal cerebrospinal fluid pressure: observations on cerebrospinal fluid hydrodynamics. J Neurol Sci 2:307–327
Hebb AO, Cusimano MD, Mapstone TB, Cohen AR, McComb JG, Gjerris F et al (2001) Idiopathic normal pressure hydrocephalus: a systematic review of diagnosis and outcome. Neurosurgery 49:1166–1186
Hughes C, Siegel B, Coxe W, Gado M, Grubb R, Coleman R et al (1978) Adult idiopathic communicating hydrocephalus with and without shunting. J Neurol Neurosurg Psychiatry 41:961
Ishikawa M, Hashimoto M, Kuwana N, Mori E, Miyake H, Wachi A et al (2008) Guidelines for management of idiopathic normal pressure hydrocephalus. Neurol Med Chir (Tokyo) 48:1–23
Jones HC, Klinge PM (2008) Hydrocephalus 2008, 17–20th September, Hannover Germany: a conference report. Cerebrospinal Fluid Res 5:19
Lim TS, Yong SW, Moon SY (2009) Repetitive lumbar punctures as treatment for normal pressure hydrocephalus. Eur Neurol 62:293–297
Malm J, Kristensen B, Stegmayr B, Fagerlund M, Koskinen LO (2000) Three-year survival and functional outcome of patients with idiopathic adult hydrocephalus syndrome. Neurology 55:576–578
Marmarou A, Bergsneider M, Klinge P, Relkin N, Black PML (2005) The value of supplemental prognostic tests for the preoperative assessment of idiopathic normal-pressure hydrocephalus. Neurosurgery 57:S2
Pfisterer WK, Aboul-Enein F, Gebhart E, Graf M, Aichholzer M, Muhlbauer M (2007) Continuous intraventricular pressure monitoring for diagnosis of normal-pressure hydrocephalus. Acta Neurochir 149:983–990
Razay G, Vreugdenhil A, Liddell J (2009) A prospective study of ventriculo-peritoneal shunting for idiopathic normal pressure hydrocephalus. J Clin Neurosci 16:1180–1183
Relkin N, Marmarou A, Klinge P, Bergsneider M, Black PML (2005) Diagnosing idiopathic normal-pressure hydrocephalus. Neurosurgery 57:S2
Savolainen S, Hurskainen H, Paljarvi L, Alafuzoff I, Vapalahti M (2002) Five-year outcome of normal pressure hydrocephalus with or without a shunt: predictive value of the clinical signs, neuropsychological evaluation and infusion test. Acta Neurochir 144:515–523
Scollato A, Tenenbaum R, Bahl G, Celerini M, Salani B, Di Lorenzo N (2008) Changes in aqueductal CSF stroke volume and progression of symptoms in patients with unshunted idiopathic normal pressure hydrocephalus. AJNR Am J Neuroradiol 29:192–197
Stein SC, Burnett MG, Sonnad SS (2006) Shunts in normal-pressure hydrocephalus: do we place too many or too few? J Neurosurg 105:815–822
Disclosure
Clinical research fellow at Victor Horsley Department of Neurosurgery (Mr Toma) is supported by a grant from B. Braun/Aesculap.
Author information
Authors and Affiliations
Corresponding author
Additional information
Comments
Ernst Delwel, Rotterdam, The Netherlands
The authors have performed a literature search for studies that looked into the outcome of unshunted patients who were diagnosed as idiopathic normal-pressure hydrocephalus (INPH).
The authors state that based on different inclusion criteria, the overall improvement rate after shunting is 45–60%. This means that the not-improved patients had another disease mimicking INPH or the patients were already in the phase of irreversibility, for instance because of a delay in treatment. Of course, shunt dysfunction should always be ruled out.
So if a group of patients suspected of INPH without a shunt are followed, it depends on the inclusion criteria for INPH what the result will be. In case of very strict and limiting criteria and implementation of the extended lumbar drainage with its very high positive predictive value, the chance of improvement is expected to be very high. However, in case of liberal inclusion criteria, the chance of postoperative improvement for the whole group is expected to be much lower.
In the first case, one would expect that most patients will more likely show the disease course of real INPH patients. In the second case however, one would expect more INPH-mimicking diseases included like (vascular) dementia, Parkinson, depression, etc. In this group the expected disease course during follow-up is expected to be less predictable and more heterogeneous. In the second case, one would expect very slow progression in some cases, stable disease in other cases and sometimes even temporary improvement dependent on the real pathology.
In other words, the best group to study the natural history of INPH is the group in which very strict inclusion criteria are used and in which the decision to include is based on a test or a combination of tests with a very high positive predictive value, like extended lumbar drainage for a couple of days [1].
The six studies that were presented used different inclusion criteria. Only one cohort study of Razay et al. [2] compared two groups without applying any further factors, while the other five cohort studies compared two groups depending on the results of prognostic tests. So in the last five cohort studies, the unshunted group that was followed was less likely to have INPH and the natural history of the groups in these five cohorts might particularly reflect the natural history of INPH-mimicking diseases. In the study of Razay et al. [2], inclusion criteria were mild cognitive impairment or dementia and/or gait disorders and enlarged ventricles on brain imaging. These are rather liberal criteria which might have lead to inclusion of relatively more patients who have no real INPH which is the drawback of their study. Despite differences in inclusion criteria, confounding elements and bias in the presented studies, it is obvious that most not-shunted patients will deteriorate within the period of 3 months after initial assessment, which is a valid and useful conclusion.
A prospective randomized study on a shunted and a not-shunted group of INPH patients, in which very strict and limited inclusion criteria and tests with a high positive predictive value are used, would be needed in search of a more valuable answer to the question what the natural history of INPH really is.
References
1. Haan J, Thomeer RTWM (1988) Predictive value of temporary external lumbar drainage in normal pressure hydrocephalus. Neurosurgery 22:388–391
2. Razay G, Vreugdenhil A, Liddell J (2009) A prospective study of ventriculo-peritoneal shunting for idiopathic normal pressure hydrocephalus. J Clin Neurosci 16:1180–1183
Siamak Asgari, Ingolstadt, Germany
The authors present a review of the literature with selection of reported patients with suspect of idiopathic normal-pressure hydrocephalus (NPH), who did not undergo CSF shunting. The authors wanted to get evidence-based analysis of the spontaneous course of NPH without surgical therapy. They could summarize 102 patients from totally six studies. During a follow-up time from 3 months to 7 years, nearly 50% of patients remained clinically unchanged and the other 50% of patients showed deterioration. However, this paper corroborates the effectiveness of shunt procedures in NPH. The impact of this paper would be higher if it would focus on the untreated patients. Detailed informations of the patients in the follow-up are necessary. What kind of psychological and neurological tests were used for measuring the patient’s functions? A graphic illustration showing clinical deterioration or status over the follow-up period would be of great help. Finally, a comment to newer strategies in the treatment of NPH like endoscopic third ventriculostomy should be mentioned.
Veit Rohde, Göttingen, Germany
The authors performed a literature research to define the natural history of idiopathic NPH (iNPH). They identified six studies with a total number of 102 patients. In two of these studies, outcome after ventriculoperitoneal shunt was compared with that in patients who either refused surgery or are on the waiting list (23 patients). In the remaining four studies, outcome after ventriculoperitoneal shunt was compared with that of patients who were considered to be no good candidates for shunting according to diagnostic tests. To take the worst case scenario, none of these patients are iNPH patients, which would mean that the conclusions which are drawn by the authors are only based on the findings in 23 patients.
Nonetheless the findings in these 23 untreated patients with worsening of at least one of the components of the Hakim triad or worsening in global tests within 24 months in all of them are striking and indicate that the outcome of iNPH without shunt is poor. This especially holds true, because the assumption that none of the remaining patients in whom shunt surgery was not considered to be indicated has an iNPH possibly is too puristic.
Rights and permissions
About this article
Cite this article
Toma, A.K., Stapleton, S., Papadopoulos, M.C. et al. Natural history of idiopathic normal-pressure hydrocephalus. Neurosurg Rev 34, 433–439 (2011). https://doi.org/10.1007/s10143-011-0316-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-011-0316-7