
Abstract
The “whirl sign” is an uncommon finding on emergency CT. However, it is easy to overlook if not kept in mind. Its recognition is of capital importance, being most of its causes potentially lethal. Surgical treatment is also mandatory when signs of complication are found. The whirl sign is usually found associated to midgut, cecal and sigmoid volvulus, small-bowel volvulus and closed-loop obstructions, and post-surgical mesenteric windows (including retroanastomotic hernias). CT is an optimal imaging technique to depict the so-called sign and associated CT features suggesting complication (circumferential wall thickening, pneumatosis intestinalis, pneumoperitoneum, mesenteric fat stranding, free intraperitoneal fluid, mesenteric haziness). Radiologists must be able to recognize the whirl sign and seek associated findings that strongly support the diagnosis of a spectrum of entities, some of them lethal if no treatment is established.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In the literature, there are different names given to the whirling appearance of bowel loops wrapped around mesenteric vessels such as the “whirl sign”, the “superior mesenteric vein (SMV) rotation sign”, and the ultrasonographic “whirlpool sign”. In addition, the “barber-pole sign” has recently been described. Most whirling patterns detected on CT are not indicative of a specific pathologic condition, and therefore, a differential diagnosis should be considered when this non-specific finding is observed. Hence, a definition of what we have considered to be a whirl sign in our paper is mandatory: central vessels producing a whirl-like pattern, partly, or entirely encircled by bowel loops, excluding cases where the “whirl” appearance involves only vessels or bowel. The direction of bowel rotation was also determined (clockwise/counterclockwise), as is the presence of small or large bowel obstruction.
We also focus on associated findings that strongly support a specific diagnosis, such as mesenteric vascular engorgement, mesenteric hemorrhage and/or free intraperitoneal fluid, thickened bowel wall, and presence of pneumatosis intestinalis.
The aims of this pictorial essay are (1) to describe the so-called whirl sign features on emergency CT; (2) to distinguish the differences between the CT whirl sign, the SMV rotation sign, and the recently described barber-pole sign, all of them on CT, as well as the ultrasonographic whirlpool sign, the latter considered to be a sign of midgut volvulus due to malrotation; (3) to illustrate the spectrum of entities that may show this sign; and (4) to depict associated findings that support the diagnosis.
Description of the signs on CT and ultrasound
The CT whirl sign
The CT whirl sign was first described by Fischer [1] in 1981 (in a patient thought to have chronic pancreatitis) as the “small-bowel loops encircling the superior mesenteric artery [to] create a whirl-like pattern”. Subsequent case reports have described this sign in association with midgut volvulus and malrotation [2–4], small-bowel volvulus [5], closed-loop obstructions with variable degree of volvulus [6], cecal volvulus [7], and post-surgical mesenteric fenestrations [8].
However, Blake et al. [9] reported a series of six patients with this sign and found that only two had surgically proven volvulus, concluding that the whirl sign was non-specific at best.
Given the uncertain significance of this sign on CT, we summarize the features of the whirl sign in Table 1.
The whirl sign can be defined as twisted bowel loops encircling mesenteric vessels. The direction of the twist (clockwise/counterclockwise) using the vessels as the central axis is defined cranio-caudally. As suggested by Gollub et al. [10], a minimum rotation of bowel loops for at least 90° is needed before a volvulus can be diagnosed. Most of the publications have not described the role of picture archive and communications system in detecting the whirl sign. It may be easier to detect the whirling appearance due to the use of image scrolling, which could allow a summation effect in our minds.
The SMV rotation sign
The SMV rotation sign refers to an abnormal position of the SMV on the left ventral side of the SMA. This sign was first described by Nichols [11] in a series of three patients thought to have chronic pancreatitis. Its importance lies within the fact that a midgut malrotation should be considered if such a sign is observed (as shown on Fig. 1).

Axial contrast-enhanced abdominal CT scan depicts an abnormal position of the superior mesenteric vein (blue arrowhead) on the left ventral side of the superior mesenteric artery (red arrowhead), instead of being on the right side. Small-bowel loops are crowded in the right upper quadrant (yellow arrow) and loops of colon lie on the opposite side (C) of the abdomen, consistent with bowel malrotation. The duodenojejunal transition point (Treitz angle) was located on the right side of the upper abdomen. Cholelithiasis and signs of cholecystitis are also noted
The barber-pole sign
Recently, Buranasiri described “a counterclockwise twisting of the mesenteric vessels upon themselves in a rare case of counterclockwise volvulus” as the angiographic barber-pole sign. There have been only six reported descriptions of this sign, and only three of them were proven to be pathological [12]. Therefore, this sign may represent a NORMAL relationship of mesenteric vessels (see Fig. 11).
The ultrasonographic whirlpool sign
The ultrasonographic whirlpool sign, first described by Pracros, is found on transverse sonograms when the SMV and the mesentery wrap around the SMA in a clockwise direction [13]. This is thought to represent a midgut (portion of the bowel supplied by the SMA) volvulus, secondary to malrotation. This is an entity almost exclusively seen on pediatric age group.
Shimanuki et al. [2] found that the whirlpool sign consists of a side-by-side arrangement of vessels with opposing flow directions, indicating that the whirlpool contains not only the SMV and its tributaries but also branches of the SMA.
Visualization of this sign is enhanced by the vascular signal obtained on color Doppler flow ultrasound [13] (see Fig. 2).

a Transverse sonogram in a 1-month-old infant demonstrates the whirlpool-like pattern of the SMV and mesentery twisted around the SMA, indicative of a midgut volvulus. The SMA (green arrow) is seen in the middle of the volvulus and anterior to the aorta (red arrow). b Transverse color Doppler flow ultrasonogram of the mid-upper abdomen depicts the whirlpool sign enhanced by the vascular flow signal
Imaging findings
We retrospectively reviewed CT studies performed at Hospital La Paz from our database of emergency pathology over a 2-year period. All studies were performed using a two-slice scanner (Asteion; Toshiba, Tokyo, Japan) and following a standardized protocol, featuring 4 mm of slice thickness, data reconstruction interval of 2 mm, rotation time of 0.75 s, kV 120, mA 200, and a pitch of 1.5. In addition, 120 mL of iodinated contrast media (Omnipaque TM 300 mg/mL Iohexol, GE Healthcare, Milwaukee, USA) was administered at a rate of 2.5 mL/s. Images were obtained in a portal venous phase, 60 s after administration of a bolus of contrast media. An abdominal CT angiogram was performed in cases of suspected midgut volvulus using a dual-phase abdominal CT scan with an arterial phase using 3 mm of slice thickness, data reconstruction interval of 1.5 mm, and an injection rate of iodinated contrast of 3 mL/s. The portal venous phase parameters were the same as previously described.
Examinations were reviewed on a workstation (Vitrea software, Vital Images, Minnesota, USA) in order to achieve multiplanar reconstructions, maximum intensity projection (MIP), and volume-rendered (VR) images for better image characterization.
Malrotation and midgut volvulus
Intestinal malrotation associated with midgut volvulus is a pathological process almost exclusively seen in the pediatric population.
Both the duodenojejunal and ileocolic segments of the primitive digestive tube rotate counterclockwise around the omphalomesenteric vessels (future superior mesenteric artery and vein) before reaching their final normal positions [14]. This rotation is followed in the last stage by fixation of the bowel by the peritoneum. Midgut malrotation results when the midgut undergoes less than the normal 270° of counterclockwise rotation.
The midgut volvulus entity combines malrotation of the gut in the developing embryo with a lack of proper attachment of the intestine to the posterior abdominal wall. As a result, the small bowel encircles the superior mesenteric vessels, leading to volvulus.
The twisting is, by definition, Clockwise, whereas in small-bowel volvulus, the twisting can be either clockwise or counterclockwise. Sometimes, a corkscrew appearance of the SMV can be seen on VR images (Fig. 3a–d).

a Axial contrast-enhanced abdominal CT scan below the celiac trunk demonstrates an abnormal position of the superior mesenteric vein (blue arrowhead), which lies to the left of the superior mesenteric artery (red arrowhead). The green arrow points to the duodenojejunal junction, which lies in an abnormal right-sided position, suspicious for malrotation with an initial clockwise twisting. b Axial contrast-enhanced abdominal CT scan caudal to a shows the SMA as the central axis (red arrowhead) of a clockwise twisting of jejunal bowel loops (green arrow). c Coronal MIP depicts a whirling appearance of mesenteric vessels (red arrow). d Frontal VR demonstrates a corkscrew-like SMV (blue arrow) around the SMA (yellow arrow) due to a volvulus
Small-bowel volvulus
The small intestine is the most common site for intestinal volvulus, accounting for 10% of intestinal and 11% of strangulating obstructions. According to Juler et al. [15], small-bowel volvulus should be always associated with small-bowel obstruction. The twisting can be either clockwise or counterclockwise. The degree of circulatory impairment depends on the tightness of the twist and infarction that occurs in approximately 50% of cases [15].
Primary or idiopathic volvulus is rare in Western society. Secondary causes include adhesions, tumors, intussusception, internal hernia, and enteroenterostomy [15] (Fig. 4).

a Distinctive whirl-like pattern (yellow arrow, case recorded as approximately 270°) consisting of central vessels surrounded by loops of small bowel. Note bowel wall thickening (red asterisk) with adjacent mesenteric fat stranding and vascular engorgement, consistent with small-bowel volvulus. b Axial CT image, cranial to the previous image, demonstrating dilated small-bowel loops filled with fluid (red asterisks) proximal to the volvulus and collapsed loops of bowel distal to it (yellow asterisks)
The onset of symptoms includes acute abdominal pain with or without early persistent vomiting. An associated radiological sign to this gnosological entity is the “beak sign” (Fig. 5b), that is, a fusiform tapering of a bowel loop at the site of the twist in the longitudinal view.

a–b Patient initially diagnosed as acute pancreatitis. a Axial CT scan image shows a counterclockwise wrapping of the SMV (blue arrow) around the distal SMA (red asterisk). The yellow arrow points to dilated small-bowel loops, and the red arrow points to collapsed small-bowel loops distal to the whirl. b Axial CT scan image of the same patient than in a shows dilated bowel loops associated with mesenteric fat stranding (red asterisks). The yellow arrow points to the so-called beak sign, that is, the beginning of the obstruction where the loop twists. The final diagnosis was small-bowel volvulus
Closed-loop obstructions
The frequency of strangulating obstruction (or closed-loop obstruction) in patients with small-bowel obstruction varies in different studies from 5% to a maximum of 42%.
A closed-loop obstruction is defined as a form of mechanical intestinal obstruction in which a segment of bowel is occluded at two points along its length. By far, the most common causes are adhesive bands and internal or external hernias [6]. Strangulating obstruction is defined as an intestinal obstructive process associated with intestinal ischemia.
Imaging abnormalities observed at the point of the obstruction can include a U-shaped, fluid-filled bowel loop, the whirl sign, the beak sign, and a triangular loop (Figs. 6 and 7). Balthazar et al. [6] reported in a series of 19 patients in which the most common CT finding were fluid-filled, distended, U-shape loops of bowel in a radial configuration with stretched and thickened mesenteric vessels converging toward the point of the obstruction.

a–b Proven closed-loop obstruction at operation. a Axial CT scan image of the pelvis shows wall thickening of a U-shaped bowel loop (yellow arrow) with fusiform bowel tapering, that is, the beak sign (green arrow). In the center of the loop (red asterisk), a whirl sign can be seen. b Axial CT scan image of the same patient with the whirl sign marked by the red asterisk, accompanied by the presence of free intraperitoneal fluid (yellow arrow)

a Axial abdominal contrast-enhanced CT scan shows the crowding, whirl-like appearance of mesenteric vessels (red arrow), that is, the whirl sign. Dilated bowel loops filled with fluid with lack of enhancement of their wall suggesting ischemia (yellow arrowhead). The blue asterisk points to free intraperitoneal fluid. b Axial CT scan image, slightly more caudal to a shows the central vascular whirl pattern (blue arrow). Note that there is lack of enhancement of the central mesenteric vessels, indicating vascular compromise. The red arrow points to the beak sign of a loop of small bowel. Pneumatosis intestinalis is noted
Cecal volvulus
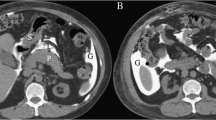
Cecal volvulus is a rare condition, representing 1–3% of cases of all intestinal obstructions. It is assumed to develop due to an improper fusion of the cecal mesentery with the posterior parietal peritoneum. The causes of hypermobility may be congenital or acquired. Delabrousse et al. [7] suggested that the classification of cecal volvulus be divided into three different types based on the pathophysiological mechanism: type I, axial torsion (Fig. 8a–b); type II, loop type; and type III, cecal bascule type (Fig. 10). In the axial torsion type, the CT images depict a whirl sign in a clockwise direction associated to a cecum located in the lower abdomen. In the second type (loop type), there is a counterclockwise whirl sign associated with the cecum located in the upper abdomen (Fig. 9).

a Axial CT scan image the of lower abdomen shows a dilated and normally positioned cecum (C), with a double air–fluid level (red asterisks). An abnormal position of the terminal ileum and ileocecal valve (yellow arrow), which lie lateral to, instead of medial to the cecum, consistent with an axial torsion type (type I) cecal volvulus. Note the collapsed left colon (red arrow). b Clockwise whirl sign of the ileocecal artery (yellow arrow) wrapped around terminal ileum (red asterisk). The blue star points to a normally positioned cecum

a Coronal reformatted image shows the rotation site of a strangulated cecal volvulus. b Volume-rendered image shows cecal pole of the volvulus
The cecal bascule type (Fig. 10) is interesting as it is characterized by a lack of the whirl sign, and the cecum is located centrally in the abdomen.

a Axial CT scan image of lower abdomen depicts grossly dilated cecum (C) located in the center of the abdomen. The red arrow points to collapsed bowel loops, and the blue asterisk points to free intraperitoneal fluid. b Axial CT scan image of the central abdomen in same patient reveals the beak sign (red arrow) of the right colon and the tip of the dilated cecum (C). No whirl sign is demonstrated within mesenteric vessels. Note fluid-filled bowel loops, free intraperitoneal fluid, and mesenteric fat stranding
Table 2 summarizes the CT findings for the different types of cecal volvulus.
Other CT findings associated with a cecal volvulus include distension of the cecum (more than 10 cm), an air–fluid level in the cecum, the presence of an ileocecal twist, a distended terminal ileum, collapse of the left colon, and evidence of complications such as pneumatosis intestinalis and portal venous gas.
Patients with cecal volvulus usually present non-specifically with acute cramping abdominal pain, abdominal distension, nausea, and vomiting.
Barber-pole sign
Initially described as an angiographic sign by Buranasiri, it consists of a counterclockwise twisting of the mesenteric vessels in a clinical case of midgut volvulus. There have been only six reported descriptions of this sign, and only three of them were proven to be pathological. Latest publications suggest this finding can be a normal relationship of mesenteric vessels.
Therefore, this finding could be reported as SMA/SMV orientation variance without midgut malrotation, in a counterclockwise direction (see Fig. 11).

a–d Axial CT scan images depicting the anatomical relationship between the SMA (red arrowhead) and the SMV (blue arrowhead) from cranial (a) to caudal (d). The SMV is wrapped counterclockwise around the SMA. The SMA is thought to lie in the central axis (red arrowhead)
Retroanastomotic hernias
Subsequent to gastric surgery, the presence of a whirl sign may indicate a herniation of the efferent or afferent limbs through a defect created behind the anastomosis, after ante- or retrocolic reparation. Axial CT imaging features include (1) location of the whirl: left, right, or superior periumbilical; (2) loop involved: afferent, efferent, or both; and (3) associated findings: wall thickening, decreased enhancement, etc. (Fig. 12).

a–d Patient following a total gastrectomy and esophagojejunostomy demonstrating a retroanastomotic hernia with a whirl sign. a Axial CT scan image depicting post-surgical changes of the total gastrectomy and esophagojejunostomy (arrowhead). Bilateral pleural effusions noted. b The efferent loop (arrowheads), anterior to aorta. c Whirling of mesenteric vessels in the left periumbilical abdomen. At operation, the efferent loop was herniated through the defect behind the anastomosis. d The efferent loop (arrowheads) in an antecolic position with wall thickening and decreased contrast enhancement. Bilateral renal atrophy noted incidentally
Pitfalls
The whirl sign on CT may be a clue for abdominal pathology. However, it is not a pathognomonic sign. We list some cases from our database in which the whirl is not due to a pathological condition.
Figure 13 shows a normal variant, which probably will not confuse a trained radiologist, consisting on a middle colic vein draining in a whirl-like pattern.

A particularly conspicuous and common location of the whirl appearance is near the root of the mesentery, involving the right or middle colic vein rotating counterclockwise (blue arrowhead) near the SMA (red arrow). This is thought to represent a normal appearance
Sometimes, a vascular whirl-like pattern can be misleading, especially if associated with dilated and fluid-filled bowel loops and mural thickening. In Fig. 14a–d, the initial diagnosis of small-bowel loop obstruction was later amended to gallstone ileus.

a and b Axial CT scans images in which a whirl appearance is seen near the root of the mesentery (red arrowhead). Dilated and fluid-filled bowel loops (red asterisk) with mural thickening (green arrow) pointing to a small-bowel volvulus. c The guilty gallstone (red arrow), located in a small-bowel loop (probably a loop of jejunum), causing the ileus. Note mural thickening of bowel loops (green arrowhead). d Gas within gallbladder (blue arrow), initially mistaken for colon. A communication between gallbladder and stomach was retrospectively seen on CT scan images (not shown)
Conclusion
The whirl sign on CT is not a pathognomonic sign.
Nevertheless, it can be helpful as a clue for intra-abdominal pathology, especially if associated findings are present.
Radiologists should be able to recognize normal variants and pathological conditions, as failure to recognize a surgical emergency such as midgut volvulus may have catastrophic consequences.
References
Fisher JK (1981) Computed tomographic diagnosis of volvulus in intestinal malrotation. Radiology 140:145–146
Shimanuki Y, Aihara T, Takano H et al (1996) Clockwise whirlpool sign at color Doppler US: an objective and definite sign of midgut volvulus. Radiology 199:261–264
Berrocal T, Lamas M, Gutiérrez J et al (1999) Congenital anomalies of the small intestine, colon, and rectum. Radiographics 19:1219–1236
Aidlen J, Anupindi SA, Jaramillo D, Doody DP (2005) Malrotation with midgut volvulus: CT findings of bowel infarction. Pediatr Radiol 35:529–531. doi:10.1007/s00247-004-1355-9
Loh YH, Dunn GD (2000) Computed tomography features of small bowel volvulus. Australas Radiol 44:464–467. doi:10.1046/j.1440-1673.2000.00856.x
Balthazar EJ, Birnbaum BA, Megibow AJ et al (1992) Closed-loop and strangulating intestinal obstruction: CT signs. Radiology 185:769
Delabrousse E, Sarliève P, Sailley N, Aubry S, Kastler BA (2007) Cecal volvulus: CT findings and correlation with pathophysiology. Emerg Radiol 14:411–415. doi:10.1007/s10140-007-0647-4
Kwon JH, Jang HY (2005) Retroanastomotic hernia after gastrojejunostomy: US and CT findings with an emphasis on the whirl sign. Abdom Imaging 30:656–664. doi:10.1007/s00261-005-0310-z
Blake MP, Mendelson RM (1996) The whirl sign: a non-specific finding of mesenteric rotation. Australas Radiol 40:136–139. doi:10.1111/j.1440-1673.1996.tb00367.x
Gollub MJ, Yoon S, Smith LM, Moskowitz CS (2006) Does the CT whirl sign really predict small bowel volvulus? Experience in an oncologic population. J Comput Assist Tomogr 30:25–32. doi:10.1097/01.rct.0000191680.28344.f0
Nichols DM, Li DK (1983) Superior mesenteric vein rotation: a CT sign of midgut malrotation. AJR Am J Roentgenol 141:707–708
Clark P, Ruess L (2005) Counterclockwise barber-pole sign on CT: SMA/SMV variance without midgut malrotation. Pediatr Radiol 35:1125–1127. doi:10.1007/s00247-005-1517-4
Epelman M (2006) The Whirlpool sign. Radiology 240:910–911. doi:10.1148/radiol.2403040370
Long FR, Kramer SS (1996) Radiographic patterns of intestinal malrotation in children. Radiographics 16:547–556
Juler GL, Stemmer EA, Connoly JE (1971) Preoperative diagnosis of small bowel volvulus in adults. Am J Gastroenterol 56:235–247
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Suárez Vega, V.M., Martí de Gracia, M., Verón Sánchez, A. et al. Trapped on the “whirl”: diagnostic sign on emergency CT. Emerg Radiol 17, 139–147 (2010). https://doi.org/10.1007/s10140-009-0816-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-009-0816-8