
Abstract
Background
The systemic inflammation score (SIS), based on preoperative serum albumin (Alb) level and lymphocyte-to-monocyte ratio (LMR), has been shown to be a novel prognostic score for some tumors. We investigate the prognostic value of the SIS in patients with resectable gastric cancer (GC).
Methods
Patients with GC who underwent curative resection between December 2008 and December 2013 were included. Time-dependent receiver operating characteristics analysis (t-ROC), concordance index (C-index) and AUC were used to compare the prognostic impact.
Results
Totally, 1786 patients with resectable GC were included in the study. By multivariate analysis, the SIS was not an independent prognostic factor. However, the normal Alb level (≥ 40 g/l) and LMR ≥ 3.4 both remained independent protective factors for GC (both P < 0.05). Due to the similar survival of patients with LMR ≥ 3.4 and LMR < 3.4 in the normal Alb group, we combined the two subgroups to establish the modified SIS (mSIS). Multivariate analysis revealed that the mSIS was the only significant independent biomarker (P < 0.05). The t-ROC curve and C-index for the mSIS were superior to those of the SIS throughout the observation period. Furthermore, the AUC of the mSIS was significantly greater than that of the SIS at 3 and 5 years after operation (both P < 0.05).
Conclusion
The preoperative mSIS is a novel, simple and useful prognostic factor for postoperative survival in patients with GC and can be used as a part of the preoperative risk stratification process to improve the prediction of clinical outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastric cancer (GC) is the fifth most common malignancy and the third most common cause of cancer-related death worldwide [1]. Despite advancements in surgical techniques and adjuvant therapy, the survival of patients with advanced GC remains poor. In 1863, Virchow first proposed an association between cancer and inflammation [2]. Systemic inflammation has been reported to play a critical role in the pathogenesis and progression of cancer [3]. Pretreatment serum-based inflammatory biomarkers, such as the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR) and the Glasgow prognostic score (GPS), have shown potential prognostic values in a variety of tumors [3,4,5]. Preoperative serum albumin (Alb) levels have also been reported as clinical prognostic indicators for cancer [3]. However, there is no widely accepted optimal value for circulating blood cell-based biomarkers and no established scoring system that integrates the biomarkers to refine the prognostic prediction for cancer patients. Recently, the systemic inflammation score (SIS), based on the preoperative Alb level and LMR, was reported as a powerful prognostic marker for clear cell renal cell carcinoma and colorectal cancer [6, 7]. However, whether the SIS can predict the prognosis of GC patients remains unclear. Therefore, the purpose of this study was to examine the prognostic value of the combination of Alb level and LMR (SIS) for patients with resectable GC in a dataset from a large center.
Patients and methods
Study population
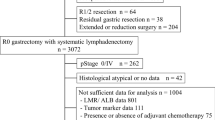
We retrospectively assessed all patients with resectable GC who were treated between December 2008 and December 2013 at Fujian Medical University Union Hospital. The following inclusion criteria were applied: (1) a histologically confirmed adenocarcinoma of the stomach; (2) no evidence of tumors invading adjacent organs, paraaortic lymph node enlargement or distant metastasis demonstrated by abdominal computed tomography and/or abdominal ultrasound and posteroanterior chest radiography; and (3) a D1/D1 +/D2 lymphadenectomy with a curative R0 resection. The following exclusion criteria were applied: (1) no routine blood examination before surgery, (2) metastatic disease, (3) neoadjuvant chemotherapy, (4) malignant disease in other organs, (5) incomplete/inaccurate medical records, (6) follow-up less than 3 months. Finally, 1786 patients were included in the study (Supplemental Fig. 1). All surgical procedures, including D2 lymphadenectomy, were performed according to the guidelines of the Japanese Gastric Cancer Association [8]. Staging was performed according to the corresponding seventh edition of the AJCC Staging Manual [9]. Adjuvant chemotherapy using 5-fluorouracil (5-FU)-based regimens (mostly oxaliplatin with either Xeloda or S-1) was recommended to the majority of patients with advanced GC [10, 11].
Recurrences were categorized as locoregional, peritoneal, or distant [12]. Locoregional recurrence included dominant masses in the gastric bed, upper abdominal retroperitoneal lymph nodes, or anastomotic recurrence. Peritoneal recurrence was documented by positive cytology in ascitic fluid or by convincing peritoneal nodules on cross-sectional imaging. Distant metastases were further defined according to the specific organ involved. Periumbilical and cervical lymph nodes were considered distant metastases. Multiple recurrences in the same area (e.g., anastomotic and gastric bed) were coded in a single category. The mode of recurrence detection was also recorded as histologic, radiologic, or clinical. Recurrence was considered histologically proven if it was documented by surgical biopsy, needle biopsy, or by cytology of appropriate fluid. Radiologic proof of recurrence was specifically reviewed in the context of the clinical situation and usually required sequential imaging demonstrating progression of metastatic lesions. In rare situations, specific recurrences were detected by clinical examination alone, such as in progressing subcutaneous nodules, or obvious diffuse peritoneal recurrence. Mediastinal lymph node recurrence was considered locoregional for gastroesophageal junction tumors and distant for the other gastric tumors. Tumors involving the ovaries (Krukenberg’s tumor) were considered peritoneal. Multiple metastatic foci were considered 1 recurrence episode if they were diagnosed within a 3-month period. Although some patients had multiple recurrence episodes, this study analyzed the initial recurrence episode as defined above.
Definition of inflammation-based indicators
Patients routinely underwent blood testing during the 7 days before surgery. All results of blood tests performed in the 7 days before surgery were obtained from local pathology databases [4]. These included the full blood count (FBC), Alb level, and C-reactive protein (CRP) level (where available). The SIS was defined as follows: patients with Alb level < 40 g/l and LMR < 4.44 were assigned a score of 2; patients with either Alb level ≥ 40 g/l or LMR ≥ 4.44 were assigned a score of 1; and patients with both Alb level ≥ 40 g/l and LMR ≥ 4.44 were assigned a score of 0 [7]. The Glasgow prognostic score (GPS) was derived as previously described [3]. The optimal cutoff levels for NLR and PLR were calculated by the software X-tile (Yale University, New Haven, CT, USA) [13]. In the current study, the novel cutoff value of LMR was 3.4 determined by the software X-tile (Supplemental Fig. 2).
Follow-up investigation
A postoperative follow-up assessment was performed every 3 months for 2 years and then every 6 months during years 2–5. The final follow-up evaluation was conducted in December 2017. Most routine follow-up appointments included a physical examination, laboratory testing (including cancer antigen [CA] 19-9, CA72-4, and carcinoembryonic antigen [CEA]-level measurements), chest radiography, and abdominopelvic ultrasonography or computed tomography, along with an annual endoscopic examination. Overall survival (OS) was defined as the time from surgery to death from any cause or to the time of censoring on the date of the last follow-up.
Statistical methods
Categorical variables were analyzed using the Chi-square test or Fisher’s exact test, whereas continuous variables were analyzed using Student’s t tests. Survival curves were constructed according to the Kaplan–Meier method, and differences between curves were analyzed using the log-rank test. Variables that significantly affected survival were investigated by multivariate analysis according to the Cox regression model. Concordance indices (C-indices) were calculated to evaluate the discriminatory power of the inflammation-based scores. The prognostic abilities of the scores were compared by generating time-dependent receiver operating characteristic (t-ROC) curves and by calculating the estimated area under the curve (AUC). The t-ROC curve analysis is an extension of the ROC curve, which assesses the discriminatory power of continuous variables for time-dependent disease outcomes [14]. In addition to visually comparing the ROC curves, the AUC can be calculated [15]. Sequential AUCs were compared between two scores using independent and identically distributed representations of AUC estimators. All tests were 2-sided, and statistical significance was inferred at a P value of < 0.05. Statistical analyses were performed using SPSS for Windows version 18.0 (SPSS Inc., Chicago, IL, USA) and R ver. 3.1.2 (R Foundation for Statistical Computing, Vienna, Austria). The R packages “rms” and “timeROC” were used for calculation of the C-index and t-ROC analysis, respectively.
Results
Clinicopathological characteristics
Totally, 1786 patients were included in the study. There were 1356 (75.9%) males and 430 (24.1%) females. The median patient age at the time of surgery was 61 years [interquartile range (IQR): 55–69 years]. Based on the TNM staging system, 514 (28.8%), 430 (24.1%), and 842 (47.1%) of the patients had stages I, II, and III disease, respectively. All patients were categorized into the following three groups according to the SIS: 427 patients (23.7%) in the SIS = 0 group, 725 (40.6%) in the SIS = 1 group, 634 (35.5%) in the SIS = 2 group (Supplemental Table 1).
Survival analysis
The median follow-up period was 51.0 months (range 3–101 months). The 5-year OS rates for the entire cohort were 68.0%. Univariate analysis showed that all the inflammatory indicators associated with OS included the SIS, Alb level, LMR ≥ 3.4, NLR and PLR (all P < 0.05, Table 1). In addition, other variables, including age, body mass index (BMI), the American Society of Anesthesiologists (ASA) score, tumor location, diameter, vascular invasion and perineural invasion, had a significant effect on OS (all P < 0.05, Table 1). In multivariate analyses, the SIS was not an independent factor for prognosis (P > 0.05, Table 1). However, normal Alb level (≥ 40 g/l) and LMR ≥ 3.4 were still associated with good OS (both P < 0.05, Table 1).
The prognostic effect of the SIS was evaluated by preoperative Alb and LMR, and the novel cutoff value of LMR, which exhibits superior prognostic prediction, was determined at 3.4 by the software X-tile. Therefore, we combined Alb level and LMR to generate four subgroups. We found significant differences among the four subgroups (P < 0.05, Fig. 1a). In the normal Alb subgroup, the survival of patients with LMR ≥ 3.4 was similar to that of patients with LMR < 3.4 (P > 0.05, Fig. 1a). In the decreased Alb subgroup, the survival of patients with LMR ≥ 3.4 was better than that of patients with LMR < 3.4 (P < 0.05), but the survival of both subgroups were worse than that of the normal Alb subgroup (all P < 0.05).

a Recombination of preoperative serum Alb level and LMR; b Kaplan–Meier analysis for OS according to the mSIS. c Association of the SIS with the OS in the surgery alone group. d Association of the SIS with the OS in the adjuvant chemotherapy group
Establishment of the modified SIS (mSIS)
Based on the results above, we constructed a modified SIS (mSIS) defined as follows: patients with Alb level ≥ 40 g/l were assigned a score of 0; patients with both Alb level < 40 g/l and LMR ≥ 3.4 were assigned a score of 1; and patients with both Alb level < 40 g/l and LMR < 3.4 were assigned a score of 2 (Supplemental Table 2). Supplemental Fig. 3 depicts the association between the mSIS and SIS as a bubble chart. The distribution of mSIS values was relatively balanced mSIS = 0: 781 (43.7%), mSIS = 1: 614 (34.4%), mSIS = 2: 391 (221.9%). The mSIS and SIS values were different in up to 32.6% of patients (Supplemental Fig. 3).
The relationship between clinicopathological factors and the mSIS is given in Table 2. The mSIS was significantly higher in patients who were older than 65 years with high ASA scores (both P < 0.05, Table 2). Additionally, proximal tumor location, larger tumor size, higher pTNM stage, vascular involvement, perineural invasion, and postoperative adjuvant chemotherapy were significantly associated with higher mSIS (all P < 0.05, Table 2). The higher mSIS was also found to be associated with more prevalence of local recurrence, peritoneal metastasis, and distant metastasis (all P < 0.001, Table 2).
mSIS independently predicts OS
Three Kaplan–Meier curves for the 5-year OS rates were constructed according to the mSIS (mSIS = 0: 78.6%, mSIS = 1: 66.0%, mSIS = 2: 50.2%, log-rank test: P < 0.05, Fig. 1b). Furthermore, the 5-year OS rates were differed significantly according to the mSIS in both surgery alone group and postoperative adjuvant chemotherapy group (both P < 0.05, Fig. 1c, d). Multivariate analyses revealed that mSIS was associated with OS (mSIS = 1: hazard ratio [HR] = 1.250, P = 0.038; mSIS = 2: HR = 1.728, P < 0.001) and RFS (mSIS = 1: hazard ratio [HR] = 1.248, P = 0.055; mSIS = 2: HR = 1.648, P < 0.001, Table 3). In addition, when stratified by TNM stage, significant differences in survival were found for patients with mSIS of 0, 1 and 2 in stages I, II and III subgroups (all P < 0.05, Fig. 2).

Kaplan–Meier analysis of OS of GC patients at each TNM stage according to the mSIS. a Association of the mSIS with the OS of patients with stage I GC. b Association of the mSIS with the OS of patients with stage II GC. c Association of the mSIS with the OS of patients with stage III GC
Prognostic value of mSIS
To evaluate the prognostic value of the mSIS and SIS, we constructed t-ROC curves (Fig. 3). The t-ROC curve of the mSIS was persistently superior to that of the mSIS throughout the observation period. In addition, the mSIS had a higher C-index than did the SIS (0.616 vs. 0.597). Furthermore, when we compared the predictive performance for OS after 1, 3, and 5 years of follow-up, the AUC values of the mSIS were significantly higher than those of the SIS at 3 and 5 years after operation (3 years: 0.641 vs. 0.620, P = 0.011; 5 years: 0.636 vs. 0.616, P = 0.008) and were similar to those of the SIS at 1 year after operation (1 years: 0.611 vs. 0.601, P = 0.452).

Time-dependent ROC curves for the mSIS and SIS. The horizontal axis represents year after surgery, and the vertical axis represents the estimated AUC for survival at the time of interest. Red and blue solid lines represent the estimated AUCs for the mSIS and SIS, respectively, and broken lines represent the 95% confidence intervals for each AUC
Of the 1786 patients in our cohort with complete data, 237 also had GPS values available for analysis. In subgroup analysis of patients with GPS, we found that the mSIS remained the only significant independent biomarker (mSIS = 1: HR = 2.312, P = 0.008; mSIS = 2: HR = 3.950, P < 0.001, Supplemental Table 3). Additionally, C-index (0.636 vs. 0.567) and t-ROC curve (Supplemental Fig. 4) for the mSIS were also superior than those for the GPS.
Discussion
Since Virchow originally established a link between cancer and inflammation in the nineteenth century, an increasing number of investigations have revealed that the levels of inflammatory markers also play an important role in tumor progression and metastasis [2, 16]. Recently, a novel inflammation-based prognostic score, the SIS, based on the preoperative serum Alb level and LMR, was reported to have prognostic value in clear cell renal cell carcinoma and colorectal cancer, [6, 7] which considers both influences of nutritional status and systemic inflammation on the prognosis of tumors. It can reflect the comprehensive effects of nutrition and systemic inflammation on tumor progression. Therefore, SIS is a better indicator than other single nutritional or inflammatory markers. However, whether the SIS can predict the prognosis of GC patients remains unclear. In a large cohort of resectable GC patients, our study found that SIS is associated with the prognosis; however, it is not an independent prognostic factor. The cutoff value of LMR for the SIS in previous studies was 4.44 based on the median value of LMR in renal clear cell carcinoma, [7] and this value showed good prognostic efficacy in colorectal cancer. Gu et al. found that the cutoff value of LMR varies in many types of cancer, [17] which may be related to yet unknown clinicopathological parameters and/or each tumor entity on its own [18]. Therefore, further research is needed for the utilization of the SIS and LMR in GC.
In this study, the cutoff value of LMR was re-calculated by the software X-tile. By a novel time-dependent cutoff value analysis based on survival information, X-tile plot identified the cutoff value with minimum P values from log-rank χ2 statistics for the categorical biomarkers in terms of survival, which has been widely used in previous studies [4, 19, 20]. According to the survival data, the optimal cutoff value of LMR was identified to be 3.4 using the X-tile software, and multivariable analysis also demonstrated that LMR ≥ 3.4 was associated with favorable OS. By comparing the distribution of mSIS and SIS values, we found that the mSIS and SIS were different in more than 30% patients. Additionally, based on our results, elevated mSIS was associated with a number of variables that were previously shown to be predictive of poor outcomes.
Recently, t-ROC analysis, which was developed to apply ROC curve analysis to time-dependent variables, [14] has been used in some studies. The advantage of this method is that it enables the analysis of survival data with censoring using ROC curves, which is a popular method of determining sensitivity and specificity. Additionally, the significance of individual prognostic factors can be visually assessed [6]. The t-ROC curve for the mSIS was persistently superior to that for the SIS after surgery. Moreover, the mSIS yielded a higher C-index than did the SIS. The reason that mSIS is superior to SIS may be that we reconfirm the optimal cut-off point of LMR for the prognosis of GC using the X-tile, and mSIS was accurately grouped according to the survival curve of each group. Therefore, the mSIS can predict the prognosis of GC more accurately and exhibits a higher prognostic value than the SIS. The effect of mSIS on tumor prognosis is mainly determined by LMR and Alb level. LMR consists of lymphocytes and monocytes. As the basic components of the adaptive and innate immune system and the cellular basis of immunosurveillance and immunoediting, lymphocytes can enhance cancer immune-surveillance to inhibit tumour cell proliferation, invasion and metastasis [21]. Azimi et al. found that the presence of tumor-infiltrating lymphocytes is associated with improved outcomes in a variety of cancers, possibly due to tumor-infiltrating lymphocyte-induced antitumor activity and inhibition of angiogenesis [22]. Thus, lymphopenia has been associated with poor outcomes in cancer patients. The circulating monocytes may contribute to both tumor growth and reduced immunosurveillance, which is supported by previous literature [23]. Furthermore, monocytes have been proposed to promote tumor metastasis through circulation and the tumor–monocyte–endothelial interaction [24]. Therefore, LMR plays an important role in the prognosis of gastric cancer. The level of Alb is usually regarded as a good index for malnutrition and cachexia in patients with advanced cancer. Crumley and Lien found that hypoalbuminemia was associated with poor survival in GC, [25, 26] which was also observed in the present study. The mSIS, which is based on both LMR and Alb level, may enable a better appreciation of the effects of the tumor on both ongoing systemic inflammation and malnutrition.
The GPS, based on preoperative serum Alb and CRP levels, has been reported to be associated with survival in numerous cancers [27,28,29,30] and shown to be a reliable inflammatory-based scoring system. Melling et al. found that the GPS also represents an independent prognostic factor for long-term outcomes in resected GC patients [31]. Therefore, the current study also attempted to clarify the utility of the GPS in comparison to that of the mSIS. We found that the mSIS yielded a better t-ROC curve and higher C-index than did the GPS, indicative of a superior prognostic predictive power. As CRP level is not routinely detected preoperatively in many centers, the clinical application of the GPS has some limitations. Thus, as a simple and easily available inflammatory scoring system, the mSIS, may be may be used as an alternative to the GPS. In addition, the mSIS can be considered a supplement to cross-sectional imaging, endoscopic ultrasound and endoscopic examination to improve the risk stratification of GC patients before treatment and postoperative follow-up.
Recently, Sato et al. also found that SIS can predict the survival in a small cohort of patients with pT2–4 GC after radical gastrectomy, and they found that the SIS was not an independent prognostic factor, [32] this finding was consistent with the current study. Compared with the study of Sato, our study has the following advantages. First, this is a large sample study which included 1786 patients undergoing radical gastrectomy. Second, because the SIS was not an independent prognostic factor, we re-evaluated the optimal cut-off value of LMR by scientific statistical method, then we combined with preoperative Alb, and established the mSIS based on the 5-year survival rate of patients. Finally, we results showed that mSIS was an independent prognostic factor, and the time-ROC and C-index confirmed that mSIS was a superior predictor to SIS and GPS.
Our study has certain limitations. First, as a retrospective study, it may have been subject to selection bias. Second, although we excluded patients with neoadjuvant therapy, we are unsure of whether all patients were in the same state before blood sampling, and the results of this study are not suitable for GC patients after neoadjuvant therapy. Despite these limitations, our study is the first to demonstrate that the preoperative mSIS is a novel and simple prognostic factor for GC and can be used as a part of the preoperative risk stratification process and the postoperative follow-up to formulate the individualized treatment for GC patients.
References
Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–86.
Balkwill F, Mantovani A. Inflammation and cancer: back to Virchow? Lancet. 2001;357(9255):539–45.
McMillan DC. The systemic inflammation-based Glasgow Prognostic Score: a decade of experience in patients with cancer. Cancer Treat Rev. 2013;39(5):534–40.
Lin JP, Lin JX, Cao LL, et al. Preoperative lymphocyte-to-monocyte ratio as a strong predictor of survival and recurrence for gastric cancer after radical-intent surgery. Oncotarget. 2017;8(45):79234–47.
Kim EY, Lee JW, Yoo HM, et al. The platelet-to-lymphocyte ratio versus neutrophil-to-lymphocyte ratio: which is better as a prognostic factor in gastric cancer? Ann Surg Oncol. 2015;22(13):4363–70.
Suzuki Y, Okabayashi K, Hasegawa H, et al. Comparison of preoperative inflammation-based prognostic scores in patients with colorectal cancer. Ann Surg. 2018;267(3):527–31.
Chang Y, An H, Xu L, et al. Systemic inflammation score predicts postoperative prognosis of patients with clear-cell renal cell carcinoma. Br J Cancer. 2015;113(4):626–33.
Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer. 2011;2:113–23.
Edge SB, Byrd D. AJCC Cancer Staging Manual. 7th ed. New York: Springer; 2010.
Bang YJ, Kim YW, Yang HK, et al. Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): a phase 3 open-label, randomised controlled trial. Lancet. 2012;379(9813):315–21.
Sasako M, Sakuramoto S, Katai H, et al. Five-year outcomes of a randomized phase III trial comparing adjuvant chemotherapy with S-1 versus surgery alone in stage II or III gastric cancer. J Clin Oncol. 2011;29(33):4387–93.
D’Angelica M, Gonen M, Brennan MF, et al. Patterns of initial recurrence in completely resected gastric adenocarcinoma. Ann Surg. 2004;240(5):808–16.
Camp RL, Dolled-Filhart M, Rimm DL. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin Cancer Res. 2004;10(21):7252–9.
Heagerty PJ, Lumley T, Pepe MS. Time-dependent ROC curves for censored survival data and a diagnostic marker. Biometrics. 2000;56(2):337–44.
Rodriguez-Alvarez MX, Meira-Machado L, Abu-Assi E, Raposeiras-Roubin S. Nonparametric estimation of time-dependent ROC curves conditional on a continuous covariate. Stat Med. 2016;35(7):1090–102.
Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–44.
Gu L, Li H, Chen L, et al. Prognostic role of lymphocyte to monocyte ratio for patients with cancer: evidence from a systematic review and meta-analysis. Oncotarget. 2016;7(22):31926–42.
Koh YW, Park CS, Yoon DH, et al. Should the cut-off values of the lymphocyte to monocyte ratio for prediction of prognosis in diffuse large B-cell lymphoma be changed in elderly patients? Eur J Haematol. 2014;93(4):340–8.
Zheng G, Feng F, Guo M, et al. Harvest of at least 23 lymph nodes is indispensable for stage N3 gastric cancer patients. Ann Surg Oncol. 2017;24(4):998–1002.
Qureshi YA, Sarker SJ, Walker RC, Hughes SF. Proximal resection margin in Ivor–Lewis oesophagectomy for cancer. Ann Surg Oncol. 2017;24(2):569–77.
Dunn GP, Old LJ, Schreiber RD. The immunobiology of cancer immunosurveillance and immunoediting. Immunity. 2004;2:137–48.
Azimi F, Scolyer RA, Rumcheva P, et al. Tumor-infiltrating lymphocyte grade is an independent predictor of sentinel lymph node status and survival in patients with cutaneous melanoma. J Clin Oncol. 2012;21:2678–83.
Augier S, Ciucci T, Luci C, Carle GF, Blin-Wakkach C, Wakkach A. Inflammatory blood monocytes contribute to tumor development and represent a privileged target to improve host immunosurveillance. J Immunol. 2010;12:7165–73.
Evani SJ, Prabhu RG, Gnanaruban V, Finol EA, Ramasubramanian AK. Monocytes mediate metastatic breast tumor cell adhesion to endothelium under flow. FASEB J. 2013;8:3017–29.
Crumley AB, Stuart RC, McKernan M, McMillan DC. Is hypoalbuminemia an independent prognostic factor in patients with gastric cancer? World J Surg. 2010;34(10):2393–8.
Lien YC, Hsieh CC, Wu YC, et al. Preoperative serum albumin level is a prognostic indicator for adenocarcinoma of the gastric cardia. J Gastrointest Surg. 2004;8(8):1041–8.
Forrest LM, McMillan DC, McArdle CS, et al. A prospective longitudinal study of performance status, an inflammation-based score (GPS) and survival in patients with inoperable non-small-cell lung cancer. Br J Cancer. 2005;92(10):1834–6.
Al MA, Bartlett JM, Canney PA, et al. Evaluation of an inflammation-based prognostic score (GPS) in patients with metastatic breast cancer. Br J Cancer. 2006;94(2):227–30.
Crumley AB, McMillan DC, McKernan M, et al. Evaluation of an inflammation-based prognostic score in patients with inoperable gastro-oesophageal cancer. Br J Cancer. 2006;94(5):637–41.
Glen P, Jamieson NB, McMillan DC, et al. Evaluation of an inflammation-based prognostic score in patients with inoperable pancreatic cancer. Pancreatology. 2006;6(5):450–3.
Melling N, Gruning A, Tachezy M, et al. Glasgow Prognostic Score may be a prognostic index for overall and perioperative survival in gastric cancer without perioperative treatment. Surgery. 2016;159(6):1548–56.
Sato B, Kanda M, Tanaka C, et al. Significance of preoperative systemic inflammation score in short-term and long-term outcomes of patients with pathological T2–4 gastric cancer after radical gastrectomy. World J Surg. 2018. https://doi.org/10.1007/s00268-018-4597-7.
Acknowledgements
Scientific and technological innovation joint capital projects of Fujian Province, China (no. 2016Y9031). Minimally invasive medical center of Fujian Province (no. [2017]171). Project supported by the Science Foundation of the Fujian Province, China (Grant no. 2018J01307). Startup Fund for scientific research, Fujian Medical University (no. 2016QH024).
Author information
Authors and Affiliations
Contributions
LJX, LJP, ZCH, HCM and LP conceived of the study, analyzed the data, and drafted the manuscript; TRH, LP, XJW, WJB, and LP helped revise the manuscript critically for important intellectual content; LJ, CQY, CLL, and LM helped collect data and design the study.
Corresponding authors
Ethics declarations
Conflict of interest
There are no conflicts of interest or financial ties to disclose from any of author.
Human rights statement
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions.
Informed consent
Informed consent or substitute for it was obtained from all patients for being included in the study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Lin, JX., Lin, JP., Xie, JW. et al. Prognostic importance of the preoperative modified systemic inflammation score for patients with gastric cancer. Gastric Cancer 22, 403–412 (2019). https://doi.org/10.1007/s10120-018-0854-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10120-018-0854-6