
Abstract
The aim of this in-vitro study was to compare the performance of laser-based (DIAGNOdent, KaVo, Biberach, Germany) and LED-based (Midwest Caries I.D., DENTSPLY Professional, New York, USA) caries detectors in the detection of occlusal caries in permanent molars. The study consisted of 129 visually sound or non-cavitated pits or fissures in 82 extracted permanent human molar teeth. Two trained examiners used the laser-based and LED-based caries detectors to examine the fissures for caries. The teeth were then sectioned at the surfaces suspected of containing occlusal caries and histologically evaluated using stereomicroscopy as a gold standard. Inter-examiner reliability of the caries detector examination was assessed using Cohen’s Kappa statistics. The sensitivity, specificity, and accuracy in diagnosing occlusal caries using the two devices were calculated according to appropriate cut-off scores. Receiver operating characteristic (ROC) curves were also determined to compare the diagnostic performance of the devices in occlusal caries diagnosis. The cut-off level of significance was taken as p = 0.005. Cohen’s Kappa showed substantial agreement for the laser-based caries detector (0.74), and almost perfect agreement for the LED-based (0.89) caries detector. The specificity of the laser-based device varied from 0.49 to 0.97 at T1 and T2. Its sensitivity varied from 0.33 to 0.65 at T1 and T2. The specificity of the LED-based device varied from 0.48 to 0.56 at T1 and T2. Its sensitivity varied from 0.65 to 0.84 at T1 and from 0.80 to 0.84 at T2. Taking the limitations of the current study into consideration, the DIAGNOdent laser pen was more accurate in determining when teeth were free of occlusal caries than was the Midwest Caries I.D. LED-based device, although the Midwest Caries I.D. device more often revealed the presence of occlusal caries than did the DIAGNOdent pen.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Dental caries are an important public health problem worldwide [1] and the detection of caries lesions is key in preventing and treating dental caries [2]. Modern management of dental caries has three major components: prevention, control, and appropriate diagnosis of the disease and detection of pathological changes (that is, detection of lesions at their earliest stages of formation) [3, 4]. However, the detection of small lesions, especially on occlusal surfaces, is still difficult for dental professionals. The difficulty of precise detection is related to several factors, including the complex anatomy of pits and fissures [1, 5, 6]; the superimposition of structures during radiographic evaluation, making it difficult to obtain a clear view of the area of interest; and an increase in the number of hidden carious lesions due to the widespread use of fluoride [7, 8]. Therefore, studies about the processes and results of treatment decisions are necessary to determine whether new and existing methods are being used effectively [3].
Clinicians need resources of high diagnostic accuracy to both detect incipient caries and monitor the remineralization of lesions [9]. Currently, several methods are used to detect occlusal caries, with visual inspection being one of the most common methods. Visual inspection is non-invasive [10–12] and highly specific, but also has low sensitivity values and reproducibility [13, 14]. A combination of visual inspection with bite-wing radiographic examination has shown good results in detecting dentinal occlusal caries [5]. Novel diagnostic systems for caries detection include an electronic caries monitor (ECM), fiber-optic transillumination (FOTI and DiFOTI), visible light fluorescence (QLF), laser fluorescence (DIAGNOdent), optical coherence tomography (OCT), and ultrasound [15].
Incident light wavelength shows differences between sound (healthy) enamel and caries lesions through changes in the reflection of this light on the tooth surface. While the DIAGNOdent 2095, introduced in 1998, was the first introduced DIAGNOdent device to detect these differences, DIAGNOdent pen 2190 (introduced in 2005) is now the more popular diagnostic tool [16]. One reason is that the DIAGNOdent pen is smaller in diameter than the original DIAGNOdent device [16]. The DIAGNOdent devices are based on the capturing, analysis, and quantification of fluorescence emitted from bacterial porphyrins and other chromophores when the tooth surface is illuminated by a diode laser at a wavelength of 655 nm [17]. These fluorescence characteristics are different when compared for healthy and dematerialized teeth. Additionally, the DIAGNOdent is used to detect the absence or presence of caries lesions. Several studies have shown the effectiveness of the DIAGNOdent pen for detection of occlusal caries [16, 18–21]. It was found that both devices performed similarly, with the pen producing slightly higher readings and having a slightly lower sensitivity. In addition, Kühnisch et al. showed that the cut-off point used for the values of the DIAGNOdent for the diagnosis of caries lesions cannot be used for the DIAGNOdent pen [16]. However, both devices have been used as adjunct caries detection devices [19, 20]. The DIAGNOdent pen device could permit quantitative evaluation of smooth surface and occlusal caries lesions. Using a small laser, the system produces an excitation wavelength of 655 nm that produces a red light [15]. This method allows quantifiable, noninvasive examination of the tooth surface, thereby facilitating early detection of lesions so that preventive measures may be adopted to prevent caries progression [22]. Several studies have examined the effectiveness of this method for the detection of occlusal caries lesions both in vitro [5, 23–25] and in vivo [26–29]. Histological examination is the gold standard in in vitro studies related to dental caries [5, 23–25].
The Midwest Caries I.D. is the newest tool for the detection of caries lesions. Healthy teeth are generally more translucent than are teeth with decalcified enamel. For this reason, there is a difference in optical appearance for healthy teeth and demineralized teeth. In the Midwest Caries I.D. device, the reflectance and refraction of the LED off the tooth surface is captured by fiber-optics and converted into an electrical signal for analysis. The device contains a microprocessor with a computer-based algorithm and differentiates according to the presence or absence of changes in optical translucency and opacity. The LED changes from green to red (with an accompanying audible signal) with demineralization, confirming the presence of caries [30]. The detection hand piece is a portable, handheld device designed to aid in detecting caries in non-restored occlusal pits and fissures and interproximal areas on adult posterior teeth. To our knowledge, there are no reports on the effectiveness of the Midwest Caries I.D. in diagnosing dental caries. For that reason, the aim of the present study was to investigate the validity of the Midwest Caries I.D. for occlusal caries detection compared to the DIAGNOdent pen device.
Materials and methods
A total of 129 visually sound or non-cavitated pits or fissures in 82 fresh extracted permanent human molar teeth were used in this study. The teeth were stored separately from each other in distilled water, and were cleaned with water and a rotating bristle brush. All calculus and other remnants were removed completely from the pits or fissures. Drawings of the occlusal surfaces at the selected sites were then made in order to indicate the suspected sites for the examiners. The study was approved by the local ethics committee.
Examination methods
Caries lesions on the selected sites of the occlusal surfaces were examined by two experienced examiners using the laser-based and LED-based caries detectors as follows:
-
DIAGNOdent pen readings
A DIAGNOdent 2190 Pen with Cylindrical Tip (DIAGNOdent 2190, KaVo, Biberach, Germany) was used for laser fluorescence examination to take measurements after it had been calibrated with the ceramic standard. The performance was assessed according to the cut-off limits suggested by Lussi and Helwig [31], as follows: Score 0 (0–13 sound); score 1 (14–20, caries in the enamel); score 2 (21–99, caries in the dentin). The teeth were assessed according to the manufacturer’s instructions. The laser tip was rotated around its long axis after being positioned on a dried surface of the target site; this tooth calibration was performed before each measurement. In order to identify the area where the caries process was most advanced, the highest value was taken. The values displayed on the screen were then recorded.
-
Midwest Caries I.D. readings
Midwest Caries I.D. (Midwest Caries I.D., DENTSPLY Professional, New York, USA) was used to take measurements after calibration with the ceramic standard. For occlusal caries, wet pits and fissures were probed in direct contact. The tip of the probe was always parallel to the long axis of the occlusal area. The emission of a red light (with an audible tone) indicated the presence of decay or decalcification of the tooth structure; emission of a green light without an audible tone indicated the test site was sound. The extent of decay was further clarified by the three types of audible tones that accompanied emission of the red light. The performance was assessed according to the cut-off limits suggested by the manufacturer, as follows: Score 0 (No signal / Green light, sound); score 1 (Slow or medium signal / Red light, caries in the enamel); score 2 (Rapid or continuous signal / Red light, caries in the dentin).
After completion of all the examinations, buccolingual sections of the teeth were cut perpendicular to the suspected occlusal sites using an Isomet (Buehler, Lake Bluff, IL, USA) for the purpose of histological validation, which is considered the gold standard. One calibrated, blinded examiner evaluated teeth slices using a stereomicroscope with a magnification of x25 under reflected light (Leica Microsystems, Germany). The depth of enamel demineralization was assessed at the area showing the greatest opacity along the direction of the rods. The depth of dentin demineralization was measured at the area where the color changed from brownish/yellowish to gray along a line at a right angle to the enamel-dentin junction toward the pulp [10]. The examiner was not aware of the previous diagnostic results. As a measure of histological assessment reliability, 25 of the sections were re-examined after 20 days. Almost perfect agreement was reached between the first and the second histological examination.
The criteria for each diagnostic method used are summarized in Table 1.
Statistical analysis
Inter-examiner reliability of the caries detector examinations was assessed using Cohen’s Kappa statistics. Sensitivity, specificity, and accuracy in diagnosing occlusal caries using the two devices were calculated according to appropriate cut-off scores. The McNemar test was also calculated to compare their performance (sensitivity, specificity, accuracy, and area under the receiver operating characteristic [ROC] curve) of both devices. The area under the ROC curve was measured for both devices to compare their diagnostic performance for occlusal caries diagnosis at Threshold 1 (considering both the gold standard scores 1 and 2 as evidence of disease) and Threshold 2 (considering only the gold standard score 2 as evidence of disease) [10]. Analyses were performed using the SPSS statistics program for Windows, version 11.5 (SPSS Inc., Chicago, IL, USA). The cut-off level of significance was taken as p = 0.005.
Results
The histological examination revealed that 54 of the 129 occlusal sites were caries-free (score 0), 48 had caries in the enamel (score 1), and 27 had caries in the dentin (score 2). The Midwest Caries I.D. examination revealed 75 caries-free occlusal sites (score 0), 27 caries in the enamel (score 1), and 27 caries in the dentin (score 2). The DIAGNOdent pen examination revealed 33 caries-free occlusal sites (score 0), 21 caries in the enamel (score 1), and 75 caries in the dentin (score 2). Table 2 is a cross table that shows the distribution and number of teeth according to diagnostic methods and caries classification. High inter-examiner agreement was present for the Midwest Caries I.D. readings and DIAGNOdent pen readings in the present study (κ: 0.89 and κ: 0.74, respectively).
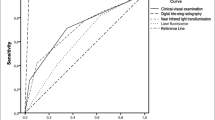
The sensitivity, specificity, accuracy, and ROC of the both devices and their McNemar test results for caries detection are shown in Table 3. The specificity of the laser-based device varied from 0.49 to 0.97 at T1 and T2. Its sensitivity varied from 0.33 to 0.65 at T1 and T2. The specificity of the LED-based device varied from 0.48 to 0.56 at T1 and T2. Its sensitivity varied from 0.65 to 0.84 at T1 and from 0.80 to 0.84 at T2. The accuracy of the laser-based device varied from 0.77 to 0.78 at T1 and from 0.47 to 0.50 at T2; in comparison, the accuracy of the LED-based device varied from 0.78 to 0.83 at T1 and from 0.88 to 0.92 at T2. The area under the ROC curve (Az) of the laser-based device varied from 0.755 to 0.769 at T1 and from 0.697 to 0.729 at T2. The ROC of the LED-based device varied from 0.682 to 0.696 at T1 and from 0.669 to 0.678 at T2.
Discussion
Early caries detection is crucial in the management of dental caries, as early lesions can be treated preventively with increased presence of fluoride, improved oral hygiene, and reduced sugar intake. Such preventive therapy can result in the delayed progression, arrest, or even remineralization of lesions. Due to the shift from operative to non-operative interventions [32], the accurate early detection of caries lesions has become a prerequisite for measures to arrest caries progression. A way of monitoring the success of this preventive approach is integral in the search for new detection devices [33]. Thus, several novel techniques have been introduced for the diagnosis of caries by dental practitioners. The DIAGNOdent is one of the most common and familiar detection devices. The Midwest Caries I.D. is the newest device, but dentists remain unsure about its clinical and laboratory performance for caries detection, and more research into its performance must be planned. To the best of our knowledge, this is the first study testing the LED-based Midwest Caries I.D. device for the detection of occlusal caries lesions in the dental literature. For that reason, the present study focused on the validity of the Midwest Caries I.D. for detecting initial occlusal caries lesions by comparing the device with the DIAGNOdent pen values.
Several studies have included the DIAGNOdent pen device in testing whether devices accurately detect occlusal caries. These studies showed the high reproducibility of the device and its usefulness for occlusal caries detection. In addition, Farah and colleagues [18] found that increased DIAGNOdent pen readings can indicate enamel hypomineralization in the absence of dental caries. In the study by Kühnisch and colleagues [16], DIAGNOdent and DIAGNOdent pen were compared; it was determined that the devices should only be used in dental practice as adjunct tools due to their imperfect reproducibility, a finding concurred with by Huth and colleagues [20]. As noted earlier, Kühnisch et al. also found that the DIAGNOdent pen had higher means and continuously higher range values than did DIAGNOdent [16], and that the values for the DIAGNOdent cannot be used for the DIAGNOdent pen. These findings have been contradicted; one study found that both can be used as adjunct tools by dentists and students, as no difference existed between their results [18]. However, the authors stressed that the DIAGNOdent pen should be used additionally for visual inspection and for dental radiographs.
Occlusal surfaces have shown to be more susceptible than other surfaces to caries [34]. The conditions for detection of caries are better in in vitro studies as compared to in vivo studies due to the absence of bacterial plaque, acquired pellicle, presence of saliva, or soft tissue [35, 36]. However, laboratory studies permit histopathological validation for more accurate assessment of the lesions’ extent [37, 38]. Histological examination in the present study revealed a limited percentage of dentine caries and a higher percentage of sound teeth, most likely affecting the results of the present study. Although in vivo diagnosis studies are performed under clinical conditions, caries lesions can only be evaluated operatively where disease is thought to be present. One drawback is that this method cannot detect false-negative results. For this reason, the present study used an in vitro method to investigate the performance of the Midwest Caries I.D. device for occlusal caries detection. However, further studies evaluating teeth indicated for extraction in vivo, followed by histopathological validation in vitro, are needed to more correctly extrapolate results for clinical practice.
Studies related to the performance of the DIAGNOdent pen and other devices for caries detection have used either permanent or primary teeth (some studies used one or the other) [16, 20, 21, 27]. In this study, only caries in the permanent molars were evaluated because primary teeth are contraindicated for the Midwest Caries I.D. device, which can only be used for permanent dentition.
The working principle of the two devices is different. The DIAGNOdent pen uses a small laser with an excitation wavelength of 655 nm that produces a red light, and displays a numerical value on two LED displays. The first value displays the current reading; the second displays the peak reading for the examination. In contrast, the Midwest Caries I.D. device does not produce numerical values to classify caries lesions, and the examination is therefore subjective. It emits a red or green light and an audible tone that indicate the presence of decay or decalcification of the tooth structure. There is only one button on the Midwest Caries I.D. device and it is more easily used than is the DIAGNOdent pen. To differentiate the emitting signals accurately and compare the results from the Midwest Caries I.D. device to scores from histological examination and the DIAGNOdent pen, the slow and medium signals were combined and their differentiation from the rapid or continuous signals was evaluated.
According to the present results, Midwest Caries I.D. values suggest that higher sensitivity and unacceptably lower specificity at Threshold 2 indicating a high risk of false-positive results. The sensitivity of the Midwest Caries I.D. values was higher than that of DIAGNOdent pen at Threshold 2; thus, it is suggested that the Midwest Caries I.D. provides more accurate diagnosis of occlusal caries lesions than does DIAGNOdent pen, in contrast to the findings with Threshold 1 values. The specificity of the DIAGNOdent pen values was higher than that of the Midwest Caries I.D. in both the threshold values. The diagnostic performance of the DIAGNOdent pen provided better diagnostic accuracy is indicated by the area under the ROC curve, than Midwest Caries I.D. (Figs. 1 and 2). These results suggested that the DIAGNOdent pen could provide a more accurate diagnosis for the absence of caries on the occlusal surface of the permanent molars than could the Midwest Caries I.D. device. In previous studies, the specificity of the DIAGNOdent pen for permanent teeth ranged from 0.5 to 1.00 in vitro [1, 2, 24, 26, 39] and from 0.43 to 1.00 in vivo [1, 10, 14], and the sensitivity of the DIAGNOdent pen for permanent teeth ranged from 0.16 to 1.00 in vitro [1, 26, 39] and from 0.22 to 0.93 in vivo [1, 10, 14]. These values were similar to those in the present study. Any differences in values might be related to the practitioners’ experience of using the devices and the study method. Moreover, the results of this study may be affected by the type of the sample, the cut-off limits used in this study, and the solution in which the teeth were stored.

Receiver operating characteristic curves and areas under the curves for DIAGNOdent pen

Receiver operating characteristic curves and areas under the curves Midwest Caries I.D
One of the most important requirements for the ideal diagnostic method for caries detection is good intra- and inter-examiner agreement about the method. The most recent investigations have shown that the DIAGNOdent pen seems to be a reliable method for occlusal caries detection. In the present study, the DIAGNOdent pen and the Midwest Caries I.D. device had high inter-examiner agreement. Small differences in value arising from numerical values can be seen on the monitor, whereas values of the Midwest Caries I.D. cannot be displayed on the monitor. In light of the present study, it can be concluded that each method has high inter-examiner agreement and that use of the DIAGNOdent pen is a more objective method for the diagnosis of occlusal caries (or for determining their absence) than is the use of the Midwest Caries I.D. device.
Conclusions
Taking the limitations of the current study into consideration, the sensitivity, specificity, and ROC values indicate that the DIAGNOdent pen yields more accurate diagnosis of teeth that are free of occlusal caries than does the Midwest Caries I.D. device, which was able to more accurately (i.e., with greater sensitivity) reveal the presence of caries than was the DIAGNOdent pen. Further in vivo studies of caries detection for the Midwest Caries I.D. device are suggested to yield results that would be more useful for clinical practice.
References
de Paula AB, Campos JA, Diniz MB, Hebling J, Rodrigues JA (2009) In situ and in vitro comparison of laser fluorescence with visual inspection in detecting occlusal caries lesions. Lasers Med Sci 26:1–5
Bader JD, Shugars DA (2004) A systematic review of the performance of a laser fluorescence device for detecting caries. J Am Dent Assoc 135:1413–1426
Valera FB, Pessan JP, Valera RC, Mondelli J, Percinoto C (2008) Comparison of visual inspection, radiographic examination, laser fluorescence and their combinations on treatment decisions for occlusal surfaces. Am J Dent 21:25–29
Tranaeus S, Shi XQ, Angmar-Mansson B (2005) Caries risk assessment: methods available to clinicians for caries detection. Community Dent Oral Epidemiol 33:265–273
Rodrigues JA, Hug I, Diniz MB, Lussi A (2008) Performance of fluorescence methods, radiographic examination and ICDAS II on occlusal surfaces in vitro. Caries Res 42:297–304
Ricketts D, Kidd E, Weerheijm K, de Soet H (1997) Hidden caries: what is it? Does it exist? Does it matter? Int Dent J 47:259–265
Weerheijm KL, Kidd EA, Groen HJ (1997) The effect of fluoridation on the occurrence of hidden caries in clinically sound occlusal surfaces. Caries Res 31:30–34
Chong MJ, Seow WK, Purdie DM, Cheng E, Wan V (2003) Visual-tactile examination compared with conventional radiography, digital radiography, and DIAGNOdent in the diagnosis of occlusal occult caries in extracted premolars. Pediatr Dent 25:341–349
Carneiro LS, Nunes CA, Silva MA, Leles CR, Mendonca EF (2009) In vivo study of pixel grey-measurement in digital subtraction radiography for monitoring caries remineralization. Dentomaxillofac Radiol 38:73–78
Reis A, Mendes FM, Angnes V, Angnes G, Grande RH, Loguercio AD (2006) Performance of methods of occlusal caries detection in permanent teeth under clinical and laboratory conditions. J Dent 34:89–96
Heinrich-Weltzien R, Weerheijm KL, Kuhnisch J, Oehme T, Stosser L (2002) Clinical evaluation of visual, radiographic, and laser fluorescence methods for detection of occlusal caries. ASDC J Dent Child 69:127–132, 123
Heinrich-Weltzien R, Kuhnisch J, Ifland S, Tranaeus S, Angmar-Mansson B, Stosser L (2005) Detection of initial caries lesions on smooth surfaces by quantitative light-induced fluorescence and visual examination: an in vivo comparison. Eur J Oral Sci 113:494–498
Ketley CE, Holt RD (1993) Visual and radiographic diagnosis of occlusal caries in first permanent molars and in second primary molars. Br Dent J 174:364–370
Costa AM, Yamaguti PM, De Paula LM, Bezerra AC (2002) In vitro study of laser diode 655-nm diagnosis of occlusal caries. ASDC J Dent Child 69:249–253, 233
Pretty IA (2006) Caries detection and diagnosis: novel technologies. J Dent 34:727–739
Kuhnisch J, Bucher K, Henschel V, Hickel R (2007) Reproducibility of DIAGNOdent 2095 and DIAGNOdent pen measurements: results from an in vitro study on occlusal sites. Eur J Oral Sci 115:206–211
Kesler G, Masychev V, Sokolovsky A, Alexandrov M, Kesler A, Koren R (2003) Photon undulatory non-linear conversion diagnostic method for caries detection: a pilot study. J Clin Laser Med Surg 21:209–217
Farah RA, Drummond BK, Swain MV, Williams S (2008) Relationship between laser fluorescence and enamel hypomineralisation. J Dent 36:915–921
Kuhnisch J, Bucher K, Hickel R (2007) The intra/inter-examiner reproducibility of the new DIAGNOdent pen on occlusal sites. J Dent 35:509–512
Huth KC, Neuhaus KW, Gygax M, Bucher K, Crispin A, Paschos E, Hickel R, Lussi A (2008) Clinical performance of a new laser fluorescence device for detection of occlusal caries lesions in permanent molars. J Dent 36:1033–1040
De Benedetto MS, Morais CC, Novaes TF, de Almeida Rodrigues J, Braga MM, Mendes FM Comparing the reliability of a new fluorescence camera with conventional laser fluorescence devices in detecting caries lesions in occlusal and smooth surfaces of primary teeth. Lasers Med Sci 26:157–162
Lussi A, Imwinkelried S, Pitts N, Longbottom C, Reich E (1999) Performance and reproducibility of a laser fluorescence system for detection of occlusal caries in vitro. Caries Res 33:261–266
Shi XQ, Tranaeus S, Angmar-Mansson B (2001) Validation of DIAGNOdent for quantification of smooth-surface caries: an in vitro study. Acta Odontol Scand 59:74–78
Rodrigues JA, Diniz MB, Josgrilberg EB, Cordeiro RC (2009) In vitro comparison of laser fluorescence performance with visual examination for detection of occlusal caries in permanent and primary molars. Lasers Med Sci 24:501–506
Lennon AM, Buchalla W, Switalski L, Stookey GK (2002) Residual caries detection using visible fluorescence. Caries Res 36:315–319
Chu CH, Lo EC, You DS Clinical diagnosis of fissure caries with conventional and laser-induced fluorescence techniques. Lasers Med Sci 25:355–362
Diniz MB, Rodrigues JA, de Paula AB, Cordeiro Rde C (2009) In vivo evaluation of laser fluorescence performance using different cut-off limits for occlusal caries detection. Lasers Med Sci 24:295–300
Astvaldsdottir A, Tranaeus S, Karlsson L, Peter Holbrook W DIAGNOdent measurements of cultures of selected oral bacteria and demineralized enamel. Acta Odontol Scand 68:148–153
Kuhnisch J, Berger S, Goddon I, Senkel H, Pitts N, Heinrich-Weltzien R (2008) Occlusal caries detection in permanent molars according to WHO basic methods, ICDAS II and laser fluorescence measurements. Community Dent Oral Epidemiol 36:475–484
Strassler HE, Sensi LG (2008) Technology-enhanced caries detection and diagnosis. Compend Contin Educ Dent 29:464–465, 468, 470 passim
Lussi A, Hellwig E (2006) Performance of a new laser fluorescence device for the detection of occlusal caries in vitro. J Dent 34:467–471
Pitts NB (2004) Are we ready to move from operative to non-operative/preventive treatment of dental caries in clinical practice? Caries Res 38:294–304
Jablonski-Momeni A, Ricketts DN, Rolfsen S, Stoll R, Heinzel-Gutenbrunner M, Stachniss V, Pieper K (2011) Performance of laser fluorescence at tooth surface and histological section. Lasers Med Sci 26:171–178
Baelum V, Machiulskiene V, Nyvad B, Richards A, Vaeth M (2003) Application of survival analysis to carious lesion transitions in intervention trials. Community Dent Oral Epidemiol 31:252–260
Nyvad B (2004) Diagnosis versus detection of caries. Caries Res 38:192–198
Ricketts DN, Kidd EA, Wilson RF (1995) A re-evaluation of electrical resistance measurements for the diagnosis of occlusal caries. Br Dent J 178:11–17
Bader JD, Shugars DA, Bonito AJ (2002) A systematic review of the performance of methods for identifying carious lesions. J Public Health Dent 62:201–213
Ekstrand KR, Ricketts DN, Kidd EA (1997) Reproducibility and accuracy of three methods for assessment of demineralization depth of the occlusal surface: an in vitro examination. Caries Res 31:224–231
Umemori S, Tonami K, Nitta H, Mataki S, Araki K (2010) The possibility of digital imaging in the diagnosis of occlusal caries. Int J Dent. doi:10.1155/2010/860515
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Aktan, A.M., Cebe, M.A., Çiftçi, M.E. et al. A novel LED-based device for occlusal caries detection. Lasers Med Sci 27, 1157–1163 (2012). https://doi.org/10.1007/s10103-011-1020-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10103-011-1020-0