
Abstract
This study aimed to evaluate a laser fluorescence device (the DIAGNOdent) and a visual classification system (ICDAS-II) for occlusal caries diagnosis. It also aimed to determine whether fluorescence measurements taken at the tooth surface correlate with the fluorescence measurements taken within the body of the lesion. The occlusal surfaces of 100 extracted permanent teeth were examined using ICDAS-II and DIAGNOdent (LF-tooth). Serial sections were made and lesion depth was assessed histologically. DIAGNOdent readings were also taken from the sections (LF-section). There were significant positive strong correlations between ICDAS-II and histology (rS = 0.71) and LF-section and histology (rS = 0.70), and only moderate correlations between LF-tooth and histology (rS = 0.51) and LF-tooth and LF-section (rS = 0.60). Diagnostic accuracy for ICDAS-II was generally better than for LF-tooth. While the DIAGNOdent device provides an objective reading for detection and monitoring of carious lesions, using the cut-off ranges previously suggested leads to inferior performance.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Commonly, the validity of a detection system is established by using a gold standard against which the sensitivity (true positive proportion) and specificity (true negative proportion) can be calculated. The most common gold standard used for dental caries is histological evaluation of hard-tissue sections [1]. Occlusal surfaces of posterior teeth pose a specific diagnostic problem for the dentist; the invaginated anatomy in pits and fissures means that the lesions begin at the entrance to the fissure or on its walls and spread laterally into the dentine. Topical fluoride makes the superficial enamel harder and more resistant to collapse, so that large undermining dentine lesions can occur with relatively minor visual changes at the surface (Fig. 1). Occlusal caries have therefore been the focus of much research into caries-detection methods.

Occlusal view of a molar tooth (left) showing the fissure pattern. The section of the tooth (right) taken at the site marked with the black line shows that small subtle changes at the entrance to the fissure can correspond to extensive lesions in dentine
It is well known that a tooth surface will fluoresce when irradiated by light of a given wavelength [2]. The laser light is absorbed by organic and inorganic substances present in the dental tissues, as well as by metabolites from oral bacteria. It is these metabolites that have been shown to result in the red fluorescence of carious dentine; those have been shown to lead to fluorescence to date are protoporphyrin IX, and coproporphyrin I and II, but it is anticipated that other as yet unidentified porphyrin derivatives may be implicated [3].
There is a small baseline fluorescence level for sound enamel and a different fluorescence level after the caries process has started [4]. The initial carious process begins with the formation of a biofilm on the surface of the tooth. Cariogenic bacteria within the biofilm produce acids from sugar substrates in the oral cavity causing demineralization of the tooth tissue beneath. As the carious process progresses and the lesion becomes deeper, more mineral is lost and eventually bacteria invade the demineralized lesion in progressively increasing numbers. It has been shown that deeper lesions have a higher fluorescence reading at the surface of the tooth, however, whether this corresponds to an increased reading and bacterial load within the lesion has yet to be shown.
A laser fluorescence device, the DIAGNOdent 2095 (KaVo, Biberach, Germany), has been produced which exploits this principle in an attempt to aid dentists in the early detection and quantitative assessment of carious lesions [5]. This device has the ability to emit red light at a 655-nm wavelength, which is transmitted to the tooth surface by an excitation optical fiber and tip. Fluorescent light emitted by oral bacteria metabolites is captured by detection optical fibers, incident light is filtered out, and the fluorescence intensity is translated to a numerical scale varying from 0 to 99; the higher the scores, the deeper the caries lesion [6]. Normally, the readings are categorized into diagnostic thresholds in order to determine sound tooth tissue (D0), caries in enamel only (D1,2) and caries that extends into dentine (D3,4).
Medical devices always come with a financial cost and poor detection of occlusal caries from a visual examination has been attributed to the fact that teeth are not cleaned satisfactorily prior to examination and they are not examined whilst wet and dry. In addition, the subtle changes seen at the surface of the tooth are not related to the histopathology of the disease. Baring these issues in mind, a new visual classification system has been devised for caries detection, the International Caries Detection and Assessment System (ICDAS-II), which was developed to provide clinicians, epidemiologists, and researchers with an evidence-based system that would allow standardized data collection in different settings and better comparison between studies [7]. Sensitivity and specificity of ICDAS-II has already found to be promising when used for occlusal caries lesions [8].
The aims of this study were three-fold: firstly, to determine the diagnostic accuracy and reproducibility of the laser fluorescence device, the DIAGNOdent, and the ICDAS-II visual classification system for occlusal caries detection and to determine the relationship between the two methods of detection; secondly, to determine the relationship between laser fluorescence readings taken at the entrance to the fissure and the histological depth of the lesion; and finally to determine whether there was any relationship between the fluorescence readings taken at the surface of the tooth and those taken from a histological section within the “body” of the lesion, and hence reflecting the bacterial load.
Material and methods
Sample selection and visual examination
One hundred unrestored molar (n = 85) and premolar (n = 15) teeth were selected from a group of extracted teeth collected at Dundee and Marburg Dental Schools according to regulations in place at the time of tooth collection in both countries. These were cleaned thoroughly and stored in water. The teeth used in this study were the same as those used in previously published studies [8, 9].
One to four discrete and easily reproducible sites within the pit-and-fissure system of each tooth were chosen for investigation, representing the full range of appearances from sound to gross cavitation (n = 181 investigations sites). The investigation sites were marked on black-and-white images of the tooth surface for ease of re-location, but not of sufficient quality to influence the ICDAS-II visual scoring. Each investigation site was independently examined by four investigators blind to the others results using the visual International Caries Detection and Assessment System (ICDAS-II) [10]. Following this, the results were discussed and a consensus score for each site was achieved as detailed in Jablonski-Momeni et al. [9]. The chosen sites were recorded as:
-
0 = sound (n = 39);
-
1 = first visible sign of non-cavitated lesion seen only when the tooth is dried (n = 51);
-
2 = clinically visible non-cavitated lesion seen when wet (n = 33);
-
3 = microcavitation in enamel (n = 20);
-
4 = non-cavitated lesion extending into dentine seen as an undermining shadow (n = 15);
-
5 = small cavitated lesion with visible dentine: less than 50% of surface (n = 21);
-
6 = large cavitated lesion with visible dentine: more than 50% of surface (n = 2).
Examination of tooth surface with laser fluorescence (LF-tooth)
The DIAGNOdent 2095 laser fluorescence device was used by one examiner (A. J.-M.) who was trained in the use of the device. The device was first calibrated using a ceramic standard, in accordance with the manufacturer’s instructions. Prior to the laser fluorescence readings, the device was zeroed using an obviously sound enamel spot on the tooth (zero value). This overcomes inherent differences in tooth color. Using tip A, the laser fluorescence device was moved along the surface of the investigation site and the peak value was recorded. Intra-examiner reproducibility was assessed by repeated measurements for all investigation sites within 1 day.
Histological preparation
For histological examination, the roots were resected from the teeth just apical to the cement enamel junction and the crowns were serially sectioned using a technique that allowed accurate allocation of section to the specific investigations sites as previously described [8, 9, 11]. In total, 11–15 sections were produced per crown (section width = 200 µm ± 30 µm) and 1–4 sections were available to view for each investigation site.
Histological examination
For each investigation site, the selected sections were examined by four examiners using a binocular microscope (Wild Heerbrugg AG, Gais Switzerland) using 16× magnification and reflected light. The Downer histological classification system [1] was used to record caries severity at each investigation site:
-
0 = No enamel demineralization or a narrow surface zone of opacity (edge phenomenon)
-
1 = Enamel demineralization limited to the outer 50% of the enamel layer
-
2 = Demineralization involving the inner 50% of the enamel, up to the enamel–dentine junction
-
3 = Demineralization involving the outer 50% of the dentine
-
4 = Demineralization involving the inner 50% of the dentine
Emphasis was placed on differentiating pulp-dentine-complex reactions with dental tissues affected by caries and on differentiating staining from caries. A histological score was given to each section corresponding to each investigation site and the worse/deepest score was taken as the definitive score for further analysis. All the sites were investigated by each examiner blind to each other. The results were compared and a consensus histological score was derived following discussion as described previously [9].
Assessments with the laser fluorescence device at teeth sections (LF-section)
The DIAGNOdent 2095 laser fluorescence device was then used on the section surfaces (Fig. 2) by a second examiner who was also trained with the use of the device (S.R.) following DIAGNOdent calibration and zeroing for each tooth. Prior to the laser fluorescence readings of each section, the fluorescence of the specimen holder (plate made of acrylic glass) and of the mineral glass which coated the specimen was measured. Both materials showed no fluorescence, so it could be assumed that neither the specimen holder nor the top coat of the section would influence the readings.

a View of a tooth section with caries into enamel. b Tip of the DIAGNOdent is "scanning" the section
For the section readings, the DIAGNOdent tip (tip A) was moved along the surface of each section that corresponded to each investigation site and the peak value for each section was recorded. The highest fluorescence reading from the investigation site sections was used in subsequent analyses. Intra-examiner reproducibility was assessed by repeated measurements for 30% of the sections after 1 week.
Data management and statistical evaluation
Statistical analysis was performed using SPSS (Version 15). For the laser fluorescence measurements, intra-examiner reproducibility was calculated using the Intraclass Correlation Coefficient (ICC). The distribution of the laser fluorescence measurements taken on the tooth surface and tooth section were plotted according to ICDAS-II codes and histological measurements using box plots. The relationships between ICDAS-II, the histological scores, and laser fluorescence readings were assessed using Spearman's rank correlation coefficients (rS).
The limits of agreement [12] were used to identify any systematic differences between the laser fluorescence readings taken on the tooth surface and on the corresponding sections. For this, the difference between paired readings (LF-tooth vs. LF-section) was plotted against their means. The limits of agreement were then taken as the mean difference ± 1.96 SD.
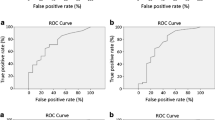
The performance of ICDAS-II and LF-tooth was shown by calculating the specificity and sensitivity against the gold standard at the D1 and D3 diagnostic threshold. At the D1 diagnostic threshold all histological scores 1–4 were classed as caries and at the D3 diagnostic threshold histological scores 3 and 4 only were classed as caries. For the DIAGNOdent, each reading was used as a cut-off point to determine sound and caries and the sensitivity and specificity calculated for each reading. Using these sensitivity and specificity values, receiver operating characteristic (ROC) curves were prepared for the D1 and D3 thresholds. For the ICDAS-II, each code was used as a cut-off and ROC curves were constructed in a similar manner for the D1 and D3 thresholds.
In order to be consistent and compare the results of this study with previously published data, the LF cut-off limits suggested by Lussi and Hellwig [13] were used to calculate sensitivity and specificity, in addition to the optimum values determined by the ROC analysis above:
LF cut-off points used by Lussi and Hellwig [13]:
-
I
(caries-free, D0) = 0–7,
-
II
(caries extending up to halfway through the enamel, D1) = 8–14,
-
III
(caries in the inner half of enamel, D2) = 15–24,
-
IV
(caries in dentine D3,4) > 24).
Results
Initially, 181 investigation sites at 100 teeth were examined visually and with the DIAGNOdent, but owing to section damage on some teeth and to some not being scored by all examiners, only 166 investigation sites and 339 corresponding sections were available for histological and LF examinations.
The intra-examiner reproducibility for the laser fluorescent measurements was excellent: intra-class-correlation coefficient (ICC) for LF-tooth was 0.957 (95% confidence interval: 0.942–0.967) and for LF-section 0.988 (95% confidence interval: 0.979–0.994). Intra-examiner reproducibility for the ICDAS-II codes was not calculated in this study as these were decided by consensus. Data on kappa values for each examiner’s reproducibility has been presented previously (weighted kappa = 0.74–0.83) [8].
The box plots showing the distribution of DIAGNOdent readings on the tooth surface and section are shown in Fig. 3 according to ICDAS-II codes and histological scores. The horizontal line gives the median reading for all LF readings in each group, the top of the shaded box gives the median of the upper readings and the bottom of the box the median of the lower readings. The whiskers give the minimum and maximum readings, which are no outliners. Outliners are labeled as dots, and extreme outliners as stars. The box-and-whisker plots divide the readings into quartiles.

Box plots for a laser fluorescence readings on the tooth surfaces (LF-tooth) according to ICDAS-II codes, b laser fluorescence readings on sections (LF-section) according to ICDAS-II codes, c LF-tooth according to histology classification and d LF-section according to histology classification. Box plots show median, 1st, and 3rd quartiles, minimum and maximum values (whiskers) and outliers
It is generally accepted that a correlation co-efficient from 0 to 0.3 represents a weak relationship, 0.3–0.7 a moderate relationship, and those above 0.7, a strong relationship [14]. Strong relationships were found between ICDAS-II and histology (rS = 0.71) and between LF-section and histology (rS = 0.70). Weaker relationships were found between LF-tooth and ICDAS-II (rS = 0.61), LF-tooth and LF section (rS = 0.60) LF-tooth and histology (rS = 0.51) and LF-section and ICDAS-II (rS = 0.44). All correlations were significant at the 0.01 level (two-tailed).
Figure 4 shows the limits of agreement between paired LF-tooth and LF-section DIAGNOdent readings. The mean difference in readings was −3.67, the upper limit was +43.43, and the lower limit was −50.77. This demonstrates that there is large variation between LF readings taken on the tooth surface and those taken on the section. The largest variations occur for readings over 20, which, according to Lussi and Hellwig [13], correspond to dentine lesions.

The limits of agreement [12] for paired LF-tooth and LF-section readings. This shows the difference between two readings plotted against the mean of the two readings. The mean of the differences is −3.67, the upper and lower limits between which 95% of the differences between readings would fall are 43.43 and −50.77, respectively
Specificity and sensitivity of ICDAS-II and DIAGNOdent readings at tooth surface are shown in Table 1. The use of ICDAS-II on tooth surfaces showed higher values of sensitivity and specificity than the laser fluorescence measurements both at D1 and D3 diagnostic threshold, however, at the D1 diagnostic threshold the specificity was unacceptably low for both detection methods.
Discussion
Early caries detection is pivotal in the management of dental caries as early lesions can be treated preventively with improved oral hygiene in the presence of fluoride and a reduced frequency of sugar intake. Lesions treated in this way can arrest or even remineralize and a way of monitoring the success of this preventive approach is integral in the quest for new detection devices. Occlusal surfaces are the most caries-affected sites in the teeth of children and young adults because of the special morphology of pits and fissures and also because of the difficulty of plaque removal.
Several methods of caries detection and monitoring have been described including visual inspection, radiographic methods and electrical conductance methods in addition to laser fluorescence or quantitative light-induced fluorescence [15]. Unfortunately, where occlusal caries is concerned, many lesions are undetected in a conventional visual examination and a lesion which is reliably detected from a bitewing radiograph will be advanced, having extended into the middle third of dentine [16]. Thus the quest for detection and monitoring devices continues.
Both in vitro and in vivo studies show that laser fluorescence devices have a good intra- and inter examiner reproducibility [4, 17]. This is supported in this study as an excellent intra-class correlation coefficient for intra-examiner repeatability was found (ICC 0.957 for LF-tooth).
In previous studies, the performance of the laser fluorescence device DIAGNOdent has been related to cut-off limits used in laboratory or clinical studies to determine sound sites from those with enamel caries and those with caries extending into dentine. Several cut-off limits have been suggested by different manufacturers and by in vivo and in vitro studies [18]. If the cut-off points described by Lussi and Hellwig [13] are compared to the results from this study, it can be seen that over half of histologically sound sites have readings above the upper threshold of 7 (Fig. 3). This is echoed in the low specificity of 0.48 obtained at the D1 diagnostic threshold (Table 1). A systematic review of the literature has also shown that the majority of studies using the DIAGNOdent device in vitro obtain high levels of false-positive results or low specificity [19]. This has been attributed to the high readings that are also obtained from plaque, calculus, some dental materials, stains, or hypomineralized non-carious teeth [17].
The thresholds set by Lussi and Hellwing [13] for enamel caries (8–24) would broadly be in agreement with the results from this study as approximately 75% of the readings fall into this range. However, the box-and-whisker plots indicate that the LF readings do not differentiate shallow and deep enamel lesions (Fig. 3). Of those lesions extending into the outer half of the dentine, 50% give an LF reading below that suggested for dentine lesions of 24.
There is a great deal of overlap of the box-and-whisper plots for LF readings taken on the tooth surface and the sections corresponding to ICDAS codes 2 to 6 (Fig. 3). Thus LF thresholds could not be set to differentiate between increasing visual severities of the carious lesions as documented by the ICDAS-II codes.
It would therefore seem that the LF-tooth readings are unable to differentiate histologically sound, enamel caries and dentine caries in a precise manner using set cut-off limits and while there is a positive correlation with histological depth, this relationship is only moderate (rS = 0.51). The relationship between ICDAS-II scores and histological depth was however much better (rS = 0.71).
It might be argued that it is not only the histological depth of a lesion that is important in determining lesion severity; it might also be the degree of demineralization and the level of bacterial infection within the dentine lesion. Thus this study aimed to determine the relationship of DIAGNOdent readings taken on the surface of the tooth to that within the lesion determined on the section, as the fluorescence measurement is inextricably linked to bacterial products; only a moderate relationship was found between the two LF readings (rS = 0.60). It could be argued that the storage method [20], embedding, and sectioning technique led to wash-out of some of the bacterial fluorophores affecting this relationship. This would however, have lead to a systematic error where LF tooth readings would always be higher than LF section readings. The limits of agreement between the two illustrate that this is not the case; there is an equal spread of differences between the two readings above and below the mean of the differences (Fig. 4). That is, sometimes the readings on the sections were lower, but sometimes they were higher than on the tooth surface.
The diagnostic performance of the ICDAS-II visual detection method gave a better overall diagnostic accuracy, as indicated by the area under the ROC curve, than LF-tooth method (Table 1). As previously noted at the D1 diagnostic threshold, while sensitivity is high, specificity is low, indicating a high risk of false-positive results. This may be due to stained fissures impacting upon both techniques. Care must therefore be exercised when interpreting the results of both examinations in clinical practice and should not be used to make operative decisions upon. Where dentine caries is concerned (D3 diagnostic threshold, Table 1), specificity is higher for both systems, but the sensitivity is low for the DIAGNOdent using the recommended cut-off reading of 24. If the optimum reading determined from the ROC curve constructed in this study of 17 was used the sensitivity is higher (0.72) but specificity lower (0.76).
Many studies have shown that the DIAGNOdent device is a valuable adjunct to clinical examination and suitable for longitudinal monitoring of the caries process due to the objective readings [4]. Nevertheless, there are potential “confounders” that may lead to false-positive diagnostic decisions when implemented strictly to previous recommendations. Different diagnostic methods have different characteristics, indications, and limitations for use. In order to detect caries on occlusal surfaces thoroughly, a combination of methods would be the best practice moderated by clinical knowledge and experience [21, 22]. Rodrigues et al. [23] demonstrated that ICDAS-II combined with bitewing radiography was the best diagnostic combination for detecting occlusal caries, followed by the combination of ICDAS-II and laser fluorescence measurements which would allow objective monitoring; the results of this study would support this.
References
Downer MC (1975) Concurrent validity of an epidemiological diagnostic system for caries with the histological appearance of extracted teeth as validating criterion. Caries Res 9:231–246
Stübel H (1911) Die Fluoreszenz tierischer Gewebe im ultra-violetten Licht. Pflugers Arch 142:1–14
Buchalla W, Attin T, Niedmann Y, Niedmann PD, Lennon ÁM (2008) Porphyrins are the cause of red fluorescence of carious dentine: verified by gradient reversed-phase HPLC (Abstract). Caries Res 42:223
Lussi A, Hibst R, Paulus R (2004) DIAGNOdent: An optical method for caries detection. J Dent Res 83(Spec Iss C):C80–C83
Lussi A, Imwinkelried S, Pitts NB, Longbottom C, Reich E (1999) Performance and reproducibility of a laser fluorescence system for detection of occlusal caries in vitro. Caries Res 33:261–266
Hibst R, Paulus R, Lussi A (2001) A detection of occlusal caries by laser fluorescence: basic and clinical investigations. Med Laser Appl 16:205–213
Pitts N (2004) “ICDAS”- an international system for caries detection and assessment being developed to facilitate caries epidemiology, research and appropriate clinical management. Community Dent Health 21:193–198
Jablonski-Momeni A, Stachniss V, Ricketts DN, Heinzel-Gutenbrunner M, Pieper K (2008) Reproducibility and accuracy of the ICDAS-II for detection of occlusal caries in vitro. Caries Res 42:79–87
Jablonski-Momeni A, Ricketts DN, Stachniss V, Maschka R, Heinzel-Gutenbrunner M, Pieper K (2009) Occlusal caries: evaluation of direct microscopy versus digital imaging used for two histological classification systems. J Dent 37:204–211
International Caries Detection and Assessment System (ICDAS) Coordinating Committee: The rationale and evidence for the International Caries Detection and Assessment System (ICDAS II) & Criteria Manual, Baltimore 2005 (www.icdas.org)
Stachniss V (2005) Zur Hartschnitt-Technik nicht entkalkter Zähne und digitale makrofotografische Reproduktion histologischer Präparate. Research Report, Philipps-University Marburg, Germany
Bland JM, Altman DG (1999) Measuring agreement in method comparison studies. Stat Methods Med Res 8:135–160
Lussi A, Hellwig E (2006) Performance of a new laser fluorescence device for the detection of occlusal caries in vitro. J Dent 34:467–471
Ricketts DNJ, Watson TF, Liepins PJ, Kidd EAM (1998) A comparison of two histological validating techniques for occlusal caries. J Dent 26:89–96
Bader JD, Shugars DA, Bonito AJ (2001) Systematic reviews of selected dental caries diagnostic and management methods. J Dent Educ 65:960–968
Ricketts DN, Kidd EA, Smith BG, Wilson RF (1995) Clinical and radiographic diagnosis of occlusal caries: a study in vitro. J Oral Rehabil 22:15–20
Rodrigues JA, Diniz MB, Josgrilberg EB, Cordeiro RC (2009) In vitro comparison of laser fluorescence performance with visual examination for detection of occlusal caries in permanent and primary molars. Lasers Med Sci 24:501–506
Diniz MB, Rodrigues JA, de Paula AB, Cordeiro RC (2009) In vivo evaluation of laser fluorescence performance using different cut-off limits for occlusal caries detection. Lasers Med Sci 24:295–300
Bader JD, Shugars DA (2004) A systematic review of the performance of a laser fluorescence device for detecting caries. J Am Dent Assoc 135:1413–1426
Francescut P, Zimmerli B, Lussi A (2006) Influence of different storage methods on laser fluorescence values: a two-year study. Caries Res 40:181–185
Ricketts DNJ, Ekstrand KR, Kidd EA, Larsen T (2002) Relating visual and radiographic ranked scoring systems for occlusal caries detection to histological and microbiological evidence. Operative Dent 27:231–237
Souza-Zaroni WC, Ciccone JC, Souza-Gabriel AE, Ramos RP, Corona SAM, Palma-Dibb RG (2006) Validity and reproducibility of different combinations of methods for occlusal caries detection: an in vitro comparison. Caries Res 40:194–201
Rodrigues JA, Hug I, Diniz MB, Lussi A (2008) Performance of fluorescence methods, radiographic examination and ICDAS II on occlusal surfaces in vitro. Caries Res 42:297–304
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jablonski-Momeni, A., Ricketts, D.N.J., Rolfsen, S. et al. Performance of laser fluorescence at tooth surface and histological section. Lasers Med Sci 26, 171–178 (2011). https://doi.org/10.1007/s10103-010-0768-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10103-010-0768-y