
Abstract
Using scanning electron microscopy (SEM) we evaluated the morphology of cavity surfaces in deciduous teeth prepared in vitro with the Er:YAG laser with different power parameters. Eight extracted cavity-free deciduous teeth with an intact crown were prepared using a traditional handpiece or an Er:YAG laser with different parameters (10 Hz/200 mJ, 10 Hz/300 mJ and 10 Hz/400 mJ). Samples were then processed and cavity surface morphology was evaluated by SEM to detect open dentinal tubules, or melting or cracking of the dentin. SEM showed that laser cavity preparation in deciduous teeth using different parameters left no smear layer and the dentinal tubules were clear. Dentin melting was not seen after cavity preparation at 200 mJ or 300 mJ, while visible dentin melting and cracks were detected at 400 mJ. The use of the laser at 10 Hz/200 mJ and 10 Hz/300 mJ for cavity preparation in deciduous teeth is safe and effective, but higher powers may damage the dentin.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Pediatric dentists generally use a traditional handpiece for caries removal before filling in the treatment of cavities in deciduous teeth. Although the handpiece can quickly remove caries, it may also cause excessive abrasion of the tooth structure, and the significant amount of pain during the drilling cannot be tolerated by many children. In addition, the vibration and noise of the drilling device are often feared by children. With its many advantages such as painlessness, minimal invasiveness and comfort, laser has been widely used in dental practice since its introduction. The Er:YAG laser is a new dental treatment for use in the clinic approved by the US FDA in 1997 for dental hard tissues, which can effectively cut enamel and dentin without damaging the pulp [1, 2]. In China and abroad, the laser has been used for cavity preparation in the permanent teeth. Many studies have been conducted on the parameters, cavity morphology and filling forms for laser preparation of permanent teeth cavities. The surface morphology of cavities has been evaluated by scanning electron microscopy (SEM) after laser preparation in the permanent teeth, and the laser has been shown to be able to remove smear layer while keeping the dentinal tubules clear [3]. There is also no smear layer after laser cavity preparation in deciduous teeth. However, since the structures of deciduous and permanent teeth are different, the laser parameters should differ accordingly. Currently, since few studies have been done on the surface morphology of cavities prepared using lasers of different powers, the parameters for laser cavity preparation in deciduous teeth have not yet been determined. The objective of this study was to evaluate the status of cavities in deciduous teeth by SEM after preparation using lasers with different parameters, in order to provide evidence for the use of lasers in the treatment of deciduous teeth.
Materials and methods
This study was reviewed and approved by the Ethics Committee of Peking University Medical College (no. IRB0001052-08073).
Eight cavity-free second primary molars with an intact crown were collected, placed in 0.9% saline and stored in 4°C. The Er:YAG laser therapy instrument was a Smart 2940D (Deka, Florence, Italy) which can generate pulsed radiation at a wavelength of 2,940 nm.
As the control group two primary teeth were prepared using a traditional handpiece Dia-Burs BR-S46 (Mani, Japan).
The laser-treated teeth were divided into three groups according to different laser parameters, two teeth per group. The Er:YAG laser at 10 Hz with energies of 200, 300 and 400 mJ (groups 1, 2 and 3, respectively) was used to prepare class I cavities 2 mm deep in the dentin of the occlusal surface of the deciduous teeth, followed by spray rinsing for 10 s and air gun drying for 10 s. The samples were prefixed in 2.5% glutaraldehyde fixation solution and postfixed in 1% osmium tetroxide, followed by dehydration in a graded series of 30%, 50%, 70%, 80%, 90% and 100% ethanol, air drying and gold-plating. They were then viewed under JSM-5600 secondary electron imaging SEM (Jeol Technics, Tokyo, Japan) at magnifications in the range 500–5,000. The morphological characteristics of the dentin surface, surface roughness, the presence of a smear layer, the appearance of the dentinal tubules, and the presence of melting and cracks in the dentin were evaluated and compared.
Results
The cavity surfaces in the control group were covered by a smear layer, with scattered irregular debris, and dentinal tubules could be seen occasionally (Fig. 1).

Control group. Representative scanning electron micrograph of the smear layer produced on the dentin surface by a diamond burr in a high-speed drill (×2,000)
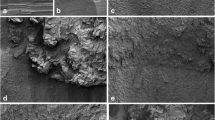
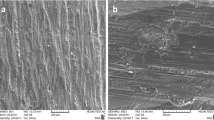
No smear layer was seen on the dentin surface in the three laser groups. The surfaces were scale-like and uneven with open dentinal tubules. The density of the peritubular dentin was seen to be higher than that of the intertubular dentin, and there was no plugging of the tubules. There were no obvious cracks or melting of the dentin in groups 1 and 2. In group 3, (i.e. the 10 Hz/400 mJ laser group) the cavities showed a significantly more uneven surface, visible cracks and partial dentin melting locally. Longitudinal profiles of the dentinal tubules could be seen in the lateral walls, and showed irregular dentin particles (Figs. 2, 3, 4, 5, 6).

Experimental group 1. Representative scanning electron micrograph of dentin irradiated with the Er:YAG laser (10 Hz/200 mJ) showing the absence of a smear layer and open dentinal tubules (×1,000)

Experimental group 2. Representative scanning electron micrograph of dentin irradiated with the Er:YAG laser (10 Hz/300 mJ) showing the absence of a smear layer and open dentinal tubules (×1,000)

Experimental group 2. Representative scanning electron micrograph of dentin irradiated with the Er:YAG laser (10 Hz/300 mJ) showing the absence of a smear layer and open dentinal tubules (×2,000)

Experimental group 3. Representative scanning electron micrograph of dentin irradiated with the Er:YAG laser (10 Hz/400 mJ) showing the absence of a smear layer, open dentinal tubules, visible cracks and an area of partial dentin melting (×1,000)

Experimental group 3. Representative scanning electron micrograph of dentin irradiated with the Er:YAG laser (10 Hz/400 mJ) showing a crack (arrow) (×5,000)
Discussion
The results of this study show that the surface morphologies as shown by SEM of cavities prepared using a traditional handpiece and a laser are completely different. Surfaces prepared using a handpiece are covered by a smear layer but cavities prepared using a laser are not, consistent with the results of other studies in permanent teeth [4–8] and deciduous teeth [9, 10].
Driven by a mechanical motor, the traditional handpiece drill rotates at high speed and cuts the tooth structure on contact. The accompanying heat from friction and mechanical vibration may stimulate the nerve fibers in the dental pulp and cause pain and discomfort. In particular, local heating and shear forces during the cutting process may cause elastic and plastic deformation of the tooth structure, leading to the breaking of inorganic material and the degeneration of organic material to form a smear layer, comprising denatured collagen, coagulated proteins, saliva, blood, dentinal tubule fluid, various microorganisms, broken tooth structural material, dental pulp tissue debris, and pollutants. This smear layer is usually in tight contact with the cavity wall or root canal wall, and cannot be easily removed by rinsing and wiping [11]. The presence of a smear layer can cause microleakage and affect the bonding of adhesive resin. Currently, dentists use the method of acid erosion to remove the smear layer [12–15].
Laser cavity preparation and handpiece cavity preparation are totally different. The Er:YAG laser has a wavelength of 2,940 μm, close to the absorption peak of water. Upon laser irradiation of the target tissue, the energy of the laser is absorbed by water and hydroxyapatite inside the tissue and the water is quickly evaporated generating a "microexplosion", and resulting in breaking of the target tissue. The broken pieces fly away from the tissue surface at a very high speed. Since the thermal energy is converted to kinetic energy, little heat remains in the residual tissue, so mechanical and thermal damage to the surrounding tissue is minimal [16]. Therefore, the cavity surface remains clean, with no smear layer or melting effect, and clear dentinal tubules. In addition, the laser does not contact the tooth structure during cavity preparation; rather there is a distance of more than 10 mm between the laser generator and the tooth structure. Also according to literature reports, the vibration amplitude and frequency of lasers are much lower than those of traditional high-speed handpieces [17]. Therefore, laser removal of the tooth structure is not only effective, but also results in far less pain and discomfort than removal with the traditional handpiece.
The floor of the laser-prepared cavities in deciduous teeth was not flat, but rather had a wave-like or scale-like appearance, consistent with previous reports [9, 10, 18]. This is because of the different water contents of different dentin structures. So lasers of the same power will remove more intertubular dentin tissues rich in water than dry peritubular dentin. Therefore, a cuff-like high-density circle can be seen around the dentinal tubules in images. Our findings regarding laser power match those of Freitas et al. [6], Esteves-Oliveira et al. [19] and Delme and De Moor [20] regarding permanent teeth. The morphology of dentin surfaces in deciduous teeth after laser irradiation are similar to those in permanent teeth, but have a loose surface, a highly stratified appearance and clear openings of the dentin tubules that are regularly aligned. This appearance may be related to the dentin structure of deciduous teeth. Deciduous teeth are less calcified than permanent teeth, and contain more water and organic substances. The dentin tubules are loosely aligned, and the intertubular dentin contains more water than the intratubular dentin. Lasers of the same power will remove more tissue in deciduous teeth than in permanent teeth. Thus, the parameters used should be lower than those used in permanent teeth. In brief, The higher the power, the more distinct the layer at the cavity floor. In group 3 irradiated at a power of 4 W, more obvious waves were present at the cavity floor and small cracks were seen. As the laser's cutting ability is proportional to its power [21], more small cracks and a deeper melting layer at the cavity surface are formed with higher power lasers. This study found that the cavity surfaces irradiated at 10 Hz with energies of 200 mJ and 300 mJ were similar, but those irradiated at 10 Hz with an energy of 400 mJ show cracks and melting of the dentin, indicating that the use of a power of 4 W in the dentin of primary teeth is too high and may damage the dentin.
In summary, cavity preparation in deciduous teeth with laser power parameters of 10 Hz and 200 or 300 mJ is safe and effective for the removal of tooth structure, while 10 Hz and 400 mJ for cavity preparation causes dentin cracks. Therefore, deciduous teeth should be prepared using a laser power of less than 4 W.
References
Cozean C, Arcoria CJ, Pelagalli J, Powell GL (1997) Dentistry for the 21st century? Erbium:YAG laser for teeth. J Am Dent Assoc 128:1080–1087
Pelagalli J, Gimbell CB, Hansen RT et al (1997) Investigational study of the use of Er:YAG laser versus dental drill for caries removal and cavity preparation – phase I. J Clin Laser Med Surg 15:109–115
Hossain M, Nakamura Y, Yamada Y, Kimura Y et al (1999) Ablation depths and morphological changes in human enamel and dentin after Er:YAG laser irradiation with or without water mist. J Clin Laser Med Surg 17:105–109
Camerlingo C, Lepore M, Gaeta GM, Riccio R, Riccio C, De Rosa A et al (2004) Er:YAG laser treatments on dentine surface: micro-Raman spectroscopy and SEM analysis. J Dent 32:399–405
Khabbaz MG, Makropoulou MI, Serafetinides AA et al (2004) SEM analysis of dentin treated with the Er:YAG laser. J Endod 30(8):585–588
Freitas PM, Navarro RS, Barros JA et al (2007) The use of Er:YAG laser for cavity preparation: an SEM evaluation. Microsc Res Tech 70:803–808
Israel M, Cobb CM, Rossmann JA et al (1997) The effects of CO2, Nd:YAG and Er:YAG lasers with and without surface coolant on tooth root surfaces. An in vitro study. J Clin Periodontol 24:595–602
Sassi JF, Chimello DT, Borsatto MC et al (2004) Comparative study of the dentin/adhesive systems interface after treatment with Er:YAG laser and acid etching using scanning electron microscope. Lasers Surg Med 34:385–390
Kohara EK, Hossain M, Kimura Y, Matsumoto K, Inoue M, Sasa R (2002) Morphological and microleakage studies of the cavities prepared by Er:YAG laser irradiation in primary teeth. J Clin Laser Med Surg 20:141–147
Kornblit R, Bossù M, Mari D et al (2009) Enamel and dentine of deciduous teeth Er:YAG laser prepared. A SEM study. Eur J Paediatr Dent 10(2):75–82
Pashley DH, Tao L, Boyd L et al (1988) Scanning electron microscopy of the substructure of smear layers in human dentin. Arch Oral Biol 33(4):265–270
Yu XY, Davis EL, Joynt RB et al (1992) Origination and progression of microleakage in a restoration with a smear layer-mediated dentinal bonding agent. Quintessence Int 23(8):551–555
Vassiliadis L, Liolios E, Kouvas V et al (1996) Effect of smear layer on coronal microleakage. Oral Med Oral Pathol Oral Radiol Endod 82(3):315–320
Hayakawa T, Nemoto K, Horie K (1995) Adhesion of composite to polished dentin retaining its smear layer. Dent Mater 11(3):218–222
Gettleman BH, Messe HH, Deeb M (1991) Adhesion of sealer cements to dentin with and without the smear layer. J Endod 17(1):15–20
Tokonabe H (1999) Morphological changes of human teeth with Er:YAG laser Irradiation. J Clin Laser Med Surg 17(1):7–12
Takamori K (2003) Basic study on vibrations during tooth preparations caused by high-speed drilling and Er:YAG laser irradiation. Lasers Surg Med 32:25–31
Armengol V, Jean A, Rohanizadeh R et al (1999) Erbium laser ablation of dental hard tissue: effect of water cooling. J Endod 25(8):543–546
Esteves-Oliveira M, de Guglielmi CA, Ramalho KM et al (2010) Comparison of dentin root canal permeability and morphology after irradiation with Nd:YAG, Er:YAG, and diode lasers. Lasers Med Sci 25:755–760
Delme KI, De Moor RJ (2007) Scanning electron microscopic evaluation of enamel and dentin surfaces after Er:YAG laser preparation and laser conditioning. Photomed Laser Surg 25(5):393–401
Corona SA, Souza-Gabriel AE, Chinelatti MA et al (2008) Influence of energy and pulse repetition rate of Er:YAG laser on enamel ablation ability and morphological analysis of the laser-irradiated surface. J Biomed Mater Res A 84(3):569–575
Acknowledgment
The authors thank the Beijing BaoLiKangYe Science Technology Co., Ltd. Beijing for providing the DEKA Smart 2940D laser treatment apparatus for this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zhang, S., Chen, T. & Ge, Lh. Scanning electron microscopy study of cavity preparation in deciduous teeth using the Er:YAG laser with different powers. Lasers Med Sci 27, 141–144 (2012). https://doi.org/10.1007/s10103-010-0854-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10103-010-0854-1