
Abstract
The results of studies investigating the associations between GSTM1 and GSTT1 polymorphisms and anti-tuberculosis drug-induced hepatotoxicity (ADIH) risk exhibit much controversy. Therefore, a meta-analysis was performed in order to examine the associations between GST variants and ADIH risk. A total of 451 relevant studies were identified through the digital medical databases Medline, Embase, and CBM published up to October 2012. Thirteen individual case–control studies were eventually recruited for GSTM1 null polymorphism (including 951 ADIH cases, 1,922 controls) and 12 studies for GSTT1 null polymorphism (847 cases, 1,811 controls). Pooled odds ratios (ORs) and 95 % confidence intervals (CIs) were appropriately calculated from fixed-effects or random-effects models. Subgroup analyses were stratified by ethnicity and different treatment combinations. The overall ORs of relevant studies that exhibited elevated ADIH risk was significantly associated with GSTM1 null genotypes (OR = 1.36, 95 % CI 1.04–1.79), but for the GSTT1 polymorphism, no difference was found (OR = 0.98, 95 % CI 0.82–1.18). In the subgroup analyses, the pooled results showed that GSTM1 null allele carriers had a significant association with ADIH risk in East Asians and the patients who used isoniazid (INH) + rifampicin (RMP) + pyrazinamide (PZA) + ethambutol (EMB), or + streptomycin (SM) (HRZES), but the opposite result was observed for patients using HR. Moreover, the GSTT1 null genotype evaluated the susceptibility to ADIH for tuberculosis using HRZ. This meta-analysis provides evidence that there may be an increased risk of ADIH in individuals with null genotypes of GSTM1 in the total population, especially East Asians and patients receiving HRZE or HRZES. However, polymorphisms of the GSTT1 null genotype seem to have no association with susceptibility to ADIH, except for patients receiving HRZ.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Tuberculosis (TB) is a serious fatal infectious disease, having become one of the major causes of illness and death worldwide, especially in Asia and Africa. Annually, more than 9 million new cases and 1.7 million deaths caused by TB were reported in 2009 [1]. Strategies have been adopted to reduce the relevant disease burden by improving early case detection and treatment compliance. Isoniazid (INH), rifampicin (RMP), ethambutol (EMB), and pyrazinamide (PZA), as the first-line anti-tubercular drugs (ATD) and components of the standard therapeutic regimen [2, 3], are used conventionally in combination for treating the disease. Despite the availability of effective chemotherapeutic agents to treat TB, the most commonly encountered and also severely presenting side effects of these drugs are potentially hepatotoxic, and toxicity increases when used in combination, impeding scheduled treatment and adding to disease morbidity because of treatment interruptions and negative impact on treatment compliance [4, 5]. Acharya et al. had demonstrated that ATD were the most common reason for drug-induced liver disease in India [6]. Although many researchers had proposed the influence factors of ATD hepatotoxicity involved in a number of environmental factors and the acetylator phenotype of the individual, its exact pathogenic mechanism still remains largely obscure [7, 8]. It is reported that there is a close relation between anti-tuberculosis drug-induced hepatotoxicity (ADIH) and drug-metabolizing enzymes [9].
Generally speaking, the dynamic processes of drugs including toxic metabolite generation and its detoxification in the liver made for hepatotoxicity. It is suggested that ATD reactions are attributed to reactive metabolites, rather than direct toxicities of the parent drugs. Drug-metabolizing enzymes make pivotal impacts in the course of the synthesis and detoxification of reactive metabolites [10]. Glutathione S-transferases (GST) are recognized as common detoxifying enzymes, playing an extremely important protection role as they catalyze the conjugation of various reactive drug toxicity metabolites causing cellular damage with glutathione, thereby, decreasing drug hepatotoxicity [11–14]. They exist in several isoforms, with varying tissue-specific expression [15]. As two members of isoenzymes of the GST enzyme family encoding phase II metabolic enzymes in the human body, GSTM1 and GSTT1 have polymorphisms predominantly in some genetic loci of these isoenzymes. Homozygous null mutations at the GSTM1 and GSTT1 loci lead to the absence of GST activity, which may modulate susceptibility to drug- and xenobiotic-induced hepatotoxicity [16, 17]. GSTM1 and GSTT1 had been considered as candidate drug-metabolizing genes by some studies looking at genetic predisposition to ATD-induced hepatotoxicity. For instance, Roy et al., in 2001, demonstrated firstly that there was a possible excess risk of ADIH in individuals with homozygous null mutations in the GSTM1 genes, but not in the GSTT1 genes [18]. Subsequently, many studies have been published, but these results have not been replicated and have reported inconclusive data, since both positive and negative results were documented in our view. These conflicting conclusions might stem from various designs, different methodologies, and insufficient power. Moreover, the prevalence of both GSTM1 and GSTT1 null polymorphisms may vary among populations and races.
A meta-analysis has the advantage of reducing random error and obtaining precise estimates for some potential genetic associations between GSTM1 and GSTT1 polymorphisms and ADIH risk by performing a quantitative synthesis of data from all eligible studies. Regarding the GSTM1 and GSTT1 null genotypes in ADIH, two meta-analyses have appeared in 2008 and 2012 [19, 20], respectively. However, two otherwise eligible case–control studies [21, 22] published have not been taken into account. It is worth mentioning that the above-mentioned meta-analyses had reached some conclusions, but concerning the GSTM1 null genotype, Monteiro et al. [20] did not support any association. In addition, two foregoing meta-analyses did not take the effect of different drug treatment combinations on the relationship between GSTM1 and GSTT1 genetic polymorphisms and susceptibility to ADIH into consideration.
Therefore, an updated meta-analysis of published case–control and cohort studies was performed, aimed at further clarifying the effects of GSTM1 and GSTT1 polymorphisms on the risk of developing ADIH and, simultaneously, subgroup analyses for ethnicity and combinations of different drug treatments were performed. In this study, several additional epidemiologic studies were included which took a greater number of subjects into consideration and, hence, more detailed and accurate risk was assessed compared to the previous meta-analyses.
Materials and methods
Literature search strategy and selection criteria
A comprehensive systematic bibliographic search was conducted through the digital medical databases Medline, Embase, and CBM for all medical publications up to October 2012 using the following keywords, variably combined: (“Anti-tuberculosis drug-induced hepatotoxicity”, “Anti-tuberculosis drug-induced liver injury”, “ADILI”, or “ADIH”) and (“glutathione S-transferase”, “GST”, “GSTM”, “GSTM1”, “GSTT”, or “GSTT1”) and (“Polymorphism”, “Polymorphisms”, or “Genetic polymorphism”). The search was conducted on human subjects, having no restrictions on time period, sample size, population, language, or type of report, in order to minimize the potential publication bias.
The inclusion criteria were as follows: (1) case–control studies which evaluated associations between GST polymorphisms and ADIH risk; (2) use of an unrelated case–control design; (3) estimation of odds ratios (ORs) with 95 % confidence intervals (CIs) or other available data for estimating the OR (95 % CI).
The following exclusion criteria were applied: studies without genotype data of cases and controls, case-only studies, duplicates, case reports, non-human studies, interim analyses, comparisons of laboratory methods, editorials, and review articles (including meta-analyses).
Data extraction and study design
For each of the eligible case–control studies, the following information was extracted: the surname of the first author, year of publication, country, ethnicity of subjects, sample size of genotyped cases and controls, gender, anti-tuberculosis drugs used, genotype studied, and genotyping methods. To ensure the accuracy of the extracted data, two investigators (Cuiping Li and Yang Zhou), working independently, searched the initially relevant literature using the keywords mentioned above in the search strategy. After having identified the related titles, the abstracts of these studies were reviewed in order to decide whether a study was eligible. The reference lists of reviews and retrieved articles were hand-searched manually at the same time. When more than one article was available for a single unique study population, only the most updated report with larger sample size was selected [23]. Then, information was extracted independently from each eligible case–control study and differences in eligibility were resolved by coming to an agreement between the two investigators. Subgroup analyses were mainly performed by ethnicity and the anti-tuberculosis drugs used. Ethnic groups were mainly defined as East Asian, Indian, and non-Asian (Brazilians and Caucasian). Different treatment combinations were defined as H, HRZ, HRZ, HRZE, and HRZES simultaneously.
Statistical analysis
The strength of the associations between GSTM1 and GSTT1 polymorphisms and risk of ADIH was measured by ORs with corresponding 95 % CIs. The associations of null genotypes of GSTM1 and GSTT1 with the risk of ADIH were examined compared with genotypes present according to the genetic model (null genotype vs. non-null genotype). In the present study, as two models of meta-analysis for calculating the pooled ORs, the random-effects model and the fixed-effects model were conducted using the DerSimonian and Laird and Mantel–Haenszel methods, respectively [24, 25]. The former assumed that the study sample was taken from populations with varying effect sizes, calculating the study weights both from in-study and between-study variances, while the latter assumed that the study sample came from populations with the same effect size, making an adjustment to the study weights on the basis of the in-study variance. Both the Chi-square statistic and the Q statistic (Cochran’s Q statistic) were calculated to in order evaluate statistical heterogeneity; when the p-value was < 0.1, the presence of heterogeneity among studies existed [26]. The I2 statistic was calculated in order to quantify the proportion of the total variation due to heterogeneity, with I2 > 50 % indicating statistical significance [27]. The overall or pooled estimate of risk (OR) was calculated by the Mantel–Haenszel fixed-effects model initially [25]. We employed sensitivity analyses in order to exclude the studies that potentially biased the overall summary estimate when heterogeneity between studies existed, but the random-effects model was applied to settle the studies with the presence of heterogeneity [28]. When the results had differences amongst constituent studies, random-effects models were used to incorporate an estimate of the between-study variance and provide wider 95 % CIs. Random effects were reported unless stated otherwise.
Subgroup analyses were conducted to evaluate the covariate effects, grouping primarily studies which showed similar characteristics, such as ethnicity and drug treatment combinations. Ethnic subgroups were categorized into four groups (East Asian, Indian, Brazilians, and Caucasian), while drug treatment combinations were analyzed as five groups (H, HR, HRZ, HRZE, and HRZES). Potential publication bias was determined with both visual inspection with a funnel plot and statistical evaluation with Begg and Egger’s unweighted regression test [29, 30], measuring the magnitude of funnel plot asymmetry. Statistical analyses were implemented with Stata version 11.2 (Stata Corporation, College Station, TX). It was considered to be statistically significant when a two-tailed p-value was less than 0.05.
Results
Identification and characteristics of the included studies
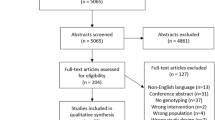
A total of 451 studies were yielded meeting the search criteria through the literature databases. We screened 19 potentially relevant studies exploring the effect of GSTM1 and GSTT1 polymorphism on the susceptibility of ADIH. However, after obtaining and reading the full articles, six studies were excluded: two studies without data of interest or raw data [31, 32], three review articles [19, 20, 33], and one duplicated/overlapped article [34, 35]. Searching the references cited in the published studies manually did not reveal any additional articles. As a result, only 13 studies finally met the predetermined inclusion criteria and were included in this meta-analysis [18, 36–45]. The specific process of publication selection and exclusion is shown in Fig. 1. Among these studies, 13 studies including a total of 951 ADIH cases, 1,922 controls dealt with the GSTM1 null polymorphism, whereas 12 studies providing 847 cases, 1,811 controls dealt with the GSTT1 null polymorphism.

Flow diagram of this meta-analysis
Of the included studies, the populations of seven studies were of East Asian descent, two studies of Brazilians descent, three studies of Indian descent, and one study of Caucasian descent. Concerning the effects of different drug interactions, two articles used H or HR, two articles used HRZ, four articles used HRZE, and three articles used HRZES. Multiplex polymerase chain reaction (PCR) and PCR assays were performed in all the included studies. The main characteristics of the eligible studies are summarized in Table 1.
Quantitative synthesis
Overall, in these 13 studies meeting the inclusion criteria selected in this meta-analysis, five demonstrated an association between the GSTM1 null genotype and an increased risk of ADIH, which was statistically significant [18, 21, 36, 41, 45], while the remaining eight studies showed no significant difference [22, 37–43]. All groups were pooled and the OR was 1.36 (95 % CI: 1.04–1.79), which showed an increased risk effect of the GSTM1 null genotype on the susceptibility to ADIH using random-effects models, reaching statistical significance in the Q-test of between-study heterogeneity (I2 = 57.6 %, p = 0.005) (Table 2, Fig. 2). The 12 included studies dealt with the GSTT1 null polymorphism, only one of which considered that the GSTT1 null genotype was a risk factor for ADIH [39], and no association was found by the other studies [18, 21, 22, 36–38, 40, 42–45]. The result of this meta-analysis showed a statistically non-significant association between the genotype deficiency of GSTT1 and ADIH risk (fixed-effects model; OR = 0.98, 95 % CI: 0.82–1.18; I2 = 30.7 %, p = 0.848 for heterogeneity) (Table 2, Fig. 3). Table 2 summarizes the meta-analyses of the association of the null GSTM1 and GSTT1 genotype polymorphisms with ADIH risk, respectively. The above analysis pooled all data, not taking into account the different ethnic groups and drug treatment combinations.

Forest plot for the overall association between the null GSTM1 genotype and ADIH risk. Each comparison is presented by the surname of the first author and the year of publication. The point estimate of the OR by subgroup analysis (different ethnicity and treatment combinations, respectively) and the corresponding 95 % CI for each comparison are shown; the pooled OR and 95 % confidence interval have been appropriately derived from the random-effects model. OR, odds ratio; CI, confidence interval; ADIH, anti-tuberculosis drug-induced hepatotoxicity. INH, isoniazid; RMP, rifampicin; PZA, pyrazinamide; EMB, ethambutol; SM, streptomycin. NA, relative data were not available in the original studies

Forest plot for the overall association between the null GSTT1 genotype and ADIH risk. The format of the figures is as per Fig. 2, except that the pooled results were derived from the fixed-effects model. NA, relative data were not available in the original studies
Subgroup analyses were performed in order to evaluate the covariate effects in the different ethnic groups and drug combinations. In the subgroup analyses for the null GSTM1 and GSTT1 genotype polymorphisms, the combined results showed that the null GSTM1 genotype polymorphism was significantly associated with increased risk of ADIH in the East Asian population under a fixed-effects model (OR = 1.59, 95 % CI: 1.3–1.93; I2 = 26.6 %, p = 0.226 for heterogeneity) and in the patients receiving HRZE under a fixed-effects model (OR = 1.47, 95 % CI: 1.14–1.9; I2 = 0 %, p = 0.406 for heterogeneity) and HRZES under a random-effects model (OR = 1.89, 95 % CI: 1.09–3.27; I2 = 61.6 %, p = 0.076 for heterogeneity) (Table 2, Fig. 2). In addition, it was observed that there was, in fact, a statistically significant association between GSTT1 deficiency and the risk of ADIH in the patients receiving HRZ (OR = 2.46, 95 % CI: 1.14–5.32; I2 = 0 %, p = 0.791 for heterogeneity) (Table 2, Fig. 3). It was worth noting that, owing to only a single study, two results deserved further investigation, which revealed that GSTM1 deficiency was significantly associated with decreased ADIH risk in the patients receiving HR and GSTT1 deficiency increased ADIH risk in the Caucasian population.
Sensitivity analyses and publication bias
Sensitivity analysis was carried out to determine the effect of individual study on the summary meta-analysis estimate, wherein an individual study was excluded each time. Substantial changes did not occur for the corresponding combined ORs, so our results were considered to be statistically robust. Both Begg’s and Egger’s funnel plot asymmetry test in the overall meta-analysis performed on the GSTM1 (p-values were 0.855 and 0.495, respectively) and GSTT1 (p-values were 0.373 and 0.161, respectively) polymorphism status revealed no evidence of publication bias.
Discussion
GST, as an important phase 2 enzyme, is principally expressed in the liver, occupying a key position in detoxification and metabolism. As two of the most relevant human isoenzymes, GSTM1 and GSTT1, their genes are polymorphic. The homozygous deletions of GSTM1 and GSTT1 genotypes have been speculated to be predictors of liver injury. Some studiers have provided evidence that homozygous null mutations of these genes increased the risk of liver injury induced by drugs such as methotrexate [46], troglitazone [47], tacrine [48], carbamazepine [49], and so on. However, whether GSTM1 and GSTT1 null genotypes are genetic predictors of ADIH is still unclear. The published studies have shown discordant results.
Meta-analysis has been recognized to have a very strong ability to more precisely define the effect of selected genetic polymorphisms on the susceptibility to disease and identify potentially important sources of between-study heterogeneity. Concerning the relationship between GSTM1 and GSTT1 null genotypes and ADIH risk, Sun et al. [19] and Cai et al. [20] have made an evaluation using meta-analysis in 2008 and 2012, respectively. After that, to the best of our knowledge, only two case–control studies have been published, and one provided a controversial result [47]. The most likely and reasonable explanation for the inconsistent results of previous studies was that the small sample sizes of individual studies may result in low statistical power. Therefore, the principal purpose of this updated meta-analysis was to examine an association of two polymorphisms of GST (M1 and T1) with ADIH risk containing a larger sample size which included all the available published studies (13 studies) with a total of 951 cases and 1,922 controls concerning the GSTM1 polymorphism, and 12 studies with 847 cases and 1,811 controls concerning the GSTT1 polymorphism. Moreover, this was the first systematic review to evaluate the interaction of different drug combinations in the subgroup analysis. Heterogeneity analysis and sensitivity analysis were also critically carried out to ensure the epidemiological credibility of this meta-analysis. Overall, the main results of our review provided evidence that the GSTM1 polymorphism was associated with the increased susceptibility to ADIH in the total population but not for GSTT1 null/null genotypes, which was consistent with two previous meta-analyses [19, 20]. For the non-significant differences in the GSTT1 polymorphism between the case group and the control group, the most likely explanations were as follows: (1) in the substrates of GSTM1 and GSTT1 enzymes existed a cross-phenomenon in the human body, toxic metabolites of anti-tuberculosis drugs may be detoxified more by GSTM1 enzyme, compensating partly for the role of GSTT1 enzyme; (2) the low frequency of ADIH patients with GSTT1 and a small sample size may lead to the statistically non-significant results. Confirmation with a large-scale study is mandatory.
The sources of heterogeneity, as a potential problem when interpreting the results of all meta-analyses, is one of the most important goals of meta-analysis [50]. Generally, there was significant between-study heterogeneity in the association between GSTM1 and ADIH in the overall populations, rather than GSTT1 null genotypes. To find the major sources of heterogeneity for the GSTM1 polymorphisms, we first performed two subgroup meta-analyses by ethnicity and different treatment combinations. Subgroup analyses indicated that the heterogeneity was still significant in the Indian and HRZES use populations, which contributed greatly to the existence of overall heterogeneity. Galbraith plots then indicated two studies [21, 45] as outliers, which were possibly the sources of heterogeneity. The heterogeneity was adjusted and eliminated (I2 = 3.1 %) after the exclusion of these studies. Meanwhile, the evaluation magnitude was increased (OR = 1.39) and a more precise 95 % CI (1.16–1.66) was obtained. Therefore, we could draw a conclusion that the studies by Guo et al. [45] and Rana et al. [21] may be the major reason for the heterogeneity in the GSTM1 polymorphisms analysis and that they might have some differences in comparison with other studies in the control selection procedures or other ambiguous aspects. For example, as two major risk factors of ADIH analyzed, body mass index and alcohol drinking were significantly associated with ADIH between the case group and the control group in Guo et al.’s study [45]. Nevertheless, the data were integrated without adjusting for the influences of body mass index and drinking. This discordance in the selection of controls among different publications might possibly lead to between-study heterogeneity. The hypothesis above was further validated.
The different distribution of various ethnicities between cases and controls may be the answer for confounding when pooling studies [51, 52]. Furthermore, major ethnic differences in the frequency of these GSTM1 and T1 null genotypes may exist [50]. Hence, we performed subgroup analyses by ethnicity and different treatment combinations in order to avoid potential overestimation of the true effect of polymorphism on ADIH risk. We found that the GSTM1 null genotype was significantly associated with the risk of ADIH in the East Asian population and patients receiving HRZE and HRZES rather than in other population. Regarding GSTT1 null allele carriers, the subgroup analyses showed that the associations above were significant in the Caucasian population and patients receiving HR and HRZ, and there was no association in the other subgroup. These observations may suggest racial predisposition and, potentially, different mechanisms occurring with different drug treatments. However, these associations are still not fully certain. The same polymorphism playing different roles in disease susceptibility amongst the different ethnicities and treatment combinations may be due to several possibilities deserving attention. (1) They may indicate authentically different effects of the GSTM1 deleted genotype on ADIH risk, but not for GSTT1 null allele carriers. ADIH is a complicated multigenetic disease and different ethnic genetic backgrounds and drug interactions may contribute to the discrepancy. (2) Owing to the lack of a large number of relevant studies included in this meta-analysis, especially for Caucasians and HR and HRZ use patients, with only one article each, the ethnic and drug use collocations observed in this meta-analysis are also likely to be the result of happenstance because studies with small sample sizes possibly have no inadequate statistical power to detect a slight effect or may have created a fluctuation of risk estimates. (3) The discrepancy was also likely to stem from different study designs, insufficient power, and various methodology, including inclusion and/or exclusion criteria, quality of included studies, selection bias, and type I error, with no connection with ethnicities and treatment combinations of cases. Currently, the association between the GSTM1 and GSTT1 polymorphisms and ADIH risk remained enigmatic, the finding of which needs further confirmation in a large-scale study.
Some potential limitations in our study deserve consideration. Firstly, some potential confounding factors, such as age, sex, nutrition, complications of diseases, alcohol abuse, body mass index, smoking status, HIV infection, and viral hepatitis B and C infections, cannot be ruled out, stemming from the unadjusted data used. Secondly, the between-study heterogeneity is a problem in the present analysis. A fairly large degree of heterogeneity was identified for the association between GSTM1 and ADIH in the overall populations. The observed heterogeneity did not disappear when subgroup analyses were performed; therefore, it should be prudent to consider this when drawing corresponding conclusions. Thirdly, it should also be necessary to emphasize that the conclusion for Caucasians and HR and HRZ used tuberculosis must be interpreted prudently, owing to a single report of an association between a genetic variant and disease susceptibility in this meta-analysis. Fourthly, although according to a sensitive search strategy set eligible studies were retrieved, we cannot eliminate the fact that some studies and unpublished reports might have been missed. Therefore, we might miss a chance to obtain a larger sample size and increased statistical power. Fifthly, tuberculosis diagnosis standard and ADIH patients’ enrollment criteria were not absolutely identical in the involved studies, increasing the likelihood of selection bias in our study. Sixthly, this meta-analysis took no account of some other important factors when using anti-tuberculosis drugs, such as type and dosage, therapeutic regimes (DOTS or non-DOTS), and so on, which may possibly affect the susceptibility to ADIH for GSTM1 or GSTT1 null genotypes.
In summary, this meta-analysis provides evidence that the GSTM1 polymorphism is associated with increased risk of ADIH in the entire population, especially among East Asians. Moreover, no significant differences were observed for the association between the GSTT1 polymorphism and the risk of ADIH in the whole population. To date, there is inadequate evidence implicating GSTM1 and GSTT1 polymorphisms in the etiology of ADIH for population testing; greater attention, should, therefore be paid to the design of future studies. Due to the relatively limited studies on the relationship between different GST genotypes and ADIH, the role of these genes cannot be elucidated fully; thus, larger sample sizes and well-designed multicentric studies must be conducted in order to reassess such an association.
References
WHO global tuberculosis control report 2010 (2010) Summary. Cent Eur J Public Health 18:237
Blumberg HM, Burman WJ, Chaisson RE, Daley CL, Etkind SC, Friedman LN, Fujiwara P, Grzemska M, Hopewell PC, Iseman MD, Jasmer RM, Koppaka V, Menzies RI, O’Brien RJ, Reves RR, Reichman LB, Simone PM, Starke JR, Vernon AA; American Thoracic Society, Centers for Disease Control and Prevention and the Infectious Diseases Society (2003) American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis. Am J Respir Crit Care Med 167:603–662
Chemotherapy and management of tuberculosis in the United Kingdom: recommendations 1998(1998) Joint Tuberculosis Committee of the British Thoracic Society. Thorax 53:536–548
Garibaldi RA, Drusin RE, Ferebee SH, Gregg MB (1972) Isoniazid-associated hepatitis. Report of an outbreak. Am Rev Respir Dis 106:357–365
Saukkonen JJ, Cohn DL, Jasmer RM, Schenker S, Jereb JA, Nolan CM, Peloquin CA, Gordin FM, Nunes D, Strader DB, Bernardo J, Venkataramanan R, Sterling TR; ATS (American Thoracic Society) Hepatotoxicity of Antituberculosis Therapy Subcommittee (2006) An official ATS statement: hepatotoxicity of antituberculosis therapy. Am J Respir Crit Care Med 174:935–952
Acharya SK, Dasarathy S, Kumer TL, Sushma S, Prasanna KS, Tandon A, Sreenivas V, Nijhawan S, Panda SK, Nanda SK, Irshad M, Joshi YK, Duttagupta S, Tandon RK, Tandon BN (1996) Fulminant hepatitis in a tropical population: clinical course, cause, and early predictors of outcome. Hepatology 23:1448–1455
Grönhagen-Riska C, Hellstrom PE, Fröseth B (1978) Predisposing factors in hepatitis induced by isoniazid–rifampin treatment of tuberculosis. Am Rev Respir Dis 118:461–466
Mitchell JR, Zimmerman HJ, Ishak KG, Thorgeirsson UP, Timbrell JA, Snodgrass WR, Nelson SD (1976) Isoniazid liver injury: clinical spectrum, pathology, and probable pathogenesis. Ann Intern Med 84:181–192
Tostmann A, Boeree MJ, Aarnoutse RE, de Lange WC, van der Ven AJ, Dekhuijzen R (2008) Antituberculosis drug-induced hepatotoxicity: concise up-to-date review. J Gastroenterol Hepatol 23:192–202
Naisbitt DJ, Williams DP, Pirmohamed M, Kitteringham NR, Park BK (2001) Reactive metabolites and their role in drug reactions. Curr Opin Allergy Clin Immunol 1:317–325
Meister A (1983) Selective modification of glutathione metabolism. Science 220:472–477
Meister A, Anderson ME (1983) Glutathione. Annu Rev Biochem 52:711–760
Andreoli SP, Mallett CP, Bergstein JM (1986) Role of glutathione in protecting endothelial cells against hydrogen peroxide oxidant injury. J Lab Clin Med 108:190–198
Mitchell JR, Jollow DJ, Potter WZ, Gillette JR, Brodie BB (1973) Acetaminophen-induced hepatic necrosis. IV. Protective role of glutathione. J Pharmacol Exp Ther 187:211–217
Fontana X, Peyrottes I, Rossi C, Leblanc-Talent P, Ettore F, Namer M, Bussière F (1998) Study of the frequencies of CYP1A1 gene polymorphisms and glutathione S-transferase mu1 gene in primary breast cancers: an update with an additional 114 cases. Mutat Res 403:45–53
Hussey AJ, Stockman PK, Beckett GJ, Hayes JD (1986) Variations in the glutathione S-transferase subunits expressed in human livers. Biochim Biophys Acta 874:1–12
Meyer DJ, Coles B, Pemble SE, Gilmore KS, Fraser GM, Ketterer B (1991) Theta, a new class of glutathione transferases purified from rat and man. Biochem J 274(Pt 2):409–414
Roy B, Chowdhury A, Kundu S, Santra A, Dey B, Chakraborty M, Majumder PP (2001) Increased risk of antituberculosis drug-induced hepatotoxicity in individuals with glutathione S-transferase M1 ‘null’ mutation. J Gastroenterol Hepatol 16:1033–1037
Sun F, Chen Y, Xiang Y, Zhan S (2008) Drug-metabolising enzyme polymorphisms and predisposition to anti-tuberculosis drug-induced liver injury: a meta-analysis. Int J Tuberc Lung Dis 12:994–1002
Cai Y, Yi J, Zhou C, Shen X (2012) Pharmacogenetic study of drug-metabolising enzyme polymorphisms on the risk of anti-tuberculosis drug-induced liver injury: a meta-analysis. PLoS One 7:e47769
Rana SV, Sharma SK, Ola RP, Sinha SK, Arora SK, Singh K (2012) Antitubercular treatment induced hepatotoxicity in north Indians—role of glutathione-S-transferase, N-acetyltransferase2 and cytochrome P4502E1 gene polymorphisms. J Clin Exp Hepatol 2:S36–S37
Monteiro TP, El-Jaick KB, Jeovanio-Silva AL, Brasil PE, Costa MJ, Rolla VC, de Castro L (2012) The roles of GSTM1 and GSTT1 null genotypes and other predictors in anti-tuberculosis drug-induced liver injury. J Clin Pharm Ther 37:712–718
Petitti DB (2000) Meta-analysis, decision analysis, and cost-effectiveness analysis: methods for quantitative synthesis in medicine, 2nd edn. Oxford University Press, New York
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7:177–188
Sutton AJ, Abrams KR, Jones DR, Sheldon TA, Song F (2000) Methods for meta-analysis in medical research. Wiley, Chichester
Cochran WG (1954) The combination of estimates from different experiments. Biometrics 10:101–129
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
Lau J, Ioannidis JP, Schmid CH (1997) Quantitative synthesis in systematic reviews. Ann Intern Med 127:820–826
Begg CB, Mazumdar M (1994) Operating characteristics of a rank correlation test for publication bias. Biometrics 50:1088–1101
Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629–634
Forestiero FJ, Cecon L, Hirata MH, de Melo FF, Cardoso RF, Cerda A, Hirata RD (2013) Relationship of NAT2, CYP2E1 and GSTM1/GSTT1 polymorphisms with mild elevation of liver enzymes in Brazilian individuals under anti-tuberculosis drug therapy. Clin Chim Acta 415:215–219
Costa GN, Magno LA, Santana CV, Konstantinovas C, Saito ST, Machado M, Di Pietro G, Bastos-Rodrigues L, Miranda DM, De Marco LA, Romano-Silva MA, Rios-Santos F (2012) Genetic interaction between NAT2, GSTM1, GSTT1, CYP2E1, and environmental factors is associated with adverse reactions to anti-tuberculosis drugs. Mol Diagn Ther 16:241–250
Huang YS (2007) Genetic polymorphisms of drug-metabolizing enzymes and the susceptibility to antituberculosis drug-induced liver injury. Expert Opin Drug Metab Toxicol 3:1–8
Wang J, Deng Y, Li L, Kuriki K, Ding J, Pan X, Zhuge X, Jiang J, Luo C, Lin P, Tokudome S (2003) Association of GSTM1, CYP1A1 and CYP2E1 genetic polymorphisms with susceptibility to lung adenocarcinoma: a case–control study in Chinese population. Cancer Sci 94:448–452
Wang T, Yu HX, Wang W, Pan YY, He LX, Wang ZY (2011) Association of GSTM1 genetic polymorphisms with susceptibility to antituberculosis drug induced hepatotoxicity, a study in Chinese population. Chin J Med Guide 13:2164–2165
Huang YS, Su WJ, Huang YH, Chen CY, Chang FY, Lin HC, Lee SD (2007) Genetic polymorphisms of manganese superoxide dismutase, NAD(P)H:quinone oxidoreductase, glutathione S-transferase M1 and T1, and the susceptibility to drug-induced liver injury. J Hepatol 47:128–134
Teixeira RL, Morato RG, Cabello PH, Muniz LM, Moreira Ada S, Kritski AL, Mello FC, Suffys PN, Miranda AB, Santos AR (2011) Genetic polymorphisms of NAT2, CYP2E1 and GST enzymes and the occurrence of antituberculosis drug-induced hepatitis in Brazilian TB patients. Mem Inst Oswaldo Cruz 106:716–724
Chatterjee S, Lyle N, Mandal A, Kundu S (2010) GSTT1 and GSTM1 gene deletions are not associated with hepatotoxicity caused by antitubercular drugs. J Clin Pharm Ther 35:465–470
Leiro V, Fernández-Villar A, Valverde D, Constenla L, Vázquez R, Piñeiro L, González-Quintela A (2008) Influence of glutathione S-transferase M1 and T1 homozygous null mutations on the risk of antituberculosis drug-induced hepatotoxicity in a Caucasian population. Liver Int 28:835–839
Tang SW, Lv XZ, Zhang Y, Wu SS, Yang ZR, Xia YY, Tu DH, Deng PY, Ma Y, Chen DF, Zhan SY (2012) CYP2E1, GSTM1 and GSTT1 genetic polymorphisms and susceptibility to antituberculosis drug-induced hepatotoxicity: a nested case–control study. J Clin Pharm Ther 37:588–593
Wang T, Yu HT, Wang W, Pan YY, He LX, Wang ZY (2010) Genetic polymorphisms of cytochrome P450 and glutathione S-transferase associated with antituberculosis drug-induced hepatotoxicity in Chinese tuberculosis patients. J Int Med Res 38:977–986
Zhu DL, Xi Y, Wu XQ (2011) Relationship between genetic polymorphisms of GSTM1, GSTT1 and the susceptibility to antituberculosis drug-induced liver injury. Zhongguo Kang Sheng Su Za Zhi 36:864–868
Kim SH, Kim SH, Yoon HJ, Shin DH, Park SS, Kim YS, Park JS, Jee YK (2010) GSTT1 and GSTM1 null mutations and adverse reactions induced by antituberculosis drugs in Koreans. Tuberculosis (Edinb) 90:39–43
Sotsuka T, Sasaki Y, Hirai S, Yamagishi F, Ueno K (2011) Association of isoniazid-metabolizing enzyme genotypes and isoniazid-induced hepatotoxicity in tuberculosis patients. In Vivo 25:803–812
Guo M, Sun YH, Li SM, Wang D, Liu Q, Zhang XY, Liu XX, Feng FM (2009) The effect of GST M1 and GST T1 gene mutations on anti-tuberculous drug induced hepatic injury. Zhonghua Jie He He Hu Xi Za Zhi 32:266–269
Imanishi H, Okamura N, Yagi M, Noro Y, Moriya Y, Nakamura T, Hayakawa A, Takeshima Y, Sakaeda T, Matsuo M, Okumura K (2007) Genetic polymorphisms associated with adverse events and elimination of methotrexate in childhood acute lymphoblastic leukemia and malignant lymphoma. J Hum Genet 52:166–171
Watanabe I, Tomita A, Shimizu M, Sugawara M, Yasumo H, Koishi R, Takahashi T, Miyoshi K, Nakamura K, Izumi T, Matsushita Y, Furukawa H, Haruyama H, Koga T (2003) A study to survey susceptible genetic factors responsible for troglitazone-associated hepatotoxicity in Japanese patients with type 2 diabetes mellitus. Clin Pharmacol Ther 73:435–455
Simon T, Becquemont L, Mary-Krause M, de Waziers I, Beaune P, Funck-Brentano C, Jaillon P (2000) Combined glutathione-S-transferase M1 and T1 genetic polymorphism and tacrine hepatotoxicity. Clin Pharmacol Ther 67:432–437
Ueda K, Ishitsu T, Seo T, Ueda N, Murata T, Hori M, Nakagawa K (2007) Glutathione S-transferase M1 null genotype as a risk factor for carbamazepine-induced mild hepatotoxicity. Pharmacogenomics 8:435–442
Ioannidis JP, Patsopoulos NA, Evangelou E (2007) Uncertainty in heterogeneity estimates in meta-analyses. BMJ 335:914–916
Ye Z, Song H (2005) Glutathione s-transferase polymorphisms (GSTM1, GSTP1 and GSTT1) and the risk of acute leukaemia: a systematic review and meta-analysis. Eur J Cancer 41:980–989
Garte S (1998) The role of ethnicity in cancer susceptibility gene polymorphisms: the example of CYP1A1. Carcinogenesis 19:1329–1332
Acknowledgments
We are thankful to all the participants of our study. This study was not supported by any grants.
Conflict of interest
We declare that we have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Cuiping Li, Jianxiong Long, and Xueying Hu contributed equally to this work.
Rights and permissions
About this article
Cite this article
Li, C., Long, J., Hu, X. et al. GSTM1 and GSTT1 genetic polymorphisms and risk of anti-tuberculosis drug-induced hepatotoxicity: an updated meta-analysis. Eur J Clin Microbiol Infect Dis 32, 859–868 (2013). https://doi.org/10.1007/s10096-013-1831-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-013-1831-y