
Abstract
Acute stroke and transient ischemic attack (TIA) is a great burden not only during hospitalization but also after hospital discharge. The objective of this meta-analysis was to evaluate the hospital readmissions, causes and risk factors after survival of acute stroke and TIA. Pubmed, Web of Science, Cochrane Library, OVID and EMBASE databases were searched to identify studies reporting hospital readmissions after acute stroke and TIA. The primary outcomes were hospital readmission rates during 30 days and 1 year after discharge. The primary causes and risk factors of hospital readmissions were also identified. Ten studies with 253,680 patients were eligible for inclusion. The pooled 30-day and 1-year hospital readmission rates were 17.4 % (95 % CI, 12.7–23.5 %) and 42.5 % (95 % CI, 34.1–51.3 %), respectively. The three major causes of 30-day hospital readmissions were infection (19.9 %), coronary artery disease (CAD) (17.8 %) and recurrent stroke (16.0 %) successively, while the three major causes were recurrent stroke (19.4 %), infection (19.3 %) and CAD (16.3 %) during 1 year’s follow-up. There were more patients with CAD in readmits group than that in control group (p = 0.030). The length of index admission, defined as any eligible admission to an acute care hospital assessed in the measure for the outcome, was longer (p = 0.000) and admission National Institutes of Health Stroke Score (NIHSS) was higher (p = 0.002) in readmits group than these in control group. In conclusion, there is high risk of early and long-term hospital readmissions after survival of acute stroke and TIA. These patients with coronary artery disease, longer length of index admission and higher NIHSS deserve deep attention after hospital discharge.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acute stroke and transient ischemic attack (TIA) is emerging as a leading cause of preventable death and disability worldwide [1]. Stroke survivors often face high risks of mortality and stroke recurrence. For stroke patients, hospitalizations can be stressful and even more so when they result in subsequent readmissions to the hospital. It has been found that 16 % of stroke patients may experience two or more readmissions within 30 days of the incident admission [2] and about 50 % of 30-day readmissions have been classified as avoidable [3].
Hospital readmissions contribute significantly to the cost of inpatient care and are targeted as a marker for quality of care [4]. Researchers have found wide variation in hospitals’ readmission rates [5] and a number of studies show that hospitals can engage in several activities to lower their rate of readmissions [6]. In USA, Medicare has started implementing incentives to reduce hospital readmissions, such as the Hospital Readmissions Reduction Program (HRRP).
We conducted a meta-analysis to estimate the pooled short-term and long-term readmission rates, the common causes and the risk factors of readmissions after discharge of acute stroke and TIA during various follow-up periods. This effort hopes to raise awareness of hospital readmissions after acute stroke and TIA, and to provide considerable healthcare resources after hospital discharge.
Methods
Search strategy and data sources
We performed a computerized search to identify relevant published original studies (1985 to November 2015). Pubmed, Web of Science, Cochrane Library, OVID and EMBASE databases were searched using medical subject headings (MeSH) or keywords. These words were “acute stroke, acute ischemic stroke (AIS), transient ischemic attack, acute cerebral infarction, acute intracerebral hemorrhage (ICH), acute cerebral hemorrhage, hemorrhagic stroke” and “re*hospital*, re*admission*”. This search was not limited to English language or publication type.
Selection criteria
An initial eligibility screen of all retrieved titles and abstracts was conducted, and only studies reporting rehospitalization after acute stroke or TIA were selected for further review. The following included criteria were used for final selection: (1) studies reporting the hospital readmissions after AIS, TIA or ICH, (2) studies providing detailed information about the rehospitalization rates during follow-up periods (30 days or 1 year). We restricted our search to clinical studies performed in adult populations. Studies without clear rehospitalization rates or experimental studies were excluded.
Data extraction and quality assessment
WBZ performed the first screening of published reports, while two reviewers (WBZ and NG) independently examined the studies, and disagreement was resolved by discussion. Data extraction included country of origin, year of publication, study period, source of data, primary diseases, sample size, patient characteristics (age and sex). The primary outcomes were hospital readmission rates during 30 days and 1 year after discharge. The primary causes and risk factors of hospital readmissions were also identified. The study selection, data extraction, and reporting of results were all based on the preferred reporting items for systematic reviews and meta-analyses checklist [7]. The quality of the cohort studies was assessed independently by pairs of two authors, using the Newcastle–Ottawa scale (NOS) [8], which allocates a maximum of nine points for quality of the selection, comparability, and outcome of study populations. Study quality scores were defined as poor (0–3), fair (4–6), or good (7–9).
Data synthesis and statistical analysis
Comprehensive meta-analysis (version 2.0; Biostat) was used to perform the meta-analysis. Pooled estimates were obtained for rates, causes and risk factors of hospital readmissions reported using random-effects meta-analysis based on the methods of DerSimonian and Laird [9]. Meta-analyses were performed using odds ratio (OR) for dichotomous outcomes and standard difference (Std diff) in means for continuous outcomes. All confidence intervals (CI) were reported at 95 percent. P value statistical significance was measured at 0.05. Heterogeneity across trials was evaluated with using the I 2 index and the Q test p value. A p value of less than 0.05 and an I 2 index of more than 25 % indicated the presence of interstudy heterogeneity [10]. Publication bias was assessed by constructing a funnel plot and Egger’s regression test.
Results
Study selection
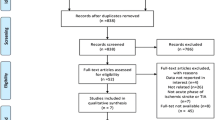
The article selection process is outlined in Fig. 1. After primary screening, 116 articles were excluded without meeting criteria of final selection. At the full-text review stage, 35 articles were not about acute stroke or TIA, 18 did not involve rehospitalization and 15 were reviews. Four studies were excluded from the primary meta-analysis as they did not report the number of patients rehospitalizing during the follow-up periods, and the corresponding authors were unable to provide the requisite data. After screening, ten studies with 253,680 patients were included in this systematic review. Agreement between investigators at the full-text review stage was excellent as indicated by a κ of 0.8.

Flowchart of literature search and study selection
Study description and quality assessment
A detailed description of the included studies is provided in Table 1. The included studies were published between 2006 and 2015. Most of the included studies (n = 7) occurred in the United States of America, and two in China (Taiwan). The total number of patients included in the primary meta-analysis was 253,680 with a median (interquartile range) of 1009 (121–200,900) patients per study. Detailed information of age and gender is also listed in Table 1. Overall study quality was good with a mean NOS score of 7.6 out of a possible nine (range, 6–9) and with eight studies (80 %) receiving a NOS greater than or equal to seven Table 2.
Hospital readmission rates after acute stroke
Five studies reported 30-day post-discharge hospital readmissions after acute stroke, including AIS, TIA and ICH, and six reported 1-year rehospitalization. The pooled 30-day and 1-year hospital readmission rates were 17.4 % (95 % CI, 12.7–23.5 %) and 42.5 % (95 % CI, 34.1–51.3 %), respectively. Three studies including patients only with AIS reported 30-day and 1-year rehospitalization, and the pooled 30-day and 1-year readmission rates of these patients were 12.4 % (95 % CI, 10.8–14.1 %) and 53.0 % (95 % CI, 49.7–56.2 %), respectively (Fig. 2). There were not enough trials to conduct the readmission rates in other subgroups, such as ICH.

The pooled hospital readmission rates after acute stroke within 30-day and 1-year follow-up
Causes of hospital readmissions after acute stroke
Five studies identified the causes of hospital readmissions within 30 days after discharge, while six reported the causes within 1 year’s follow-up. The three major causes of 30-day hospital readmissions were infection, coronary artery disease (CAD) and recurrent stroke, and the pooled percentage of these causes was 19.9 % (95 % CI, 5.1–53.1 %), 17.8 % (95 % CI, 5.6–44.2 %) and 16.0 % (95 % CI, 8.6–27.7 %), respectively (Fig. 3). During 1 year’s follow-up, the three major causes of readmissions were recurrent stroke, infection and CAD, and the pooled percentage of these causes was 19.4 % (95 % CI, 14.8–25.0 %), 19.3 % (95 % CI, 15.5–23.7 %) and 16.3 % (95 % CI, 14.8–18.1 %).

Pooled estimators for three major causes of hospital readmission after acute stroke
Risk factors of hospital readmissions after acute stroke
Four studies compared the risk factors of hospital readmissions with control group. There were more patients with CAD in readmits group than that in control group (OR 0.326, 95 % CI 0.119–0.897, p = 0.030). No significant differences were identified when comparing other risk factors such as diabetes mellitus (DM), hypertension, atrial fibrillation (AF), and in-hospital neurologic deterioration (Fig. 4). The length of index admission, defined as any eligible admission to an acute care hospital assessed in the measure for the outcome, was longer (Std diff in means 0.254, 95 % CI 0.129–0.380, p = 0.000) and admission National Institutes of Health Stroke Score (NIHSS) was higher (Std diff in means 0.281, 95 % CI 0.107–0.454, p = 0.002) in readmits group than these in control group (Fig. 5).

Risk factors of hospital readmission after acute stroke—dichotomous variables. DM diabetes mellitus, CAD coronary artery disease, AF atrial fibrillation

Risk factors of hospital readmission after acute stroke—continuous variables
Publication bias
The funnel plots for Fig. 6 showed no evidence of publication bias. Egger’s test for a regression intercept gave a p value of 0.401 for 30-day rehospitalization rates after acute stroke and TIA, indicating no publication bias.

Funnel plot to evaluate for publication bias for 30-day rehospitalization rates after acute stroke
Discussion
Our meta-analysis showed that about 17.4 % of discharges after acute stroke and TIA resulted in hospital readmissions within 30 days and 42.5 % within 1 year. To our knowledge, this was the first time to conduct a meta-analysis reporting hospital readmissions after acute stroke and TIA. Given the high heterogeneity, it is best to consider the confidence interval rather than the pooled result. It is likely that the reported rates underestimate the true rate of readmissions, as patients may be treated at a different hospital and may not be reflected in the included studies. The readmission rates might be different for patients with various primary diseases, such as AIS, TIA and ICH. But we only identified enough studies to conduct the pooled readmission rates in patients with AIS. The readmission rates in AIS subgroup seemingly were lower within 30 days and higher within 1 year when comparing with total stroke patients. For limited data, further investigation may be needed to compare different readmission rates within various types of stroke.
This review also identified several common causes that lead to hospital readmissions after acute stroke. Infection, CAD and recurrent stroke were the three leading reasons not only within 30 days but also 1 year after discharge. The three major causes of 30-day hospital readmissions were infection, coronary artery disease (CAD) and recurrent stroke successively, while the three major causes were recurrent stroke, infection and CAD during 1 year’s follow-up. Infection seemingly accounted for the more proportion of readmissions within 30 days than CAD and recurrent stroke.
Although this study highlights predictors associated with unplanned readmission, it was not possible to perform a meta-regression analysis evaluating how these risk factors were associated with the overall pooled estimates, because too few studies comparably collected or reported individual factors. Four included studies compared the risk factors of hospital readmissions with control group. There were more patients with CAD in readmits group than that in control group, and stroke patients with longer length of index admission and higher NIHSS were more likely to readmit within 30 days after discharge. These factors and other factors that were identified as risk factors of readmissions may be potentially modifiable targets in future studies.
Study limitations
The present study may have limitations. Firstly, significant difference across studies in primary diseases, age and the assessment of variables, such as causes and risk factors of hospital readmissions, may lead to high heterogeneity. Secondly, all publications included in this analysis were retrospective observational studies, which are considered moderate evidence, and so the conclusions drawn in this analysis are limited by this study type. Finally, for limited studies, we could not estimate the causes and risk factors in subgroups, such as AIS and ICH, and there must be differences in these subgroups.
In conclusion, results of our systematic review suggest that there is high risk of early and long-term hospital readmissions after discharge of acute stroke and TIA. These patients with CAD and longer length of index admission and higher NIHSS deserve deep attention after hospital discharge. Further large-scale, multicenter studies with careful matching and enough follow-up periods needed for more persuasive analysis.
References
Feigin VL, Forouzanfar MH, Krishnamurthi R et al (2014) Global and regional burden of stroke during 1990–2010: findings from the global burden of disease study 2010. Lancet 383:245–255
Kind AJ, Smith MA, Frytak JR, Finch MD (2007) Bouncing back: patterns and predictors of complicated transitions 30 days after hospitalization for acute ischemic stroke. J Am Geriatr Soc 55:365–373. doi:10.1111/j.1532-5415.2007.01091.x
Nahab F, Takesaka J, Mailyan E, Judd L, Culler S, Webb A, Frankel M, Choi D, Helmers S (2012) Avoidable 30-day readmissions among patients with stroke and other cerebrovascular disease. Neurohospitalist 2:7–11. doi:10.1177/1941874411427733
Rumball-Smith J, Hider P (2009) The validity of readmission rate as a marker of the quality of hospital care and a recommendation for its definition. N Z Med J 122:63–70
Epstein AM, Jha AK, Orav EJ (2011) The relationship between hospital admission rates and rehospitalizations. N Engl J Med 365:2287–2295
Ahmad FS, Metlay JP, Barg FK, Henderson RR, Werner RM (2013) Identifying hospital organizational strategies to reduce readmissions. Am J Med Qual 28:278–285. doi:10.1177/1062860612464999
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the prisma statement. J Clin Epidemiol 62:1006–1012. doi:10.1016/j.jclinepi.2009.06.005
Hu J, Chen R, Liu S, Yu X, Zou J, Ding X (2015) Global incidence and outcomes of adult patients with acute kidney injury after cardiac surgery: a systematic review and meta-analysis. J Cardiothorac Vasc Anesth 30:82–89. doi:10.1053/j.jvca.2015.06.017
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7:177–188
Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21:1539–1558. doi:10.1002/sim.1186
Strowd RE, Wise SM, Umesi UN, Bishop L, Craig J, Lefkowitz D, Reynolds PS, Tegeler C, Arnan M, Duncan PW, Bushnell CD (2015) Predictors of 30-day hospital readmission following ischemic and hemorrhagic stroke. Am J Med Qual 30:441–446. doi:10.1177/1062860614535838
Shah SV, Corado C, Bergman D, Curran Y, Bernstein RA, Naidech AM, Prabhakaran S (2015) Impact of poststroke medical complications on 30-day readmission rate. J Stroke Cerebrovasc Dis 24:1969–1977. doi:10.1016/j.jstrokecerebrovasdis.2015.04.037
Bjerkreim AT, Thomassen L, Waje-Andreassen U, Selvik HA, Naess H (2015) Hospital readmission after intracerebral hemorrhage. J Stroke Cerebrovasc Dis. doi:10.1016/j.jstrokecerebrovasdis.2015.09.009
Qian FMDP, Fonarow GCMD, Smith EEMDMPH et al (2013) Racial and ethnic differences in outcomes in older patients with acute ischemic stroke. Circ Cardiovasc Qual Outcomes 6:284–292. doi:10.1161/circoutcomes.113.000211
Olson DM, Cox M, Pan W, Sacco RL, Fonarow GC, Zorowitz R, Labresh KA, Schwamm LH, Williams L, Goldstein LB, Bushnell CD, Peterson ED (2013) Adherence evaluation of acute ischemic stroke-longitudinal AR death and rehospitalization after transient ischemic attack or acute ischemic stroke: 1-year outcomes from the adherence evaluation of acute ischemic stroke-longitudinal registry. J Stroke Cerebrovasc Dis 22:181–188
Li HW, Yang MC, Chung KP (2011) Predictors for readmission of acute ischemic stroke in taiwan. J Formos Med Assoc 110:627–633. doi:10.1016/j.jfma.2011.08.004
Lakshminarayan KMDP, Schissel CMPH, Anderson DCMD, Vazquez GP, Jacobs DRJP, Ezzeddine MMD, Luepker RVMDMS, Virnig BAPMPH (2011) Five-year rehospitalization outcomes in a cohort of patients with acute ischemic stroke: medicare linkage study. Stroke 42:1556–1562
Tseng MC, Lin HJ (2009) Readmission after hospitalization for stroke in taiwan: results from a national sample. J Neurol Sci 284:52–55. doi:10.1016/j.jns.2009.04.009
Bravata DMMD, Ho S-YP, Meehan TPMD, Brass LMMD, Concato JMD (2007) Readmission and death after hospitalization for acute ischemic stroke: 5-year follow-up in the medicare population. Stroke 38:1899–1904. doi:10.1161/strokeaha.106.481465
Smith MAa, Liou JIa, Frytak JRb, Finch MDc (2006) 30-day survival and rehospitalization for stroke patients according to physician specialty. Cerebrovasc Dis 22:21–26
Acknowledgments
The study was supported by no grant.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
All authors have no potential conflicts of interest for this work.
Rights and permissions
About this article

Cite this article
Zhong, W., Geng, N., Wang, P. et al. Prevalence, causes and risk factors of hospital readmissions after acute stroke and transient ischemic attack: a systematic review and meta-analysis. Neurol Sci 37, 1195–1202 (2016). https://doi.org/10.1007/s10072-016-2570-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-016-2570-5