
Abstract
Amyotrophic lateral sclerosis (ALS) is a progressive degenerative disease of upper and lower motor neurons. Sensory involvement is thought not to be a feature of ALS. We reviewed 17 cases of sural nerve biopsies performed in a large cohort of ALS patients referred to our centre over a 23-year period. More than two-third of biopsies revealed a variable degree of axonal loss. In one case, pathological findings suggested the concomitant presence of an inherited neuropathy, subsequently confirmed by genetic evaluation. In another case, pathological and neurographic data were similar to those of an inflammatory demyelinating neuropathy, but the clinical course corroborated the diagnosis of ALS. Our data confirm that sensory nerve involvement may be found in ALS patients. This finding should prompt physicians to carefully investigate a possible alternative diagnosis, but does not exclude the possibility that the patient may have ALS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Amyotrophic Lateral Sclerosis (ALS) is a progressive degenerative disease characterized by relentless degeneration of both upper and lower motor neurons, leading to progressive muscular paralysis, with death usually occurring 1–5 years after clinical onset [1]. Normal electrophysiological studies on sensory nerves are generally required for the diagnosis of ALS [2]. Nevertheless, several neurological, clinical neurophysiological and neuropathological studies suggested that ALS is a more generalized neurodegenerative disorder [3–6]. In addition, patients with ALS often complain of sensory symptoms, and objective sensory signs were detected in 2–10% of patients in a multicentre case series [7]. On the other hand, peripheral sensory neuropathy has not been widely recognised as part of the ALS syndrome. Consequently, the occasional presence of sensory features in ALS has long been a cause of diagnostic uncertainty [8, 9].
In this report we describe pathological findings from sural nerve biopsy from 17 cases of our cohort of ALS patients.
Patients and methods
Among more than 700 cases referred to our centre from 1987 to 2010, 17 ALS patients underwent sural nerve biopsy [10], either because of clinical or neurophysiological signs suggesting sensory involvement or because patients presented with an atypical form of ALS (upper motor neuron dominant-ALS with or without young-adult onset, Flail Arm syndrome or Progressive Muscular Atrophy). Patients underwent extensive laboratory studies to rule out possible causes of neuropathy, including fasting plasma glucose, glycosylated haemoglobin, fT3, fT4, TSH, anti-thyroid antibodies, serum vitamin B12 and folates, hepatic enzymes, creatinine, urinalysis, antinuclear antibodies (ANA), anti-extractible nuclear antigens, anti-DNA antibodies, antineutrophil cytoplasmic antibodies (ANCA), circulating C3 and C4, immunofixation electrophoresis and serologic tests for HBV, HCV and HIV. Clinical phenotypes were established on the basis of clinical features observed in the fully developed state, independently from the presenting symptoms [10]. Electromyographic examination and nerve conduction studies in upper and lower limbs were performed in all patients. All cases were screened for SOD1, TARDP and FUS mutations. Archived sural nerve biopsy specimens were investigated. Sural nerve biopsy was performed under local anaesthesia following informed consent and standardized procedures [11]. Nerve specimens were reanalysed that had been processed for standard morphology as follows: 6 μm frozen sections stained with haematoxylin-eosin (H&E) and 1 μm semithin plastic sections stained with toluidine blue.
Results
All patients with ALS met El-Escorial diagnostic criteria for definite or probable ALS [2]. Extensive laboratories studies proved normal in all cases. Clinical phenotype was defined according to the previous studies [10]. Clinical, demographic, morphologic and neurographic findings are summarized in Table 1.
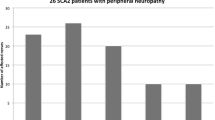
On sural nerve biopsy, five patients (29%) revealed normal findings, while in the remaining patients axonal loss was mild in seven (41%), moderate in four (24%) and marked in one (6%).
Regenerating clusters were observed in nine biopsies (53%); Wallerian degenerations were noted in six cases (35%).
In two cases electrophysiological studies revealed a slowed nerve conduction velocity in all nerves tested. In one of these cases sural nerve biopsy showed mild axonal loss with tomacula-like myelin thickenings (Fig. 1 a–c). Analysis for a microdeletion of the PMP22-containing region confirmed the presence of a hereditary neuropathy with liability to pressure palsy (HNPP). In the other case, sural nerve biopsy revealed moderate axonal loss and an inflammatory infiltrate around an epineural vessel (Fig. 2 a–b). Teased fibre analysis showed widespread segmental de-remyelination. We tried to characterize the inflammatory infiltrate with immunohistochemistry using antibodies against human B cells (CD20), helper/inducer T cells (CD4), suppressor/cytotoxic T cells (CD8) and macrophages (CD68), but we could not find in any section other than the one we show.

Sural nerve biopsy from the patient with ALS and HNPP. a Light microscopy. Transverse semithin sections stained with toluidine blue. This fascicle shows a mild reduction of myelinated fibres; occasional tomacula-like thickenings of myelin sheath are clearly visible (insert in b). c Teased fibres examination confirms the presence of tomacula

Sural nerve biopsy in a patient with ALS. a Haematoxylin-eosin (H&E) staining shows an epineurial perivascular cellular infiltrate. b Transverse semithin sections stained with toluidine blue. This fascicle shows a moderate reduction of myelinated fibres without active degenerations
Morphometric evaluation and pathological results are summarized in Table 2.
All patients underwent genetic evaluation, which in one case revealed the SOD1 p.L144F mutation and in another one the TDP43 p.A382T mutation.
Discussion
We describe pathological findings from 17 sural nerve biopsies from a large cohort of ALS patients.
In a previous paper, more than 90% of patients who underwent sural nerve biopsy showed pathologic evidence of sensory nerve pathology [3]. Furthermore a recent article indicates that small, distal epidermal nerve fibres are involved in ALS too [12].
Our study confirms that sural nerve biopsy revealed in 70% of cases an involvement of sensory fibres in patients with motor neuron disease.
Interestingly, in two of our patients electrophysiological studies were also misleading, revealing slowed nerve conduction velocity resembling a chronic inflammatory demyelinating neuropathy (CIDP) [13]. In one of these cases pathological examination of the sural nerve showed the presence of tomacula, suggesting the possible concomitance of a HNPP. The patient reported no sensory disturbance and had no history of compressive neuropathies. FISH (fluorescence in situ hybridization) analysis revealed a microdeletion of the PMP22-containing region, confirming the diagnosis of HNPP. The association of HNPP with ALS had been reported previously in three unrelated patients [14–16].
In the other case sural nerve biopsy showed an inflammatory infiltrate. In a recent paper, Devigili et al. [17] retrospectively analysed sural nerve pathology and clinical course of 18 patients with ALS and found in 11 cases the presence of inflammatory cell infiltrates on sural nerve biopsy resembling those seen in patients with vasculitic neuropathy; however, our patient did not satisfy diagnostic criteria for a definite pathological diagnosis of vasculitic neuropathy [18]. Furthermore a CIDP-like presentation has been reported in ALS patients [19]. Pathological and neurophysiological findings in our case were similar to those previously described and, as in the previous cases, in our patient too immunosuppressive treatment did not prevent clinical progression of the motor neuron disease.
Genetic evaluation revealed in one case the TDP43 p.A382T mutation. Interestingly this patient presented a mild axonal loss on sural nerve biopsy. The association of this TDP43 mutation with peripheral neuropathy has been previously reported [20].
This study provides further demonstration of sensory nerve involvement in patients affected with ALS and confirms previous evidence that ALS is not confined to motor neurons, but may also affect sensory neurons and their axonal projections [3, 7–9, 12].
In conclusion, we confirm that the diagnosis of ALS cannot be excluded on the basis of pathological sural nerve findings and that inflammatory infiltrates may be found in a subset of nerve biopsies from ALS patients. However, an alternative diagnosis should be carefully investigated in patients with ALS and sensory neuropathy.
References
Haverkamp LJ, Appel V, Appel SH (1995) Natural history of amyotrophic lateral sclerosis in a database population. Validation of a scoring system and a model for survival prediction. Brain 118:707–719
Brooks BR, Miller RG, Swash M, Munsat TL, World Federation of Neurology Research Group on Motor Neuron Diseases (2000) El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord 1:293–299
Hammad M, Silva A, Glass J, Sladky JT, Benatar M (2007) Clinical, electrophysiologic, and pathologic evidence for sensory abnormalities in ALS. Neurology 69:2236–2242
Oey PL, Vos PE, Wieneke GH, Wokke JH, Blankestijn PJ, Karemaker JM (2002) Subtle involvement of the sympathetic nervous system in amyotrophic lateral sclerosis. Muscle Nerve 25:402–408
Desai J, Swash M (1999) Extrapyramidal involvement in amyotrophic lateral sclerosis: backward falls, retropulsion. J Neurol Neurosurg Psychiatry 67:214–216
Lloyd CM, Richardson MP, Brooks DJ, Al-Chalabi A, Leigh PN (2000) Extramotor involvement in ALS: PET studies with the GABA(A) ligand [(11)C]flumazenil. Brain 23:2289–2296
Pugdahl K, Fuglsang-Frederiksen A, de Carvalho M, Johnsen B, Fawcett PR, Labarre-Vila A, Liguori R, Nix WA, Schofield IS (2007) Generalised sensory system abnormalities in amyotrophic lateral sclerosis: a European multicentre study. J Neurol Neurosurg Psychiatry 78:746–749
Isaacs JD, Dean AF, Shaw CE, Al-Chalabi A, Mills KR, Leigh PN (2007) Amyotrophic lateral sclerosis with sensory neuropathy: part of a multisystem disorder? J Neurol Neurosurg Psychiatry 78:750–753
Wechsler IS, Brock S, Weil A (1929) Amyotrophic lateral sclerosis with objective and subjective (neuritic) sensory disturbances A clinical and pathologic report. Arch Neurol Psychiatry (Chic) 21:299–310
Sabatelli M, Zollino M, Luigetti M, Del Grande A, Lattante S, Marangi G, Lo Monaco M, Madia F, Meleo E, Bisogni G, Conte A (2011) Uncovering ALS phenotypes: clinical features and long-term follow-up of UMN-D ALS. Amyotroph Lateral Scler 12:278–282
Sommer CL, Brandner S, Dyck PJ, Harati Y, LaCroix C, Lammens M, Magy L, Mellgren SI, Morbin M, Navarro C, Powell HC, Schenone AE, Tan E, Urtizberea A, Weis J, Society Peripheral Nerve (2010) Peripheral Nerve Society Guideline on processing and evaluation of nerve biopsies. J Peripher Nerv Syst 15:164–175
Weis J, Katona I, Müller-Newen G, Sommer C, Necula G, Hendrich C, Ludolph AC, Sperfeld AD (2011) Small-fiber neuropathy in patients with ALS. Neurology 76: 2024–2029
Joint Task Force of the EFNS, the PNS. European Federation of Neurological Societies/Peripheral Nerve Society (2010) Guideline on management of chronic inflammatory demyelinating polyradiculoneuropathy: report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society—First Revision. J Peripher Nerv Syst 15:1–9
O’Sullivan SS, McCarthy A, Mullins GM, McNamara B, Sweeney BJ (2006) ALS in a patient with hereditary neuropathy with liability to pressure palsy. Neurology 67:2260
Canali E, Chiari A, Sola P, Fioravanti V, Valzania F, Pentore R, Nichelli P, Mandrioli J (2010) Rapidly progressive amyotrophic lateral sclerosis in a young patient with hereditary neuropathy with liability to pressure palsies. Amyotroph Lateral Scler 11:335–336
Bhatt A, Farooq MU, Aburashed R, Kassab MY, Majid A, Bhatt S, Naravetla B, Dhaliwal G (2008) Hereditary neuropathy with liability to pressure palsies and amyotrophic lateral sclerosis. Neurol Sci 30:241–245
Devigili G, Uçeyler N, Beck M, Reiners K, Stoll G, Toyka KV, Sommer C (2011) Vasculitis-like neuropathy in amyotrophic lateral sclerosis unresponsive to treatment. Acta Neuropathol 122:343–352
Collins MP, Dyck PJ, Gronseth GS, Guillevin L, Hadden RD, Heuss D, Léger JM, Notermans NC, Pollard JD, Said G, Sobue G, Vrancken AF, Kissel JT, Society Peripheral Nerve (2010) Peripheral Nerve Society Guideline on the classification, diagnosis, investigation, and immunosuppressive therapy of non-systemic vasculitic neuropathy: executive summary. J Peripher Nerv Syst 1:176–184
Rajabally YA, Jacob S (2008) Chronic inflammatory demyelinating polyneuropathy-like disorder associated with amyotrophic lateral sclerosis. Muscle Nerve 38:855–860
Camdessanché JP, Belzil VV, Jousserand G, Rouleau GA, Créac’h C, Convers P, Antoine JC (2011) Sensory and motor neuronopathy in a patient with the A382P TDP-43 mutation. Orphanet J Rare Dis 6:4
Conflicts of Interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Luigetti, M., Conte, A., Del Grande, A. et al. Sural nerve pathology in ALS patients: a single-centre experience. Neurol Sci 33, 1095–1099 (2012). https://doi.org/10.1007/s10072-011-0909-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-011-0909-5