
Abstract
The aims of this article were to assess the methodological challenges of randomized controlled trials (RCTs) on cognitive interventions for people with multiple sclerosis, and to discuss specific problems related to rehabilitation trials. A bibliographic search was carried out. Selected articles were examined using five methodological quality criteria related to description of the target population, method of allocation, masking of patient and examiner, the outcome measures and analysis. A total of 12 RCTs, published between 1996 and 2010, were found. Five RCTs were on drug therapy (two on disease-modifying therapies, one on donepezil and two on drugs for fatigue). Seven RCTs were on rehabilitation (six on PC-based retraining techniques). The quality of the studies was overall low, inadequate selection of the target population and limited study size being the most frequent limitations. No clear improvement was found in the most recent studies. Additional methodological problems specific to rehabilitation trials are difficulties in defining and reproducing the study intervention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cognitive impairment is a common manifestation of multiple sclerosis (MS), affecting 40–65% of patients irrespective of disease subtype. Cognitive compromise can be present early in the course of the disease and impacts patient’s fulfillment of role in the family, social and work life. Over the last two decades, interventions for cognitive compromise in MS have been published.
This study examines the methodological challenges of randomized controlled trials (RCTs) on cognitive symptoms in MS and discusses specific problems related to rehabilitation trials. Clinical aspects of these interventions are discussed in other articles of this issue.
A search of the following databases was carried out in March 2010: Medline (Pubmed), embase, cinahl, psycINFO, Cochrane Collaboration’s trial register, and Database of Reviews of Effectiveness (DARE). The following five methodological criteria were considered [1]: the target population (eligibility criteria stated; baseline comparability); allocation (random and concealed); masking (subjects and assessors); outcomes (explicit primary outcome stated; sample size calculation reported; adequate follow-up); and analysis (intention to treat; between-group comparisons). Furthermore, description of the intervention in nonpharmacological trials was considered.
Results
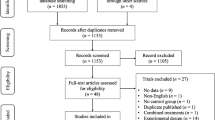
A total of 12 RCTs, published between 1996 and 2010, were found. Of these, five were on pharmacological interventions (three symptomatic treatments and two disease-modifying) (Table 1), while seven were on rehabilitation (one on compensatory strategy [7] and six on PC-based retraining [8–12]) (Table 2).
The target population
Eligibility criteria depended on the type of intervention. For disease-modifying drugs, trials should target cognitively preserved MS patients and follow them for a sufficient time to assess the treatment effects on prevention of cognitive compromise. The two published RCTs on disease-modifying treatment provide exploratory data on RCTs designed for different primary outcomes [2, 3]. In the interferon β 1a trial, patients’ cognitive functioning at baseline was quite heterogeneous [3]. In the glatiramer acetate trial, baseline neuropsychological assessment was within the normal range and remained stable in both arms during the 2-year follow-up. Trials on symptomatic drugs [4–6] and those on rehabilitation [7–13] included mildly to severely compromised patients, mostly on the basis of neuropsychological assessment. In all the RCTs considered, eligibility criteria were specified and, despite the limited size of most of these studies, comparability at baseline was fine in all but one instance [6].
Allocation
Three of the included studies (25%) had a randomization method that was considered inadequate (alternate assignment) [11, 12] or not reported [5, 9, 13]. Concealed allocation was not specified in two pharmacological (40%) [4, 5] and three rehabilitation studies (43%) [8, 12, 13].
Concealment
Four drug trials (80%) and two rehabilitation trials (29%) [10, 11] were double-blind studies [2–4, 6]. It should be noted that having the patient blind is often unfeasible in rehabilitation trials; however, a sham intervention or a low-intensity intervention can be conceived for PC-based retraining, allowing patient’s masking [10, 11].
Outcomes
Only one drug trial (20%) [6] and one rehabilitation trial (14%) [10] specified the primary outcome measure and provided the sample size justification. A practice effect was almost universally reported. The length of follow-up depends on the chosen study population, the main study outcomes, as well as the type and predicted efficacy of the study intervention. It was considered to be adequate in three drug trials (60%) [2, 3, 6] and five rehabilitation trials (71%) [7–11].
Analysis
All the published studies correctly performed between-arm comparisons, but intention to treat analysis was conducted only in two drug trials (40%) [2, 6] and three rehabilitation trials (43%) [8, 10, 12]. Considering the interferon β 1a trial [3], attrition was very high, exceeding 40%.
Description of the intervention in rehabilitation trials
The CONSORT statement on reporting clinical trials recommends that “precise details of the interventions intended for each group and how and when they were actually administered” should always be reported [14]. Adherence to this recommendation is particularly important for RCTs on rehabilitation interventions: full description of the specific rehabilitation technique or theory on which the intervention is based, the setting, intensity, duration of the retraining program, and the required experience and training of the therapist is essential to document the intervention, and make it understandable and replicable. Another reason why rehabilitation interventions should be described in detail is that their potential value can only then be appreciated. It must be clear whether the trial is pragmatic (focussing on measuring benefit of the intervention when introduced into current clinical practice) or primarily exploratory (aiming to measure benefit under ideal conditions or determine which component of the intervention is efficacious). In drug RCTs, the experimental intervention is compared to placebo or an established drug. The comparator in rehabilitation RCTs is much more problematic. An adequate sham intervention can be devised only in selected cases. Waiting list patients are not a good solution, since the patients know they are receiving/not receiving the intervention, and this can result in bias. A more acceptable option is to use a low-intensity intervention as comparator, although this is likely to reduce the study power and require recruitment of more patients. In view of these issues, the CONSORT Group recently developed an extension of the CONSORT statement for nonpharmacological treatments [15]. Furthermore, the Medical Research Council has produced guidance on how to develop and evaluate such interventions (Fig. 1) [16, 17].

Phases in the development of a clinical trial involving a complex intervention (adapted from the UK Medical Research Council framework for the development and evaluation of complex interventions by RCT) [16]
Conclusions
The methodological quality of an RCT has been defined as the likelihood of the trial design generating unbiased results that are sufficiently precise and allow application in clinical practice [1]. Evidence for the effectiveness of interventions to help cognitively compromised MS people is scarce. Twelve RCTs [2–13] have been published since 1993 and their quality is overall insufficient. Pitfalls of RCTs on interventions for cognitive compromise in MS include difficulty in choosing the appropriate study population and outcome measure, and a limited study size. It is also noteworthy that the most recent trials are not of high quality. Other problems are specific to rehabilitation studies and arise because: these interventions are multifaceted, complex, and difficult to define and quantify; the training and skills of clinicians administering the intervention can vary; and patient blinding is difficult and often impossible. Furthermore, the resources necessary to conduct rehabilitation trials according to good clinical practice and high quality standards are generally lacking. The recently updated CONSORT statement and MRC guideline should improve clarity, completeness and transparency of reporting trial findings; moreover, they should help researchers in designing and conducting future studies [14–17].
References
Verhagen AP, de-Vet HCW, de-Bie RA et al (1998) The Delphi list: a criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. J Clin Epidemiol 51:1235–1241
Weinstein A, Schwid SIL, Schiffer RB et al (1999) Neuropsychologic status in multiple sclerosis after treatment with glatiramer. Arch Neurol 56:319–324
Fischer JS, Priore RL, Jacobs LD et al (2000) Neuropsychological effects of interferon B-1a in relapsing multiple sclerosis. Ann Neurol 48:885–892
Smits RC, Emmen HH, Bertlesmann FW et al (1994) The effects of 4-aminopyridine on cognitive function in patients with multiple sclerosis. Neurology 44:1701–1705
Geisler MW, Sliwinski M, Coyle PK et al (1996) The effects of amantadine and pemoline on cognitive functioning in multiple sclerosis. Arch Neurol 53:185–188
Krupp LB, Christdoulou C, Melville RN et al (2004) Donepezil improved memory in multiple sclerosis in a randomized controlled trial. Neurology 63:1579–1585
Jønsson A, Korfitzen EM, Heltberg A et al (1993) Effect of neuropsychological treatment in patients with multiple sclerosis. Acta Neurol Scand 88:394–400
Mendozzi L, Pugnetti L, Motta A et al (1998) Computer-assisted memory retraining of patients with multiple sclerosis. Neurol Sci 19:S431–S438
Lincoln NB, Dent A, Harding J et al (2002) Evaluation of cognitive assessment and cognitive intervention for people with multiple sclerosis. J Neurol Neurosurg Psychiatry 72:93–98
Solari A, Motta A, Mendozzi L et al (2004) Computer-aided retraining of memory and attention in people with multiple sclerosis: a randomized, double-blind controlled trial. J Neurol Sci 222:99–104
Chiaravalloti ND, DeLuca J, Moore NB, Ricker JH (2005) Treating learning impairments improves memory performance in multiple sclerosis: a randomized clinical trial. Mult Scler 11:58–68
Hildebrandt H, Lanz M, Hahn HK et al (2007) Cognitive training in MS: effects and relation to brain atrophy. Restor Neurol Neurosci 25:33–43
Mattioli F, Stampatori C, Zanotti D et al (2010) Efficacy and specificity of intensive cognitive rehabilitation of attention and executive functions in multiple sclerosis. J Neurol Sci 288:101–105
Kenneth F, Schulz KF, Altman DG, Moher D, for the CONSORT Group (2010) CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. BMJ 340:c332
Boutron I, Moher D, Altman DG, Schulz KF, Ravaud P, for the CONSORT Group (2008) Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: explanation and elaboration. Ann Intern Med 148:295–309
Medical Research Council (2000) A framework for development and evaluation of RCTs for complex interventions to improve health. Medical Research Council, London
Medical Research Council (2008) Developing and evaluating complex interventions: new guidance. Medical Research Council, London
Conflict of interest statement
The author declares that she has no conflict of interests related to the publication of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Solari, A. Methodological aspects of randomized controlled trials on cognitive interventions. Neurol Sci 31 (Suppl 2), 279–282 (2010). https://doi.org/10.1007/s10072-010-0375-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-010-0375-5