
Abstract
Objective
A growing body of research examining the effect of exercise on cognitive function in people with multiple sclerosis (MS), while findings of available studies were conflicting. We aimed to explore the effect of exercise on cognitive function in MS patients.
Methods
For this systematic review and meta-analysis, we searched PubMed, Web of Science, EBSCO, Cochrane, and Scopus electronic databases, through July 18, 2022. Cochrane risk assessment tool was used to evaluate the methodological quality of the included literature.
Results
Twenty-one studies with a total of 23 experimental groups and 21 control groups met the inclusion criteria. There was a significant effect of exercise on improving cognitive function in MS patients, while the effect size was small (Cohen's d = 0.20, 95% CI 0.06–0.34, p < 0.001, I2 = 39.31%). Subgroup analysis showed that exercise significantly improved memory (Cohen's d = 0.17, 95% CI 0.02–0.33, p = 0.03, I2 = 7.59%). In addition, multicomponent training, exercise conducted 8 weeks and 10 weeks, up to 60 min per session, 3 times or more per week, 180 min or more per week increased cognitive function significantly. Furthermore, a worse basal MS status (defined by the Expanded Disability Status Scale) and an older age were associated with greater improvement in cognitive function.
Conclusion
MS patients are recommended to participate in at least three multicomponent training sessions per week, with each session lasting up to 60 min, and the exercise goal of 180 min per week can be achieved by increasing the frequency of exercise. Exercise lasting 8 or 10 weeks is best for cognitive function improvement. Additionally, a worse basal MS status, or the older the age, the greater effect on cognitive function.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Multiple sclerosis (MS) is a chronic autoimmune disease with both inflammatory and degenerative components [1], characterized by focal lymphocytic central nervous system (CNS) infiltration leading to inflammatory demyelination, astroglial proliferation, and axonal degeneration, resulting in neurologic syndromes and physical disability [2, 3]. Previous studies have shown that cognitive impairment is a common and disabling feature of MS and may occur in the early stages of MS even in the absence of other neurological deficits [4, 5].
MS patients often suffer from muscle weakness, walking abnormalities, poor balance, and fatigue [6, 7], so for many years, physicians have advised MS patients to avoid physical exercise. However, in recent years, appropriate exercise has been found to be beneficial for MS improvements such as aerobic capacity, muscle strength, flexibility, balance, fatigue levels, and cognitive function [8]. Furthermore, exercise is considered an effective non-pharmacological intervention to improve and delay MS symptoms, but little is known about the effects of exercise on cognitive dysfunction in MS patients.
A growing body of research examining the effect of exercise on cognitive function in MS patients, while findings of available studies were conflicting. Ozkul et al. [9] found beneficial effects of combination of aerobic and Pilates exercise in improving MS patients with cognitive impairment and a correlation between improvements in cognition, mood, and quality of life after exercise. In addition, Sandroff et al. [10,11,12] showed that exercise is a promising tool for improving cognitive function in MS patients. However, Savšek et al. [13] showed that aerobic exercise had a weak improvement in walking speed, brain-derived neurotrophic factor levels, but no improvement cognitive function in MS patients. In addition, Langeskov-Christensen et al. [14] found that 24 weeks of supervised progressive aerobic exercise had no effect on cognitive function in MS patients. Moreover, Ozkul et al. [15] found that exercise was more effective in improving balance and walking ability in MS patients, but no significant improvement in cognitive function was found. Furthermore, Kooshiar et al. [16] showed that aquatic exercise was effective in improving quality of life and reducing fatigue, but not in improving cognitive function in MS patients.
Therefore, we conducted a comprehensive systematic review and meta-analysis of randomized controlled trials (RCTs) to investigate the effects of exercise on cognitive function in MS patients, with the ultimate goal of this study being to determine whether there is sufficient evidence to support that exercise interventions can improve cognitive function in MS patients.
Methods
Cochrane Selection Manual [17] and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA, 2020) guidelines [18] were followed for conducting this systematic review and meta-analysis. The protocol was registered on PROSPERO (CRD42022379251).
Search strategy
For this study, we searched PubMed, Web of Science, EBSCO, Cochrane, and Scopus databases, through July 18, 2022. All studies on exercise and cognitive function in MS patients were searched using the following MESH terms and keywords: exercise, multiple sclerosis, and cognitive function. We also hand-searched the reference lists of all identified studies and, in addition, references of reviews and meta-analyses for any additional relevant studies that could be added to the relevant literature. Two authors (GL and QY) completed the process independently using a standard format. If there was disagreement between the two authors, a third author (LY) would join the discussion until the three reach a consensus.
Eligibility criteria
Inclusion criteria were as follows: eligible studies should (1) be RCTs; (2) include an intervention group and a control group; (3) use MS patients as subjects; and (4) include outcome indicators of cognitive function. Non-English publications, animal model publications, review, conference articles or full-text analyses with a high risk of bias were excluded.
Data extraction
Two authors (GL and QY) independently performed the data extraction, mainly including: (a) characteristics of included studies (first author's last name, year of study publication, sample size); (b) intervention features (intervention type, duration of intervention, frequency, session duration); (c) participant characteristics [age, type of disease, Expanded Disability Status Scale (EDSS)]; and (d) treatment effects [mean and standard deviation (SD) values reflecting changes in cognitive function from baseline to post-intervention].
Methodological quality assessment
We assessed the methodological quality of included studies using the Cochrane risk of bias criteria, which included 7 items: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), and outcome-blind assessment (detection bias), incomplete result data (loss bias), selective reporting (report bias), and other biases [19, 20]. Based on the responses to the signaling questions, each item was judged as "low risk", "uncertain risk" or "high risk" to make an overall judgement of bias for the study being assessed [17]. Two reviewers (GL and QY) independently performed methodological quality assessments. If there was disagreement between the two authors, a third author (LY) would join the discussion until the three reach a consensus.
Statistical analysis
As the included studies tended to report multiple cognitive outcomes, we cannot assume that the results of each study are independent and estimate the same results, statistical analyses were based on a three-level restricted maximum likelihood random effects model, using the metafor for R package [21]. Using the computational approach described in the study by Assink et al. [22]. The model illustrates the dependence of within-study effect sizes by providing within-study (level 2) and between-study (level 3) variance estimates. The primary outcome indicator included in this study was expressed as "mean ± SD", using Cohen's d to standardize the difference in change from baseline to post-intervention between the exercise and control groups. A positive Cohen's d indicates an increase in cognitive performance in the exercise group compared to the control group. Total effect size values were assessed according to the Cohen's d classification (d = 0.2–0.5, small; d = 0.5–0.8, medium; d = 0.8, large) [17]. Heterogeneity was assessed by I2 static. I2 < 25% indicates no significant heterogeneity; 25% < I2 < 50%, low heterogeneity; 50% < I2 < 75%, medium heterogeneity; I2 > 75%, high heterogeneity [23, 24].
In subgroup analyses, we tried to investigate the effect of exercise on cognitive function in MS patients using cognitive function type [executive function (EF), memory, and cognitive speed] [25, 26], intervention type [aerobic exercise, resistance exercise, and multicomponent training (a training modality that involves different physical capacities in the same exercise session)], minutes of intervention per session (up to 60 min per session and more than 60 min per session), frequency of intervention per week (less than 3 times per week and 3 times or more per week), duration of intervention (6 weeks, 8 weeks, 10 weeks, 12 weeks, and 24 weeks), minutes of intervention per week (less than 180 min per week and 180 min or more per week), participants' age (less than 45 years old and 45 years old or more), and basal MS status (0 < EDSS ≤ 3.5, mild; EDSS > 3.5, moderate to severe) [27]. All analyses were performed using R4.2.2 (R Foundation for Statistical Computing, Vienna, Austria) [28].
Results
Study selection
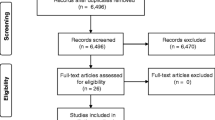
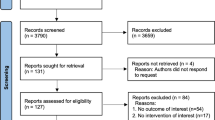
As shown in Fig. 1, a total of 1853 articles were initially retrieved from the databases and 4 records from other sources. After excluding the duplicates, 1153 studies were remaining, and 1105 studies were not eligible for inclusion through the title and abstract screening. Twenty-seven studies were excluded by reading the full text of 48 studies: (1) the experimental group combined with other treatments (n = 1); (2) no control group (n = 1); (3) the data could not be extracted (n = 9); (4) duplicate article (n = 1); (5) non-English article (n = 1); and (6) experimental design articles (n = 14). Finally, 21 studies [9, 11, 13, 14, 16, 27, 29,30,31,32,33,34,35,36,37,38,39,40,41,42,43] examining the effect of exercise on cognitive function in people with MS were considered eligible for systematic review and meta-analysis.

PRISMA flowchart of study selection
Study characteristics
The main characteristics of participants and interventions are shown in Table 1. The included studies involved 580 participants in 23 exercise groups and 507 participants in 21 control groups. Of the 21 studies, 3 studies [16, 27, 30] involved only women, 1 study [41] did not report the gender of participants, and 17 studies [9, 11, 13, 14, 29, 31,32,33,34,35,36,37,38,39,40, 42, 43] involved both men and women. The most common MS phenotype was the relapsing–remitting (n = 8) [9, 13, 14, 27, 30, 36, 37, 41], but it was usually mixed with other phenotypes [11, 16, 31, 39, 40, 42], and 7 studies [29, 32,33,34,35, 38, 43] did not report the MS phenotype. The mean age of the participants ranged from 29.24 to 64.3 years. Twelve studies [9, 13, 16, 27, 30, 31, 34, 36, 37, 39, 41, 43] involved participants with mean age < 45 years, and 9 studies [11, 14, 29, 32, 33, 35, 38, 40, 42] involved participants with mean age ≥ 45 years. Seven studies [27, 29, 33, 35, 38, 40, 42] included participants with a mean EDSS > 3.5, 12 studies [9, 13, 14, 16, 30,31,32, 36, 37, 39, 41, 43] included participants with a mean 0 < EDSS ≤ 3.5, and 2 studies [11, 34] did not report EDSS. Most interventions specified aerobic exercise (n = 10) [11, 13, 14, 30, 32, 34, 37, 38, 40, 42], resistance exercise alone (n = 2) [39, 41], or combined (n = 8) [9, 16, 27, 29, 31, 35, 36, 43]. The total duration of the intervention ranged from 6 to 24 weeks and minutes of intervention per session ranged from 20 to 90 min. However, descriptions of minutes of intervention per session were lacking or missing in 5 studies [11, 33, 34, 39, 43]. The frequency of intervention per week ranged from 1 to 7 times, and 1 study [11] did not report the frequency of intervention per week. Because the frequency and duration of the interventions varied in each study, we calculated the minutes of intervention per week based on the minutes of intervention per session and frequency in the included studies. The minutes of intervention per week ranged from 45 to 180 min.
Risk of bias
The quality of the included studies was evaluated using the Cochrane risk assessment tool according to the following 6 aspects: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other biases. As shown in Fig. 2, we classified included studies as low, moderate, or high quality based on the following criteria: (1) a trial was considered low quality if randomization or allocation concealment was assessed as high risk of bias, regardless of the risk of other items; (2) a trial was considered high quality if randomization and allocation concealment were assessed as low risk of bias, and all other items were assessed as low or unclear risk of bias; and (3) a trial was considered moderate quality if it did not meet the high or low risk criteria [44]. The publication bias for included studies was assessed visually by examining the funnel plot (Fig. 3).

Results of Cochrane risk of bias tool. Above: Risk of bias summary: review authors' judgments about each risk of bias item for each included study. Below: Risk of bias graph: review authors' judgments about each risk of bias item presented as percentages across all included studies

Funnel plot
Meta-analysis results
Effects of exercise on cognitive function in MS patients
Overall, 21 studies reported 83 effect sizes for meta-analysis. We found a significant effect of exercise on improving cognitive function in MS patients, while the effect size was small [Cohen's d = 0.20, 95% confidence interval (CI), 0.06–0.34, p < 0.01, Table 2 and supplementary Fig. 1], and there was no significant heterogeneity (I2 = 39.31%).
Subgroup analysis
Of the 21 studies [9, 11, 13, 14, 16, 27, 29,30,31,32,33,34,35,36,37,38,39,40,41,42,43], 7 studies [9, 13, 14, 31, 34, 37, 42] provided data for memory, 15 studies [9, 11, 13, 14, 29,30,31, 34,35,36,37, 40,41,42,43] provided data for cognitive speed, and 7 studies [9, 14, 30, 32, 34, 37, 40] provided data for EF. As shown in Table 2, different results were shown when considering cognitive function type. Specifically, exercise significantly improved memory (Cohen's d = 0.17, 95% CI 0.02–0.33, p = 0.03, I2 = 7.59%) in MS patients. However, exercise had no significant effect on improving cognitive speed (Cohen's d = 0.07, 95% CI − 0.07 to 0.21, p = 0.29, I2 = 6.07%), and EF (Cohen's d = 0.09, 95% CI − 0.01 to 0.28, p = 0.39, I2 = 1.71%) in MS patients.
Ten studies [11, 13, 14, 30, 32, 34, 37, 38, 40, 42] provided data for aerobic exercise, 2 studies [39, 41] provided data for resistance exercise, and 8 studies [9, 16, 27, 29, 31, 35, 36, 43] provided data for multicomponent training. Subgroup analyses showed that multicomponent training significantly improved cognitive function (Cohen's d = 0.32, 95% CI 0.22–0.43, p < 0.01, I2 = 2.22%). However, aerobic exercise (Cohen's d = 0.03, 95% CI − 0.05 to 0.10, p = 0.5, I2 = 0%) and resistance exercise (Cohen's d = 0.43, 95% CI − 0.20 to 1.06, p = 0.18, I2 = 11.55%) had no significant associations with cognitive function in MS patients. Subgroup analysis indicated that multicomponent interventions were more effective in improving cognitive function.
Two studies [35, 36] conducted the intervention for 6 weeks, 4 studies [9, 16, 27, 31] conducted the intervention for 8 weeks, 1 study [39] conducted the intervention for 10 weeks, 8 studies [13, 30, 33, 34, 37, 38, 40, 42] conducted the intervention for 12 weeks, and 6 studies [11, 14, 29, 32, 41, 43] conducted the intervention for 24 weeks. Specifically, 8 weeks (Cohen's d = 0.50, 95% CI 0.31 to 0.70, p < 0.01, I2 = 1.60%) and 10 weeks (Cohen's d = 2.23, 95% CI 1.71–3.19, p < 0.01) of exercise significantly improved cognitive function. However, 6 weeks (Cohen's d = 0.29, 95% CI − 0.45 to 1.02, p = 0.44), 12 weeks (Cohen's d = 0.06, 95% CI − 0.05 to 0.18, p = 0.25, I2 = 2.31%), and 24 weeks (Cohen's d = 0.09, 95% CI − 0.05 to 0.23, p = 0.21, I2 = 2.85%) of exercise had no significant associations with cognitive function in MS patients.
Fourteen studies [13, 14, 16, 27, 29,30,31, 35,36,37,38, 40,41,42] conducted the intervention for up to 60 min per session and 2 studies [9, 32] conducted the intervention for more than 60 min per session. Interventions conducted up to 60 min per session significantly improved cognitive function (Cohen's d = 0.18, 95% CI 0.00–0.36, p = 0.05, I2 = 29.98%). However, interventions conducted more than 60 min per session had no significant associations with cognitive function in MS patients (Cohen's d = 0.03, 95% CI − 0.36 to 0.75, p = 0.07, I2 = 2.61%).
The frequency of interventions in 13 studies [9, 13, 16, 27, 30, 33,34,35,36, 38,39,40, 43] was 3 times or more per week and the frequency of interventions in 5 studies [13, 14, 31, 32, 41] was less than 3 times per week. Interventions conducted 3 times or more per week significantly improved cognitive function (Cohen's d = 0.34, 95% CI 0.10–0.59, p < 0.01, I2 = 5.73%). However, interventions conducted less than 3 times per week had no significant associations with cognitive function in MS patients (Cohen's d = 0.04, 95% CI − 0.28 to 0.35, p = 0.82, I2 = 27.56%).
Regarding minutes of intervention per week, 4 studies [9, 29, 32, 35] provided data for 180 min or more per week and 7 studies [13, 14, 16, 30, 31, 38, 40] provided data for less than 180 min per week. Interventions conducted 180 min or more per week significantly improved cognitive function (Cohen's d = 0.27, 95% CI 0.06–0.48, p = 0.01, I2 = 1.68%). However, interventions conducted less than 180 min per week had no significant associations with cognitive function in MS patients (Cohen's d = 0.10, 95% CI − 0.10 to 0.29, p = 0.32, I2 = 15.21%).
Seven studies [27, 29, 33, 35, 38, 40, 42] included participants with a mean EDSS > 3.5 and 12 studies [9, 13, 14, 16, 30,31,32, 36, 37, 39, 41, 43] included participants with a mean 0 < EDSS ≤ 3.5. Exercise significantly improved cognitive function in moderate to severe MS patients (Cohen's d = 0.41, 95% CI 0.15–0.67, p < 0.01, I2 = 40.58%). However, exercise had no significant effect on improving cognitive function in mild MS patients (Cohen's d = 0.12, 95% CI − 0.08 to 0.32, p = 0.25, I2 = 30.77%). Subgroup analysis indicated that the worse basal MS status, the greater effect on cognitive function.
Twelve studies [9, 13, 16, 27, 30, 31, 34, 36, 37, 39, 41, 43] involved participants with mean age < 45 years and 9 studies [11, 14, 29, 32, 33, 35, 38, 40, 42] involved participants with mean age ≥ 45 years. Exercise significantly improved cognitive function in middle-aged and elderly MS patients (Cohen's d = 0.28, 95% CI 0.05–0.52, p = 0.03, I2 = 6.10%). However, exercise had no significant effect on improving cognitive function in young MS patients (Cohen's d = 0.16, 95% CI − 0.03 to 0.35, p = 0.10, I2 = 39.62%). Subgroup analysis indicated that the older the age, the greater effect on cognitive function.
Discussion
The aim of this study was to explore the effect of exercise on cognitive function in MS patients. From 1853 search records initially identified, 21 studies were considered eligible for systematic review and meta-analysis. However, because the included studies were RCTs of exercise interventions, full blinding could not be used. For most of the non-pharmacological interventions in the trials, the results may have been biased even if the best experimental design was used, and therefore we did not regard the trials without blind method as low quality during the quality assessment of the literature, as this would not be reasonable. In the literature quality assessment of included studies, 20 studies were of high quality, which helped to strengthen our findings. Our results showed that exercise, especially multicomponent training, had a significant effect on improving cognitive function, especially cognitive memory, in MS patients. Subgroup analyses showed that exercise conducted 8 and 10 weeks, 3 times or more per week, up to 60 min per session, and 180 min or more per week improved cognitive function significantly. In addition, a worse basal MS status, or the older the age, the greater effect on cognitive function.
It is now widely accepted that regular exercise may be a potential solution to improve cognitive function in MS patients [9, 11, 12, 29, 42, 45, 46]. However, the evidence for exercise interventions in MS remains controversial, and most countries do not include exercise interventions as a routine part of care in MS treatment. It is widely accepted that low levels of exercise are inversely associated with the risk ratio of cognitive decline [47]. Exercise promotes the cellular and molecular processes of angiogenesis, neurogenesis and synaptogenesis and is thought to be strongly associated with improved cognitive function [48]. Studies have shown that people with reduced expression of BDNF in the hippocampus and temporal cortex are at increased risk of neurodegenerative diseases, and that BDNF levels can increase two–threefold after acute exercise compared to quiet controls, positively correlating with improved cognitive function [49]. De la Rosa et al. [50] showed that long-term regular exercise can positively affect cognitive function by delaying physiological memory loss and increasing associated neurotrophy as well as improving peripheral regulation of redox, making exercise an effective measure to prevent and improve cognitive deterioration. Colcombe et al. [51] found that a 6-month aerobic exercise intervention increased the volume of gray and white matter regions in older subjects, suggesting a positive effect of aerobic exercise on central nervous system health and cognitive function improvement in older adults, as found in an adolescent study [52]. One meta-analysis showed that resistance training was effective in improving cognitive function (SMD = 0.71) [53], and no adverse events associated with the exercise intervention were found.
Because of the variety of methods to assess cognitive function, we divided cognition into three outcome subdomains based on different types of cognitive function [54], namely EF, memory, and cognitive speed. Of the 21 studies [9, 11, 13, 14, 16, 27, 29,30,31,32,33,34,35,36,37,38,39,40,41,42,43], 8 studies [9, 13, 14, 31, 33, 34, 37, 42] provided data for memory, and memory was tested mainly by brief visual memory test (BVMT-R, 4 studies) [13, 31, 37, 42], California verbal learning test (CVLT, 3studies) [13, 31, 42], selective reminding test (SRT, 3 studies) [9, 14, 34], spatial recall test (SPART, 3 studies) [9, 14, 34], verbal learning memory test (VLMT, 1 study) [37], and Corsi block-tapping task (1 study) [37]. In addition, 15 studies [9, 11, 13, 14, 29,30,31, 34,35,36,37, 40,41,42,43] provided data for cognitive speed, and cognitive speed was tested mainly by symbol digit modalities test (SDMT, 10 studies) [9, 11, 13, 14, 29,30,31, 37, 40, 42], paced auditory serial attention test (PASAT, 9 studies) [9, 14, 29, 34,35,36,37, 41, 43], interference control of reaction time (IC-RT, 1 study) [30], Digit Symbol Substitution Test (DSST, 1 study) [34], and test battery for attention (TAP, 1 study) [37]. Moreover, 7 studies [9, 14, 30, 32, 34, 37, 40] provided data for EF, and EF was tested mainly by word list generation (WLG, 3 studies) [9, 14, 34], Delis–Kaplan executive function system (DKEFS, 1 study) [30], modified flanker task (MFT, 1 study) [30], Stroop color–word interference (SCWT, 1 study) [32], Regensburg verbal fluency test (RWT, 1 study) [37], trail making test B-A (TMT B-A, 1 study) [40], timed up-and-go dual task (TUG dual task, 1 study) [40], movie for assessment of social cognition (MASC, 1 study) [37]. Subgroup analysis showed that exercise significantly improved memory, while exercise had no significant effect on improving cognitive speed and EF in MS patients, which was inconsistent with the result of Gharakhanlou et al. [55], showing that exercise training had no significant effects on cognitive speed, EF, and memory. The difference between their results and ours may be due to the following reasons. On the one hand, they searched the databases from the inception of indexing until January 2020, while we also included 8 studies published in 2020, 2021, and 2022. On the other hand, they included both RCTs and non-RCTs, while we included only RCTs. However, Hötting et al. [56] found that 6 months of aerobic exercise or stretching significantly improved memory capacity in the experimental group compared to the sedentary control group, which was consistent with our study. The human brain adapts to the external world through neuroplasticity, and exercise can promote neuroplasticity in the human brain and thus improve cognitive ability [57]. Previous studies have found that memory is particularly susceptible to movement, and that movement modulates neurogenesis and plasticity in the hippocampus, which is associated with improvements in hippocampus-dependent learning and memory [48, 58].
Our previous study showed that the characteristics of the intervention (such as intervention type, minutes of intervention per session, frequency of intervention per week, and duration of intervention) can influence the effect of exercise on cognitive function [59]. First, we determined whether intervention type influenced the effect of exercise on cognitive function in MS patients. The improvement of cognitive function in MS patients varies between intervention types, with aerobic exercise being the most common option used to study exercise to improve cognitive function. Of 21 studies, 10 studies [11, 13, 14, 30, 32, 34, 37, 38, 40, 42] provided data for aerobic exercise, 2 studies [39, 41] provided data for resistance exercise, and 8 studies [9, 16, 27, 29, 31, 35, 36, 43] provided data for multicomponent training. Although aerobic exercise was the most used intervention, our study only found multicomponent training to be effective for cognitive function in MS patients. Subgroup analysis showed that aerobic exercise had no significant associations with cognitive function in MS patients, which may be related to the duration and frequency of the aerobic exercise intervention. In recent years, there has been interest in the effect of resistance training on cognitive function, and one meta-analysis showed a positive effect of resistance training on cognitive function [53], but showed a high degree of heterogeneity and no improvement in cognitive function in MS patients, which may be due to the small number of included studies, with only 2 studies using resistance training as exercise intervention.
We next determined whether duration of intervention influenced the effect of exercise on cognitive function in MS patients. In this study, we divided the included studies into 5 subgroups according to duration of intervention, namely 6 weeks, 8 weeks, 10 weeks, 12 weeks, and 24 weeks. Our subgroup analysis showed that 8 and 10 weeks of exercise significantly improved cognitive function, while 6, 12, and 24 weeks of exercise had no significant associations with cognitive function in MS patients. We suspected that 6 weeks of intervention may be too short to improve brain structure and function, whereas 12- and 24-week interventions are too long, leading to exercise resistance effects in MS patients. Of the included studies, only 1 study was conducted for 6 or 10 weeks, which may be biased, studies focused on duration of exercise intervention need to be cautious when referring to our finding.
As for frequency of intervention per week, our subgroup analysis showed that interventions conducted 3 times or more per week significantly improved cognitive function, while interventions conducted less than 3 times per week had no significant associations with cognitive function in MS patients. In addition, the effect size for MS patients engaged in high-frequency exercise was larger than that for those engaged in low-frequency exercise, which indicated that high-frequency interventions have better cognitive effects than low-frequency interventions [9, 32]. We noted that the use of exercise intervention frequency alone cannot exclude the influence of other confounding factors, such as the duration of intervention per session and the duration of intervention per week, which may influence effects of exercise on cognitive function.
Previous study has shown that exercise has a dose–effect relationship with health, that an appropriate loading is the key to exercise for health [60], and that extra-long exercise does not provide health benefits and may even have negative effects on the organism. Our subgroup analysis showed that interventions conducted up to 60 min per session significantly improved cognitive function, while interventions conducted more than 60 min per session had no significant associations with cognitive function in patients with MS, which was in consistent with the results of Cai et al. [61], showing that performing a combination of 45–60 min of exercise three times per week was effective in improving working memory in older adults. In addition, a meta-analysis by Northey et al. [62] found that exercise interventions longer than 60 min were not associated with cognitive function in older adults over 50 years of age, suggesting that longer exercise interventions do not produce greater benefits on cognitive function and that 45–60 min interventions should be chosen when formulating exercise prescriptions. Furthermore, previous studies have shown that 20 min of exercise per session can have a favorable effect on cognitive function in older adults, but exercise for too short a time does not lead to improvements in brain structure and function, and exercise for too long can lead to fatigue and result in a reduced brain plasticity [61, 63], suggesting that the timing of exercise intervention to improve cognitive function in MS patients is important, and future studies should elucidate the effect of the timing of exercise intervention.
However, we found that using only the frequency of intervention per week and minutes of intervention per session did not exclude the effects of other variables, so we considered using frequency of intervention per week and minutes of intervention per session to calculate minutes of intervention per week for each study and to provide new ideas for exercise prescription. The World Health Organization (WHO) recommends that adults should perform 150–300 min of moderate-intensity aerobic exercise, 75–150 min of vigorous-intensity aerobic exercise, or an equivalent combination of moderate-intensity and vigorous-intensity aerobic exercises per week [64]. Our subgroup analysis showed that interventions conducted 180 min or more per week significantly improved cognitive function, while interventions conducted less than 180 min per week had no significant associations with cognitive function in MS patients, which was in consistent with the results of Groot et al. [65], showing that interventions conducted more than 150 min per week yielded a positive effect on cognitive function. Combining the results of frequency of intervention per week and minutes of intervention per session above, we suggest that MS patients should exercise for up to 60 min per session, which can be used to achieve better gains in cognitive function improvement by increasing the frequency of intervention per week.
In recent decades, researchers have developed a number of assessment tools to describe the clinical severity and functional deficits of MS patients, the most popular of which is the EDSS, an assessment scale primarily used to assess central nervous system function [66]. EDSS scores range from 0 to 10, representing the entire range from normal neurological status to death, with the higher scores associated with greater impairment [67], including normal (EDSS = 0), mild (0 < EDSS ≤ 3.5), moderate to severe MS (EDSS > 3.5) [27]. In the above results, we suspected that the improvement of cognitive function by exercise was influenced by the basal MS status of participants, so this study divided the included studies into 2 subgroups, the mild group and moderate to severe group. Because only one of the included studies focused on patients with severe MS, we combined the moderate and severe outcomes. Our subgroup analysis showed that exercise significantly improved cognitive function in moderate to severe MS patients, while exercise had no significant effect on improving cognitive function in mild MS patients, which indicated that the worse basal MS status, the greater effect on cognitive function. A previous study in patients with moderate cognitive impairment showed that cognitive decline was faster in the control group than in the exercise intervention group [68] thus allowing for a more sensitive determination of the cognitive benefits of exercise.
Regarding exercise to improve cognitive function, most studies have chosen middle-aged and elderly population because of the decrease in cognitive function with age and changes in the structure and function of some brain regions [69]. Our subgroup analysis showed that exercise significantly improved cognitive function in middle-aged and elderly MS patients (age ≥ 45 years), while exercise had no significant effect on improving cognitive function in young MS patients (age < 45 years), which indicated that the older the age, the greater effect on cognitive function. Previous studies have long considered exercise interventions to be the most widely available option for reducing age-related cognitive decline, and long-term exercise intervention plays a positive role in reducing delayed cognitive loss, thus suggesting that exercise is effective as a strategy for improving age-related neurodegenerative disorders [70, 71]. Northey et al. [62] showed that exercise was effective in improving cognitive function in adults over 50 years of age, regardless of cognitive status. However, other studies have reported the failure of exercise interventions to improve cognitive function in middle-aged and elderly MS patients [29, 32, 35, 40], which may be related to type, duration, and frequency of the exercise intervention.
Limitations of the review
There are some limitations of this study that should be addressed. First, because our studies were RCTs, the exercise interventions could not be blinded, and therefore there was a bias due to subjective factors when performing quality assessment of the included studies. Second, many of the included studies did not report the intensity of the exercise intervention, and therefore we were unable to understand the effects of different exercise intensities on cognitive function in MS patients. Finally, the most common MS patient in our included studies was RRMS, but it was often mixed with other phenotypes, weakening the possibility of performing subgroup analyses.
Conclusion
MS patients are recommended to participate in at least three multicomponent training sessions per week, with each session lasting up to 60 min, and the exercise goal of 180 min per week can be achieved by increasing the frequency of exercise. Exercise lasting 8 or 10 weeks is best for cognitive function improvement. Additionally, a worse basal MS status, or the older the age, the greater effect on cognitive function.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
References
Rodríguez Murúa S, Farez MF, Quintana FJ (2022) The immune response in multiple sclerosis. Annu Rev Pathol 17:121–139. https://doi.org/10.1146/annurev-pathol-052920-040318
Bhargava P, Hartung HP, Calabresi PA (2022) Contribution of B cells to cortical damage in multiple sclerosis. Brain 145(10):3363–3373. https://doi.org/10.1093/brain/awac233
Carotenuto A, Cacciaguerra L, Pagani E, Preziosa P, Filippi M, Rocca MA (2022) Glymphatic system impairment in multiple sclerosis: relation with brain damage and disability. Brain 145(8):2785–2795. https://doi.org/10.1093/brain/awab454
De Meo E, Portaccio E, Giorgio A, Ruano L, Goretti B, Niccolai C, Patti F, Chisari CG, Gallo P, Grossi P, Ghezzi A, Roscio M, Mattioli F, Stampatori C, Simone M, Viterbo RG, Bonacchi R, Rocca MA, De Stefano N, Filippi M, Amato MP (2021) Identifying the distinct cognitive phenotypes in multiple sclerosis. JAMA Neurol 78(4):414–425. https://doi.org/10.1001/jamaneurol.2020.4920
Benedict RHB, Amato MP, DeLuca J, Geurts JJG (2020) Cognitive impairment in multiple sclerosis: clinical management, MRI, and therapeutic avenues. Lancet Neurol 19(10):860–871. https://doi.org/10.1016/S1474-4422(20)30277-5
Petajan JH, White AT (1999) Recommendations for physical activity in patients with multiple sclerosis. Sports Med 27(3):179–191. https://doi.org/10.2165/00007256-199927030-00004
Gutierrez GM, Chow JW, Tillman MD, McCoy SC, Castellano V, White LJ (2005) Resistance training improves gait kinematics in persons with multiple sclerosis. Arch Phys Med Rehabil 86(9):1824–1829. https://doi.org/10.1016/j.apmr.2005.04.008
Halabchi F, Alizadeh Z, Sahraian MA, Abolhasani M (2017) Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC Neurol 17(1):185. https://doi.org/10.1186/s12883-017-0960-9
Ozkul C, Guclu-Gunduz A, Eldemir K, Apaydin Y, Yazici G, Irkec C (2020) Combined exercise training improves cognitive functions in multiple sclerosis patients with cognitive impairment: a single-blinded randomized controlled trial. Mult Scler Relat Disord 45:102419. https://doi.org/10.1016/j.msard.2020.102419
Sandroff BM, Wylie GR, Sutton BP, Johnson CL, DeLuca J, Motl RW (2018) Treadmill walking exercise training and brain function in multiple sclerosis: Preliminary evidence setting the stage for a network-based approach to rehabilitation. Mult Scler J Exp Transl Clin 4(1):2055217318760641. https://doi.org/10.1177/2055217318760641
Sandroff BM, Klaren RE, Pilutti LA, Dlugonski D, Benedict RH, Motl RW (2014) Randomized controlled trial of physical activity, cognition, and walking in multiple sclerosis. J Neurol 261(2):363–372. https://doi.org/10.1007/s00415-013-7204-8
Sandroff BM, Johnson CL, Motl RW (2017) Exercise training effects on memory and hippocampal viscoelasticity in multiple sclerosis: a novel application of magnetic resonance elastography. Neuroradiology 59(1):61–67. https://doi.org/10.1007/s00234-016-1767-x
Savšek L, Stergar T, Strojnik V, Ihan A, Koren A, Špiclin Ž, ŠegaJazbec S (2021) Impact of aerobic exercise on clinical and magnetic resonance imaging biomarkers in persons with multiple sclerosis: an exploratory randomized controlled trial. J Rehabil Med 53(4):178. https://doi.org/10.2340/16501977-2814
Langeskov-Christensen M, Hvid LG, Jensen HB, Nielsen HH, Petersen T, Stenager E, Hämäläinen P, Dalgas U (2021) Efficacy of high-intensity aerobic exercise on cognitive performance in people with multiple sclerosis: a randomized controlled trial. Mult Scler 27(10):1585–1596. https://doi.org/10.1177/1352458520973619
Ozkul C, Guclu-Gunduz A, Eldemir K, Apaydin Y, Gulsen C, Yazici G, Soke F, Irkec C (2020) Effect of task-oriented circuit training on motor and cognitive performance in patients with multiple sclerosis: a single-blinded randomized controlled trial. NeuroRehabilitation 46(3):343–353. https://doi.org/10.3233/nre-203029
Kooshiar H, Moshtagh M, Sardar MA, Foroughipour M, Shakeri MT, Vahdatinia B (2015) Fatigue and quality of life of women with multiple sclerosis: a randomized controlled clinical trial. J Sports Med Phys Fitness 55(6):668–674
Higgins J, Green S (2011) Cochrane handbook for systematic reviews for interventions, version 5.1.0. Wiley-Blackwell, New York
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 4(1):1. https://doi.org/10.1186/2046-4053-4-1
You Q, Yu L, Li G, He H, Lv Y (2022) Effects of different intensities and durations of aerobic exercise on vascular endothelial function in middle-aged and elderly people: a meta-analysis. Front Physiol 12:803102. https://doi.org/10.3389/fphys.2021.803102
Tao X, Chen Y, Zhen K, Ren S, Lv Y, Yu L (2023) Effect of continuous aerobic exercise on endothelial function: a systematic review and meta-analysis of randomized controlled trials. Front Physiol 14:1043108. https://doi.org/10.3389/fphys.2023.1043108
Viechtbauer W (2010) Conducting meta-analyses in R with the metafor package. J Stat Softw 36(3):1–48. https://doi.org/10.18637/jss.v036.i03
Assink M, Wibbelink CJ (2016) Fitting three-level meta-analytic models in R: a step-by-step tutorial. Quant Methods Psychol 12(3):154–174. https://doi.org/10.20982/tqmp.12.3.p154
Zhen K, Zhang S, Tao X, Li G, Lv Y, Yu L (2022) A systematic review and meta-analysis on effects of aerobic exercise in people with Parkinson’s disease. NPJ Parkinsons Dis 8(1):146. https://doi.org/10.1038/s41531-022-00418-4
Li G, Lv Y, Su Q, You Q, Yu L (2022) The effect of aerobic exercise on pulse wave velocity in middle-aged and elderly people: a systematic review and meta-analysis of randomized controlled trials. Front Cardiovasc Med 9:960096. https://doi.org/10.3389/fcvm.2022.960096
Firth J, Stubbs B, Rosenbaum S, Vancampfort D, Malchow B, Schuch F, Elliott R, Nuechterlein KH, Yung AR (2017) Aerobic exercise improves cognitive functioning in people with schizophrenia: a systematic review and meta-analysis. Schizophr Bull 43(3):546–556. https://doi.org/10.1093/schbul/sbw115
Angevaren M, Aufdemkampe G, Verhaar HJ, Aleman A, Vanhees L (2008) Physical activity and enhanced fitness to improve cognitive function in older people without known cognitive impairment. Cochrane Database Syst Rev 3:5381. https://doi.org/10.1002/14651858.CD005381.pub3
Shariat A, Ingle L, Cleland JA, Cleland JA, Kargarfard M (2017) Randomized controlled trial to examine the impact of aquatic exercise training on functional capacity, balance, and perceptions of fatigue in female patients with multiple sclerosis. Arch Phys Med Rehabil 99(2):234–241. https://doi.org/10.1016/j.apmr.2017.06.015
Team RC (2011) R: A language and environment for statistical computing. Computing 1:12–21. https://doi.org/10.1890/0012-9658(2002)083[3097:CFHIWS]2.0.CO;2
Sandroff BM, Bollaert RE, Pilutti LA, Peterson ML, Baynard T, Fernhall B, McAuley E, Motl RW (2017) Multimodal exercise training in multiple sclerosis: a randomized controlled trial in persons with substantial mobility disability. Contemp Clin Trials 61:39–47. https://doi.org/10.1016/j.cct.2017.07.016
Sandroff BM, Balto JM, Klaren RE, Sommer SK, DeLuca J, Motl RW (2016) Systematically developed pilot randomized controlled trial of exercise and cognition in persons with multiple sclerosis. Neurocase 22(5):443–450. https://doi.org/10.1080/13554794.2016.1237658
Ozdogar AT, Ertekin O, Kahraman T, Yigit P, Ozakbas S (2020) Effect of video-based exergaming on arm and cognitive function in persons with multiple sclerosis: a randomized controlled trial. Mult Scler Relat Disord 40:101966. https://doi.org/10.1016/j.msard.2020.101966
Oken BS, Kishiyama S, Zajdel D, Bourdette D, Carlsen J, Haas M, Hugos C, Kraemer DF, Lawrence J, Mass M (2004) Randomized controlled trial of yoga and exercise in multiple sclerosis. Neurology 62(11):2058–2064. https://doi.org/10.1212/01.wnl.0000129534.88602.5c
Jeong IC, Karpatkin H, Finkelstein J (2021) Physical telerehabilitation improves quality of life in patients with multiple sclerosis. Stud Health Technol Inform 284:384–388. https://doi.org/10.3233/shti210752
Feys P, Moumdjian L, Van Halewyck F, Wens I, Eijnde BO, Van Wijmeersch B, Popescu V, Van Asch P (2019) Effects of an individual 12-week community-located “start-to-run” program on physical capacity, walking, fatigue, cognitive function, brain volumes, and structures in persons with multiple sclerosis. Mult Scler 25(1):92–103. https://doi.org/10.1177/1352458517740211
Carter A, Daley A, Humphreys L, Snowdon N, Woodroofe N, Petty J, Roalfe A, Tosh J, Sharrack B, Saxton JM (2014) Pragmatic intervention for increasing self-directed exercise behaviour and improving important health outcomes in people with multiple sclerosis: a randomised controlled trial. Multi Scler (Houndmills, Basingstoke, England) 20(8):1112–1122. https://doi.org/10.1177/1352458513519354
Bilek F, Cetisli-Korkmaz N, Ercan Z, Deniz G, Demir CF (2022) Aerobic exercise increases irisin serum levels and improves depression and fatigue in patients with relapsing remitting multiple sclerosis: a randomized controlled trial. Multi Scler Relat Disord 61:103742. https://doi.org/10.1016/j.msard.2022.103742
Baquet L, Hasselmann H, Patra S, Stellmann JP, Vettorazzi E, Engel AK, Rosenkranz SC, Poettgen J, Gold SM, Schulz KH, Heesen C (2018) Short-term interval aerobic exercise training does not improve memory functioning in relapsing-remitting multiple sclerosis-a randomized controlled trial. PeerJ 6:e6037. https://doi.org/10.7717/peerj.6037
Backus D, Moldavskiy M, Sweatman WM (2020) Effects of functional electrical stimulation cycling on fatigue and quality of life in people with multiple sclerosis who are nonambulatory. Int J MS Care 22(4):193–200. https://doi.org/10.7224/1537-2073.2019-101
Andreu-Caravaca L, Ramos-Campo DJ, Chung LH, Manonelles P, Boas JPV, Rubio-Arias JÁ (2022) Fast-velocity resistance training improves force development and mobility in multiple sclerosis. Int J Sports Med 43(7):593–599. https://doi.org/10.1055/a-1710-1492
Hoang P, Schoene D, Gandevia S, Smith S, Lord SR (2016) Effects of a home-based step training programme on balance, stepping, cognition and functional performance in people with multiple sclerosis–a randomized controlled trial. Mult Scler 22(1):94–103. https://doi.org/10.1177/1352458515579442
Kjølhede T, Siemonsen S, Wenzel D, Stellmann JP, Ringgaard S, Pedersen BG, Stenager E, Petersen T, Vissing K, Heesen C, Dalgas U (2018) Can resistance training impact MRI outcomes in relapsing-remitting multiple sclerosis? Mult Scler 24(10):1356–1365. https://doi.org/10.1177/1352458517722645
Sebastião E, McAuley E, Shigematsu R, Adamson BC, Bollaert RE, Motl RW (2018) Home-based, square-stepping exercise program among older adults with multiple sclerosis: results of a feasibility randomized controlled study. Contemp Clin Trials 73:136–144. https://doi.org/10.1016/j.cct.2018.09.008
Romberg A, Virtanen A, Ruutiainen J (2005) Long-term exercise improves functional impairment but not quality of life in multiple sclerosis. J Neurol 252(7):839–845. https://doi.org/10.1007/s00415-005-0759-2
Zhao JG, Zeng XT, Wang J, Liu L (2017) Association between calcium or vitamin D supplementation and fracture incidence in community-dwelling older adults: a systematic review and meta-analysis. JAMA 318(24):2466–2482. https://doi.org/10.1001/jama.2017.19344
Sandroff BM, Wylie GR, Johnson CL, Sutton BP, Deluca J, Motl RW (2016) Treadmill walking exercise training effects on processing speed and thalamic resting-state functional connectivity in multiple sclerosis: a pilot study. Mult Scler J 22:398–398. https://doi.org/10.1177/1352458516663081
Proschinger S, Joisten N, Rademacher A, Schlagheck ML, Walzik D, Metcalfe AJ, Oberste M, Warnke C, Bloch W, Schenk A, Bansi J, Zimmer P (2019) Influence of combined functional resistance and endurance exercise over 12 weeks on matrix metalloproteinase-2 serum concentration in persons with relapsing-remitting multiple sclerosis-a community-based randomized controlled trial. BMC Neurol 19(1):314. https://doi.org/10.1186/s12883-019-1544-7
Laurin D, Verreault R, Lindsay J, MacPherson K, Rockwood K (2001) Physical activity and risk of cognitive impairment and dementia in elderly persons. Arch Neurol 58(3):498–504. https://doi.org/10.1001/archneur.58.3.498
van Praag H, Christie BR, Sejnowski TJ, Gage FH (1999) Running enhances neurogenesis, learning, and long-term potentiation in mice. Proc Natl Acad Sci U S A 96(23):13427–13431. https://doi.org/10.1073/pnas.96.23.13427
Rasmussen P, Brassard P, Adser H, Pedersen MV, Leick L, Hart E, Secher NH, Pedersen BK, Pilegaard H (2009) Evidence for a release of brain-derived neurotrophic factor from the brain during exercise. Exp Physiol 94(10):1062–1069. https://doi.org/10.1113/expphysiol.2009.048512
De la Rosa A, Solana E, Corpas R, Bartrés-Faz D, Pallàs M, Vina J, Sanfeliu C, Gomez-Cabrera MC (2019) Long-term exercise training improves memory in middle-aged men and modulates peripheral levels of BDNF and Cathepsin B. Sci Rep 9(1):3337. https://doi.org/10.1038/s41598-019-40040-8
Colcombe SJ, Erickson KI, Scalf PE, Kim JS, Prakash R, McAuley E, Elavsky S, Marquez DX, Hu L, Kramer AF (2006) Aerobic exercise training increases brain volume in aging humans. J Gerontol A Biol Sci Med Sci 61(11):1166–1170. https://doi.org/10.1093/gerona/61.11.1166
Herting MM, Nagel BJ (2012) Aerobic fitness relates to learning on a virtual Morris water task and hippocampal volume in adolescents. Behav Brain Res 233(2):517–525. https://doi.org/10.1016/j.bbr.2012.05.012
Landrigan JF, Bell T, Crowe M, Clay OJ, Mirman D (2020) Lifting cognition: a meta-analysis of effects of resistance exercise on cognition. Psychol Res 84(5):1167–1183. https://doi.org/10.1007/s00426-019-01145-x
Markun S, Gravestock I, Jäger L, Rosemann T, Pichierri G, Burgstaller JM (2021) Effects of vitamin B12 supplementation on cognitive function, depressive symptoms, and fatigue: a systematic review, meta-analysis, and meta-regression. Nutrients. https://doi.org/10.3390/nu13030923
Gharakhanlou R, Wesselmann L, Rademacher A, Lampit A, Negaresh R, Kaviani M, Oberste M, Motl RW, Sandroff BM, Bansi J, Baker JS, Heesen C, Zimmer P, Javelle F (2021) Exercise training and cognitive performance in persons with multiple sclerosis: a systematic review and multilevel meta-analysis of clinical trials. Mult Scler 27(13):1977–1993. https://doi.org/10.1177/1352458520917935
Hötting K, Holzschneider K, Stenzel A, Wolbers T, Röder B (2013) Effects of a cognitive training on spatial learning and associated functional brain activations. BMC Neurosci 14:73. https://doi.org/10.1186/1471-2202-14-73
Hötting K, Röder B (2013) Beneficial effects of physical exercise on neuroplasticity and cognition. Neurosci Biobehav Rev 37(9):2243–2257. https://doi.org/10.1016/j.neubiorev.2013.04.005
van Praag H, Kempermann G, Gage FH (2000) Neural consequences of environmental enrichment. Nat Rev Neurosci 1(3):191–198. https://doi.org/10.1038/35044558
Zhang S, Zhen K, Su Q, Chen Y, Lv Y, Yu L (2022) The effect of aerobic exercise on cognitive function in people with Alzheimer’s disease: a systematic review and meta-analysis of randomized controlled trials. Int J Environ Res Public Health 19(23):15700. https://doi.org/10.3390/ijerph192315700
Izquierdo M, Merchant RA, Morley JE, Anker SD, Aprahamian I, Arai H, Aubertin-Leheudre M, Bernabei R, Cadore EL, Cesari M, Chen LK, de Souto BP, Duque G, Ferrucci L, Fielding RA, García-Hermoso A, Gutiérrez-Robledo LM, Harridge SDR, Kirk B, Kritchevsky S, Landi F, Lazarus N, Martin FC, Marzetti E, Pahor M, Ramírez-Vélez R, Rodriguez-Mañas L, Rolland Y, Ruiz JG, Theou O, Villareal DT, Waters DL, Won Won C, Woo J, Vellas B, Fiatarone Singh M (2021) International exercise recommendations in older adults (ICFSR): expert consensus guidelines. J Nutr Health Aging 25(7):824–853. https://doi.org/10.1007/s12603-021-1665-8
Cai Z, Wang X, Yin J, Song D, Chen Z (2021) Effects of physical exercise on working memory in older adults: a systematic and meta-analytic review. Eur Rev Aging Phys Act 18(1):18. https://doi.org/10.1186/s11556-021-00272-y
Northey JM, Cherbuin N, Pumpa KL, Smee DJ, Rattray B (2018) Exercise interventions for cognitive function in adults older than 50: a systematic review with meta-analysis. Br J Sports Med 52(3):154–160. https://doi.org/10.1136/bjsports-2016-096587
Chen FT, Etnier JL, Wu CH, Cho YM, Hung TM, Chang YK (2018) Dose-response relationship between exercise duration and executive function in older adults. J Clin Med 7(9):279. https://doi.org/10.3390/jcm7090279
Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, Carty C, Chaput JP, Chastin S, Chou R, Dempsey PC, DiPietro L, Ekelund U, Firth J, Friedenreich CM, Garcia L, Gichu M, Jago R, Katzmarzyk PT, Lambert E, Leitzmann M, Milton K, Ortega FB, Ranasinghe C, Stamatakis E, Tiedemann A, Troiano RP, van der Ploeg HP, Wari V, Willumsen JF (2020) World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med 54(24):1451–1462. https://doi.org/10.1136/bjsports-2020-102955
Groot C, Hooghiemstra AM, Raijmakers PG, van Berckel BN, Scheltens P, Scherder EJ, van der Flier WM, Ossenkoppele R (2016) The effect of physical activity on cognitive function in patients with dementia: a meta-analysis of randomized control trials. Ageing Res Rev 25:13–23. https://doi.org/10.1016/j.arr.2015.11.005
Meyer-Moock S, Feng YS, Maeurer M, Dippel FW, Kohlmann T (2014) Systematic literature review and validity evaluation of the expanded disability status scale (EDSS) and the multiple sclerosis functional composite (MSFC) in patients with multiple sclerosis. BMC Neurol 14:58. https://doi.org/10.1186/1471-2377-14-58
Kurtzke JF (1983) Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 33(11):1444–1452. https://doi.org/10.1212/wnl.33.11.1444
Venturelli M, Scarsini R, Schena F (2011) Six-month walking program changes cognitive and ADL performance in patients with Alzheimer. Am J Alzheimers Dis Other Demen 26(5):381–388. https://doi.org/10.1177/1533317511418956
Hedden T, Gabrieli JD (2004) Insights into the ageing mind: a view from cognitive neuroscience. Nat Rev Neurosci 5(2):87–96. https://doi.org/10.1038/nrn1323
Sofi F, Valecchi D, Bacci D, Abbate R, Gensini GF, Casini A, Macchi C (2011) Physical activity and risk of cognitive decline: a meta-analysis of prospective studies. J Intern Med 269(1):107–117. https://doi.org/10.1111/j.1365-2796.2010.02281.x
De la Rosa A, Olaso-Gonzalez G, Arc-Chagnaud C, Millan F, Salvador-Pascual A, García-Lucerga C, Blasco-Lafarga C, Garcia-Dominguez E, Carretero A, Correas AG, Viña J, Gomez-Cabrera MC (2020) Physical exercise in the prevention and treatment of Alzheimer’s disease. J Sport Health Sci 9(5):394–404. https://doi.org/10.1016/j.jshs.2020.01.004
Funding
This study was supported by the National Key R&D Program of China (2022YFC3600201) and the Chinese Universities Scientific Fund (2022QN015).
Author information
Authors and Affiliations
Contributions
GL and QY wrote the manuscript. LY and YL contributed to the conception and design. GL and QY extracted data the data and evaluated the quality. XH, SZ, and LD verified the data. GL, QY, XH, SZ, LD, YL, and LY contributed to the analysis and interpretation of the data. GL, QY, XH, SZ, LD, YL, and LY revised it critically for important intellectual content. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical approval
No ethical approval was needed. All studies in this review have been approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Li, G., You, Q., Hou, X. et al. The effect of exercise on cognitive function in people with multiple sclerosis: a systematic review and meta-analysis of randomized controlled trials. J Neurol 270, 2908–2923 (2023). https://doi.org/10.1007/s00415-023-11649-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-023-11649-7