
Abstract
Joint lavage for knee osteoarthritis is an invasive procedure that can be stressful and painful. We aimed to assess the impact of music therapy on perioperative anxiety, pain and tolerability of the procedure in patients undergoing joint lavage performed with two needles. We randomized all patients diagnosed with knee osteoarthritis and undergoing joint lavage in our department from November 2009 to October 2010 to an experimental group listening to recorded music or a control group receiving no music intervention. Perioperative anxiety and pain related to the procedure were self-reported on a visual analogic scale (0–100 mm visual analog scale [VAS]), and heart rate and blood pressure were measured during the procedure. Tolerability was assessed on a four-grade scale directly after the procedure. We included 62 patients (31 in each group). Mean age was 68.8 ± 12.6 years (72% females). As compared with the control group, the music group had lower levels of perioperative anxiety (40.3 ± 31.1 vs. 58.2 ± 26.3 mm; p = 0.046) and pain related to the procedure (26.6 ± 16.2 vs. 51.2 ± 23.7 mm; p = 0.0005). Moreover, heart rate was lower in the music group (69.5 ± 11.4 vs. 77.2 ± 13.2; p = 0.043) but not diastolic or systolic blood pressure. Tolerability was higher in the music group (p = 0.002). Music is a simple and effective tool to alleviate pain and anxiety in patients undergoing joint lavage for knee osteoarthritis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Knee osteoarthritis (OA) is a major cause of pain and disability, particularly in elderly people [1]. Joint lavage of the knee, most often performed with one or two large needles, aims to remove debris such as microscopic or macroscopic fragments of cartilage matrix, bone macromolecules and calcium crystals that may induce synovitis, a likely source of pain [2–4].
Some studies [5–7], but not all [8], have suggested that joint lavage may decrease pain and improve function in patients with knee OA. However, joint lavage is an invasive procedure that can be stressful and painful [7]. To improve the tolerability of this procedure, video information proposed before joint lavage was shown to significantly decrease pain and anxiety [9]. Although of interest, use of videotapes to provide information requires equipment not always available in rheumatologic departments.
Music intervention has been used to reduce anxiety and distress related to invasive procedures such as colonoscopy, breast biopsy or coronarography [10, 11] and to decrease pain in patients with leg fracture [12]. In addition, a recent meta-analysis found that listening to music may have a beneficial effect on blood pressure, heart rate, respiratory rate, anxiety, and pain in patients with coronary heart disease [13]. Music therapy promotes relaxation responses, triggers positive associations and diverts attention away from anxiety during pain and stressful procedures [14].
We aimed to assess the impact of music therapy on anxiety and pain during joint lavage for knee OA.
Patients and methods
Ethics statement
The Institutional Review Board (No. IRB00006477) of Paris North Hospitals reviewed and approved this study. All patients gave their written informed consent to participate.
Patients
All patients with knee OA who were scheduled for knee joint lavage in the Day Unit of our rheumatology department from November 2009 to October 2010 were considered for enrolment. Joint lavage was indicated for inadequate pain control and/or persistence of chronic joint effusion with prior failure of intra-articular glucocorticoid injection, physical exercises, analgesics, and nonsteroidal anti-inflammatory drugs.
Study design
The study was prospective and monocenter. On arrival at the Day Unit on the day of lavage, patients were randomized to music or no-music groups.
Joint lavage procedure
The procedure was performed by two trained rheumatologists (JLB and SO) under sterile conditions by the technique proposed by Ayral and Dougados [15]. After the skin was prepared with iodine, arthrocentesis of the knee was performed by use of the lateral suprapatellar portal. Next, a local anesthetic (1% lidocaine) was injected intra-articularly (10 ml) and throughout the capsula, subcutaneous tissue, and skin of the lateral suprapatellar portal (10 ml). The medial suprapatellar portal was similarly injected with 1% lidocaine. Two 14-gauge cannulae were introduced into the medial and lateral suprapatellar portals (1 for inflow and the other for outflow). The medial suprapatellar cannula was connected to an extension line and infusion set containing sterile 0.9% saline. Evacuation was by the lateral cannula. Adequate lavage was ensured by transient obturation of the lateral outflow needle, mobilization of the joint (10–20° flexion and extension combined with stress in valgus and varus positions to open and irrigate tibiofemoral compartments), and manual compression of the distended joint cavity. A total of 1 l of 0.9% saline was injected into and evacuated from the knee joint [15]. Finally, a corticosteroid was injected intra-articularly.
Anxiety and pain assessment
Anxiety and pain were evaluated during the procedure after 14-gauge cannulae were introduced. Anxiety was measured on a 100-mm visual analog scale (VAS), 0 indicating the absence of anxiety and 100 the most severe anxiety. Pain was evaluated on a 100-mm VAS, 0 indicating the absence of pain and 100 the most severe pain. In addition, blood pressure and heart rate were automatically measured. At the end of the lavage, with the patient still lying on the operating table, tolerability of the procedure was assessed as very tolerable, tolerable, intolerable, or very intolerable. A good response for tolerability was arbitrarily defined as very tolerable. This information was collected for all patients by a single observer (i.e., the nurse working in the operating room).
Music intervention
All patients randomized to the music group listened to the same recorded lyric music without headphones during the preparation for the procedure (5–10 min) and during the whole procedure (10–20 min).
Statistical analysis
Data are presented as mean ± SD. Wilcoxon’s test was used for quantitative variables (anxiety, pain, blood pressure and heart rate), and chi-square test was used for categorical data (tolerability). A two-sided p < 0.05 was considered statistically significant. Analysis involved use of StatView v5.0 (SAS, Gary, IN, USA).
Results
Characteristics of patients
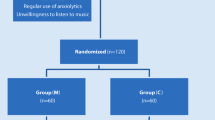
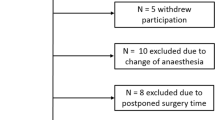
From November 2009 to October 2010, 88 patients underwent joint lavage for knee OA; 26 refused to participate in the study (Fig. 1). Therefore, we randomized 31 patients each to the music and control groups. The groups did not differ in baseline characteristics (Table 1).

Flowchart of the study
Impact of music therapy
Perioperative levels of anxiety and pain related to the procedure were significantly lower in the music than control group: 40.3 ± 31.1 vs. 58.2 ± 26.3 mm (p = 0.046) and 26.6 ± 16.2 vs. 51.2 ± 23.7 mm (p = 0.0005), respectively (Table 2). Tolerability was significantly better in the music than control group (good responders 18/31 vs. 6/31; p = 0.002) (Table 2).
Music therapy was associated with decreased heart rate (69.5 ± 11.4 vs. 77.2 ± 13.2; p = 0.043) (Table 2) but not systolic or diastolic blood pressure.
Impact of gender, age, anxiolytic drugs, operator, and previous joint lavage
Perioperative anxiety was significantly lower for males than females (36.2 ± 21.5 vs. 54.2 ± 31.3 mm; p = 0.03), with no difference by gender for tolerability (p = 0.36) or pain (p = 0.36).
Pain, anxiety and tolerability did not differ by operator (JLB or SO), use of anxiolytic drugs or the age of patients (data not shown).
In contrast, for patients who had previous experience with joint lavage (n = 11), the level of anxiety was lower, although not significantly, than for those with no previous experience (39.5 ± 28.8 vs. 51.4 ± 30.1 mm; p = 0.24) and pain (27.0 ± 19.4 vs. 41.5 ± 23.9 mm; p = 0.08).
Discussion
We evaluated the effect of music on pain and anxiety in patients undergoing joint lavage for knee OA. Our results suggest that listening to music during the procedure can alleviate pain and anxiety and improve the tolerability of the procedure.
Several non-pharmacological approaches such as providing video information and hypnosis have been used to avoid the use of anxiolytic and/or analgesic drugs before or during invasive procedures or stressful conditions such as labour or leg fracture pain [12, 16]. In rheumatology, video information before joint lavage for OA decreased anxiety during the procedure and improved tolerability [9]. The beneficial effects of music therapy during several invasive procedures have been reported [10]. A recent meta-analysis showed that music improved patients’ overall experience with colonoscopy but had no effect on pain or the use of analgesic drugs [11]. In patients with leg fracture [12] or undergoing bone marrow biopsy [17] or breast core-needle biopsy [18], music could reduce pain and/or anxiety score.
In our study, we found the perioperative levels of both anxiety and pain significantly lower in the music than control group, which suggested a beneficial impact of this therapy. Moreover, tolerability was improved and heart rate, which is affected by external stresses, was lower in the music group. These results agree with previous studies of music for coronary heart disease. A Cochrane systematic review concluded that listening to music may reduce heart rate, respiratory rate, pain and blood pressure even if the beneficial effect is modest and clinical significance unclear [13].
Demographic characteristics seemed to have little influence on the impact of music during the procedure. Indeed, despite a higher anxiety level in female than male patients, the effect of music did not differ by gender. Moreover, we found no impact of age, operator or concomitant use of anxiolytic drugs on the music effect. Therefore, all patients could benefit from music therapy. A lower level of anxiety and pain, although not significant, in patients who had previous experience with the procedure was also suggested in another study of precolonoscopy anxiety [19].
Because of its open design, our study has some limitations that deserve attention. Trials evaluating non-pharmacologic treatments are more difficult to perform than are those evaluating pharmacologic treatments. Indeed, the placebo effect is impossible to analyse and is potentially important in such therapies. Moreover, surgeons were not blinded to the treatment group, so an effect of music on the quality of the procedure could not be ruled out. We thus cannot rule out a potential bias that might have influenced our results.
Conclusion
Our study suggests that music therapy is a simple and effective tool to reduce pain and anxiety during joint lavage for knee OA. Because music seems to work as well for various invasive medical procedures, assessing its beneficial effects for other painful procedures frequently performed in rheumatology such as synovial biopsies, joint, spinal and soft tissue injections [20] is of interest.
References
Hadler NM (1985) Osteoarthritis as a public health problem. Clin Rheum Dis 11(2):175–185
Hill CL, Hunter DJ, Niu J, Clancy M, Guermazi A, Genant H, Gale D, Grainger A, Conaghan P, Felson DT (2007) Synovitis detected on magnetic resonance imaging and its relation to pain and cartilage loss in knee osteoarthritis. Ann Rheum Dis 66(12):1599–1603
Bradley JD (2003) Joint irrigation as treatment for osteoarthritis. Curr Rheumatol Rep 5(1):20–26
Ayral X (2005) Arthroscopy and joint lavage. Best Pract Res Clin Rheumatol 19(3):401–415
Ike RW, Arnold WJ, Rothschild EW, Shaw HL (1992) Tidal irrigation versus conservative medical management in patients with osteoarthritis of the knee: a prospective randomized study. Tidal Irrigation Cooperating Group. J Rheumatol 19(5):772–779
Ravaud P, Moulinier L, Giraudeau B, Ayral X, Guerin C, Noel E, Thomas P, Fautrel B, Mazieres B, Dougados M (1999) Effects of joint lavage and steroid injection in patients with osteoarthritis of the knee: results of a multicenter, randomized, controlled trial. Arthritis Rheum 42(3):475–482
Chang RW, Falconer J, Stulberg SD, Arnold WJ, Manheim LM, Dyer AR (1993) A randomized, controlled trial of arthroscopic surgery versus closed-needle joint lavage for patients with osteoarthritis of the knee. Arthritis Rheum 36(3):289–296
Avouac J, Vicaut E, Bardin T, Richette P (2010) Efficacy of joint lavage in knee osteoarthritis: meta-analysis of randomized controlled studies. Rheumatology (Oxford) 49(2):334–340
Ayral X, Gicquere C, Duhalde A, Boucheny D, Dougados M (2002) Effects of video information on preoperative anxiety level and tolerability of joint lavage in knee osteoarthritis. Arthritis Rheum 47(4):380–382
Nilsson U (2008) The anxiety- and pain-reducing effects of music interventions: a systematic review. AORN J 87(4):780–807
Bechtold ML, Puli SR, Othman MO, Bartalos CR, Marshall JB, Roy PK (2009) Effect of music on patients undergoing colonoscopy: a meta-analysis of randomized controlled trials. Dig Dis Sci 54(1):19–24
Kwon IS, Kim J, Park KM (2006) Effects of music therapy on pain, discomfort, and depression for patients with leg fractures. Taehan Kanho Hakhoe Chi 36(4):630–636
Bradt J, Dileo C (2009) Music for stress and anxiety reduction in coronary heart disease patients. Cochrane Database Syst Rev (2):CD006577
Cook JD (1981) The therapeutic use of music: a literature review. Nurs Forum 20(3):252–266
Ayral X, Dougados M (1995) Joint lavage. Rev Rhum Engl Ed 62(4):281–287
Kimber L, McNabb M (2008) Mc Court C, Haines A, Brocklehurst P: Massage or music for pain relief in labour: a pilot randomised placebo controlled trial. Eur J Pain 12(8):961–969
Shabanloei R, Golchin M, Esfahani A, Dolatkhah R, Rasoulian M (2010) Effects of music therapy on pain and anxiety in patients undergoing bone marrow biopsy and aspiration. AORN J 91(6):746–751
Bugbee ME, Wellisch DK, Arnott IM, Maxwell JR, Kirsch DL, Sayre JW, Bassett LW (2005) Breast core-needle biopsy: clinical trial of relaxation technique versus medication versus no intervention for anxiety reduction. Radiology 234(1):73–78
Luck A, Pearson S, Maddern G, Hewett P (1999) Effects of video information on precolonoscopy anxiety and knowledge: a randomised trial. Lancet 354(9195):2032–2035
Perrot S, Laroche F, Poncet C, Marie P, Payen-Champenois C (2010) Are joint and soft tissue injections painful? Results of a national French cross-sectional study of procedural pain in rheumatological practice. BMC Musculoskelet Disord 11:16
Acknowledgements
We thank Martine Binet and Maggy Lefebvre, who helped with the joint lavage procedures. We also thank the “Rhumatisme et travail” (Hospital Lariboisière) association for funding the study.
Disclosures
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article can be found at http://dx.doi.org/10.1007/s10067-012-1944-1.
Rights and permissions
About this article
Cite this article
Ottaviani, S., Jean-Luc, B., Thomas, B. et al. Effect of music on anxiety and pain during joint lavage for knee osteoarthritis. Clin Rheumatol 31, 531–534 (2012). https://doi.org/10.1007/s10067-011-1925-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-011-1925-9