
Abstract
The objective of the study was to analyse the impact of fibromyalgia (FM) on health-related quality of life (HRQOL) and to identify clinical and psychological factors associated with the disease. A cross-sectional study was conducted with adult Portuguese women with FM. Analysed data were demographic, clinical and psychological variables and HRQOL: SF-36 and Fibromyalgia Impact Questionnaire (FIQ). The relationship between HRQOL and the other variables was made with a bivariate analysis. To assess the relative contribution of clinical and psychological variables, a series of multiple regression analyses were designed and made. The study sample consisted of 76 women with FM (49.61 ± 10.07 years). All dimensions of HRQOL were affected in FM, especially Physical Functioning, Physical Role Functioning and General Health. The mean FIQ total score was 68.59 ± 17.54, and 40 patients (53%) presented scores ≥70. Pain intensity, assessed by a 10-cm visual analogue scale (VAS), was a significant predictor of HRQOL in expressing association with FIQ and all dimensions of SF-36, except Emotional Role Functioning. Anxiety (Hospital Anxiety and Depression Scale (HADS)) was a significant predictor of the Mental Component and General Health (SF-36). Depression (HADS) was related with Vitality, Mental Health and FIQ. Emotion-focused coping was related with General Health and Emotional Role Functioning, and social support (Satisfaction with Social Support Scale (ESSS)) was related with the Social Functioning. These clinical and psychological variables explained an acceptable proportion of variability (R 2), ranging from 31.3% on Emotional Role Functioning to 70.6% on FIQ, except for Physical Role Functioning (R 2 = 6.1). FM has a negative impact on both general and specific dimensions of HRQOL, especially the physical dimensions. Pain intensity, anxiety and depression symptoms and the emotion-focused coping are the most relevant explanatory variables of the impact of FM on HRQOL.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Fibromyalgia (FM) is a rheumatic disorder that affects 2–3% of the general population [1], and it is predominant in women [2]. With unknown aetiology, it is characterized by chronic widespread muscular pain, often accompanied by somatic and psychological symptoms which can cause a marked deterioration in health-related quality of life (HRQOL), although there are no pathologic lesions or deformity involved. The aim of the 2000–2010 Bone and Joint Decade was to improve the HRQOL of patients with musculoskeletal disorders [3]. Therefore, in recent years, there has been increased interest in the study of the impact of FM on HRQOL. To evaluate the effect of FM on patients HRQOL, it is important not only to quantify the degree of decline but also to determine the impact on the different physical, psychological and social domains. Such information may support health professionals to establish areas in which to direct their research to; this will enable improvement to the clinical management and the health status. However, few studies have been conducted for this purpose, so in many aspects the information we currently have on the connection between HRQOL and the variables of socio-demographic, clinical or psychological character cannot be considered convincing.
As far as socio-demographic data are concerned, the impacts of age, sex, employment status and economic income on HRQOL results are contradictory, as different studies suggest both the presence and the absence of correlation between variables [4–10]. Other variables such as educational level and number of children are only mentioned in a recent study [9], which suggests a higher impairment of quality of life, reported by the FIQ, in FM patients with lower academic education and with a higher number of children.
As to the clinical factors, only pain intensity results show consistent and significant effect on HRQOL [11, 12], but the relationships between HRQOL and the number of tender points and pain threshold, as well as fatigue and illness duration, are controversial [8, 11–15]. The pharmacological treatment has been scarcely studied, and the only study we found that examines the impact of this aspect on HRQOL indicates that patients in pharmacological therapy had a poorer HRQOL [9].
When it comes to the psychological variables, the influence of depression and anxiety symptoms on HRQOL of patients with FM was studied by different researchers, and they are unanimous in pointing to its significant impact on HRQOL [12, 14, 16]. Social support was also positively and significantly associated with HRQOL [9, 17], although the number of studies is reduced. Finally, for coping strategies the results are controversial [14, 15], so the potential role of this variable still remains to be clarified.
Given the current state of literature, this study focuses on assessing the HRQOL of women with FM with a dual purpose: firstly, to analyse the impact of FM in the general and specific dimensions of HRQOL and secondly, to indentify the socio-demographic, clinical and psychological factors that have a higher impact on this disease.
Method
Patients
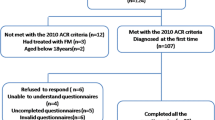
A cross-sectional study was conducted with a sample of Portuguese women diagnosed with FM according to the American College of Rheumatology (ACR) criteria [18], belonging to the National Association Against Fibromyalgia and Chronic Fatigue Syndrome (MYOS). Patients were selected with age ≥ 18 years and without physical or psychological limitations that would prevent them from filling out questionnaires.
Variables studied and measuring instruments
Socio-demographic characteristics
Using a researcher-designed form, participants gave information about their age, residence, marital status, studies, employment status, economic status, impact of FM on economic incomes and possible change of workplace due to FM.
Clinical variables
A clinical data sheet was designed for this study to collect information about age at onset of symptoms, age at diagnosis, time elapsed since the onset of symptoms, time elapsed since diagnosis, number of medical visits/emergency room visits due to FM (last year), number of hospitalizations due to FM (last year), pain experienced during the past week, fatigue felt during the past week, morning stiffness felt last week, morning vigour last week, hours of physical activity last week, physical comorbidity (present or absent), psychiatric comorbidity (present or absent) and pharmacological treatment (present or absent).
Psychological variables
Depression and anxiety symptoms were assessed using the Hospital Anxiety and Depression Scale (HADS) [19, 20]. It consists of 14 items divided into two subscales of seven items. Each subscale ranges from 0–21, and a score of 0–7 points is within normal values. Values between 8 and 10 indicate possible depression/anxiety, and ≥11 suggests clinical depression/anxiety [21].
Coping strategies were assessed with the Brief Cope [22, 23] which consists of 28 items in 14 subscales including: active coping, planning, using instrumental support, emotional social support usage, religion, positive reinterpretation, self-blame, acceptance, expression of feelings, denial, self-distraction, behavioural disinvestment, substance use (drugs/alcohol) and humour. Each strategy is scored from 1 (it is never done) to 4 (it is often done). According to Coolidge et al. [24] it is possible to cluster the coping strategies in three distinct subgroups: the emotion-focused coping, problem-focused coping and dysfunctional coping. The emotion-focused coping includes acceptance, use of emotional social support, humour, positive reinterpretation and religion. The problem-focused coping consists of active coping, instrumental support and the use of planning. The dysfunctional coping is made through disinvestment behaviour, denial, self-distraction, self-blame, substance use and expression of feelings.
Social support was evaluated with the Satisfaction with Social Support Scale (ESSS) [25], and it consists of 15 items divided into four dimensions: satisfaction with friends, intimacy, satisfaction with family and social activities. Each item is scored from 1 (totally agree) to 5 (totally disagree).
Health-related quality of life
The HRQOL was assessed with the generic instrument Short-Form 36 Health Survey (SF-36) [26, 27] and the Fibromyalgia Impact Questionnaire (FIQ) [28, 29].
The SF-36 consists of 36 items, divided into eight dimensions which are grouped into two components: the Physical Component and the Mental Component. The final scores for each dimension ranges from 0 to 100, with the highest scores corresponding to a better condition. The physical component includes the following dimensions: Physical Functioning (PF), Physical Role Functioning (RP), Bodily Pain (BP) and General Health (GH). The Mental Component is measured by the following dimensions: Vitality (VT), Mental Health (MH), Social Functioning (SF) and Emotional Role Functioning (RE).
The FIQ includes 20 items that measure functional capacity, number of days the patient felt well and that failed to work (last week), work capacity, pain, fatigue, morning tiredness, stiffness, anxiety and depression. The overall scores range from 0 to 100, one hundred being the higher negative impact. Patients with a score >70 are considered to be severely affected cases [9].
The original and Portuguese version of the instruments had adequate psychometric properties: HADS [19, 30], Brief Cope [22, 23, 31], ESSS [25], SF-36 [26, 32] and FIQ [29, 33].
Procedures
All women who met the inclusion criteria signed a written informed consent and completed the socio-demographic and clinical data and the following questionnaires: HADS, Brief Cope, ESSS, SF-36 and FIQ (presented randomly to avoid the effect of fatigue).
Statistical analysis
The description of socio-demographic, clinical and psychological variables was based on observed frequencies (categorical variables), and mean and standard deviation (quantitative variables). Internal consistency of the instruments was assessed by Cronbach's α coefficient with acceptable values ≥ 0.70 [34]. Regarding the SF-36 the scores were compared with normative data from Portuguese female population [26]. The scores for the different dimensions of SF-36 were standardized following the method proposed by the authors of SF-36 [35] and using the Portuguese population normative data according to gender and age [26]. The formula applied was: standardized score = (patient score−population mean score)/population standard deviation.
The bivariate relationships between socio-demographic, clinical and psychological variables, and the scores of SF-36 and FIQ were calculated by the H Kruskal–Wallis and the U Mann–Whitney (with Bonferroni correction) and r Spearman. Multiple regression analysis was used to assess the relative contribution of clinical and psychological variables as HRQOL predictors. SF-36 dimensions and FIQ scores were the dependent variables, and the socio-demographic, clinical and psychological variables related with the scales (p < 0.05) were the independent variables. Backward method was used for variable inclusion. The presence of collinearity was assessed by the statistical factor of tolerance and variance inflation (VIF).
The statistical significance level was p < 0.05, and the statistical analysis was made using the SPSS version 17.0 for windows.
Results
The sample studied was formed by 76 women with FM with a mean age of 49.61 ± 10.07 years (range 22–75 years). Most patients (69, 91%) were being medicated. While 1/3 of the sample had no comorbidity (n = 24), 29 (38%) women expressed physical comorbidity, 10 (13%) presented psychiatric comorbidity and 13 (17%) had physical and psychiatric comorbidity.
All the instruments used presented a high internal consistency, with a Cronbach’s α > 0.70 except the Dysfunctional Coping of the Brief Cope (α = 0.66).
The sample expressed a high level of psychological distress for individuals suffering from FM as recorded by HADS. According to the criteria established by Zigmond and Snaith [20], 57 patients (75%) had clinical suspicion of anxiety and 42 (55%) had clinical suspicion of depression.
As far as coping strategies are concerned, following the dimensions of Coolidge et al. [24], the problem-focused coping had the highest scores (3.40 ± 1.28) and the dysfunctional coping showed the lower scores (2.22 ± 0.82). Social Support Scale (ESSS) revealed low levels of general social support (ESSS Total Score), with a mean of 44.04 points.
Socio-demographic, clinical and psychological characteristics are presented in Table 1.
The impact of FM on the generic and specific dimensions of HRQOL and the internal consistency for each scale are presented in Table 2.
The least affected SF-36 dimension was the SF (43.45 ± 22.85), contrasting with RP (11.51 ± 21.38) which presented the most degraded values. FIQ had an average score of 68.59 ± 17.54, and a total of 40 patients (53%) had scores ≥ 70, considered severely affected cases [9].
The SF-36 scores obtained were compared with the Portuguese female population [26], and FM patients showed lower values in all dimensions (p < 0.001). According to score standardization (Ss) of the SF-36 dimensions, the most impaired dimensions were PF (Ss = −2.42), RP (Ss = −1.83) and GH (Ss = −1.81) corresponding to the Physical Component. Comparatively less impaired were SF (Ss = −1.38), RE (Ss = −1.32) and MH (Ss = −1.23) (see Fig. 1).

Standardized scores of the SF-36 dimensions. PF Physical Functioning, RP Physical Role Functioning, BP Bodily Pain, GH General Health, VT Vitality, SF Social Functioning, RE Emotional Role Functioning, MH Mental Health
The relationship analysis between socio-demographic variables and HRQOL showed that patients with FM, living in urban areas, had a better quality of life on RE (U = 208; p < 0.005). This suggests that living in urban areas was the only socio-demographic variable associated with HRQOL.
As far as clinical variables are concerned, significant relationships were found (p < 0.05) between the following: age at diagnosis with RE (r = −0.299); time elapsed since diagnosis with SF (r = 0.280); number of medical/emergency rooms visits due to FM with PF (r = −0.345), BP (r = −0.407), GH (r = −0.343), VT (r = −0.281), SF (r = −0.323), RE (r = −0.279), MH (r = −0.470) and FIQ (r = 0.432); number of hospitalizations due to FM with PF (r = −0.230); pain felt last week with all SF-36 dimensions (range from r = −0.275 to r = −0.606) and with FIQ (r = 0.620); fatigue felt last week with the majority of SF-36 dimensions (except on RP and RE) (range from r = −0.169 to r = −0.465) and with FIQ (r = 0.544); morning vigour felt last week with PF (r = −0.360), BP (r = −0.371), GH (r = −0.279), VT (r = −0.301) and FIQ (r = 0.518); morning stiffness felt last week with PF (r = −0.389), RP (r = −0.282), BP (r = −0.396), GH (r = −0.384), VT (r = −0.434), SF (r = −0.355), RE (r = −0.262) and FIQ (r = 0.541); number of hours of physical activity last week with SF (r = 0.172); presence of physical comorbidity with RE (U = 483.5; p < 0.05); and the pharmacological treatment with PF (U = 27; p < 0.05).
When it comes to psychological variables, as evaluated by HADS, a significant association was found with all SF-36 dimensions (p < 0.05), except RP (range from r = −0.156 to r = −0.714), and a positive association with FIQ (depression: r = 0.650; anxiety: r = 0.570) included. As to emotion-focused coping, a significant relationship was found (p < 0.05) between the following data: GH (r = 0.401), SF (r = 0.263), RE (r = 0.346) and MH (r = 0.463). Regarding the problem-focused coping, no significant correlation was found with the HRQOL. As to dysfunctional coping, a significant correlation was found between HRQOL dimensions GH (r = −0.487), SF (r = −0.272), RE (r = −0.362), MH (r = −0.392) and FIQ (r = 0.230). Social support was significantly correlated with BP (r = 0.298), GH (r = 0.260), VT (r = 0.256), SF (r = 0.456), RE (r = 0.300), MH (r = 0.307) and FIQ (r = −0.403).
Finally the multivariate analysis revealed that among dimensions of SF-36 and FIQ, the pain felt last week was a significant predictor of HRQOL (SF-36 + FIQ) because it expressed associations with all dimensions excepting RE. Morning stiffness predicted a worst HRQOL assessed by the FIQ. Both the pharmacological treatment and the number of medical/emergency rooms visits were significant predictors for the PF dimension. Depression symptoms were a significant predictor of a higher impact on VT and MH and of higher scores on FIQ. Anxiety symptoms were significant predictors of a worst GH, SF, RE and MH. Emotion-focused coping was a predictor of a worst GH and RE. At last, social support was only a significant predictor of a better SF (Table 3).
The clinical and psychological variables analysed explained an acceptable proportion of variability (R 2), ranging from 31.3% on RE to 70.6% on FIQ. The percentage of explained variance, in all cases, exceeded 25%, the minimum to consider the model an acceptable one [36]. The exception occurred in RP with 6.10% of explained variance, presenting an unacceptable model, indicating that the variance of this dimension on HRQOL may be better explained by other variables that were not considered in this study. The results of regression analysis are presented in Table 3.
Discussion
The data reported in this study indicate that FM has a negative impact on both general and specific dimensions that comprise HRQOL, with particular focus on physical dimensions. Pain intensity and anxiety and depression symptoms are the most relevant explanatory variables of the impact of FM on HRQOL.
In this study, and in accordance with previous findings, people with FM have a remarkably consistent pattern of health status impairment marked by deterioration in physical, psychological and social well-being [8, 13, 15, 16]. The FIQ results are close to the threshold of 70 points (68.59) considered severely affected cases [9], and it is higher than in preceding studies showing scores ranging from 42.30 [37] to 63.60 [9]. Similarly, the percentage of patients with scores ≥70 is high (52.63%) and higher than recently reported in a Spanish sample of 214 FM patients (♂ = 17; ♀ = 197) by Ubago et al. [9] who estimated a percentage of 41.60%. Socio-demographic characteristics, health care systems and other conditions may differ from country to country, and this may explain the differences found. However, since we have no previous data on Portuguese population to compare, this aspect should be evaluated in subsequent studies.
According to the SF-36 results, all aspects related to quality of life analysed in this sample of female patients with FM are severely impaired when compared to general female population, so the multiple aspects that encompass the HRQOL in FM need to be further explored [13]. FM female patients experienced the maximum influence of their disease on physical dimensions, particularly on PF, RP, GH and BP, which is consistent with data reported in the literature [13, 14, 16, 38]. Our findings are also consistent with those of Hoffman and Dukes [39] who reviewed 34 studies and reported that patients with FM had 2 SD below the average for the Physical Component (our standardized score ranges between −2.42 on PF and −1.59 on BP) and 1 SD below average on Mental Component (our standardized score ranges between −1.55 on VT and −1.23 on MH), when compared with the general population.
The characteristics associated with higher impact are clinical and psychological variables. Of all aspects analysed, pain intensity is the most important and explanatory variable, and it is the only one that shows significant correlations with all dimensions of quality of life collected on the SF-36 (except RE) and on FIQ, which marks the important role that pain experienced last week serves as the predictor variable for the quality of life in patients with FM. These results seem expected since the main symptom in FM is diffuse and chronic pain, and it is in accordance with the results reported in the literature [7, 8, 11].
It was also found that receiving pharmacological treatment is associated with lower levels of generic HRQOL on the dimension PF. Although this result may seem surprising, it coincides with results previously reported by Ubago et al. [9] that pointed to higher FIQ scores (worse HRQOL) in patients that were receiving pharmaceuticals. According to these authors, the inherent complexity of the therapeutic treatment for FM, with its many symptoms and interactions between drugs, could explain this apparent contradiction. Furthermore, in the study by Ubago et al., patients receiving non-pharmacological treatment obtained a lower FIQ score (better HRQOL) than those who did not, although in this case it has shown no significant differences. These findings coincide with recent results on the beneficial effects of these alternative therapies [40]. Alternatively, it is possible that patients with higher intensity symptoms (and therefore with major impact on their HRQOL) will seek medical advice from their doctor who will prescribe pharmacological treatment.
The psychological variables also play a key role on HRQOL particularly on the mental component of SF-36 and on FIQ. Anxiety and depression symptoms appear as explanatory variables of the Mental Component on HRQOL (VT, SF, RE and MH), although anxiety is also associated with GH, while depression relates significantly with the impact of this illness measured by the FIQ, showing similar results to those reported by previous studies [8, 11, 14, 16]. Dobkin et al. [41] had already assessed the psychological distress and reported that it was an important predictor of HRQOL, on both a longitudinal and a transversal analysis, which is consistent with our cross-sectional analysis.
When examining the coping strategies, only the emotion-focused coping is related to the HRQOL. In this study, after controlling clinical and psychological variables, it was found that the emotion-focused coping is significantly and positively related with the GH and RE, which is consistent with the results reported by Nicassio et al. [42] who found that patients who exhibit less active coping had higher quality of life. Nicassio et al. postulated that active coping exacerbated muscular or other psychological mechanisms that might contribute to FM pain. Regarding this, it is worth mentioning that coping styles are not inherently good or bad. For example, distraction may be more efficient when a stressor (e.g. illness) is considered easy to control [43]. According to Melding [44], it can be hypothesized that the problem-focused strategies are more adaptive in groups of patients whose perception of pain control is higher and their perception of pain is lower, while emotion coping strategies may be more adaptive in patients with FM who have a higher perception of pain and are less likely to control it. Thus, one possible explanation for these findings may be that given the high degree of pain presented by this sample, the coping strategies focused on emotions would be presented as adaptive as the control of pain and its intensity seems to be beyond reach of patients.
When analysing the relationship between social support and HRQOL, we observed a significant and positive relationship between ESSS Total Score and SF (after control of clinical and psychological variables), which is consistent with the literature [9, 17].
The significant relationship observed between psychological variables and HRQOL in patients with FM suggests that when treating FM a broad therapeutic approach should be applied, taking into account the non-physical symptoms such as anxiety and depression and other psychological variables such as coping strategies and social support that are related to the effects of FM on HRQOL. Identifying factors that determine the extent of its impact will allow the design of more effective therapeutic strategies.
However, while considering this data the limitations of the study should be taken into account. Firstly, there were a limited number of patients, and all of them were women. Since the data from some studies suggest that as far as gender is concerned the profile and degree of impairment could be different in men [14], future studies should include larger populations of both sexes. Secondly, it is necessary to take into account that the data corresponds to a sample of Portuguese female patients with FM, and its extrapolation to other populations should be made with caution, since patients’ socio-demographic characteristics, health care systems and other conditions may vary in different countries. Finally, considering the cross-sectional design of this study, interrelations among factors studied can be extracted [45], but no causal relations can be established from this data.
To sum up, the data from our study shows that FM has a negative impact on the HRQOL with particular emphasis on physical dimensions. Pain intensity and anxiety/depression symptoms and emotion-focused coping are the most relevant explanatory variables of the impact of FM on HRQOL.
References
Carmona L, Ballina J, Gabriel R, Laffon A (2001) The burden of musculoskeletal diseases in the general population of Spain: results from a national survey. Ann Rheum Dis 60:1040–1045
Goldenberg DL (2003) Fibromyalgia and related syndrome. In: Hochberg M, Silman A, Smolen J, Weinblatt ME, Weisman MH (eds) Rheumatology, 3rd edn. Mosby, London, pp 701–712
Woolf AD (2000) The Bone and Joint Decade 2000–2010. Ann Rheum Dis 59:81–82
Buskila D, Neumann L, Alhoashle A, Abu-Shakra M (2000) Fibromyalgia syndrome in men. Semin Arthritis Rheum 30:47–51
Reisine S, Fifield J, Walsh S, Feinn R (2003) Do employment and family work affect the health status of women with fibromyalgia? J Rheumatol 30:2045–2053
Reisine S, Fifield J, Walsh S, Dauser D (2004) Employment and quality of life outcomes among women with fibromyalgia compared to healthy controls. Women Health 39:1–19
Soucase B, Monsalve V, Sriano JF, Andrés J (2004) Estrategias de afrontamiento ante el dolor y calidad de vida en pacientes diagnosticados de fibromialgia. Rev Soc Esp Dol 11:353–359
Tander B, Cengiz K, Alayli G, Tlhanli I, Canturk F (2008) A comparative evaluation of health-related quality of life and depression in patients with fibromyalgia syndrome and rheumatic arthritis. Rheumatol Int 28:859–865
Ubago L, Ruiz-Pérez I, Pérez MB, Labry-Lima AO, Hernández-Torres E, Pazaola-Castaño J (2008) Analysis of the impact of fibromyalgia on quality of life: associated factors. Clin Rheumatol 27:613–619
Yunus MB (2001) The role of gender in fibromyalgia syndrome. Curr Rheumatol Rep 3:128–134
Neumann L, Dudnik Y, Bolotin A, Buskila D (1999) Evaluation of a Hebrew version of the revised and expanded arthritis impact measurement scales (AIMS2) in patients with fibromyalgia. J Rheumatol 26:1816–1821
Wolfe F, Anderson J, Harkness D, Bennett RM, Caro XJ, Goldenberg DL et al (1997) Health status and disease severity in fibromyalgia: results of a six-center longitudinal study. Arthritis Rheum 40:1571–1579
Birtane M, Uzunca K, Tastekin N, Tuna H (2007) The evaluation of quality of life in fibromyalgia syndrome: a comparison with rheumatoid arthritis by using Sf-36 health survey. Clin Rheumatol 36:679–684
Neumann L, Berzak A, Buskila D (2000) Measuring health status in Israeli patients with fibromyalgia syndrome and widespread pain and health individuals: utility of the short-form 36-item health survey (SF-36). Semin Arthritis Rheum 29:400–408
Theadom A, Cropley M, Humphrey K (2007) Exploring the role of sleep and coping in quality of life in fibromyalgia. J Psychol Res 62:145–151
Tüzün EH, Albayrak G, Eker L, Sözay S, Daskapan A (2004) A comparison study of quality of life in women with fibromyalgia and myofascial pain syndrome. Dis Rehab 26:198–202
Schoofs N, Bambini D, Ronning P, Bielak E, Woehl J (2004) Death of a lifestyle: the effects of social support and health care support on the quality of life of persons with fibromyalgia and chronic fatigue syndrome. Orthop Nurs 23:364–374
Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL et al (1990) The American College of Rheumatology (1990) criteria for the classification of fibromyalgia. Arthritis Rheum 33:160–172
Pais-Ribeiro JL, Silva I, Ferreira T, Martins A, Meneses R, Baltar M (2007) Validation study of a Portuguese version of the Hospital Anxiety and Depression Scale. Psychol Health Med 12:225–237
Zigmond AS, Snaith RP (1983) The hospital anxiety and depression scale. Psych Scand 67:361–370
Snaith RP, Zigmond AS (1994) HADS: Hospital Anxiety and Depression Scale. NFER, Windsor
Carver CS (1997) You want to measure coping but your protocol’s too long: consider the brief cope. Int J Behav Med 4:92–100
Pais-Ribeiro JL, Rodrigues AP (2004) Questões acerca do coping: a propósito do estudo de adaptação do Brief Cope. Psic Sau Doen 5:3–15
Coolidge FL, Segal DL, Hook JN, Stewart S (2000) Personality disorders and coping among anxious older adults. J Anx Dis 14:157–172
Pais-Ribeiro JL (1999) Escala de Satisfação com o Suporte Social. Anál Psic 3:547–558
Pais-Ribeiro JL (2005) O importante é a saúde: estudo de adaptação de uma técnica de avaliação do estado de saúde SF-36. Fundação Merck, Lisboa
Ware JE, Sherbourne CD (1992) The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Car 30:473–483
Burckhardt CS, Clark SR, Bennett RM (1991) The fibromyalgia impact questionnaire: development and validation. J Rheumatol 18:728–733
Rosado ML, Pereira JP, Fonseca JP, Branco JC (2006) Adaptação cultural e validação do Fibromyalgia Impact Questionnaire—versão portuguesa. Reumat Port 31:157–165
Martin CR, Thompson DR (2000) A psychometric evaluation of the Hospital Anxiety and Depression Scale in coronary care patients following myocardial infarction. Psychol Health Med 5:193–202
Cooper C, Katona C, Orrell M, Livingston G (2006) Coping strategies and anxiety in caregivers of people with Alzheimer’s disease: the LASER-AD study. J Affect Disord 90:15–20
Fuh JL, Wang SJ, Lu SR, Juang KD, Lee SJ (2000) Psychometric evaluation of a Chinese (Taiwanese) version of the SF-36 health survey amongst middle-aged women from a rural community. Qual Lif Res 9:675–683
Bennett R (2005) The Fibromyalgia Impact Questionnaire: a review of its development, current version, operating characteristics and uses. Clin Exp Rheumatol 23:S154–S162
Nunnally J, Bernstein I (1994) Psychometric theory, 3rd edn. McGraw Hill, New York
Ware JE, Snow KK, Kosinski M, Grandek B (1993) SF-36 health survey manual and interpretation guide. The Health Institute of New England Medical Center, Boston
Abraira V, Pérez de Vargas AM (1996) Método Multivariante en Bioestadística. Editorial Centro de Estudios Ramón Areces, Madrid
Zijlstra TR, Van de Laar MA, Bernelot HJ, Taal E, Zakraoui L, Rasker JJ (2005) Spa treatment for primary fibromyalgia syndrome: a combination of thalassotherapy, exercise and patient education improves symptoms and quality of life. Rheumatology 44:539–546
Martinez JE, Barauna-Filho IS, Kubokawa K, Pedreira IS, Machado LA, Cevasco G (2001) Evaluation of the quality of life in Brazilian women with fibromyalgia, through the medical outcome survey 36 item short-form study. Disabil Rehabil 23:64–68
Hoffman DL, Dukes EM (2008) The health status burden of people with fibromyalgia: a review of studies that assessed health status with the SF-36 or the SF-12. Int J Clin Pract 62:115–126
Martin DP, Sletten CD, Williams BA, Berger IH (2006) Improvement in fibromyalgia symptoms with acupuncture: results of a randomized controlled trial. Mayo Clin Proc 81:749–757
Dobkin PL, De Civita M, Abrahamowicz M, Baron M, Bernatsky S (2006) Predictors of health in women with fibromyalgia: a prospective study. Int J Behav Med 13:101–108
Nicassio PM, Schoenfeld-Smith K, Radojevic V, Schuman C (1995) Pain coping mechanisms in fibromyalgia: relationship to pain and functional outcomes. J Rheumatol 22:1552–1558
Endler NS, Parker JDA, Summerfeldt LJ (1998) Coping with health problems: developing a reliable and valid multidimensional measure. Psychol Assess 10:195–205
Melding PS (1995) How do older people respond to chronic pain? A review of coping with pain and illness in elders. Pain Rev 2:65–75
Goldenberg DL (1999) Fibromyalgia syndrome a decade later: what have we learned? Arch Int Med 159:777–785
Disclosures
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article can be found at http://dx.doi.org/10.1007/s10067-011-1904-1.
Rights and permissions
About this article
Cite this article
Campos, R.P., Vázquez, M.I.R. Health-related quality of life in women with fibromyalgia: clinical and psychological factors associated. Clin Rheumatol 31, 347–355 (2012). https://doi.org/10.1007/s10067-011-1870-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-011-1870-7