
Abstract
The aim of the study was to evaluate factors that influence health status and work disability in patients with ankylosing spondylitis (AS) in the Czech Republic. Data were collected in a retrospective fashion directly from patients with AS using mailed questionnaires containing questions regarding sociodemographic characteristics of patients, the course of their disease, therapy, rehabilitation, quality of life, and ability to work. HAQ-DI (Health Assessment Questionnaire-Disability Index) and BASDAI (Bath Ankylosing Spondylitis Disease Activity Index) were also included in the questionnaires; 1,008 questionnaires were suitable for further statistical analysis. The average age ± SD of patients was 50.2 ± 10.7 years, the average symptom duration was 23.0 ± 11.6 years. Mean time from first symptoms to diagnosis was 9.1 years. Full disability had been awarded to 303 patients (30%) at some point of their disease. Twenty seven percent of patients reported receiving full disability pension for 10 or more years. Four hundred fifty six subjects (45%) were currently or had been previously receiving partial disability pension. Receiving disability pension was more frequent among men (64%) compared to women (56%) (P = 0.012), despite the fact that women had higher BASDAI (P < 0.001) and HAQ-DI (P = 0.004) scores. Patients with a family history of AS had higher BASDAI and HAQ-DI scores (P = 0.001 and P = 0.008, respectively) compared to patients without a family history of AS. BASDAI and HAQ-DI scores correlated with age and duration of illness, younger patients and those with shorter disease duration had lower values. Fifty eight percent of patients reported a BASDAI score ≥4 (current cutoff value for initiation of biological therapy), but only 1% of patients were treated by anti TNF alpha agents within the last year. Seven hundred ninety one patients underwent spa treatment in the previous year; 96% of them experienced improvement of their health condition.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ankylosing spondylitis (AS) is a chronic progressive inflammatory disease, predominantly affecting the sacroiliac joints and spine, with possible involvement of other joints, entheses, and extra-articular structures. The disease is accompanied by pain, joint stiffness, and progressive loss of spine mobility which may result in severe functional impairment. The pain, limitation of function and presence of organ involvement all contribute to worsening of patients quality of life. Socioeconomic consequences also play an important role since the disease often leads to work disability [1–8].
The rate at which functional disability worsens during the lifetime of a given patient with ankylosing spondylitis fluctuates and there is a significant variability of progression rate between affected individuals as well [9–12]. Assessment of risk factors for the development of functional limitation is a crucial process that allows identification of patients at risk and therefore early initiation of therapy. Functional disability generally worsens with age and longer symptom duration [1, 9–12]. Additional risk factors for more severe functional limitation are the level of pain and stiffness, presence of peripheral arthritis, history of total joint replacement surgery, and smoking [11, 13–15]. Results of previous studies are conflicting with regard to the influence of gender, family history of AS, and home exercise on severity of AS [9–12, 14, 16, 17]. Differences in the results of individual studies might be partially explained by heterogenity of patient groups studied, with the current socioeconomic status being an important factor. For example, in a German study evaluating disability and handicap in patients with rheumatoid arthritis (RA) and AS between years 1993–1999, disability of patients from regions of the former East Germany was 2.38 times higher when compared to patients from the former West Germany [10]. Another study demonstrated 1.54 times higher incidence of work disability in a Dutch cohort compared to patients with AS from France and Belgium [6]. Recent studies have shown that quality of life of patients with AS is influenced not only by physical aspects of the disease but also by psychological factors and the level of education [18–22].
The goal of our study was to assess factors affecting functional disability, quality of life, and social impact of ankylosing spondylitis on patients from the Czech Republic, as perceived by patients themselves. The original idea of the study was proposed by the Bechterew Disease Patients Club (BC), an organization associating more than 1,800 patients with ankylosing spondylitis (i.e., Bechterew disease) from the Czech Republic. BC is a not-for-profit organization aimed at improving lives of patients suffering from AS. Members of the BC are patients diagnosed with ankylosing spondylitis by a specialist based on the 1984 modified New York criteria [28]. We cannot exclude the possibility that some BC members did not fulfill the classification criteria completely, however membership in the BC is usually suggested by a rheumatologist after diagnosis of AS was made and therefore there should be no members without AS or with a different medical diagnosis. Prevalence of AS in the Czech Republic (population of 10 million) is estimated at 0.1% [23], therefore we can assume that every fifth patient with the disease is a member of this patient organization.
Patients and methods
We performed a cross-sectional study, in which data were collected directly from patients with ankylosing spondylitis in the form of questionnaires. The project was conceived and coordinated by the representatives of patients' organization (BC) in cooperation with specialists—rheumatologists who participated in formulation of the questionnaire and its final approval. Validated Czech language versions of standardized questionnaires were used [24]. Data processing and final analysis was performed at the Institute of Biostatistics and Analysis of Masaryk University in Brno.
The questionnaire contained questions regarding sociodemographic characteristics of patients, medical history and course of the disease, type of follow-up and therapy, rehabilitation, quality of life, and current health status. Factors influencing quality of life were analyzed. The questionnaire also contained questions probing how well patients are informed about the nature of their disease and about available treatment modalities. HAQ-DI (Health Assessment Questionnaire-Disability Index) [25] and BASDAI (Bath Ankylosing Spondylitis Disease Activity Index) [26] were also included in the questionnaire.
Possible risk factors influencing the health condition and quality of life in patients with AS evaluated in the study were: age, gender, symptom duration and time from diagnosis, disability and its duration, duration and type of pharmacotherapy, occurrence of drug side effects, engagement in sports and physical rehabilitation, spa treatment, and family history of AS (defined as occurrence of AS in parents or children). We were also curious as to how many patients had BASDAI scores of ≥4 and therefore fulfilled the criteria for initiation of biological therapy [27].
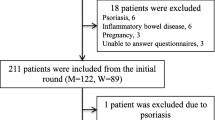
A total of 1,710 questionnaires with accompanying commentary and instructions were mailed to individual BC members from the national headquarters in 2005. One thousand two hundred twelve (70%) subjects returned completed questionnaires, of which 1,008 (59%) were suitable for further statistical analysis. Participation in the survey was voluntary and there were no additional steps employed to convince the initial non-responders to participate. Possible differences between responders and non-responders were not sought. In addition, not all the data were available in all questionnaires. Sample size for individual parameters is therefore recorded as N in descriptive tables.
Statistical methods
Data characterizing the patients, such as age, symptom duration, time since diagnosis of AS and duration of disability were collected from patients in the form of interval estimates and not as specific numeric values. For the purpose of statistical analysis, the estimates were replaced by the mean value of the given interval.
Considering a not-normal distribution of age, symptom duration, time to diagnosis, HAQ-DI, and BASDAI scores, nonparametric Mann–Whitney U test was used to compare values between two groups of patients. When more groups were compared, nonparametric Kruskall–Wallis test followed by multiple comparisons was used to identify pairs of groups with significant differences. Relationship between HAQ-DI and BASDAI scores was ascertained by means of Spearman rank correlation. The independence of categorical variables was tested by mean of χ 2 goodness-of-fit test.
Principal component analysis was used to find out relationships among such factors as age, symptom duration, sex, disability, sport participation, AS in family, and BASDAI and HAQ-DI. With the aim to find out the effect of all factors on BASDAI and HAQ-DI score, these two variables were included in the analysis as supplementary—not active—variables.
Results
Sociodemographic characteristics of patient population
Basic characteristics of subjects are recorded in Tables 1 and 2. Fifty six percent of patients were older than 50 years; only 4% of patients were younger than 30 years. Fifty one percent of patients experienced their first symptoms between 20–30 years of age. Eight hundred thirty four (83%) patients had children. Patient's father was affected in 96 instances, mother in 45 and five patients reported AS in both parents. Out of 126 subjects whose parents had AS and who themselves had children, 42 (33%) had children with AS. The incidence of AS in children of patients whose parents were not affected by the disease (n = 708) was lower with only 100 cases (14%; P < 0.001).
Disability, physical handicap certification
Physical handicap certificate is an official document issued by local authorities which entitles its holder to certain privileges. Full and partial disability pension is provided to patients by the state government and is based on the degree of disability. The mean duration of physical handicap certification was 6.9 years. Full disability at present time or in the past had been awarded to 303 patients (30%). Twenty seven percent of patients report receiving full disability pension for 10 or more years. Duration of symptoms in patients who were awarded full or partial disability pension (median 25 years) was longer than in patients who were not receiving disability pension (median 20 years; Mann–Whitney U test: U = 82,616.5, N = 972, P < 0.001). Receiving full or partial disability pension was more frequent among men (64%) than in women (56%). This difference was statistically significant (χ 2 goodness-of-fit test, χ 2 = 6.315, df = 1, P = 0.012).
Treatment of AS
Characteristics of treatment, rehabilitation and physical therapy are recorded in Table 1. In the majority of cases (78%), the medication was being prescribed by a rheumatologist, in 16% of cases by a general practitioner, in 3% by an orthopedic surgeon and in the remaining 3%, by another specialist. Most patients (77%) were taking NSAIDs. The questionnaire unfortunately did not discern between regular and on-demand use of NSAIDs. Previous or current use of sulfasalazine was reported by 158 patients (16%). Ten patients (1%) were currently receiving anti TNF alpha agents. Adverse effects of therapy were experienced by 383 subjects (43%). Seventy one percent of subjects stated that they had been informed about possible side effects of treatments used. Alternative therapies, defined as treatment other than drugs and rehabilitation, were tried by 220 subjects (22%), symptomatic relief was noted in 127 cases (58%) and most patients rated the treatment effect favorably.
Physical activity, rehabilitation, spa treatment
Forty nine percent of subjects did not participate in any sport; 81% of subjects were exercising at home, in most instances (76%) for less than 30 min daily; and 69% of subjects were exercising on individual basis, without the guidance of a physiotherapist. Improvement of health condition after spa treatment was experienced by 755 subjects (96%), and in 62% of them, the effect lasted for more than 6 months.
Blood tests
Seven hundred eighty one subjects (78%) had regular blood tests, but most of them (73%) were not aware of reasons for which the tests were being done.
Use of health devices
Forty seven percent of subjects were not using any health devices, one device was used by 22% of subjects, two devices by 14% of subjects and three or more devices were used by 17% of patients. The most commonly used health device was a bathtub handle (30%), devices to aid with dressing were used by 28% of subjects and a cane or crutches were used by 15% of patients.
Help of another person
Thirty eight percent of 1,008 subjects stated that they rely on the help of others, most commonly to reach for objects (22%). Sixteen percent of patients need help of another person during errands and household chores, 12% need help to squeeze or to open something, 12% of patients need help during dressing and self-care, and 7% of subjects require assistance during personal hygiene.
BASDAI score was calculated in 939 patients. Mean value of BASDAI score was 4.5. Fifty eight percent (n = 544) of subjects had BASDAI ≥ 4. BASDAI scores in relation to age, gender, duration of symptoms, disability physical activity, physical therapy, and family history of AS are recorded in Table 3. There was a significant difference between BASDAI scores of patients with symptom duration of less than 10 years when compared to patients with symptom duration of 21–30 years. Differences between other age groups were not statistically significant.
HAQ-DI questionnaire was completed by 901 subjects. Mean HAQ-DI value was 0.9. HAQ-DI score and its association with gender, age, symptom duration, disability, physical handicap certification, exercise, physical activity and participation in physical rehabilitation, and spa treatment is recorded in Table 4.
Correlation of HAQ-DI and BASDAI
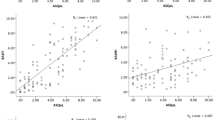
The correlation between HAQ score and BASDAI score was positive and highly significant (r s = 0.597, P < 0.001). Both BASDAI and HAQ-DI scores correlated positively with age, symptom duration, and disability; there was negative correlation with sport participation (see PCA ordination diagram; Fig. 1).

First two principal components (PCA1 = 29.4%, PCA2 = 19.3%) of multivariate analysis of factors related to AS. BASDAI and HAQ-DI score are included as supplementary variables. Patients with BASDAI < 4 are represented by a solid line; patients with BASDAI ≥ 4 represented by a dashed line
Patient characteristics and disease status in relation to disability
The correlation between age, symptom duration, time from first symptoms to diagnosis and full disability is shown in Table 5. The proportion of patients engaged in sports was significantly higher among patients who were not on full disability (38% vs. 25%, Х 2 = 15.940, df = 1, P < 0.001). On the other hand, patients who were on full disability were exercising at home more often (87% vs. 80%, Х 2 = 5.688, df = 1, P = 0.017). The strong negative relationship between sport and disability is obvious also in the PCA ordination diagram (Fig. 1).
Discussion
We are reporting results of a descriptive analysis of patients suffering from ankylosing spondylitis from the Czech Republic. The goal of the current study was to evaluate factors influencing disability, quality of life, and social consequences of the disease on patients themselves. This is the first study of such a scale ever performed in the Czech Republic which maps the characteristics of AS and some aspects of patient's lives. To our knowledge, a similar detailed analysis has not been performed in any of the former Eastern block countries. It has been shown that quality of life is influenced, among others, by mental aspects of health and that an important role is played by the health care system in a given country and the chance of success on the job market [10, 29]. The average duration of time from first symptoms to diagnosis in our cohort was 9.3 years [30–31], this finding is similar to results of surveys from other countries. Full disability had been awarded to 30% of Czech patients with AS at some point of their disease. Not surprisingly, the symptom duration of patients who were awarded full or partial disability pension was longer compared to non-disabled patients. Full or partial disability pension was more prevalent among men compared to women. BASDAI and HAQ-DI scores correlated with age and duration of illness, younger patients and those with shorter duration of illness had lower values. After detailed analysis, it becomes clear that BASDAI scores were increasing with age only up to 60 years of age, while in older patients, the scores were lower again. This observation may reflect the fact that disease activity tends to burn out in older patients. The BASDAI scores may also be influenced by presence of mechanical back pain which is undoubtedly prevalent in the subgroup of middle-aged patients. The HAQ-DI scores, which reflect disability, on the other hand, were increasing with age in all age groups. There was a significant positive correlation between BASDAI and HAQ-DI scores in the comprehensive analysis.
The leading opinion in the past was that AS in contrast to RA has less influence on the quality of life and ability to work since patients with AS retain their functional ability longer and are therefore able to keep a paid job. Recent studies however have shown that after adjustment for age, patients with RA and AS have similar levels of disability, pain, and quality of life impairment [5, 10]. Patients with AS are employed somewhat more frequently in comparison with patients with RA, this difference increases with the duration of illness [32]. An important predictor of employment is the general level of unemployment in individual countries [32] and availability of unemployment benefits. Previous studies have documented significant geographical differences in the employment rates of patients with AS. After the mean duration of illness of 12 years, 34–96% of subjects keep a paid job [1, 10, 33]. In a Danish cohort, after 20 years of illness, one third of patients with AS were no longer able to work [33], while 36% of French with AS were not working after 20 years (34%) [34]. In contrast, in the USA, only 13% of patients were not working after the mean duration of illness of 21.4 years [35]. There has been no study of employment rates of patients with AS in the Czech Republic until now. A cohort from Slovakia has described in the past in which 28.8% of AS patients in productive age were receiving full disability pension [36]. In our survey, 30% of subjects were fully disabled and 45% of patients were currently, or had been in the past, receiving partial disability pension. However, the data were not adjusted to gender or age and were not compared to the general population. Unfortunately, the level of education and the type of work, two factors which were shown to influence employment level of patients with AS [3, 33], were also not recorded. Data from our study regarding number of patients with AS receiving partial disability benefits is very different when compared for example to data from a German study in which partial disability in patients with AS, especially among men, was very uncommon [32]. A low number of patients receiving partial disability pension in Germany is given by the social system and job market, which, only in rare instances, part-time employment. The number of patients in our study receiving full disability benefits is higher when compared to data from Western Europe or USA.
In our cohort, patients receiving full disability benefits were older, with longer symptom duration, and longer time from first symptoms to diagnosis. These patients also had higher BASDAI and HAQ-DI scores, indicating more severe impairment. Patients who were not receiving full disability pension were more often engaged in sports while patients receiving full disability benefits exercised at home more often. In contrast to a study of Danish patients with AS [4], we have documented a relationship between the duration of illness and employment rate. A similar conclusion, i.e., that the degree of disability correlates with disease duration, has been reached by authors of older studies [37, 38] in which the employment rate after 20 years of AS was between 79 and 85% and after 30 years between 53 and 81%.
Some studies have shown that the degree of functional impairment in patients with family history of AS is the same when compared to sporadic cases of AS [12, 14]. In one study, patients with family history of AS had lower levels of functional impairment [39]; a finding that is discrepant with our results. In our cohort, the BASDAI and HAQ-DI scores were higher in patients with family history of AS. Questionnaires evaluating functional impairment in AS directly had not been used in this study. In agreement with other authors [10, 19, 40], we have also documented that while women recorded higher severity of symptoms of AS, it was paradoxically men who were receiving partial or full disability benefits more frequently [41].
Treatment of AS in the Czech Republic generally follows the ASAS recommendations [27]. The cornerstone of pharmacotherapy is NSAID; treatment with TNF alpha blockers is indicated for patients with high activity. In our cohort, 87% of subjects were taking drugs prescribed by a physician, mainly NSAIDs. Only 1% of Czech patients were currently treated with anti TNF alpha agents, significantly less compared to the average proportion of AS patients on biologics in the EU or USA [42]. This discrepancy is further highlighted by the fact that, unlike in RA, the role of traditional DMARDs in the treatment of AS is rather limited. Current efforts to increase the number of patients treated by anti TNF alpha agents in the Czech Republic are restrained mainly by the financial limits set by third party payers; therefore, physicians must select appropriate treatment candidates among patients with very high disease activity only.
Physical therapy has historically played an important role in the management of AS in the Czech Republic and is therefore well developed and organized. Spa treatment is very popular in the Czech Republic and the cost for AS patients with radiographic stage higher than I is covered by health insurance. Seventy nine percent of the total number of patients underwent spa treatment within the past year. A vast majority (88%) stayed in the spa for 4 weeks, which is the typical duration of treatment completely covered by health insurance. Despite limited data supporting its efficacy [43], 96% of patients in our cohort experienced improvement after spa treatment, which, in most cases, lasted longer than 6 months. However, the proportion of patients utilizing spa treatment might be higher among BC members compared to the general population since contact with others suffering from AS during a stay in the spa is one of the factors influencing the decision to join the BC.
We have documented that nearly 80% of AS patients were undergoing blood tests on a regular basis to monitor disease activity and treatment side effects, but 3/4 of patients were not aware of the reasons for which the tests were being performed. This finding may reflect a low level of patients' knowledge about their disease and at the same time may indicate significant deficiency in communication between patients and physicians. We have also documented a very limited level of awareness about the existence of anti TNF alpha agents (10% of patients). Since BC members have an undoubtedly more active approach to their disease, we presume that the level of knowledge about the disease and its treatment in general population is significantly lower than in our cohort.
One of the important findings of the study was the fact that only a very small proportion of patients is treated by anti TNF alpha therapy. In a recent international survey of practicing rheumatologists, a significant difference score between agreement with ASAS/EULAR recommendation regarding use of anti TNF alpha therapy and it's practical application was noted among Czech physicians (mean difference scores were below 1 for all European countries except UK; score for the Czech Republic was 2.7 ± 2.9). This reflects the fact that rheumatologists in the Czech republic do agree with the recommendation but frequently do not follow it in clinical practice mainly due to financial limits set by third party payers) [44].
Finally, the methodological limitations of our study have to be mentioned. Data were obtained from questionnaires completed by patients at home and mailed back on a voluntary basis; therefore, we had no means to verify the validity of the data we have worked with.
Another limitation is the fact that only members of the BC have been included in the evaluation which might be a source of a possible selection bias, since the membership by itself might be an indicator of a more active approach to the disease. It has been shown that self-reported health status is more strongly related to personality traits than to the degree of disability [45]. The questionnaire in our study did not contain questions targeting personality traits of patients directly. Therefore, the possible influence of this factor on the overall assessment of the health status of the subjects cannot be excluded. However, our questionnaire contained two internationally validated tools which record not only the activity of the disease but also the overall health status of patients. In addition, our questionnaire contained a wide array of questions which enable evaluation of the course of the disease, social situation, type of treatment, and the level of knowledge about ankylosing spondylitis.
A group of 1,008 patients with wide distribution-entailing age groups from childhood to those older than 60 years represents a sufficiently large and diverse cohort of patients with AS. We believe that the information obtained from questionnaires provides data not affected by a significant system error. We have documented that significant differences exist between our cohort and patients with AS from other countries in regard to the influence of risk factors, the degree of disability, and treatments used.
In accordance with previous reports we have documented existence of a significant delay of diagnosis and high prevalence of partial and full disability among patients with AS. Disability pension was awarded more frequently to patients with longer duration of symptoms and to men, despite the fact that women reported more severe disease symptoms. Higher BASDAI and HAQ-DI values were also recorded among patients with family history of AS. Our survey has shown that spa treatment is very popular among Czechs with AS and that it is associated with a significant and lasting effect in most cases. Very low number of patients was treated by anti TNF alpha agents, despite the fact that over 50% of subjects had BASDAI scores sufficiently high to fulfill criteria for initiation of this therapy.
References
Ward MM (1998) Quality of life in patients with ankylosing spondylitis. Rheum Dis Clin North Am 24:815–827
Boonen A, de Vet H, van der Heijde D, van der Linden S (2001) Work status and its determinants among patients with ankylosing spondylitis. A systematic literature review. J Rheumatol 28:1056–1062
Ward MM, Weisman MH, Davis JC Jr, Reveille JD (2005) Risk factors for functional limitations in patients with long-standing ankylosing spondylitis. Arthritis Rheum 53:710–717
Chorus AMJ, Boonen A, Miedema HS, Van Der Linden S (2002) Employment perspectives of patients with ankylosing spondylitis. Ann Rheum Dis 61:693–699
Chorus AM, Miedema HS, Boonen A, Van Der Linden S (2003) Quality of life and work in patients with rheumatoid arthritis and ankylosing spondylitis of working age. Ann Rheum Dis 62:1178–1184
Boonen A, van der Heijde D, Landewe R et al (2002) Work status and productivity costs due to ankylosing spondylitis: comparison of three European countries. Ann Rheum Dis 61:429–437
Boonen A, van der Heijde D, Landewe R et al (2003) Direct costs of ankylosing spondylitis and its determinants: an analysis among three European countries. Ann Rheum Dis 62:732–740
Boonen A, van der Heijde D, Landewe R et al (2003) Costs of ankylosing spondylitis in three European countries: the patient's perspective. Ann Rheum Dis 62:741–747
Taylor AL, Balakrishnan C, Calin A (1998) Reference centile charts for measures of disease activity, functional impairment, and metrology in ankylosing spondylitis. Arthritis Rheum 41:1119–1125
Zink A, Braun J, Listing J, Wollenhaupt J, German Collaborative Arthritis Centers (2000) Disability and handicap in rheumatoid arthritis and ankylosing spondylitis—results from the German rheumatological database. J Rheumatol 27:613–622
Ward MM (2002) Predictors of the progression of functional disability in patients with ankylosing spondylitis. J Rheumatol 29:1420–1425
Falkenbach A, Franke A, van der Linden S (2003) Factors associated with body function and disability in patients with ankylosing spondylitis: a cross-sectional study. J Rheumatol 30:2186–2192
Gran JT, Skomsvoll JF (1997) The outcome of ankylosing spondylitis: a study of 100 patients. Br J Rheumatol 36:766–771
Doran MF, Brophy S, MacKay K, Taylor G, Calin A (2003) Predictors of longterm outcome in ankylosing spondylitis. J Rheumatol 30:316–320
Averns HL, Oxtoby J, Taylor HG, Jones PW, Dziedzic K, Dawes PT (1996) Smoking and outcome in ankylosing spondylitis. Scand J Rheumatol 25:138–142
Ward MM (2002) Functional disability predicts total costs in patients with ankylosing spondylitis. Arthritis Rheum 46:223–231
Dagfinrud H, Mengshoel AM, Hagen KB, Loge JH, Kvien TK (2004) Health status of patients with ankylosing spondylitis: a comparison with the general population. Ann Rheum Dis 63:1605–1610
Dagfinrud H, Kjeken I, Mowinckel P, Hagen KB, Kvien TK (2005) Impact of functional impairment in ankylosing spondylitis: impairment, activity limitation, and participation restrictions. J Rheumatol 32:516–523
Dagfinrud H, Vollestad NK, Loge JH, Kvien TK, Mengshoel AM (2005) Fatigue in patients with ankylosing spondylitis: a comparison with the general population and associations with clinical and self-reported measures. Arthritis Rheum 53:5–11
Ozgul A, Peker F, Taskaynatan MA, Tan AK, Dincer K, Kalyon TA (2006) Effect of ankylosing spondylitis on health-related quality of life and different aspects of social life in young patients. Clin Rheumatol 25:168–174
Kobelt G, Andlin-Sobocki P, Maksymowych WP (2006) Costs and quality of life of patients with ankylosing spondylitis in Canada. J Rheumatol 33:289–295
Davis JC, van der Heijde D, Dougados M, Woolley JM (2005) Reductions in health-related quality of life in patients with ankylosing spondylitis and improvements with etanercept therapy. Arthritis Rheum 53:494–501
Hanova P, Pavelka K, Dostal C et al (2004) Incidence and prevalence of rheumatic diseases in a population based study in the Czech republic. Ann Rheum Dis 63(Suppl I):497–498
Sleglova O, Dusek L, Olejarova M et al (2004) Evaluation of status and quality of life in patients with ankylosing spondylitis—validation of Czech versions of Bath questionnaires—BAS-G, BASDAI and BASFI. Ces Revmatol 12:43–54
Fries JF (1980) Measurement of patients outcome in arthritis. Arthritis Rheum 23:137–145
Garrett S, Jenkinson T, Kennedy LG, Whitelock H, Gaisford P, Calin A (1994) A new approach to defining disease status in ankylosing spondylitis: the Bath Ankylosing Spondylitis Disease Activity Index. J Rheumatol 21:2286–2291
Zochling J, van der Heijde D, Burgos-Vargas R et al (2006) ASAS/EULAR recommendations for the management of ankylosing spondylitis. ‘ASsessment in AS’ International working group; European League Against Rheumatism Ann Rheum Dis 65(4):442–452
van der Linden S, Valkenburg HA, Cats A (1984) Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum 27:361–368
Fautrel B, Guillemin F (2002) Cost of illness studies in rheumatic diseases. Curr Opin Rheumatol 14:121–126
Mau W, Zeidler H, Mau R et al (1988) Clinical features and prognosis of patients with possible ankylosing spondylitis. Result of a 10-year followup. J Rheumatol 15:1109–1114
Feldtkeller E, Khan MA, van der Heijde D et al (2003) Age at disease onset and diagnosis delay in HLA-B27 negative vs. positive patients with ankylosing spondylitis. Rheumatol Int 23:61–66
Mau W, Listing J, Huscher D, Zeidler H, Zink A (2005) Employment across chronic inflammatory rheumatic diseases and comparison with the general population. J Rheumatol 32:721–728
Boonen A, Chorus A, Miedema H, van der Heijde D, Landewé R, Schouten H, van der Tempel H, van der Linden S (2001) Withdrawal from labour force due to work disability in patients with ankylosing spondylitis. Ann Rheum Dis 60:1033–1039
Guillemin F, Briancon S, Pourel J, Gaucher A (1990) Long-term disability and prolonged sick leaves as outcome measurements in ankylosing spondylitis. Possible predictive factors. Arthritis Rheum 33:1001–1006
Ward M, Kuzis S (2001) Risk factors for work disability in patients with ankylosing spondylitis. J Rheumatol 28:315–21
Urbanek T, Sitajova H, Hudakova G (1984) Problems of rheumatoid arthritis and ankylosing spondylitis in their labor and life enviroments. Czechoslovak Medicine 7:78–89
Lehtinen K (1981) Working ability of 76 patients with ankylosing spondylitis. Scand J Rheumatol 10:263–265
McGuigan LE, Hart HH, Gow PJ, Kidd BL, Grigor RR, Moore TE (1984) Employment in ankylosing spondylitis. Ann Rheum Dis 43:604–606
Calin A, Kennedy LG, Edmunds L, Will R (1993) Familial versus sporadic ankylosing spondylitis: two different diseases? Arthritis Rheum 36:676–681
Gran JT, Skomswoll JF (1997) The outcome of ankylosing spondylitis: a study of 100 patients. Br J Rheumatol 36:766–771
Boonen A, Chorus A, Miedema H, van der Heijde D, van der Tempel H, van der Linden S (2001) Employment, work disability, and work days lost in patients with ankylosing spondylitis: a cross sectional study of Dutch patients. Ann Rheum Dis 60:353–358
Ribbens C, Vastesaeger N, Brasseur J et al (2006) An epidemiological cross-sectional study of ankylosing spondylitis in Belgium: the ASPECT cohort. Ann Rheum Dis 65(SupplI):539
van Tubergen A, Landewe R, van der Heijde D et al (2001) Combined spa-exercise therapy is effective in patients with ankylosing spondylitis: a randomized controlled trial. Arthritis Rheum 45:430–438
Gossec L, Dougados M, Phillips C et al (2007) Dissemination and evaluation of the ASAS/EULAR recommendations for the management of Ankylosing Spondylitis: results of a study among 1,507 rheumatologists. Ann Rheum Dis (in press) Nov 29
Hidding A, de Witte L, van der Linden S (1994) Determinants of self-reported health status in ankylosing spondylitis. J Rheumatol 21:275–278
Acknowledgement
Supported by Research Project from Ministry of Health in the Czech Republic No: 000 000 23728
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Forejtová, Š., Mann, H., Štolfa, J. et al. Factors influencing health status and disability of patients with ankylosing spondylitis in the Czech Republic. Clin Rheumatol 27, 1005–1013 (2008). https://doi.org/10.1007/s10067-008-0845-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-008-0845-9