
Abstract
In the last two decades, migraine research has greatly advanced our current knowledge of the genetic contributions and the pathophysiology of this common and debilitating disorder. Nonetheless, this knowledge still needs to grow further and to translate into more effective treatments. To date, several genes involved in syndromic and monogenic forms of migraine have been identified, allowing the generation of animal models which have significantly contributed to current knowledge of the mechanisms underlying these rare forms of migraine. Common forms of migraine are instead posing a greater challenge, as they may most often stem from complex interactions between multiple common genetic variants, with environmental triggers. This paper reviews our current understanding of migraine genetics, moving from syndromic and monogenic forms to oligogenic/polygenic migraines most recently addressed with some success through genome-wide association studies. Methodological issues in study design and future perspectives opened by biomarker research will also be briefly addressed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Migraine is a complex neurological disorder, characterized by recurrent and severe attacks of headache, lasting from 4 to 72 h, with associated sensory and dysautonomic symptoms, such as nausea and vomiting, photophobia and phonophobia. Transient, focal neurological symptoms mostly involving the visual system occur prior to or during migraine attacks, a phenomenon known as “aura” affecting approximately 15–30 % of cases. Migraine is thus subdivided into two major categories, namely “migraine with aura” (MA) and “migraine without aura” (MO), in accordance with the classification criteria of the International Headache Society listed in Box 1 [1]. However, often a single patient suffers from both types of headache or switches from one category to the other during the course of the illness [1]. The prevalence of migraine is estimated at a striking 18 % in females and 6 % in males, making it one of the most common and frequently invalidating human disorders [2, 3]. Its peak incidence occurs between 25 and 55 years of age [2, 3].
Box 1: diagnostic criteria for headache disorders [1]. | |
Migraine with aura (MA) | Migraine without aura (MO) |
A. At least two attacks fulfilling criteria B and C B. One or more of the following fully reversible aura symptoms: 1. Visual 2. Sensory 3. Speech and/or language 4. Motor 5. Brainstem 6. Retinal C. At least two of the following four characteristics: 1. At least one aura symptom spreads gradually over ≥5 min, and/or two or more symptoms occur in succession 2. Each individual aura symptom lasts 5–60 min 3. At least one aura symptom is unilateral 4. The aura is accompanied, or followed within 60 min, by headache D. Not better accounted for by another ICHD-3 diagnosis, and transient ischaemic attack has been excluded | A. At least five attacks fulfilling criteria B–D B. Headache attacks lasting 4–72 h (untreated or unsuccessfully treated) C. Headache has at least two of the following four characteristics: 1. Unilateral location 2. Pulsating quality 3. Moderate or severe pain intensity 4. Aggravation by or causing avoidance of routine physical activity (e.g., walking or climbing stairs) D. During headache at least one of the following: 1. Nausea and/or vomiting 2. Photophobia and phonophobia E. Not better accounted for by another ICHD-3 diagnosis |
Migraine is viewed as a neurovascular disease caused by a primary brain dysfunction, leading to activation and sensitization of the trigeminovascular system and to the release of vasoactive neuropeptides. Cortical spreading depression (CSD), originating in the occipital region, is thought to represent the neurobiological underpinning of visual aura [4]. In animal models, CSD indeed activates the trigeminovascular system, triggering a series of cortical, meningeal, and brainstem events consistent with current knowledge about the pathophysiology of migraine attacks [4, 5].
Family and twin studies of migraine
The common observation that migraine tends to recur in families has long suggested that genetic factors may play a significant role in the disease. The existence and “relative weight” of genetic contributions to a complex disorder can be assessed using classical approaches, including family, twin, and adoption studies. To our knowledge, no adoption study of migraine has been published to this date. On the other hand, family and twin studies indicate that at least 50 % of patients have a first-degree relative affected by a similar condition [6–11]. Comparing familial recurrence rates with the above-mentioned incidence in the general population yields a relative risk (RR) estimated at 4.0 and 1.4 for MA and MO, respectively [10, 11]. Finally, several population-based twin studies have contrasted concordance rates for migraine between monozygotic (MZ) and dizygotic (DZ) twins to produce heritability estimates [6–8]. Mulder et al. [6] studied the prevalence and heritability of migraine in 29.717 twin pairs from six countries enrolled in Genome EUtwin Project [12]. This study did not distinguish between MA and MO, which were analyzed collectively [6]. The prevalence of migraine was highest (32–34 %) in Danish and Dutch women, and lowest (10–13 %) in Finland, a result compatible with shared environmental factors explaining a large proportion of variance. MZ concordance rates were 1.5–2.0 times higher than those recorded in DZ twins, with heritability estimated at 34–57 % (on average 50 %). Hence, both family and twin studies collectively support sizable genetic contributions to migraine pathogenesis.
The quest for single genes in migraine genetics research
Genetic contributions to any human disease can range from monogenic or oligogenic forms, due to rare or even “private” genetic variants endowed with high penetrance (i.e., phenotypic expression), to polygenic and multifactorial conditions stemming from complex epistatic interactions between multiple common genetic variants with low penetrance and small effect size, as well as from gene-environment interactions. In the latter framework, environmental factors can trigger the onset and progression of the disease by influencing epigenetic profiles directly regulating the expression of relevant genes, further increasing heterogeneity [13, 14]. In the case of migraine, higher RR rates and heritability estimates, as well as the results of molecular studies (see below), generally support greater contributions by rare variants to MA, whereas MO more frequently stems from multifactorial and polygenic mechanisms. Within the framework of gene-environment interactions, a significant role has been reliably demonstrated for several environmental factors, including female sex hormones, early and recent stress (such as low maternal care and short-lasting, intense stressful periods, respectively), decreased sensory thresholds for visual, auditory, and olfactory stimuli [13, 14]. Instead, a more controversial role has been hypothesized for weather and climate conditions, electromagnetic fields, smoking, pollution, and molds [13, 14]. An additional layer of complexity is conferred by the frequent association of migraine with other disorders, including anxiety, depression, ADHD, sleep disorders, epilepsy, as well as atopic and cardiovascular diseases [15, 16]. These comorbidities can conceivably stem from shared genetic and/or environmental underpinnings to a different extent in different patients [17, 18].
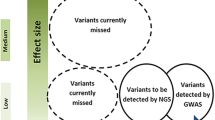
To this date, several approaches have been used to identify genetic variants either causing migraine or conferring vulnerability to the disease. The recent advent of array-based technologies and second-generation DNA sequencing has provided novel powerful tools to genetic analysis. In general, rare variants are sought by DNA sequencing in multigenerational families with many affected individuals. These studies were previously performed using a linkage approach, followed by refinement of the linkage region and targeted Sanger sequencing of candidate genes. While these approaches remain viable, whole-exome sequencing (WES) and whole-genome sequencing (WGS) can now significantly hasten the discovery of rare pathogenic variants with high penetrance. On the other hand, common variants have been typically sought using case–control or family-based association. SNP arrays now allow an unbiased search of common variants conferring disease vulnerability in large samples of cases and controls through genome-wide association studies (GWAS). Applying “classical” approaches, several forms of MA, such as familial hemiplegic migraine (FHM), have now been elucidated, with well-defined underlying causal variants identified and functionally tested. On the other hand, common forms of migraine are still less well understood at the genetic level.
We hereby review current molecular genetic evidence for MA and MO. The present work does not represent a systematic review but rather aims to (a) provide thorough coverage of this area of investigation, spanning syndromic migraines, rare monogenic forms, up to more recent GWAS data on common predisposing variants; (b) discuss methodological issues on experimental design, as pertaining to migraine genetics research; and (c) outline possible links between genetic findings and the underlying pathophysiology of migraine.
Syndromic migraines
Migraine can be part of known genetic disorders, displaying multiple manifestations and often involving various organs. The genetic syndromes most frequently associated with migraine are listed in Table 1. These disorders, though rare, may lead to a better comprehension of the mechanisms underlying more common forms of idiopathic migraine.
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is a genetic Mendelian disorder associated with strokes in adulthood. The onset of the disease is ambiguous and often characterized by migraine episodes associated with neurological symptoms or transient ischemic attacks (TIA), which anticipate strokes. The progression of the disease is a subcortical multi-infartual dementia. CADASIL is caused by mutations in NOTCH3, a highly conserved gene located in human chromosome 19q12, encoding for a transmembrane receptor expressed in the smooth muscle cells of small brain vessels [19]. This receptor protein consists in 2321 amino acids with an extracellular domain encompassing 34 EGF-like repeats hosting the vast majority (95 %) of CADASIL mutations described to date [19–24]. The prevalence of NOTCH3 mutations is approximately 4 per 100,000 adults and is probably underestimated [25, 26]. Mutations lead to a dysfunction of the signaling pathway that physiologically regulates vascular development during embryogenesis and maintains the structural/functional stability of blood vessels in adults [27, 28]. CADASIL may be caused by a vascular dysfunction resulting in increased pressure-induced vascular tone and a relative deficit in vasodilation. A specific characteristic of CADASIL is the accumulation of the NOTCH3 receptor due to its slow clearance, resulting in the formation of granular osmiophilic deposits: the effect on small vessels is decreased cell adhesion, cell loss, deposits, degeneration of smooth muscle cells in the middle layer, and fibrosis [29]. CADASIL migraine occurs typically with aura and its prevalence ranges between 0 and 40 % in studies performed to date [30]. The onset of migraine attacks in CADASIL typically occurs before 26 years of age; it is either concomitant to or can anticipate brain lesions, and females display an earlier onset of MA compared to males [31].
Mitochondrial encephalopathy, lactic acidosis, and stroke-like episodes
Mitochondrial encephalopathy, lactic acidosis, and stroke-like episodes (MELAS) is a disease caused by mutations in several mitochondrial genes, most frequently MTTL1 encoding for the mitochondrial tRNA for leucine (A to G transition at nucleotide 3243), and is characterized by epileptic seizures, stroke-like episodes, and lactic acidosis [32]. In particular, the typical presentation of MELAS includes epileptic seizures with radiologic evidence of cortical infarcts, often associated with migraine-like headaches; other clinical features include hemiparesis, hemianopsia, cortical blindness, episodic vomiting, and short stature. Systemic manifestations can include cardiac, renal, endocrine, gastrointestinal, and endothelial signs and symptoms. Ragged-red fibers are common, while a symptomatic myopathy is rare. It has been postulated that decreased brain oxidative metabolism may play an important role in the pathogenesis of migraine associated with MELAS [33].
Retinal vasculopathy and cerebral leukodystrophy
Retinal vasculopathy and cerebral leukodystrophy (RVCL) consolidates into a single autosomal dominant disease three neurovascular syndromes previously named hereditary vascular retinopathy (HVR), cerebroretinal vasculopathy (CRV), and hereditary endotheliopathy with retinopathy, nephropathy, and stroke (HERNS) [34]. These syndromes are all caused by mutations in the TREX1 gene, located on human chromosome 3p21, encoding for former DNase III (i.e., three prime repair exonuclease), an autonomous non-processive 3′–5′ DNA-specific exonuclease [35]. This enzyme, localized in the perinuclear region of the cell, plays a fundamental role in granzyme A-mediated cell death and, when mutated, in indirectly activating autoimmunity against undigested dsDNA from dying cells. RVCL-producing TREX1 mutations delete its carboxyl-terminus, leading to loss of cellular compartimentalization and widespread enzyme distribution in the presence of preserved exonuclease activity [36]. TREX1 mutations can also cause other disorders including Aicardi-Goutières syndrome, systemic lupus erythematosus, and familial chilblain lupus, through abnormal immune mechanisms [34].
Clinically, HVR is characterized by retinal microangiopathy, with microaneurysms and telangiectatic capillaries [37]. Its onset is typically in early adulthood, with disease progression yielding occlusion of large retinal arteries, proliferative arteriopathy, and avascular areas in the retinal periphery. Migraine is present in 70 % of HVR cases [37, 38]. CRV involves both the retina and the brain [34, 35]. Neuroimaging shows pseudo-tumors appearing as progressive subcortical contrast-enhancing lesions. Progressive visual loss is accompanied by neurological deficits, psychiatric symptoms, migraine, stroke, and death within 10 years of disease onset [34]. Instead, HERNS is a multi-infartual condition characterized by retinopathy, strokes, and nephropathy [39]. Capillary subendothelial basal membranes display a distinctive multilamination in brain, kidney, gastrointestinal tract, and other tissues [39]. Similarities between CRV and HERNS include pseudo-tumors, retinopathy, migraine-like headaches and neurological complications which may lead to death, while additional features may include psychiatric symptoms, dysarthria, hemiparesis, and apraxia [34, 39]. Finally, also the systemic variant of RVCL, hereditary systemic angiopathy, which shares with the RVCL spectrum many clinical features, including migraine-like headache, progressive neurological signs, and visual disturbances, has recently been shown to stem from TREX1 mutations, causing a C-terminal frameshift [40, 41].
COL4A1-related syndromes
COL4A1, located on human chromosome 13q34, encodes for the collagen type IV alpha-1 subunit. Mutations in this 52 exon-long gene can result in several autosomal dominant disorders with overlapping features, including perinatal hemorrhage with porencephaly [42–45] and a small vessel disease leading to hemorrhage and hemiparesis with infantile or adult onset [46]. The association of COLA4A1 mutations with migraine is not entirely certain. Although 10 of 52 COLA4A1 mutation carriers reported migraine with or without aura [45], the association is not entirely certain and could still represent a coincidental finding.
Familial anticipated sleep phase syndrome
Familial anticipated sleep phase syndrome (FASPS) is an autosomal dominant disorder characterized by persistent early evening sleep onset and early awakening [47]. Abnormal circadian rhythmicity results from a mutation in the circadian hPER2 gene (human period 2, on chromosome 2q37.3), within the casein kinase 1 (CK1)-binding domain of the hPer2 protein [48]. Furthermore, screening two families with MA and FASPS, Brennan et al. [49] have recently identified two missense mutations (T44A and H46R) in the gene encoding casein kinase 1δ (CK1δ), resulting in decreased enzyme activity. In addition to playing a pivotal role in the biology of circadian rhythms [50], in vivo and in vitro studies suggest that CK1δ may contribute to the pathogenesis of migraine. Mice carrying the CK1δ T44A mutation have a reduced threshold for cortical spreading depression accompanied by increased spontaneous and evoked calcium signaling in astrocytes [50].
Collectively, genetic studies of syndromic forms of migraine provide interesting leads toward the definition of the pathogenetic chain of events leading to the more common non-syndromic forms. In particular, CADASIL and RVCL provide further evidence supporting brain vascular tone dysregulation as an important contributor to the pathophysiology of migraine attacks, regardless of whether intrinsically generated or immune-mediated. Instead MELAS and FASPS point toward insufficient oxidative metabolism and abnormal circadian variation in cortical excitability, respectively, as possibly playing a role in specific subgroups of non-syndromic patients.
Monogenic forms of migraine
Familial hemiplegic migraine (FHM), is a rare monogenic subtype of migraine with motor aura (see Box 1 for general diagnostic criteria) displaying strong familiality compatible with an autosomal dominant transmission [51]. The overlap between FHM and common idiopathic migraine has thus suggested that the two forms may share common neurobiological underpinnings [52]. Despite its low incidence, FHM may thus represent an important genetic model to understand the molecular pathophysiology of common migraine. Mutation screening has revealed numerous genetic variants able to cause FHM (Table 2). Mutations in two ion channel genes, CACNA1A and SCN1A, as well as in ATP1A2 encoding the alpha2 subunit of the Na-K ATPase, cause FHM type 1, 3, and 2, respectively. De novo mutations affecting especially the latter two genes have also been reported in sporadic forms, devoid of a positive family history but clinically superimposable to FHM [53]. Furthermore, the pleiotropic effects especially of SCN1A mutations result in a variety of clinical phenotypes, including various forms of epilepsy, autism, and MA/MO without typical FHM-type aura, raising further interest in the pathophysiological overlap between FHM and sporadic forms of migraine [63–65]. Cellular and animal studies have revealed that mutated FHM genes are associated with altered ion homeostasis, cellular excitability, and neurotransmitter release; these abnormalities then predispose to the onset of cortical spreading depression (CSD), the electrophysiological underpinning of aura symptoms paving the path to migraine headache [4].
FHM type 1 is caused by missense mutations in the CACNA1A gene on chromosome 19p13 [54]. To date, at least 70 different causal missense mutations have been detected in this gene. Nonsense or missense mutations in CACNA1A are typically associated with episodic ataxia type 2 and FHM1, whereas a CAG triplet repeat expansion affecting the C-terminus causes spinocerebellar ataxia type 6, but rare cases with both FHM1 and cerebellar ataxia have also been reported [66, 67]. CACNA1A encodes the α1A subunit of the Cav2.1 (P/Q type) voltage-gated neuronal calcium channel, expressed throughout the central nervous system with highest density in the cerebellum [68, 69]. This subunit is involved in voltage sensitivity and mutations lead to increased Ca2+ influx into the neuron in response to smaller depolarizations. This, in turn, enhances the release of the excitatory neurotransmitter glutamate, because this channel is predominantly expressed presynaptically, where it couples membrane depolarization with neurotransmitter release [70]. Ultimately, transgenic mice harboring the human FHM1 R192Q or S218L (KI) mutation exhibit a lower threshold for CSD generation, increased CSD propagation velocity, and CSD extension into subcortical regions [71, 72]. Interestingly, female knock-in mice harboring these human mutations show significantly greater susceptibility to CSD compared to male carriers, which disappears after ovariectomy [73]. The regional distribution and functional role of this subunit explains why some FHM1 patients may also display cerebellar signs and episodic loss of consciousness.
FHM type 2 (FHM2) is associated with mutations in the ATP1A2 gene, located in human chromosome 1q21-q23 (Table 2). This gene encodes the α2 subunit of the Na+-K+ pump. FHM2 mutations blunt Na+-K+ ATPase activity and lower CSD threshold by (a) enhancing extracellular K+ concentrations and (b) reducing the electrochemical Na+ gradient required to drive astrocytic glutamate transporters, ultimately slowing the removal of extracellular glutamate and enhancing its concentration [51]. ATP1A2 mutations have also been very rarely encountered in basilar migraine and in common migraine, as well as in other neurological diseases, such as idiopathic cerebellar syndromes, benign familial infantile convulsions, epilepsy, alternating hemiplegia of childhood, and intellectual disability [55, 56].
FHM3 mutations are localized in the SCN1A gene, on human chromosome 2q24 [57]. This gene encodes for the α1 subunit of the neuronal voltage-gated sodium (Nav1.1) channel, which is primarily expressed in cortical neurons, where it plays an important role in the generation and propagation of action potentials. SCN1A mutations typically lead to hypersynchronous neuronal discharges resulting in seizures, autism, or migraine attacks, with either typical FHM course or appearing as sporadic MA or MO [63–65]. Data derived from a Nav1.1-knockout mouse model show that a loss of one allele predominantly decreased activity of GABAergic inhibitory interneurons, without affecting excitatory pyramidal neurons [74]. Indeed, several mutations in the SCN1A gene have also been associated with severe childhood epilepsy, such as generalized epilepsy with febrile seizures plus (GEFS+) and Dravet syndrome [75]. In contrast, mutations producing migraine only, such as Q1489K, display ambivalent effects whereby not only the rate of recovery from inactivation is accelerated, as in epileptogenic mutations, but also the transition from closed to the inactivated state of the channel, preventing neuronal discharges from becoming epileptogenic [58].
Other forms of typical FHM due to mutations in novel FHM candidate genes have been recently described (Table 2). Mutations resulting in an FHM phenotype have been identified in the PRRT2 (proline-rich transmembrane protein 2) gene, located on human chromosome 16p11 and encoding for an axonal protein associated with the exocytosis protein complex [59]. A mutation in the SLC4A4 gene, encoding for the Na+-HCO3 − cotransporter NBCe1, has been identified in two sisters with an FHM phenotype, renal tubular acidosis, and ocular abnormalities [60]. Finally, missense mutations located in the SLC1A3 gene, encoding the glial glutamate cotransporter EAAT1, have been found to cause episodic ataxia, migraine, seizures, and alternating hemiplegia [61, 62].
In conclusion, familial forms of MA, and in particular FHM, are due to rare inherited or sporadic genetic variants endowed with high penetrance. These mutations disrupt neuronal excitability by affecting the transmembrane electrochemical gradient and/or by enhancing extracellular glutamate concentrations. Each mutation is rare or even private: locus and allelic heterogeneity is clearly supported by current evidence and further heterogeneity can be anticipated. Importantly, studies investigating the role of FHM genes in common forms of MO have uncovered only few instances where mutations in FHM genes produce familial MO [56, 63]. This leads to conclude that genetic variants in FHM genes do not play widespread causative roles in common forms of MO, seemingly displaying more complex genetic underpinnings [76].
Oligogenic/polygenic forms of migraine
Candidate gene studies
Candidate gene approaches have been widely used to study migraine genetics. Replication studies have been performed with conflicting or inconclusive results for a significant number of these genes. This can be due to several reasons, such as low statistical power, interethnic differences in linkage disequilibrium, genetic, and phenotypic heterogeneity between independent case–control cohorts. Nonetheless, candidate gene studies remain of interest, as they can unveil the contribution of common genetic variants to a complex phenotype in specific ethnic groups and especially in genetic isolates (see “Methodological Issues in Migraine Genetics Research” below). Within this framework, positive findings are bound not to be replicated in all ethnic groups but are nonetheless relevant if at least some replications occur and functional allelic dimorphism is proven in vitro and/or in vivo. Candidate genes have been previously clustered around four functional gene families, namely neurological, vascular, hormonal, and inflammatory genes [76]. Tables 3, 4, 5, and 6 list positive case–control studies supporting the association between migraine and candidate genes yielding positive results in at least two independent studies. Negative studies are not listed.
-
(I)
Neurological genes. This category broadly includes candidate genes encoding: (a) ion channels (calcium channel, voltage-dependent, P/Q type, alpha 1A subunit [CACNA1A], voltage-potassium intermediate/small conductance calcium-activated channel, subfamily N, member 3 [KCCN3]), (b) Na+/K+-ATPase subunits, (c) molecules involved in the synthesis, release, and binding of neuropeptides (calcitonin gene-related peptide) or neurotransmitters (glutamate, GABA, dopamine, serotonin) relevant to neuronal excitation and/or to nociception. Some case–control association studies have yielded positive results, as listed in Table 3 [77–90], although most studies have been negative especially for the former two gene families. Nonetheless, a thorough screening of 150 brain-expressed genes involved in ion homeostasis (channels, transporters, exchangers, and accessory subunits) identified three genes encoding potassium channels associated with migraine, namely KCNK18, KCNG4, and KCNAB3 [121]. KCNK18 is especially interesting, in view of its expression in the trigeminal and dorsal root ganglia, as well as its relationship with MA also detected through linkage (see below).
-
(II)
Vascular genes. Association studies of genes involved in blood pressure regulation, endothelial cell function, vasoconstriction, and vasodilation have provided more consistent positive results (Table 4) [91–109, 122–129]. Many vascular genes associated with migraine also confer risk for stroke and heart disease [125–127]. This is especially important for MA, which displays a significant comorbidity with stroke and depression [15, 16]. Common functional variants in several vascular genes may predispose to migraine, while also influencing type and frequency of the attacks [127]:
-
(a)
Angiotensin converting enzyme (ACE) plays a key role in the maintenance of blood pressure and vessel wall tension. The D-D (“deletion-deletion”) common variant located in the ACE gene (human chr. 17q23) increases ACE enzymatic activity, as well as the frequency and duration of MA attacks [91–93];
-
(b)
An association between methylenetetrahydrofolate reductase (MTHFR) gene variants and migraine has also been found in several studies [128]. MTHFR is a key component of the remethylation of homocysteine to methionine, as it catalyzes the conversion of 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate. Rare loss-of-function mutations in the MTHFR gene, located in human chromosome 1p36.22, can lead to hyperhomocysteinemia due to decreased enzyme activity. Several studies involving different ethnic groups [78, 93–100, 122–124] and several recent metanalyses [98, 123, 124, 129] provide converging evidence of contributions by the T677 MTHFR allele at SNP rs1801133 to migraine, more consistently for carriers of the TT genotype and relative to MA than to MO. Nonetheless, lack of association with MTHFR gene variants has also been reported, which may be related to advancing age and selective survival [122];
-
(c)
NOTCH3 encodes for a transmembrane receptor regulating vascular development and differentiation during embryogenesis, as well as contributing to vascular integrity in adults [27, 28]. In addition to rare NOTCH3 mutations producing MA within the context of CADASIL [19–24], also common variants are significantly associated with migraine [101, 102]. Hence, NOTCH3 may play a broader role also in the pathogenesis of common migraine, well beyond rare forms associated with CADASIL;
-
(d)
Endothelial genes assessed for association with migraine encode for endothelin-1 (EDN1), endothelin receptor type A and B (EDNRA and EDNRB), inducible NO synthase (NOS2), endothelial NO synthase (NOS3), and vascular endothelial growth factor (VEGF) [103–109, 125]. Endothelin-1, encoded by the EDN1 gene (human chr 6p24), is involved in blood pressure regulation and produces vasoconstriction. EDN1 has two receptors, A and B, encoded by the EDNRA and EDNRB genes located on human chr 4q31 and 13q22, respectively. Several studies have found an association between EDNRA alleles and migraine (Table 4), including one study involving an experimental and a replica sample of Finnish and German migraineurs, respectively, reporting a nominal association with MA at EDNRA SNP rs2048894, especially with age at onset <20 years [103].
-
(a)
-
(III)
Hormonal genes. Genes governing estrogen and progesterone metabolism would be predicted to at least partly explain the sex-biased distribution of affection status, especially considering menstrual migraine [130]. However, results from genetic association studies are conflicting, although several positive case–control studies were published [131–136], as well as a pedigree-based association performed in the genetic isolate of Norfolk Island, a population with high prevalence of migraine descended from a small number of Isle of Man “Bounty Mutineer” and Tahitian founders [137]. In the latter study, three estrogen receptor 1 (ESR1) haplotypes were significantly associated with the disorder (P < 0.05 or 0.01). In addition to ESR1, six other hormonal genes have been investigated: estrogen receptor 2 (ESR2), progesterone receptor (PGR), androgen receptor (AR), follicle stimulating hormone receptor (FSHR), nuclear receptor interacting protein 1 (NRIP1), and cytochrome P450, family 19, subfamily A, polypeptide 1 (CYP19A1). However, a meta-analysis of eight genetic association studies investigating these genes suggests an association only with the ESR1 c.594G > A and c.325C > G polymorphisms, a finding that does not differ between MA and MO [9] (Table 5).
-
(IV)
Inflammatory genes. Animal and human studies suggest that inflammation and components of the immune system may play an important role in the pathogenesis of migraine. In the case of CSD, for example, this process triggers local neurogenic inflammation, with activation of mast cells and macrophages accompanied by the release of proinflammatory cytokines, ultimately resulting in the sensitization of meningeal nociceptive nerve endings [138]. Among several genes implicated in neurogenic inflammation, results support a positive association especially for tumor necrosis factor alfa (TNF-α) [110–120] (Table 6).
Linkage studies
Many classical linkage studies have been performed on migraine using either a genome-wide approach or targeting specific regions using microsatellite markers (139–161; Table 7). Results have been highly conflicting, and very few linkage peaks have been replicated in two independent samples (Table 7). This relative lack of success can be attributed to several causes, including locus heterogeneity, reduced penetrance, the existence of phenocopies, the separation/clustering together of MA and MO phenotypes which may represent in some families different clinical expressions of the same underlying mutation, while identical mutations may yield distinct clinical phenotypes in other families. Nonetheless, greater success has been achieved in linkage studies of FHM (162–169), which have detected several loci involved in these monogenic forms, as described above (Table 8). Some studies applying linkage to single large pedigrees, rather than combining several multiply affected families evidently afflicted by underlying heterogeneity, have also been successful. For example, a frameshift mutation in the KCNK18 gene was found to cosegregate with MA in a large pedigree from Ontario [170]. KCNK18 encodes for the TRESK pore potassium channel, highly expressed in trigeminal and dorsal root ganglia during embryogenesis: the truncated TRESK protein produces a dominant-negative effect blocking K+ flow through TRESK and yielding abnormal neuronal excitability [170, 171]. TRESK may play a broader role in common forms of migraine, since KCNK18 gene variants were found associated with migraine also in a case–control study (see above) [121]. Interestingly, the loss-of-function missense mutation C110R, found in sporadic cases, has also been detected among controls, underscoring the need for a multiple-hit model to explain TRESK contributions at least in some patients with MA [172].
To overcome the limitations of classical linkage in the presence of genetic and clinical heterogeneity and to target more homogenous subgroups of patients, latent class analysis (LCA) and trait component analysis (LTC) methods have been used in some migraine studies with promising results [141, 144, 148, 152].
Genome-wide association studies
To this date, six original GWAS of migraine with no selection based on specific comorbidities have been performed:
-
1)
The first GWAS of migraine was produced by the International Headache Genetics Consortium (IHGC) in 2010. Anttila and colleagues [173] carried out a two-stage association study in six clinic-based and one population-based European migraine samples. In the discovery stage, 2748 cases with MA, recruited from headache clinics in Finland, Germany, and Denmark, were compared with 10,747 population-matched controls. Out of 429,912 markers genotyped, only rs1835740 reached genome-wide significance, while 11 additional SNPs reached suggestive significance. This association was then replicated in 3202 cases and 40,062 controls, and combined results indicated an 18 % increase in migraine risk conferred by the minor allele at rs1835740 (OR = 1.18, 95 %; P = 1.69 × 10−11), with a stronger effect in the MA than in MO. This SNP is located on human chr 8q22.1, between the metadherin gene (MTDH), also known as astrocyte elevated gene 1, and the plasma glutamate carboxypeptidase Q gene (CPQ), also known as plasma glutamate carboxypeptidase (PGCP). Although the proximity of an association signal to a gene in GWAS does not necessarily implicate that gene in the pathophysiology of the disease, interestingly, these genes are both involved in glutamate homeostasis. In cultured astrocytes, metadherin down-regulates EAAT2, the major glutamate transporter in the brain: this in turn is predicted to increase glutamate concentrations in the synaptic cleft and/or delay glutamate removal, thus lowering the threshold for cortical spreading depression [174, 175], which plays a major role in the pathophysiology of MA, as discussed above.
-
2)
A population-based GWAS was then performed using a total of 23,330 women, divided in 5122 cases and 18,108 controls [176]. No SNP reached genome-wide significance in the discovery step. Among the seven loci showing suggestive significance (P < 5 × 10−6), SNPs tested in three independent replication cohorts provided significant results at SNPs located in or near the TRPM8, LRP1, and PRDM16 genes. TRPM8 is expressed in sensory neurons and dorsal root ganglion neurons and encodes a sensor for cold and cold-induced pain [177]. The role of TRPM8 in animal models of neuropathic pain further supports a functional link with migraine, which shares several commonalities with this pain syndrome [178]. LRP1, expressed in brain and in many other tissues [179], modulates synaptic transmission and interacts with glutamatergic NMDA receptors. Finally, PRDM16 is a pleiotropic gene important for craniofacial development, grown fat determination, and for the proliferation of cardiomyocyte, neural, and leukocyte precursor cells [180]. Interestingly, the mouse homologue Prdm16 has been shown to act as a negative regulator of TGF-β, encoded by TGFBR2, another migraine candidate gene [181]. An association with PRDM16, but not with LRP1 and TRPM8, has been recently replicated in a Chinese Han cohort [182]. Conversely, an association with LRP1 and TRPM8 has been detected in a Danish and Icelandic sample including 2523 cases and 38,170 controls, while a meta-analysis confirmed an association at all three loci [183].
-
3)
Lighthart et al. [184] performed a GWAS and meta-analysis using six European cohorts from the Dutch Icelandic migraine genetics consortium for a total of 2446 cases and 8534 controls. No SNP reached genome-wide significance, while 32 SNPs reached suggestive evidence (P < 1 × 10−5). The lowest P value was produced by a variant located in the nerve growth factor receptor (NGFR) gene. However, none of these SNPs reached significance in independent replica samples from the Netherlands and Australia. Metanalysis of the full data set provided weak evidence of association for the metadherin MTDH gene (P < 0.05).
-
4)
Freilinger et al. [185], with the aim to identify SNPs associated with MO, performed a GWAS including 2326 cases and 4580 controls from German and Dutch populations. In the discovery step, significant genome-wide association was reached by one locus located in chr. 1q22 (P < 5 × 10−8), while eleven additional loci provided suggestive evidence of association (P < 1 × 10−5). Eighteen SNPs from these 12 loci were then analyzed in four independent European replication samples consisting of 2508 cases and 2652 controls. Results showed a convincing replication at the 1q22 (MEF2D) and the 3p24 (near TGFBR2) loci, and suggestive evidence of replication for SNPs located in or near the PHACTR1 and ASTN2 genes, while previously identified loci (TRPM8 and LRP1) were also found associated. MEF2D is a transcription factor highly expressed in the brain, where it regulates neuronal differentiation and restricts excitatory synapses [186, 187]. This poses MEF2D as a strong candidate gene for migraine, given the involvement of glutamatergic neurotransmission in CSD and migraine pathogenesis [175], as well as possibly increased plasma levels of glutamate in individuals with migraine [188]. TGFBR2 encodes for transforming growth factor-β (TGF-β), involved in the regulation of cell proliferation, differentiation, and in extracellular matrix production [189]. A missense mutation has been associated with migraine headaches in 11 of 14 mutation carriers in a large pedigree [190].
-
5)
Cox et al. [191] recently performed a pedigree-based GWA study of an isolated population of Norfolk Island with a high prevalence of migraine (25.5 %). They found an association with rs4807347 located in the finger protein 555 (ZNF555) gene which was replicated in an independent case–control sample albeit with opposite alleles, as well as association with SNPs located in the ADARB2, GRM7, and HTR7 genes, mostly related to the serotoninergic system. This association is apparently specific to this isolated population but might bring insights to future research.
-
6)
A recent large meta-analysis of 29 population- and clinic-based samples including a total of 23,285 individuals with migraine and 95,425 matched controls identified 142 SNPs located in 12 different loci significantly associated with the phenotype, with 8 loci containing SNPs located in known transcripts [192]. Five loci were not previously associated with migraine (AJAP1, TSPAN, FHL5, C7orf10, and MMP16), although the TSPAN SNP is close to a previously associated SNP located near TSPAN-2 [145]. The remaining loci confirmed previous reports (PRDM16, MED2D, TRPM8, TGFBR2, PHATCTR1, ASTN2, and LRP1). The most significant P values were observed in the LRP1 locus (P = 2.69 × 10−19). Finally, an eQTL analysis performed on 394 brain tissue specimens revealed 5 additional loci potentially implicated in migraine susceptibility (APOA1BP, FUT9, STAT6, ATPB5, and TBC1D7). Results of this study analyzed by network analysis have been suggestive for a possible involvement of the identified gene into a common functional glutamate pathway [192].
Common variants identified by GWAS collectively contribute to migraine pathogenesis each exerting a small effect size, with ORs below 1.3 as typically occurs in complex disorders [192]. This contribution is detectable in common forms of polygenic migraine with multiple epistatic “gene × gene” and “gene × environment” interactions, whereas highly penetrant rare variants, such as those responsible for FHM, are able to produce sporadic and familial migraine without requiring contributions by common variants, which may at most modulate clinical features in monogenic forms. Despite the small effect size exerted by each single polymorphism, common variants unveiled by GWAS have proven very valuable by underscoring glutamatergic roles in migraine, likely underlying cortical spreading depression and the sensitization of nociceptive nerve endings, along with contributions by NGF and 5-HT signaling, as well as neuroimmune interactions.
Methodological issues in migraine genetics research
Genetic studies performed to date provide converging evidence supporting the existence of two broad migraine categories, caused either by (a) rare genetic variants with high penetrance, inherited, or de novo or by (b) a myriad of common variants, typically inherited, each providing small contributions to the overall disease risk, and collectively endowed with incomplete penetrance, hence requiring multiple gene-gene and gene-environment interactions as well as epigenetic influences in order to produce full-blown pathology. In simple terms, rare variants could be defined as “causal”, while common variants would be “predisposing”. These two categories do not overlap with current clinical categorizations, such as MA vs MO, although MA appears more frequently explained by rare causal variants compared to MO, which instead may more often fall into the latter category. Interestingly, several lines of evidence from twin and family studies already did support this prediction: for example, the presence of MA in the proband was found associated with a mean relative risk (RR) of 3.79 for MA in his/her first-degree relatives, as compared to 1.02 for MO; conversely, a diagnosis of MO conferred a RR of 1.86 and 1.44 for MO and MA, respectively [193]. It was reassuring to see this prediction confirmed by recent GWAS studies, identifying several common variants for MO, but none for MA [192]. Unfortunately, both migraines due to rare and to common variants display great heterogeneity, although in different ways: migraine forms due to rare variants are highly heterogeneous, with each rare variant causing the disorder in few families worldwide; migraine forms due to common variants are also highly heterogeneous, with multiple different combinations of common variants enhancing migraine risk in different individuals and ethnic groups, in turn, exposed to only partly overlapping environmental factors.
Experimental design must match this level of complexity for studies to provide meaningful results. Rare variants can hardly be tackled using classical linkage by combining multiple pedigrees as rare variants are so heterogeneous, while there is much greater probability of success for studies involving single large pedigrees with high recurrence rates. In this regard, the possibility that rare variants responsible for migraine in some family members may yield other disease phenotypes, perhaps among those so often comorbid with migraine, in other family members should be considered [15, 16]. Next-generation sequencing (NGS) technologies foster rare variants discovery through unbiased approaches, including whole-exome sequencing (WES) and whole-genome sequencing (WGS), whereas array-CGH can detect copy number variants (CNVs), microdeletions and microduplications acting either as rare or as common variants. Surprisingly, to our knowledge, no array-CGH study of migraine has been published to this date. WES has already been used in many monogenic disorders and also to detect mutations in complex disorders, such as autism [194]. Limitations of this technique include not only its cost and incomplete exome coverage but also the possibility that causal variants in non-coding regions are missed. WGS overcomes this limitation, at the expense of huge data production [195]. Multifactorial forms of migraine, such as most common forms of MO, can be explored by case–control or family-based association, using either a candidate gene or an unbiased GWAS approach. Within the framework of the ongoing debate on the role and meaning of candidate gene studies in the GWAS era, it is important to acknowledge the relative strengths and weaknesses of these approaches. GWAS needs extremely large sample sizes to control for multiple testing, and this typically requires the collaborative merging of pre-existing samples recruited in different countries. Hence, GWAS is a powerful and unbiased tool able to detect relevant common variation, provided it is not ethnic-specific and it is endowed with a sizable effect as compared to other common variants. Since much common variation is indeed ethnic-specific both due to disease pathophysiology and to linkage disequilibrium patterns, GWAS can discover the most consistent variants but by no means exhaust genetic contributions to common disorders. This can instead be sought also by using candidate gene approaches, which are clearly more at risk of false positives until at least some replication occurs and, more importantly, allelic variants are proven to exert functional roles. The efficacy of both candidate and unbiased association strategies can be further improved applying a qualitative diagnostic system and by implementing endophenotypes, familial, and heritable quantitative intermediate phenotypes associated with a complex disease and able to identify subgroups of patients possibly sharing a homogeneous pathophysiological basis [196, 197]. Biomarkers and endophenotypes applied in migraine research have been recently reviewed [198]. Additional endophenotypes may be represented by frequently comorbid disorders [15, 16], whereby the process leading to migraine may differ from non-comorbid forms [199]. A phenotyping approach involving endophenotypes, while requiring greater care in statistically controlling for multiple testing, has already yielded valuable results also in linkage analysis through LCA and TCA, as discussed above.
Finally, it is highly unlikely that genetic markers will be able to explain large portions of phenotypic variance in many common forms of migraine. A combination of epigenomic, trascriptomic, proteomic, and metabolomic biomarkers assessed in first-onset cases prior to starting chronic pharmacological treatment and followed longitudinally for migraine subtype characterization may provide, in combination with common genetic variants, greater amounts of clinically useful information [197]. To this date, few studies have identified biochemical biomarkers of potential clinical significance, such as the neuropeptide calcitonin gene-related peptide (CGRP) [198]. This path of investigation remains entirely to be explored. Additional areas where genetic investigations will undoubtedly play a major role, but complementary approaches will likely be necessary, include the underpinnings of treatment response, the sex bias observed in migraine, and the overlap between migraine and comorbid conditions.
Conclusions
Genetic studies have provided pivotal insights into the molecular mechanisms underlying migraine. Cellular and animal models of monogenic forms have helped in understanding the pathophysiology of migraine, which essentially leans upon three main domains, a “neural” domain (i.e., CSD-like neural activity patterns), a “vascular” domain, (intracranial vasospasm followed by excessive vasodilatation of intra and extracranial blood vessels), and a “nociceptive” domain (sensitization of perivascular trigeminal nociceptors involving inflammatory mediators, growth factors, and neuropeptides, such as CGRP) [4]. The relevance of these three pathophysiological domains has received further support by the results of many candidate gene association studies and linkage studies, as well as more recently by GWAS. Hence, despite great genetic heterogeneity, also in migraine as in other complex neurological and psychiatric disorders, pathway analysis holds promise to converge upon a relatively limited number of functional pathways starting from mutations and polymorphisms located in many different loci.
The success of migraine genetic investigations will largely rely upon their capacity on one hand to apply the methodological approaches most apt to respond to each specific experimental question, on the other hand, on their capacity to integrate multiple levels of phenotypic, functional, and genetic information, in accordance with the complexity of the disorder itself. This should ultimately lead not only to the identification of novel genes associated with migraine but more importantly with a better definition of the pathophysiological mechanisms underlying specific forms of migraine in specific patients. New reliable and valid animal models will be especially useful in studying not only monogenic forms but also the cross-talk between genetic vulnerability and epigenetic contributions in common forms of migraine. Environmental factors, such as early and recent life events, hormones, and inflammation, can indeed act upon a genetically vulnerable background to trigger the onset and determine the progression of the disease [13]. This is likely mediated through modifications of the epigenetic profiles of migraine-relevant genes [14]. Animal models will be especially helpful, because epigenetics is cell- and tissue-specific; it may thus be especially challenging in humans to move from peripheral epigenetic biomarkers to relevant chromatin signatures located in cells directly involved in migraine pathogenesis. An example is medication overuse headache, which implies both genetic vulnerability to migraine and triptan-induced chromatin changes affecting the trigeminovascular system [200]. These animal models, combining genetic and epigenetic components, will be instrumental in leading to more effective pharmacological treatments for the most common forms of this debilitating disorder.
References
Headache Classification Committee of the International Headache Society (IHS) (2013) The international classification of headache disorders, 3rd edition (beta version). Cephalalgia 33:629–808
Bigal ME, Lipton RB (2009) The epidemiology, burden, and comorbidities of migraine. Neurol Clin 27:321–334
Robbins MS, Lipton RB (2010) The epidemiology of primary headache disorders. Semin Neurol 30:107–109
Noseda R, Burstein R (2013) Migraine pathophysiology: anatomy of the trigeminovascular pathway and associated neurological symptoms, CSD, sensitization and modulation of pain. Pain 154(Suppl 1)
Eikermann-Haerter K, Moskowitz MA (2008) Animal models of migraine headache and aura. Curr Opin Neurol 21:294–300
Mulder EJ, van Baal C, Gaist D et al (2003) Genetic and environmental influences on migraine: a twin study across six countries. Twin Res 6:422–431
Svensson DA, Larsson B, Waldenlind E, Pedersen NL (2003) Shared rearing environment in migraine: results from twin reared apart and twin reared together. Headache 43:235–244
Cologno D, Pascale AD, Manzoni GC (2003) Familial occurrence of migraine with aura in a population-based study. Headache 43:231–234
Schürks M, Rist PM, Kurth T (2010) Sex hormone receptor gene polymorphisms and migraine: a systematic review and meta-analysis. Cephalalgia 30:1306–1328
Russel MB, Iselius L, Olesen J (1996) Migraine without aura and migraine with aura are inherited disorders. Cephalalgia 16:305–309
Lemos C, Alonso I, Barros J et al (2012) Assessing risk factors for migraine: differences in gender transmission. PLoS One 7:e50626
Peltonen L, GenomEUtwin (2003) GenomEUtwin: a strategy to identify genetic influences on health and disease. Twin Res 6:354–360
Friedman DI, De ver Dye T (2009) Migraine and the environment. Headache 49:941–952
Eising E, Datson NA, van den Maagdenberg AMJM, Ferrari MD (2013) Epigenetic mechanisms in migraine: a promising avenue? BMC Med 11:26–32
Diener HC, Kuper M, Kurth T (2008) Migraine-associated risks and comorbidity. J Neurol 255:1290–1301
Bellini B, Arruda M, Cescut A et al (2013) Headache and comorbidity in children and adolescents. J Headache Pain 14:79–86
Hung CI, Liu CY, Juang YY, Wang SJ (2006) The impact of migraine on patients with major depressive disorder. Headache 46:469–477
Tietjen GE, Brandes JL, Digre KB et al (2007) High prevalence of somatic symptoms and depression in women with disabling chronic headache. Neurology 68:134–140
Joutel A, Corpechot C, Ducros A et al (1996) Notch-3 mutations in CADASIL, a hereditary adult-onset condition causing stroke and dementia. Nature 383:707–710
Federico A, Bianchi S, Dotti MT (2005) The spectrum of mutations for CADASIL diagnosis. Neurol Sci 26:117–124
Ungaro C, Mazzei R, Conforti FL et al (2009) CADASIL: extended polymorphisms and mutational analysis of the NOTCH3 gene. J Neurosci Res 87:1162–1167
Mosca L, Marazzi R, Ciccone A et al (2011) NOTCH3 gene mutations in subjects clinically suspected of CADASIL. J Neurol Sci 307:144–148
Ragno M, Fabrizi GM, Cacchiò G et al (2006) Two novel Italian CADASIL families from Central Italy with mutation CGC-TGC at codon 1006 in the exon 19 Notch3 gene. Neurol Sci 27:252–256
Valenti R, Bianchi S, Pescini F et al (2011) First report of a pathogenic mutation on exon 24 of the NOTCH3 gene in a CADASIL family. J Neurol 258:1632–1636
Razvi SS, Davidson R, Bone I, Muir KW (2005) The prevalence of cerebral autosomal dominant arteriopathy with subcortical infarcts and leucoencephalopathy (CADASIL) in the west of Scotland. J Neurol Neurosurg Psychiatry 76:739–741
Narayan SK, Gorman G, Kalaria RN et al (2012) The minimum prevalence of CADASIL in Northeast England. Neurology 78:1025–1027
Iso T, Hamamori Y, Kedes L (2003) Notch signaling in vascular development. Arterioscler Thromb Vasc Biol 23:543–553
Alva JA, Iruela-Arispe ML (2004) Notch signaling in vascular morphogenesis. Curr Opin Hematol 11:278–283
Ishiko A, Shimizu A, Nagata E et al (2006) Notch3 ectodomain is a major component of granular osmiophilic material (GOM) in CADASIL. Acta Neuropathol 112:333–339
Liem MK, Oberstein SA, van der Grond J et al (2010) CADASIL and migraine: a narrative review. Cephalalgia 30:1284–1289
Dichgans M, Mayer M, Uttner I et al (1998) The phenotypic spectrum of CADASIL: clinical findings in 102 cases. Ann Neurol 44:731–739
Kaufmann P, Engelstad K, Wei Y et al (2011) Natural history of MELAS associated with mitochondrial DNA m.3243A > G genotype. Neurology 77:1965–1971
Finsterer J (2012) Inherited mitochondrial disorders. Adv Exp Med Biol 942:187–213
Federico A, Di Donato I, Bianchi S et al (2012) Hereditary cerebral small vessel diseases: a review. J Neurol Sci 322:25–30
Ophoff RA, DeYoung J, Service SK et al (2001) Hereditary vascular retinopathy, cerebroretinal vasculopathy, and hereditary endotheliopathy with retinopathy, nephropathy, and stroke map to a single locus on chromosome 3p21.1-p21.3. Am J Hum Genet 69:447–453
Bersano A, Debette S, Zanier ER et al (2012) The genetics of small-vessel disease. Curr Med Chem 19:4124–4141
Storimans CW, Van Schooneveld MJ, Oosterhuis JA, Bos PJ (1991) A new autosomal dominant vascular retinopathy syndrome. Eur J Ophthalmol 1:73–78
Terwindt GM, Haan J, Ophoff RA et al (1998) Clinical and genetic analysis of a large Dutch family with autosomal dominant vascular retinopathy, migraine and Raynaud's phenomenon. Brain 121(Pt 2):303–316
Jen J, Cohen AH, Yue Q et al (1997) Hereditary endotheliopathy with retinopathy, nephropathy, and stroke (HERNS). Neurology 49:1322–1330
Winkler DT, Lyrer P, Probst A et al (2008) Hereditary systemic angiopathy (HSA) with cerebral calcifications, retinopathy, progressive nephropathy, and hepatopathy. J Neurol 255:77–88
Di Francesco JC, Novara F, Zuffardi O, et al. (2014) TREX1 C-terminal frameshift mutations in the systemic variant of retinal vasculopathy with cerebral leukodystrophy. Neurol Sci
Gould DB, Phalan FC, Breedved GJ et al (2005) Mutations in COL4A1 cause perinatal cerebral hemorrhage and porencephaly. Science 308:1167–1171
Breedved G, de Coo IF, Lequin MH et al (2006) Novel mutations in three families confirms a major role of COL4A1 in hereditary porencephaly. J Med Genet 43:490–495
Van Der Knaap MS, Smit LM, Barkhof F et al (2006) Neonatal porencephaly and adult stroke related to mutations in collagen IV A1. Ann Neurol 59:504–511
Lanfranconi S, Markus HS (2010) COL4A1 mutations as a monogenic cause of cerebral small vessel disease: a systematic review. Stroke 41:e513–e518
Vahedi K, Massin P, Guichard JP et al (2003) Hereditary infantile hemiparesis, retinal arteriolar tortuosity, and leukoencephalopathy. Neurology 60:57–63
Ebisawa T (2007) Circadian rhythms in the CNS and peripheral clock disorders: human sleep disorders and clock genes. J Pharmacol Sci 103:150–154
Vanselow K, Vanselow JT, Westermark PO et al (2006) Differential effects of PER2 phosphorylation: molecular basis for the human familial advanced sleep phase syndrome (FASPS). Genes Dev 20:2660–2672
Brennan KC, Bates EA, Shapiro RE et al (2013) Casein kinase I mutations in familial migraine and advanced sleep phase. Sci Transl Med 5(183ra56):1–11
Xu Y, Padiath QS, Shapiro RE et al (2005) Functional consequences of a CKIδ mutation causing familial advanced sleep phase syndrome. Nature 434:640–644
Hansen JM (2010) Familial hemiplegic migraine. Dan Med Bull 57:B4183
Thomsen LL, Kirchmann M, Bjornsson A et al (2007) The genetic spectrum of a population-based sample of familial hemiplegic migraine. Brain 130(Pt 2):346–356
Riant F, Ducros A, Ploton C et al (2010) De novo mutations in ATP1A2 and CACNA1A are frequent in early-onset sporadic hemiplegic migraine. Neurology 75:967–972
Ophoff RA, Terwindt GM, Vergouwe MN et al (1996) Familial hemiplegic migraine and episodic ataxia type-2 are caused by mutations in the Ca2+ channel gene CACNL1A4. Cell 87:543–552
Ambrosini A, D’Onofrio M, Grieco G et al (2005) Familial basilar migraine associated with a new mutation in ATP1A2 gene. Neurology 65:1826–1828
Todt U, Dichgans M, Jurkat-Rott K et al (2005) Rare missense variants in ATP1A2 in families with clustering of common forms of migraine. Hum Mutat 26:315–321
Vanmolkot KR, Babini E, de Vries B et al (2007) The novel pL1649Q mutation in the SCN1A epilepsy gene associated with familial hemiplegic migraine: genetic and functional studies. Hum Mutat 28:522
Cestèle S, Scalmani P, Rusconi R et al (2008) Self-limited hyperexcitability: functional effect of a familial hemiplegic migraine mutation of the Nav1.1 (SCN1A) Na+ channel. J Neurosci 28:7273–7283
Dale RC, Gardiner A, Antony J, Hulden H (2012) Familial PRRT2 mutation with heterogeneous paroxysmal disorders including paroxysmal torticollis and hemiplegic migraine. Dev Med Child Neurol 54:958–960
Suzuki M, Van Paesschen W, Stalmans I et al (2010) Defective membrane expression of the Na(+)-HCO3(−) cotrasporter NBCe1 is associated with familial migraine. Proc Natl Acad Sci U S A 107:15963–15968
Jen JC, Wan J, Palos TP et al (2005) Mutation in the glutamate transporter EAAT1 causes episodic ataxia, hemiplegia, and seizures. Neurology 65:529–534
de Vries B, Mamsa H, Stam AH et al (2009) Episodic ataxia associated with EAAT1 mutation C186S affecting glutamate reuptake. Arch Neurol 66:97–101
Frosk P, Mhanni AA, Rafay MF (2013) SCN1A mutation associated with intractable myoclonic epilepsy and migraine headache. J Child Neurol 28:389–391
Gargus JJ, Tournay A (2007) Novel mutation confirms seizure locus SCN1A is also familial hemiplegic migraine locus FHM3. Pediatr Neurol 37:407–410
O'Roak BJ, Deriziotis P, Lee C et al (2011) Exome sequencing in sporadic autism spectrum disorders identifies severe de novo mutations. Nat Genet 43:585–589
Barros J, Ruano L, Domingos J et al (2014) The prevalence of familial hemiplegic migraine with cerebellar ataxia and spinocerebellar ataxia type 6 in Portugal. Headache 54:911–915
Bürk K, Kaiser FJ, Tennstedt S et al (2014) A novel missense mutation in CACNA1A evaluated by in silico protein modeling is associated with non-episodic spinocerebellar ataxia with slow progression. Eur J Med Genet 57:207–211
Star TV, Pristay W, Snutch TP (1991) Primary structure of a calcium channel that is highly expressed in the rat cerebellum. Proc Natl Acad Sci U S A 88:5621–5625
Westenbroek RE, Sakurai T, Elliot EM (1995) Immunochemical identification and subcellular distribution of the alpha 1A subunits of brain calcium channels. J Neurosci 15:6403–6418
Cohen-Kutner M, Nachmanni D, Atlas D (2010) CaV2.1 (P/Q channel) interaction with synaptic proteins is essential for depolarization-evoked release. Channels (Austin) 4:266–277
Van Den Magdemberg AM, Pietrobon D, Pizzorusso T et al (2004) A Cacna1A knockin migraine mouse model with increased susceptibility to cortical spreading depression. Neuron 41:701–710
Eikermann-Haerter K, Yuzawa I, Qin T et al (2011) Enhanced subcortical spreading depression in familial hemiplegic migraine type 1 mutant mice. J Neurosci 31:5755–5763
Eikermann-Haerter K, Dileköz E, Kudo C et al (2009) Genetic and hormonal factors modulate spreading depression and transient hemiparesis in mouse models of familial hemiplegic migraine type 1. J Clin Invest 119:99–109
Hedrich UB, Liautard C, Kirschenbaum D et al (2014) Impaired action potential initiation in GABAergic interneurons causes hyperexcitable networks in an epileptic mouse model carrying a human NaV1.1 mutation. J Neurosci 34:14874–14889
Escayg A, Goldin AL (2010) Sodium channel SCN1A and epilepsy: mutations and mechanisms. Epilepsia 51:1650–1658
Maher BH, Griffiths LR (2011) Identification of molecular genetic factors that influence migraine. Mol Genet Genomics 285:433–446
Corominas R, Sobrido MJ, Ribasés M et al (2010) Association study of the serotoninergic system in migraine in the Spanish population. Am J Med Genet B Neuropsychiatr Genet 153B:177–184
Ishii M, Shimizu S, Sakairi Y et al (2012) MAOA, MTHFR, and TNF-β genes polymorphisms and personality traits in the pathogenesis of migraine. Mol Cell Biochem 363:357–366
Borroni B, Brambilla C, Liberini P et al (2005) Functional serotonin 5-HTTLPR polymorphism is a risk factor for migraine with aura. J Headache Pain 6:182–184
Bayerer B, Engelbergs J, Savidou I et al (2010) Single nucleotide polymorphisms of the serotonin transporter gene in migraine—an association study. Headache 50:319–322
Lea RA, Dohy A, Jordan K et al (2000) Evidence for allelic association of the dopamine beta-hydroxylase gene (DBH) with susceptibility to typical migraine. Neurogenetics 3:35–40
Fernandez F, Lea RA, Colson NJ, Bellis C et al (2006) Association between a 19 bp deletion polymorphism at the dopamine beta-hydroxylase (DBH) locus and migraine with aura. J Neurol Sci 251:118–123
Fernandez F, Colson N, Quinlan S et al (2009) Association between migraine and a functional polymorphism at the dopamine beta-hydroxylase locus. Neurogenetics 10:199–208
Todt U, Netzer C, Toliat M et al (2009) New genetic evidence for involvement of the dopamine system in migraine with aura. Hum Genet 125:265–279
Corominas R, Ribases M, Camina M et al (2009) Two-stage case control association study of dopamine-related genes and migraine. BMC Med Genet 10:95
Ghosh J, Pradhan S, Mittal B (2011) Role of dopaminergic gene polymorphisms (DBH 19 bp indel and DRD2 Nco I) in genetic susceptibility to migraine in North Indian population. Pain Med 12:1109–1111
Ghosh J, Pradhan S, Mittal B (2013) Identification of a novel ANKK1 and other dopaminergic (DRD2 and DBH) gene variants in migraine susceptibility. Neuromol Med 15:61–73
Mochi M, Cevoli S, Cortelli P et al (2003) A genetic association study of migraine with dopamine receptor 4, dopamine transporter and dopamine-beta-hydroxylase genes. Neurol Sci 23:301–305
Formicola D, Aloia A, Sampaolo S et al (2010) Common variants in the regulative regions of GRIA1 and GRIA3 receptor genes are associated with migraine susceptibility. BMC Med Genet 25:103
Maher BH, Lea RA, Follett J et al (2013) Association of a GRIA3 gene polymorphism with migraine in an Australian case–control cohort. Headache 53:1245–1249
Paterna S, Di Pasquale P, Cottone C et al (1997) Migraine without aura and ACE-gene deletion polymorphism: is there a correlation? Preliminary findings. Cardiovasc Drugs Ther 11:603–604
Kowa H, Fusayasu E, Ijiri T et al (2005) Association of the insertion/deletion polymorphism of the angiotensin I-converting enzyme gene in patients of migraine with aura. Neurosci Lett 374:129–131
Joshi G, Pradhan S, Mittal B (2009) Role of the ACE ID and MTHFR C677T polymorphisms in genetic susceptibility of migraine in a north Indian population. J Neurol Sci 277:133–137
Kowa H, Yasui K, Takeshima T et al (2000) The homozygous C677T mutation in the methylenetetrahydrofolate reductase gene is a genetic risk factor for migraine. Am J Med Genet 96:762–764
Kara I, Sazci A, Ergul E et al (2003) Association of the C677T and A1298C polymorphisms in the 5, 10 methylenetetrahydrofolate reductase gene in patients with migraine risk. Brain Res Mol Brain Res 111:84–90
Oterino A, Valle N, Bravo Y et al (2004) MTHFR T677 homozygosis influences the presence of aura in migraineurs. Cephalalgia 24:491–494
Lea RA, Ovcaric M, Sundholm J et al (2005) Genetic variants of angiotensin converting enzyme and methylenetetrahydrofolate reductase may act in combination to increase migraine susceptibility. Brain Res Mol Brain Res 136:112–117
Samaan Z, Gaysina D, Cohen-Woods S et al (2011) Methylenetetrahydrofolate reductase gene variant (MTHFR C677T) and migraine: a case control study and meta-analysis. BMC Neurol 11:66
An XK, Lu CX, Ma QL et al (2013) Association of MTHFR C677T polymorphism with susceptibility to migraine in the Chinese population. Neurosci Lett 549:78–81
Bahadir A, Eroz R, Dikici S (2013) Investigation of MTHFR C677T gene polymorphism, biochemical and clinical parameters in Turkish migraine patients: association with allodynia and fatigue. Cell Mol Neurobiol 33(8):1055–1063
Schwaag S, Evers S, Schirmacher A et al (2006) Genetic variants of the NOTCH3 gene in migraine—a mutation analysis and association study. Cephalalgia 26:158–161
Menon S, Cox HC, Kuwahata M et al (2010) Association of a Notch 3 gene polymorphism with migraine susceptibility. Cephalalgia 31:264–270
Tikka-Klemola P, Kaunisto MA, Hamalainen E et al (2009) Genetic association study of endothelin-1 and its receptors EDNRA and EDNRB in migraine with aura. Cephalalgia 29:1224–1231
Joshi G, Pradhan S, Mittal B (2011) Vascular gene polymorphisms (EDNRA −231 G > A and APOE HhaI) and risk for migraine. DNA Cell Biol 30:577–584
Lemos C, Neto JL, Pereira-Monteiro J et al (2011) A role for endothelin receptor type A in migraine without aura susceptibility? A study in Portuguese patients. Eur J Neurol 18:649–655
Tzourio C, El Amrani M, Poirier O et al (2001) Association between migraine and endothelin type A receptor (ETA −231 A/G) gene polymorphism. Neurology 56:1273–1277
Jia S, Ni J, Chen S et al (2011) Association of the pentanucleotide repeat polymorphism in NOS2 promoter region with susceptibility to migraine in a Chinese population. DNA Cell Biol 30:117–122
de OS Mansur T, Goncalves FM, Martins-Oliveira A et al (2012) Inducible nitric oxide synthase haplotype associated with migraine and aura. Mol Cell Biochem 364:303–308
Borroni B, Rao R, Liberini P et al (2006) Endothelial nitric oxide synthase (Glu298Asp) polymorphism is an independent risk factor for migraine with aura. Headache 46:1575–1579
Rainero I, Grimaldi LM, Salani G et al (2004) Association between the tumor necrosis factor-alpha −308 G/A gene polymorphism and migraine. Neurology 62:141–143
Mazaheri S, Hajilooi M, Rafiei A (2006) The G-308A promoter variant of the tumor necrosis factor-alpha gene is associated with migraine without aura. J Neurol 253:1589–1593
Ghosh J, Joshi G, Pradhan S, Mittal B (2010) Investigation of TNFA 308G > A and TNFB 252G > A polymorphisms in genetic susceptibility to migraine. J Neurol 257:898–904
Yilmaz IA, Ozge A, Erdal ME et al (2010) Cytokine polymorphism in patients with migraine: some suggestive clues of migraine and inflammation. Pain Med 11:492–497
Ates O, Kurt S, Altinisik J et al (2011) Genetic variations in tumor necrosis factor alpha, interleukin-10 genes, and migraine susceptibility. Pain Med 12:1464–1469
Trabace S, Brioli G, Lulli P et al (2002) Tumor necrosis factor gene polymorphism in migraine. Headache 42:341–345
Lee KA, Jang SY, Sohn KM et al (2007) Association between a polymorphism in the lymphotoxin-a promoter region and migraine. Headache 47:1056–1062
Asuni C, Stochino ME, Cherchi A et al (2009) Migraine and tumour necrosis factor gene polymorphism. An association study in a Sardinian sample. J Neurol 256:194–197
Dong W, Jia S, Ye X, Ni J (2012) Association analysis of TNFRSF1B polymorphism with susceptibility for migraine in the Chinese Han population. J Clin Neurosci 19:750–752
Rainero I, Fasano E, Rubino E et al (2005) Association between migraine and HLA-DRB1 gene polymorphisms. J Headache Pain 6:185–187
Dasdemir S, Cetinkaya Y, Gencer M et al (2013) Cox-2 gene variants in migraine. Gene 518:292–295
Lafrenière RG, Rouleau GA (2012) Identification of novel genes involved in migraine. Headache 52:107–110
Scher AI, Eiriksdottir G, Garcia M et al (2013) Lack of association between the MTHFR C677T variant and migraine with aura in an older population: could selective survival play a role? Cephalalgia 33:308–315
Liu R, Geng P, Ma M et al (2014) MTHFR C677T polymorphism and migraine risk: a meta-analysis. J Neurol Sci 336:68–73
Rubino E, Ferrero M, Rainero I et al (2009) Association of the C677T polymorphism in the MTHFR gene with migraine: a meta-analysis. Cephalalgia 29:818–825
MacClellan LR, Howard TD, Cole JW et al (2009) Relation of candidate genes that encode for endothelial function to migraine and stroke: the Stroke Prevention in Young Women study. Stroke 40:e550–e557
Pizza V, Bisogno A, Lamaida E et al (2010) Migraine and coronary artery disease: an open study on the genetic polymorphism of the 5,10 methylenetetrahydrofolate (MTHFR) and angiotensin I-converting enzyme (ACE) genes. Cent Nerv Syst Agents Med Chem 10:91–96
Colson NJ, Lea RA, Quinlan S, Griffiths LR (2006) The role of vascular and hormonal genes in migraine susceptibility. Mol Genet Metab 88:107–113
Stuart S, Cox HC, Lea RA, Griffiths LR (2012) The role of the MTHFR gene in migraine. Headache 52:515–520
Schürks M, Rist PM, Kurth T (2010) MTHFR 677C > T and ACE D/I polymorphisms in migraine: a systematic review and meta-analysis. Headache 50:588–599
Colson N, Fernandez F, Griffiths L (2010) Genetics of menstrual migraine: the molecular evidence. Curr Pain Headache Rep 14:389–395
Colson NJ, Lea RA, Quinlan S et al (2004) The estrogen receptor 1 G594A polymorphism is associated with migraine susceptibility in two independent case/control groups. Neurogenetics 5:129–133
Oterino A, Pascual J, Ruiz de Alegria C et al (2006) Association of migraine and ESR1 G325C polymorphism. Neuroreport 17:61–64
Oterino A, Toriello M, Cayón A et al (2008) Multilocus analyses reveal involvement of the ESR1, ESR2, and FSHR genes in migraine. Headache 48:1438–1450
Joshi G, Pradhan S, Mittal B (2010) Role of the oestrogen receptor (ESR1 PvuII and ESR1 325 C- > G) and progesterone receptor (PROGINS) polymorphisms in genetic susceptibility to migraine in a North Indian population. Cephalalgia 30:311–320
Ghosh J, Joshi G, Pradhan S, Mittal B (2012) Potential role of aromatase over estrogen receptor gene polymorphisms in migraine susceptibility: a case control study from North India. PLoS One 7:e34828
Colson NJ, Lea RA, Quinlan S et al (2005) Investigation of hormone receptor genes in migraine. Neurogenetics 6:17–23
Rodriguez-Acevedo AJ, Maher BH, Lea RA et al (2013) Association of oestrogen-receptor gene (ESR1) polymorphisms with migraine in the large Norfolk Island pedigree. Cephalalgia 33:1139–1147
Levy D (2012) Endogenous mechanisms underlying the activation and sensitization of meningeal nociceptors: the role of immuno-vascular interactions and cortical spreading depression. Curr Pain Headache Rep 16:270–277
Thompson MD, Noble-Topham S, Percy ME et al (2012) Chromosome 1p36 in migraine with aura: association study of the 5HT(1D) locus. Neuroreport 23:45–48
Curtain RP, Lea RA, Tajouri L et al (2005) Analysis of chromosome 1 microsatellite markers and the FHM2-ATP1A2 gene mutations in migraine pedigrees. Neurol Res 27:647–652
Nyholt DR, Morley KI, Ferreira MA et al (2005) Genome wide significant linkage to migrainous headache on chromosome 5q21. Am J Hum Genet 77:500–512
Gardner K, Barmada MM, Ptacek LJ, Hoffman EP (1997) A new locus for hemiplegic migraine maps to chromosome 1q31. Neurology 49:1231–1238
Lea RA, Shepherd AG, Curtain RP et al (2002) A typical migraine susceptibility region localizes to chromosome 1q31. Neurogenetics 4:17–22
Ligthart L, Nyholt DR, Hottenga JJ et al (2008) A genome-wide linkage scan provides evidence for both new and previously reported loci influencing common migraine. Am J Med Genet B Neuropsychiatr Genet 147B:1186–1195
Lea RA, Nyholt DR, Curtain RP et al (2005) A genome-wide scan provides evidence for loci influencing a severe heritable form of common migraine. Neurogenetics 6:67–72
Björnsson A, Gudmundsson G, Gudfinnsson E et al (2003) Localization of a gene for migraine without aura to chromosome 4q21. Am J Hum Genet 73:986–993
Wessman M, Kallela M, Kaunisto MA et al (2002) A susceptibility locus for migraine with aura, on chromosome 4q24. Am J Hum Genet 70:652–662
Anttila V, Kallela M, Oswell G et al (2006) Trait components provide tools to dissect the genetic susceptibility of migraine. Am J Hum Genet 79:85–99
Carlsson A, Forsgren L, Nylander PO et al (2002) Identification of a susceptibility locus for migraine with and without aura on 6p12.2-p21.1. Neurology 59:1804–1807
Oterino A, Toriello M, Castillo J et al (2012) Family-based association study of chromosome 6p12.2-p21.1 migraine locus. Headache 52:393–399
Tikka-Kleemola P, Artto V, Vepsäläinen S et al (2010) A visual migraine aura locus maps to 9q21-q22. Neurology 74:1171–1177
Anttila V, Nyholt DR, Kallela M et al (2008) Consistently replicating locus linked to migraine on 10q22-q23. Am J Hum Genet 82:1051–1063
Del Zompo M, Cherchi A, Palmas MA et al (1998) Association between dopamine receptor genes and migraine without aura in a Sardinian sample. Neurology 51:781–786
Cader ZM, Noble-Topham S, Dyment DA et al (2003) Significant linkage to migraine with aura on chromosome 11q24. Hum Mol Genet 12:2511–2517
Nyholt DR, Curtain RP, Gaffney PT et al (1996) Migraine association and linkage analyses of the human 5-hydroxytryptamine (5HT2A) receptor gene. Cephalalgia 16:463–467
Soragna D, Vettori A, Carraro G et al (2003) A locus for migraine without aura maps on chromosome 14q21.2-q22.3. Am J Hum Genet 72:161–167
Russo L, Mariotti P, Sangiorgi E et al (2005) A new susceptibility locus for migraine with aura in the 15q11-q13 genomic region containing three GABA-A receptor genes. Am J Hum Genet 76:327–333
May A, Ophoff RA, Terwindt GM et al (1995) Familial hemiplegic migraine locus on 19p13 is involved in the common forms of migraine with and without aura. Hum Genet 96:604–608
Nyholt DR, Lea RA, Goadsby PJ et al (1998) Familial typical migraine: linkage to chromosome 19p13 and evidence for genetic heterogeneity. Neurology 50:1428–1432
Nyholt DR, Dawkins JL, Brimage PJ et al (1998) Evidence for an X-linked genetic component in familial typical migraine. Hum Mol Genet 7:459–463
Nyholt DR, Curtain RP, Griffiths LR (2000) Familial typical migraine: significant linkage and localization of a gene to Xq24-28. Hum Genet 107:18–23
Ducros A, Joutel A, Vahedi K et al (1997) Mapping of a second locus for familial hemiplegic migraine to 1q21-q23 and evidence of further heterogeneity. Ann Neurol 42:885–890
Cevoli S, Pierangeli G, Monari L et al (2002) Familial hemiplegic migraine: clinical features and probable linkage to chromosome 1 in an Italian family. Neurol Sci 23:7–10
Marconi R, De Fusco M, Aridon P et al (2003) Familial hemiplegic migraine type 2 is linked to 0.9 Mb region on chromosome 1q23. Ann Neurol 53:376–381
Fernandez DM, Hand CK, Sweeney BJ, Parfrey NA (2008) A novel ATP1A2 gene mutation in an Irish familial hemiplegic migraine kindred. Headache 48:101–108
Dichgans M, Freilinger T, Eckstein G et al (2005) Mutation in the neuronal voltage-gated sodium channel SCN1A in familial hemiplegic migraine. Lancet 366:371–377
Cuenca-León E, Corominas R, Montfort M et al (2009) Familial hemiplegic migraine: linkage to chromosome 14q32 in a Spanish kindred. Neurogenetics 10:191–198
Joutel A, Bousser MG, Biousse V et al (1994) Familial hemiplegic migraine. Localization of a responsible gene on chromosome 19. Rev Neurol (Paris) 150:340–345
Ahmed MA, Reid E, Cooke A et al (1996) Familial hemiplegic migraine in the west of Scotland: a clinical and genetic study of seven families. J Neurol Neurosurg Psychiatry 61:616–620
Lafrenière RG, Cader MZ, Poulin JF et al (2010) A dominant-negative mutation in the TRESK potassium channel is linked to familial migraine with aura. Nat Med 43:1157–1160
Lafrenière RG, Rouleau GA (2011) Role of the TRESK two-pore potassium channel. Int J Biochem Cell Biol 43:1533–1536
Andres-Enguix I, Shang L, Stansfeld PJ et al (2012) Functional analysis of missense variants in the TRESK (KCNK18) K channel. Sci Rep 2:237
Anttila V, Stefansson H, Kallela M, International Headache Genetics Consortium et al (2010) Genome-wide association study of migraine implicates a common susceptibility variant on 8q22.1. Nat Genet 42:869–873
Kang DC, Su ZZ, Sarkar D et al (2005) Cloning and characterization of HIV-1-inducible astrocyte elevated gene-1, AEG-1. Gene 353:8–15
Gasparini CF, Griffiths LR (2013) The biology of the glutamatergic system and potential role in migraine. Int J Biomed Sci 9:1–8
Chasman DI, Schürks M, Anttila V et al (2011) Genome-wide association study reveals three susceptibility loci for common migraine in the general population. Nat Genet 43:695–698
Proudfoot CJ, Garry EM, Cottrell DF et al (2006) Analgesia mediated by the TRPM8 cold receptor in chronic neuropathic pain. Curr Biol 16:1591–1605
Biondi DM (2006) Is migraine a neuropathic pain syndrome? Curr Pain Headache Rep 10:167–178
Lillis AP, Van Duyn LB, Murphy-Ullrich JE, Strickland DK (2008) LDL receptor-related protein 1: unique tissue-specific functions revealed by selective gene knockout studies. Physiol Rev 88:887–918
Arndt AK, Schafer S, Drenckhahn JD et al (2013) Fine mapping of the 1p36 deletion syndrome identifies mutation of PRDM16 as a cause of cardiomyopathy. Am J Hum Genet 93:67–77
Bjork BC, Turbe-Doan A, Prysak M et al (2010) Prdm16 is required for normal palatogenesis in mice. Hum Mol Genet 19:774–789
Fan X, Wang J, Fan W et al (2014) Replication of migraine GWAS susceptibility loci in Chinese Han population. Headache 54:709–715
Esserlind AL, Christensen AF, Le H et al (2013) Replication and meta-analysis of common variants identifies a genome-wide significant locus in migraine. Eur J Neurol 20:765–772
Ligthart L, de Vries B, Smith AV et al (2011) Meta-analysis of genome-wide association for migraine in six population-based European cohorts. Eur J Hum Genet 19:901–907
Freilinger T, Anttila V, de Vries B, International Headache Genetics Consortium et al (2012) Genome-wide association analysis identifies susceptibility loci for migraine without aura. Nat Genet 44:777–782
Shalizi A, Gaudillière B, Yuan Z et al (2006) A calcium-regulated MEF2 sumoylation switch controls postsynaptic differentiation. Science 311:1012–1017
Flavell SW, Cowan CW, Kim TK et al (2006) Activity-dependent regulation of MEF2 transcription factors suppresses excitatory synapse number. Science 311:1008–1012
Ferrari MD, Odink J, Bos KD et al (1990) Neuroexcitatory plasma amino acids are elevated in migraine. Neurology 40:1582–1586
Lin HY, Wang XF, Ng-Eaton E et al (1992) Expression cloning of the TGF-beta type II receptor, a functional transmembrane serine/threonine kinase. Cell 68:775–785
Law C, Bunyan D, Castle B et al (2006) Clinical features in a family with an R460H mutation in transforming growth factor beta receptor 2 gene. J Med Genet 43:908–916
Cox HC, Lea RA, Bellis C et al (2012) A genome-wide analysis of 'Bounty’ descendants implicates several novel variants in migraine susceptibility. Neurogenetics 13:261–266
Anttila V, Winsvold BS, Gormley P, et al.; North American Brain Expression Consortium; UK Brain Expression Consortium; International Headache Genetics Consortium (2013) Genome-wide meta-analysis identifies new susceptibility loci for migraine. Nat Genet 45:912–917
Russell MB, Olesen J (1995) Increased familial risk and evidence of genetic factor in migraine. BMJ 311:541–544
Persico AM, Napolioni V (2013) Autism genetics. Behav Brain Res 251:95–112
Rudkjobing LA, Esserlind A-L, Olesen J (2012) Future possibilities in migraine genetics. J Headache Pain 13:505–511
Gottesman II, Gould TD (2003) The endophenotype concept in psychiatry: etymology and strategic intentions. Am J Psychiatry 160:636–645
Ruggeri B, Sarkans U, Schumann G, Persico AM (2014) Biomarkers in autism spectrum disorder: the old and the new. Psychopharmacology (Berl) 231:1201–1216
Durham P, Papapetropoulos S (2013) Biomarkers associated with migraine and their potential role in migraine management. Headache 53:1262–1277
Ligthart L, Hottenga JJ, Lewis CM et al (2014) Genetic risk score analysis indicates migraine with and without comorbid depression are genetically different disorders. Hum Genet 133:173–186
De Felice M, Ossipov MH, Wang R et al (2010) Triptan-induced enhancement of neuronal nitric oxide synthase in trigeminal ganglion dural afferents underlies increased responsiveness to potential migraine triggers. Brain 133:2475–2488
Acknowledgments
The authors are grateful to Drs. Maria Dora Morgante, Anna Crapulli, and to the personnel of the library at UCBM for their assistance in collecting the literature reviewed in the present article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Other research by the authors is supported through the Italian Ministry for University, Scientific Research and Technology (PRIN n.2006058195 and n.2008BACT54_002), the Italian Ministry of Health (RFPS-2007-5-640174 and RF-2011-02350537), the Fondazione Gaetano e Mafalda Luce (Milan, Italy), Autism Speaks (Princeton, NJ), the Autism Research Institute (San Diego, CA), and the Innovative Medicines Initiative Joint Undertaking (EU-AIMS, n. 115300).
Conflict of interest
The authors declare that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Persico, A.M., Verdecchia, M., Pinzone, V. et al. Migraine genetics: current findings and future lines of research. Neurogenetics 16, 77–95 (2015). https://doi.org/10.1007/s10048-014-0433-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10048-014-0433-x