
Abstract
Purpose
The use of component separation results in myofascial release and increased rates of fascial closure in abdominal wall reconstruction(AWR). These complex dissections have been associated with increased rates of wound complications with anterior component separation having the greatest wound morbidity. The aim of this paper was to compare the wound complication rate between perforator sparing anterior component separation(PS-ACST) and transversus abdominus release(TAR).
Methods
Patients were identified from a prospective, single institution hernia center database who underwent PS-ACST and TAR from 2015 to 2021. The primary outcome was wound complication rate. Standard statistical methods were used, univariate analysis and multivariable logistic regression were performed.
Results
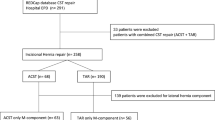
A total of 172 patients met criteria, 39 had PS-ACST and 133 had TAR performed. The PS-ACST and TAR groups were similar in terms of diabetes (15.4% vs 28.6%, p = 0.097), but the PS-ACST group had a greater percentage of smokers (46.2% vs 14.3%, p < 0.001). The PS-ACST group had a larger hernia defect size (375.2 ± 156.7 vs 234.4 ± 126.9cm2, p < 0.001) and more patients who underwent preoperative Botulinum toxin A (BTA) injections (43.6% vs 6.0%, p < 0.001). The overall wound complication rate was not significantly different (23.1% vs 36.1%, p = 0.129) nor was the mesh infection rate (0% vs 1.6%, p = 0.438). Using logistic regression, none of the factors that were significantly different in the univariate analysis were associated with wound complication rate (all p > 0.05).
Conclusion
PS-ACST and TAR are comparable in terms of wound complication rates. PS-ACST can be used for large hernia defects and promote fascial closure with low overall wound morbidity and perioperative complications.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ventral hernia repair (VHR) is one of the most common operations performed in the United States each year [1]. Over two million laparotomies are performed in the United States annually and approximately 20–25% of these patients will go on to develop an incisional hernia [2, 3]. A complicating factor in VHR can be loss of domain caused by a deficiency of abdominal wall muscle and fascia and/or lateral retraction of the abdominal wall with significant protrusion of the abdominal contents which makes fascial closure challenging at time of hernia repair. In some instances, bridging mesh is used when the fascia is not able to be approximated primarily; however, this portends to significantly higher rates of hernia recurrence and wound morbidity [4,5,6]. Many different preoperative and intraoperative techniques have been developed by surgeons in an attempt to enhance the rates of successful primary fascial closure. Most often, a form of component separation technique (CST) is performed, which results in a musculofascial advancement flap, providing a means for fascial edge medialization which can facilitate formal fascial closure [7].
CST is generally divided into two categories: anterior component separation technique (ACST) and posterior component separation (PCST). ACST refers to a posterior rectus sheath release (PRSR) combined with an external oblique release (EOR), whereby the fascia of the external oblique muscle is lacerated and dissected from the underlying internal oblique in an avascular plane [8]. PCST refers to a transversus abdominis release (TAR), which is usually performed in conjunction with a PRSR. PRSR involves making an incision in the posterior rectus sheath, generally just off midline and longitudinally along the entire length of the rectus muscle or at least the length of the hernia defect. During a TAR, an incision is made through the posterior lamella of the internal oblique medial to the neurovascular bundles entering the rectus muscle near the semilunaris. This exposes the transversus abdominus muscle for subsequent release [8, 9]. Both methods can provide several centimeters of release, although the authors favor an ACST over TAR when greater midline mobilization is needed [4, 10, 11].
The significant disadvantage to a traditional ACST and to a lesser extent the TAR is that they are associated with increased rates of wound complications [4, 9, 12]. ACST has been typically reported as having higher rates of wound complication than TAR, with wound complication rates typically ranging from 40 to 60% [12,13,14]. When ACST is performed, large lipocutaneous flaps are developed in order to gain access laterally to the fascia of the external oblique, which leads to the creation of a potential space that is prone to fluid accumulation. During this procedure, the perforating vessels arising from the deep epigastrics are also traditionally transected which can significantly impact the perfusion of overlying skin and subcutaneous tissues [15], which can increase rates of tissue necrosis. With this in mind, a novel technique for ACST was developed in which the peri-umbilical perforator arteries are spared during component separation [16, 17]. By preserving this portion of the blood supply to the flap, perforator sparing ACST (PS-ACST) has led to a reduction in wound complications in comparison to conventional ACST [12].
In this study, a prospectively maintained institutional database was utilized to compare the wound complication rates and other postoperative outcomes between PS-ACST and TAR during open AWR. This study is one of the largest to date comparing anterior component separation and TAR, and the only report directly comparing open PS-ACST with TAR. The authors hypothesize that the wound complication rates, along with related outcomes such as the need for reintervention and hospital readmission, will be comparable between patients with PS-ACST and TAR.
Methods
Patient population
This study was conducted at an 874-bed tertiary care facility in the United States (US) with a referral base extending throughout the entire country. The study took place within the Section of Gastrointestinal and Minimally Invasive Surgery, which performs over 400 open AWR cases annually. Many of the cases involve complex reconstruction, have high rates of CST, and are performed on patients that are at high risk for wound complications, such as patients with mesh infection or fistula.
Study design
Following Institutional Review Board approval, we queried our prospectively maintained institutional database for patients who underwent open ventral hernia repair with PS-ACST or TAR and PRSR, from January 2015–December 2021 Informed consent was obtained from patients in order to have their information entered into the database. Prior to 2015, the perforator sparing technique was not used at our institution. There were a total of four operative surgeons, all of whom were specialty-trained in AWR. Patients under the age of 18 were excluded. Patient characteristics were obtained, including baseline demographics and prior medical and surgical histories. Operative details were recorded, and postoperative outcomes were assessed. Data was entered into the database by a group of trained data analysts with no input from the attending surgeons.
The primary outcome that was assessed in this study were the wound complication rates, which included deep infection, cellulitis, seroma, and superficial wound dehiscence. Secondary outcomes included hernia recurrence, need for re-intervention, length of stay, costs and 30-day readmission. Follow-up was achieved through clinic visits and chart review of abdominal imaging by a full-time research team [18].
Surgical technique
Prehabilitation and preoperative management
Patients were seen preoperatively in the clinic. A history and physical exam were performed, and abdominal imaging, mostly commonly a CT scan was reviewed. Based on a patient’s physical exam and characteristics such as hernia defect size and loss of domain on imaging, the possibility and procedure details of a component separation was discussed with patients. Patient with large defects and loss of domain were also considered for preoperative botulinum toxin A (BTA) chemical component relaxation on a case-by-case basis. There was no definitive defect size that triggered BTA injections. Those who were at high risk for wound complications, such as patients with mesh infection, fistula, ongoing wound infection, or planned ostomy takedown, were considered for placement of a vacuum-assisted closure (VAC) device at the time of operation with delayed primary closure (DPC) of the skin and subcutaneous tissues [19]. Patients were optimized preoperatively targeting factors that place patients at risk for postoperative complications. Weight loss prior to surgery was encouraged through diet and exercise for those who were significantly overweight. There was no strict measure of BMI that contradicted surgery, but patients were evaluated on a case-by case basis before being scheduled for surgery. Diabetic patients were counseled concerning glycemic control with a target A1c of 7.2% or less [20]. If patients were active smokers, surgery was not offered until the patient were abstinent for at least four weeks, often confirmed by urine cotinine test. Standard preoperative antibiotic prophylaxis and thromboembolic prophylaxis were given 1 h prior to surgery.
Intraoperative considerations
A midline laparotomy incision was used for open repair of the hernia. Once the hernia sac was reduced, a lysis of adhesions was performed as needed to free the bowel from the posterior abdominal wall. Tension was applied to each side of the midline fascia by using Kocher clamps. If the fascia came together with minimal tension, then surgeons proceeded with a standard preperitoneal hernia repair without component separation [14, 20, 21]. If it did not, a PRSR was performed. The midline fascial approximation was retested, and if able to approximate without tension, surgeons proceeded with closure and hernia repair. The size of the remaining defect dictated if surgeons next performed ACST or TAR. ACST allows for greater fascial medialization than TAR it is reserved for larger defects. If a defect of greater than 6 cm remained, a PS-ACS was performed on one side. If the fascia could be brought together with a unilateral ACS, then a bilateral procedure was not performed. Otherwise, if the gap after the PRSR was less than 6 cm, then a TAR was typically performed. A bilateral procedure was performed as needed much like the ACS. A complete preperitoneal placement of the mesh was most commonly performed for the PS-ACST [14, 20, 21].
Perforator-sparing anterior component separation
The key component to the PS-ACST is to spare the deep epigastric collateral arteries that perforate through the rectus muscles with the greatest density found approximately 2 cms above to 5 cms below the umbilicus [12, 17]. As the typical subcutaneous planes are developed, the perforating vessels can be individually dissected and preserved, or they can be entirely avoided by dissecting above and below the peri-umbilical “perforator zone”, which is what was most often performed in the current study. The abdomen was marked 2–5 cm above the umbilicus and 8–9 cm lateral. Subcutaneous flaps were developed above and below perforator zone and were taken laterally to approximately the anterior axillary line. Through the superior and inferior dissection, the aponeurosis of the external oblique muscle was incised approximately 2 cm lateral from the border of the rectus sheath. The external oblique was separated from the underlying internal oblique, and the incision in the aponeurosis was carried to or above the costal margin as needed. Through the inferior incision it can be taken as low as the inguinal ligament. The dissection of the external oblique directly lateral to the intact periumbilical tissues is assisted by using a plastic Yankauer suction tip as described by Janis et al. [22]. By sliding the plastic suction tip under the external oblique from superior to inferior, the dissection between the internal and external oblique is facilitated and the external oblique can be transected using cautery applied directly over the suction device. The Yankauer is plastic, so it eliminates the spread of the cautery effects if such an instrument was metal. As mentioned, nearly all PS-ACS procedures were performed in combination with a preperitoneal dissection, which allowed for the placement of an extremely large mesh that extended laterally beyond the area of the external oblique release.
Transversus abdominis release
A PRSR was first performed by longitudinally incising the posterior rectus fascia 1 cm lateral to the linea alba [23]. The fascial incision was made along the entire length of the incision. Typically, this allows for an additional 2–3 cm of medialization of the anterior sheath. The TAR was performed by dissecting the posterior rectus sheath further laterally until the neurovascular bundles, which enter the rectus muscle posteriorly, were identified. A longitudinal incision was made in the posterior lamella of the internal oblique, and the transversus abdominus muscle which is extended at least the length of the hernia but can be taken the full length of the abdomen. The transversalis fascia can be left intact or transected with the muscle, and a pre-transversalis or preperitoneal dissection is taken well laterally to allow closure of the posterior fascial elements, exclude the intestine, and broad mesh coverage.
Data analysis
All data were analyzed using Statistical Analysis Software, version 9.4 (SAS Institute, Inc., Cary, NC). Descriptive statistics were reported as means with corresponding standard deviations where normally distributed and median and interquartile range where non-parametric for continuous variables and percentages for categorical variables. Univariate analyses were performed between the PS-ACST group and the PCS group. Categorical variables were evaluated using Pearson’s chi-square and Fisher’s exact test where appropriate. Continuous and ordinal variables were evaluated using Student’s t-test, Wilcoxon-Mann–Whitney and the Kruskal–Wallis tests. Statistical significance was set at p < 0.05 for the study, which was two-tailed. Multivariable logistic regression analysis was performed to control for potential confounding factors that may impact wound complication rate and were significant on univariate analysis.
Results
There were 172 patients that met the criteria to be included in the study, of which 39 patients underwent PS-ACST and 133 patients who underwent TAR. Baseline demographics and patient characteristics are listed in Table 1. The mean age of patients for the PS-ACST and TAR groups were 62.6 ± 10.3 vs. 60.6 ± 10.7 (p = 0.296). There were no differences in gender (33.3% vs. 50.4% female, p = 0.061), diabetes (15.4% vs 28.6%, p = 0.097), or COPD (5.1% vs 5.3%, p = 0.974). However, patients in the PS-ACST group were significantly more likely to have history of smoking (46.2% vs 14.3%, p < 0.001) and use steroids (21.1% vs 9.1%, p = 0.044). Those in TAR group had a higher BMI (29.7 ± 5.8 vs 32.4 ± 5.8, p = 0.015). Otherwise, the patients were similar in terms of medical comorbidities and ASA classification (all p > 0.05).
Hernia and operative characteristics can be found in Table 2. In both the PS-ACST and TAR groups, most patients had recurrent hernias (58.9% vs 69.9%, p = 0.199). Preoperative botulinum toxin A (BTA) injection was used more frequently in the PS-ACST (43.6% vs 6.0%, p < 0.001). The mean size of the hernia defect was nearly 150cm2 larger in the PS-ACS group (375.2 ± 156.7 cm2 vs 234.4 ± 126.9 cm2; p < 0.001), but mean mesh size was equivalent (1095.5 ± 523.1 vs. 922.3 ± 323.3 cm2; p = 0.704). PS-ACS had greater numbers of CDC Class 3 and 4 wounds (51.2% vs 30.1%, p = 0.044). With this, there tended to be more biologic mesh used in the PS-ACS group, but it did not reach significance (p = 0.077). The mesh was placed in the preperitoneal space for nearly all patients (94.7% vs. 95.3%, p = 0.128). The majority of patients in the PS-ACST group (94.9%) underwent bilateral ACST while 72.5% received a bilateral procedure in the TAR group (p = 0.010). The fascia was able to be approximated in all but 1 of the patients, which was in the PS-ACST group. Planned delayed primary closure [19] was used more frequently in the PS-ACST group (41.0% vs. 19.2%, p = 0.005), due to the presence of CDC Class 3 or 4 wounds. There was no difference between the operative time for the two groups (229 [181–263] mins vs 214 [180–253] mins, p = 0.472).
Table 3 demonstrates the postoperative complications of the two groups. The overall wound complication rate was comparable between the PS-ACST and TAR groups (23.1% vs 36.1%, p = 0.129). The rates of cellulitis (8.1% vs. 7.0%, p = 0.824), deep wound infection (2.7% vs. 5.5%, p = 0.490), superficial wound dehiscence (2.7% vs. 7.8%, p = 0.347), seroma (10.8% vs. 16.4%, p = 0.403), and mesh infection (0.0% vs 1.6%, p = 0.438) were also all comparable. Seroma drainage was required in one patient (2.7%) in the PS-ACST group and 14 patients (11.0%) in the TAR group (p = 0.122). There were two enterotomies, both in the TAR group and both developed a wound complication. There were only two instances of mesh infection, both were in the TAR group, one was a patient who had a heavyweight synthetic mesh and the other had two large pieces of medium weight synthetic mesh with a Seprafilm coating sewn together. The patient who did not have fascial closure achieved did develop a wound complication (Table 4).
Other major complications, such as respiratory failure (7.7% vs 3.0%), acute kidney injury (5.1% vs 5.3%), Deep vein thrombosis (DVT) (15.4% vs 8.3%), and Pulmonary embolism (PE) (2.6% vs 0.8%) were not statistically different (all p > 0.05). There were two deaths, one in each group, one from pulmonary failure secondary to a pneumonia and the second from a massive cardiac event despite pre-operative cardiac clearance. There was no difference in length of stay (8.3 ± 4.4 vs 7.0 ± 3.5, p = 0.063) or OR charges ($22,890 ± 12,686 vs $19,799 ± 9,851, p = 0.188), although total cost was significantly higher in PS-ACST group ($114,696 ± 68,163 vs $88,892 ± 53,741, p = 0.046), which may be secondary to the increase in biologic mesh use. There was a 5.1% 30-day readmission rate for the PS-ACST group and a 14.3% 30-day readmission for the TAR group (p = 0.283). Of the readmissions, 71% were related to wound complications. The hernia recurrence rate in the two groups was comparable (0.0% vs 1.5%, p = 0.411) with a mean follow up time of 12.1 ± 15.0 months vs. 13.9 ± 17.2 months (p = 0.571).
The multivariable logistic regression included history of smoking, steroid use, BMI, hernia defect size, bilateral vs. unilateral CST, DPC, PS-ACST and ci-NPWT (Table 4). Each of these variables were significantly different on the univariate analysis. None of them were found to be independent predictors of wound complications (each p > 0.05).
Discussion
Component separation is an important technique in AWR because it provides a means for myofascial release and leads to increased rates of successful fascial closure [24]. Lack of fascial closure in open abdominal wall reconstruction may be the most predictive factor of hernia recurrence and is associated with an increase in wound complications. However, component separation is also known to increase the rate of postoperative wound complications which is also associated with increased rates of readmission and repair failure [23, 25,26,27]. ACST has been particularly associated with a high wound-related morbidity, reported to be 40–60% in previous studies, due to the creation of large lipocutaneous flaps with compromised blood supply [12, 13, 28]. PS-ACST has been devised as a novel technique to maintain better perfusion of these flaps in order to mitigate the risk of wound complications, in particular skin necrosis and superficial wound breakdown [7, 17]. In this study, the first study directly comparing open PS-ACST with TAR, the rate of wound complication following AWR was moderate overall and equal between the two groups despite PS-ACST being used for larger and more complex hernia defects. The results of this study were strengthened using logistic regression, which did not demonstrate any confounding variables impacting the wound complication rate.
There are a small number of studies that directly compare ACST and TAR [8, 29]. The two largest series comparing these techniques were by Maloney, et al. (n = 775) at our institution, and by Rosen’s group (n = 111) at University Hospitals in Cleveland, OH [4, 30]. Both of these studies demonstrated that conventional anterior component separation leads to higher rates of wound complication than TAR. The rates of wound complication for anterior component separation vs TAR in these studies were 42.9% vs 32.1% and 48.2% vs 25.5%, respectively. In the study by Maloney et al. the perforator sparing technique was found to significantly reduce wound complication rate, but analysis was not performed comparing PS-ACST directly with TAR. Additionally, that study compared operations that occurred over a twelve-year period. The one study that compared endoscopic and minimally invasive anterior component separation to TAR found equivalence in wound complication but with higher wound morbidity rates (43% and 39%, p = 0.11) [29]. However, this study did not take into account open approach as in the present study.
The overall wound complication rate of 15.4% for the PS-ACST group is slightly improved from that previously reported (20.8%) for the first 24 patients who underwent PS-ACST at our institution [12]. This finding suggests an even lower proportion of wound complications in the most recent 15 patients. The rate of superficial wound dehiscence decreased from 13.6% to 2.7%, which may directly reflect the degree of perfusion to the skin [12]. The overall wound complication rate is quite good for complex AWR and is favorable to our previously published wound complication rate for all preperitoneal open ventral hernia repairs (24.9%) at our institution over a ten-year period, including those that did not have a CST [20]. A focus on perioperative optimization through glycemic control, smoking cessation, and diet and exercise, which we pressed for many years, along with delayed primary closure for high risk patients (e.g. mesh infection, fistula, ostomy takedown), have also played a significant role in conjunction with surgical technique in contributing to low wound morbidity in this patient population [19, 20, 31].
The results of the study were strengthened using multivariable logistic regression to control for potential confounding factors that could contribute to wound complication rate and were significant on the univariate analysis. The only factor that was significant on the univariate analysis that would potentially contribute to artificially decrease wound morbidity in the PS-ACST group would be use of closed incision Negative Pressure Therapy (ciNPT). ciNPT has been shown to decrease surgical site occurrences at 30 days postoperatively in patients undergoing incisional hernia repair [32, 33]. All other factors (e.g. smoking, operative time, defect size) would be risk factors for increasing wound complication rate [20, 34]. Furthermore, aside from an increased use of ciNPT over the last four years, other operative techniques and the perioperative management strategies have remained constant. For example, over the entire duration of the study, all patients underwent the same prehabilitation and were enrolled in an enhanced recovery after surgery pathway immediately before and after their surgery. The same set of surgeons operated throughout the period that this study took place.
Given the fascial closure-CST algorithm described in the methods, it would be expected that the PS-ACST had a much larger defect size than the TAR group. The only patient where primary fascial closure could not be achieved was in the PS-ACST group, and that patient did develop a wound complication. There was a clinically significant increase in the percentage of patients with pre-operative botulinum toxin A (BTA) injected in the PC-ACST group which was reflective of patients having larger defect sizes and significant loss of domain. We have previously described our results using BTA in a comparative study, which showed a significant improvement in fascial closure rates [35, 36].
Wound complications had a clinically significant impact on the patients in this study. All un-planned return trips to the operating room were attributable to wound complications, as were the vast majority (71%) of 30-day readmission. The result of wound complications includes continued engagement with the health care system and a downstream economic and productivity effect. A previous study at this institution demonstrated that a wound infection leads to a follow-up cost of over $20,000 per patient [37]. Wound complications are also known to result in a three to fivefold risk of hernia recurrence [20, 23, 38]. Hernia recurrence was similarly low between the two groups in this study, but follow-up time should be extended to get the most accurate assessment of recurrence for both groups.
It should be acknowledged that there are limitations to our study. This study was performed at a single center with a group of surgeons that all have similar practice styles. The relatively small sample size for individual outcomes, such as wound complications and need for operative reintervention, makes it difficult to show a significant difference between two groups. In general, Type 2 error is common in studies that have outcomes with small sample sizes [39]. However, the aim was to compare patients over the same time frame as to eliminate other variables that have been changed (e.g., prehabilitation) that may influence wound complication rate. In addition, minimally invasive component separation is not included and should compare the open to minimally invasive component separation techniques.
Conclusion
PS-ACS is a relatively new abdominal wall reconstructive technique that has proven to reduce the wound morbidity of component separation in complex AWR. PS-ACST allows for fascial medialization in patients with very large fascial defects with similar rates of wound morbidity to PCST techniques. In instances where a large degree of myofascial release is needed, PS-ACST should be considered for surgeons who have experience performing this technique.
References
Poulose BK, Shelton J, Phillips S et al (2012) Epidemiology and cost of ventral hernia repair: making the case for hernia research. Hernia 16:179–183. https://doi.org/10.1007/s10029-011-0879-9
Pauli EM, Rosen MJ (2013) Open ventral hernia repair with component separation. Surg Clin North Am 93:1111–1133
Fink C, Baumann P, Wente MN et al (2013) Incisional hernia rate 3 years after midline laparotomy. Brit J Surg. https://doi.org/10.1002/bjs.9364
Maloney SR, Schlosser KA, Prasad T et al (2019) Twelve years of component separation technique in abdominal wall reconstruction. Surgery (United States) 166:435–444
Holihan JL, Askenasy EP, Greenberg JA et al (2016) Component separation vs. bridged repair for large ventral hernias: a multi-institutional risk-adjusted comparison, systematic review, and meta-analysis. Surg Infect (Larchmt) 17:17–26. https://doi.org/10.1089/sur.2015.124
Giordano S, Garvey PB, Baumann DP et al (2017) Primary fascial closure with biologic mesh reinforcement results in lesser complication and recurrence rates than bridged biologic mesh repair for abdominal wall reconstruction: a propensity score analysis. Surgery (United States) 161:499–508
Ramirez OM, Ruas E, Dellon AL (1990) “Components separation” method for closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg 86:519–526. https://doi.org/10.1097/00006534-199009000-00023
Kumar S, Edmunds RW, Dowdy C et al (2018) Anterior versus posterior component separation. Plast Reconstr Surg 142:47S-53S. https://doi.org/10.1097/PRS.0000000000004852
Novitsky YW, Elliott HL, Orenstein SB, Rosen MJ (2012) Transversus abdominis muscle release: a novel approach to posterior component separation during complex abdominal wall reconstruction. Am J Surg 204:709–716. https://doi.org/10.1016/j.amjsurg.2012.02.008
Majumder A, Martin-del-Campo LA, Miller HJ et al (2020) Evaluation of anterior versus posterior component separation for hernia repair in a cadaveric model. Surg Endosc 34:2682–2689. https://doi.org/10.1007/s00464-019-07046-9
Loh CYY, Nizamoglu M, Shanmugakrishnan RR et al (2018) Comparing transversus abdominus release and anterior component separation techniques in reconstructing midline hernias: a cadaveric study. J Plast Reconstr Aesthetic Surg 71:1507–1517
Elhage SA, Marturano MN, Prasad T et al (2020) Impact of perforator sparing on anterior component separation outcomes in open abdominal wall reconstruction. Surg Endosc 1:3. https://doi.org/10.1007/s00464-020-07888-8
Gonzalez R, Rehnke RD, Ramaswamy A et al (2005) Components separation technique and laparoscopic approach: a review of two evolving strategies for ventral hernia repair. Am Surg 71:598–605. https://doi.org/10.1177/000313480507100713
Katzen MM, Kercher KW, Sacco JM et al (2022) Open preperitoneal ventral hernia repair: prospective observagtional study of quality improvement outcomes over 18 years and 1842 patients. Surgery. https://doi.org/10.1016/j.surg.2022.07.042
Shao JM, Alimi Y, Conroy D, Bhanot P (2020) Outcomes using indocyanine green angiography with perforator-sparing component separation technique for abdominal wall reconstruction. Surg Endosc 34:2227–2236. https://doi.org/10.1007/s00464-019-07012-5
Clarke JM (2010) Incisional hernia repair by fascial component separation: results in 128 cases and evolution of technique. Am J Surg 200:2–8. https://doi.org/10.1016/j.amjsurg.2009.07.029
Ghali S, Turza KC, Baumann DP, Butler CE (2012) Minimally invasive component separation results in fewer wound-healing complications than open component separation for large ventral hernia repairs. J Am Coll Surg 214:981–989. https://doi.org/10.1016/j.jamcollsurg.2012.02.017
Baucom RB, Ousley J, Feurer ID et al (2016) Patient reported outcomes after incisional hernia repair—establishing the ventral hernia recurrence inventory. Am J Surg 212:81–88. https://doi.org/10.1016/j.amjsurg.2015.06.007
Ayuso SA, Elhage SA, Aladegbami BG et al (2022) Delayed primary closure (DPC) of the skin and subcutaneous tissues following complex, contaminated abdominal wall reconstruction (AWR): a propensity-matched study. Surg Endosc 36:2169–2177. https://doi.org/10.1007/S00464-021-08485-Z
Heniford BT, Ross SW, Wormer BA et al (2020) Preperitoneal ventral hernia repair: a decade long prospective observational study with analysis of 1023 patient outcomes. Ann Surg 271:364–374. https://doi.org/10.1097/SLA.0000000000002966
Novitsky Y, Porter J, Rucho ZC et al (2006) Open preperitoneal retrofascial mesh repair for multiply recurrent ventral incisional hernias. J Am Coll Surg 203:283–289. https://doi.org/10.1016/J.JAMCOLLSURG.2006.05.297
Janis JE, Khansa I (2015) Evidence-based abdominal wall reconstruction: the maxi-mini approach. Plast Reconstr Surg 136:1312–1323. https://doi.org/10.1097/PRS.0000000000001831
Maloney SR, Schlosser KA, Prasad T et al (2020) The impact of component separation technique versus no component separation technique on complications and quality of life in the repair of large ventral hernias. Surg Endosc 34:981–987. https://doi.org/10.1007/s00464-019-06892-x
Ko JH, Wang EC, Salvay DM et al (2009) Abdominal wall reconstruction: lessons learned from 200 “components separation” procedures. Arch Surg 144:1047–1055. https://doi.org/10.1001/archsurg.2009.192
Butler CE (2018) Discussion. Plast Reconstr Surg 142:54S-55S. https://doi.org/10.1097/PRS.0000000000004854
Ayuso SA, Colavita PD, Augenstein VA et al (2022) Nationwide increase in component separation without concomitant rise in readmissions: a nationwide readmissions database analysis. Surgery 171:799–805. https://doi.org/10.1016/J.SURG.2021.09.012
Alkhatib H, Tastaldi L, Krpata DM et al (2019) Outcomes of transversus abdominis release (TAR) with permanent synthetic retromuscular reinforcement for bridged repairs in massive ventral hernias: a retrospective review. Hernia 24:341–352. https://doi.org/10.1007/S10029-019-02046-Z
Jones CM, Winder JS, Potochny JD, Pauli EM (2016) Posterior component separation with transversus abdominis release. Plast Reconstr Surg 137:636–646. https://doi.org/10.1097/01.prs.0000475778.45783.e2
Parent B, Horn D, Jacobson L et al (2017) Wound morbidity in minimally invasive anterior component separation compared to transversus abdominis release. Plast Reconstr Surg 139:472–479. https://doi.org/10.1097/PRS.0000000000002957
Krpata DM, Blatnik JA, Novitsky YW, Rosen MJ (2012) Midwest surgical association posterior and open anterior components separations: a comparative analysis. Am J Surg 203:318–322. https://doi.org/10.1016/j.amjsurg.2011.10.009
Walming S, Angenete E, Block M et al (2017) Retrospective review of risk factors for surgical wound dehiscence and incisional hernia. BMC Surg 17:1–6. https://doi.org/10.1186/s12893-017-0207-0
Bueno-Lledó J, Franco-Bernal A, Garcia-Voz-Mediano T et al (2020) Prophylactic single-use negative pressure dressing in closed surgical wounds after incisional hernia repair a randomized, controlled trial. Ann Surg XX. https://doi.org/10.1097/SLA.0000000000004310
Zwanenburg PR, Tol BT, Obdeijn MC et al (2020) Meta-analysis, meta-regression, and grade assessment of randomized and nonrandomized studies of incisional negative pressure wound therapy versus control dressings for the prevention of postoperative wound complications. Ann Surg 272:81–91. https://doi.org/10.1097/SLA.0000000000003644
Finan KR, Vick CC, Kiefe CI et al (2005) Predictors of wound infection in ventral hernia repair. Am J Surg 190:676–681. https://doi.org/10.1016/j.amjsurg.2005.06.041
Deerenberg EB, Elhage SA, Raible RJ, et al (2021) Image-guided botulinum toxin injection in the lateral abdominal wall prior to abdominal wall reconstruction surgery: review of techniques and results. Skelet Radiol 50:1-7
Deerenberg EB, Shao JM, Elhage SA et al (2021) Preoperative botulinum toxin A injection in complex abdominal wall reconstruction– a propensity-scored matched study. Am J Surg 222:638–642. https://doi.org/10.1016/j.amjsurg.2021.01.010
Augenstein VA, Colavita PD, Wormer BA et al (2015) CeDAR: Carolinas equation for determining associated risks. J Am Coll Surg 221:S65–S66. https://doi.org/10.1016/j.jamcollsurg.2015.07.145
Rosen MJ, Bauer JJ, Harmaty M et al (2017) Multicenter, prospective, longitudinal study of the recurrence, surgical site infection, and quality of life after contaminated ventral hernia repair using biosynthetic absorbable mesh: the COBRA study. Ann Surg 265:205–211. https://doi.org/10.1097/SLA.0000000000001601
Bababekov YJ, Stapleton SM, Mueller JL et al (2018) A proposal to mitigate the consequences of type 2 error in surgical science. Ann Surg 267:621–622. https://doi.org/10.1097/SLA.0000000000002547
Funding
No funding was received to support this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr. Heniford receives surgical research/education grants as well as honoraria for speaking from W.L. Gore and did so within the last 24 months from Allergan. Dr. Augenstein receives speaking honoraria from Medtronic, Allergan, Intuitive, Acelity, and Bard. Dr. Kercher received honoraria for speaking from Bard and Ethicon. The additional authors have nothing to disclose. No funding was received for this paper.
Ethical approval
Ethical approval was agreed by the ethical committee of the institution.
Human and animal rights
This study including human participants has been performed in accordance with the ethical standards of the Declaration of Helsinki and its later amendments.
Informed consent
Informed consent was appropriately obtained for patients included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sacco, J., Ayuso, S.A., Salvino, M.J. et al. Preservation of deep epigastric perforators during anterior component separation technique (ACST) results in equivalent wound complications compared to transversus abdominis release (TAR). Hernia 27, 819–827 (2023). https://doi.org/10.1007/s10029-023-02811-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-023-02811-1