
Abstract
Introduction
Anterior component separation (ACS) is a well-established, highly functional technique to achieve fascial closure in complex abdominal wall reconstruction (AWR). Unfortunately, ACS is also associated with an increased risk of wound complications. Perforator sparing ACS (PS-ACS) has more recently been introduced to maintain the subcutaneous perforators derived from the deep epigastric vessels. The aim of this study is to evaluate wound-related outcomes in patients undergoing open AWR after implementation of a PS-ACS technique.
Methods
A prospectively collected database were queried for patients who underwent open AWR and an ACS from 2006 to 2018. Patients who underwent PS-ACS were compared to patients undergoing ACS using standard statistical methods. Patients undergoing concomitant panniculectomy were included in the standard ACS group.
Results
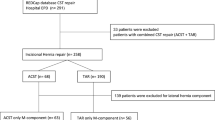
In total, 252 patients underwent ACS, with 24 (9.5%) undergoing PS-ACS. Age and specific comorbidities were similar between groups (all p > 0.05) except for the PS-ACS groups having a higher rate of prior tobacco use (45.8% vs 19.6%, p = 0.003). Mean hernia defect area was 381.6 ± 267.0 cm2 with 64.3% recurrent hernias, and both were similar between groups (all p > 0.05). The PS-ACS group did have more complex wounds with more Ventral Hernia Working Group Grade 3 and 4 hernias (p = 0.04). OR time and length of stay were similar between groups (all p > 0.05). Despite increased complexity, wound complication rates were much lower in the PS-ACS group (20.8% vs 46.1%, p = 0.02), and all specific wound complications were lower but not statistically different. Hernia recurrence rate was similar between PS-ACS and ACS groups (4.2% vs 7.0%, p > 0.99) with mean follow-up of 27.7 ± 26.9 months.
Conclusions
In complex AWR, preservation of the deep epigastric perforating vessels during ACS significantly lowers the rates of wound complications, despite its performance in more complex patients with an increased risk of infection. PS-ACS should be performed preferentially over a standard ACS whenever possible.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Over 350,000 ventral hernia repairs (VHR) are performed annually in the United States, which makes the operation one of the most common in the country [1]. Mesh combined with complete fascial closure is superior to bridging a large defect with mesh and provides the most functional, cosmetic, and durable outcome with fewer complications [2,3,4,5,6,7]. With our ability to salvage patients following major trauma, abdominal infections, other complex abdominal issues that result in open abdomens or large ventral defects, this has led to the development of several techniques to dependably release and medialize the fascia and achieve midline fascial closure. One of the first of these operations, more newly labelled components separation techniques (CST), was first described in 1920 by Gibson, where he gained laxity of the of the abdominal wall by lacerating the lateral anterior rectus sheath [8]. Albanese in 1951 and Young in the 1960′s, wrote about incising the external oblique to help repair a large abdominal defects [9, 10]. However, these CSTs were not popularized until 1990 when Ramirez published on what has come to be known as anterior component separation (ACS) [11].
Since that time, ACS has become a well-established technique to aid in achievement of fascial closure in complex abdominal wall reconstruction (AWR). The procedure as described includes mobilization of the rectus abdominis muscle to the midline by means of releases of the external oblique muscle and fascia. Development of large musculofascial flaps allows for fascial approximation of defects that are much larger than would otherwise be able to be closed. However, access to the external oblique aponeurosis typically requires mobilization of the skin and subcutaneous tissue from the fascia over a very broad area of the abdomen that markedly increases wound related complications which can reach greater than 60% [12].
In response to this increased risk, technical modifications have been made to the originally described procedure. One such modification is the perforator sparing ACS (PS-ACS) which preserves the perforators from the deep epigastric vessels [13]. Well described in plastic and reconstructive surgery literature, maintaining epigastric perforators can sustain large myocutaneous flaps and resist tissue necrosis and infection [14,15,16,17,18]. The aim of this study is to evaluate ACS wound-related and overall outcomes after implementation of a PS-ACS technique.
Materials and methods
Study design
After obtaining approval from the Institutional Review Board of Carolinas Medical Center, a prospective single institution database were queried for all patients undergoing open AWR with ACS (2006–2018). Patients were split into a standard ACS group, and a PS-ACS group. PS-ACS technique was adopted in 2015. Patients undergoing concomitant panniculectomy were included in the standard ACS group. The primary outcome of this study was wound complications. Secondary outcomes were post-operative complications, length of stay, and hernia recurrence. Wound complications were defined as seroma requiring intervention, cellulitis requiring antibiotics, superficial wound breakdown, wound infection requiring antibiotics, fascial dehiscence, and fistula. For patients who developed more than one wound complication, they were counted as one total wound complication.
Surgical technique
All ACS were performed at Carolinas Medical Center by specialized surgeons. Our algorithm for performing an ACS is based on the required length of release to achieve fascial closure. ACS is preferentially chosen over a Transversus Abdominis Release (TAR) when there is a large defect. After performing an adhesiolysis of the intestine from the abdominal wall and releasing the skin and subcutaneous tissue back to normal fascia, medial tension is applied to each side of the abdominal wall using Kocher clamps. If there is a gap, the first portion of a release is performed by cutting the posterior rectus sheath on both sides of the abdomen the full length of the hernia defect. This typically affords 3–5 cm of release to the midline. While applying tension pulling the abdominal wall together once more, if the defect is greater than 6 cm, the authors will perform an ACS at least on one side. The authors believe that an ACS affords a greater amount of release compared to a TAR. Reapproximating the midline is, obviously, a major component of AWR in complex and large hernias. Indeed, it has been emphasized as a means to significantly reduce recurrence rates. ACS is performed only in the largest and most complex hernias where closure would not be achievable with a TAR alone. As previously described, the standard ACS procedure begins by elevating the skin and subcutaneous fat from the midline to approximately the anterior axillary line, and ligating or cauterizing all perforators that are encountered [7]. Then an incision is made in the external oblique aponeurosis approximately 2 cm lateral to the border of the rectus sheath. The muscle of the external oblique is then separated from the underlying internal oblique. This is extended according to the surgeon’s judgement, as superior as above the costal margin, and as inferior as the inguinal ligament. In 2015, a perforator sparing technique was adopted whenever possible. This is performed by meticulous dissection to maintain perforators of the deep epigastric vessels, while still creating a lateral dissection to allow for incision of external oblique. These periumbilical perforators, approximately 2 cm above and 5 cm below the umbilicus, are identified and preserved in one of two ways. The first technique involves leaving a wedge of periumbilical fat that is undisturbed while dissection is carried laterally. The second involves making a tunnel at least 2 cm above the umbilicus that extends laterally, allowing for continued dissection of the plane superiorly and inferiorly. A depiction of the perforator sparing dissection can be seen in Fig. 1. Nearly all procedures were accompanied by a posterior rectus sheath release (PRSR) to maximize fascial release and ensure fascial closure. Most repairs were performed utilizing a preperitoneal dissection, to allow for placement of a very large piece of mesh which is excluded from the intra-abdominal contents. This technique allows for extension of the mesh laterally, far beyond the location of the external oblique release. The peritoneum is mobilized circumferentially from the abdominal wall and does not require a posterior component separation to be performed. This technique, even in these large, complex, and recurrent hernias, can be completed in nearly all cases. The dissection is often begun either in the space of Retzius or at the falciform and extended laterally. Dissection can then be continued bluntly in a lateral to medial approach towards the midline. This technique has been previously described in detail [19].

Perforating vessels are identified and preserved during dissection allowing for a tunnel to be created lateral to the vessels
Pre-habilitation and wound management
This study covers a large time period, over which peri-operative management and techniques have evolved. For example, patients now undergo risk factor modification, targeting active smokers, diabetics with a HgbA1C > 7.2, and obese patients with a BMI > 30. Data on pre-habilitation have been utilized at our institution to create the CeDAR app which allows for objective assessment of patient’s pre-operative risk [20]. Furthermore, patients with contaminated wounds, who were not excluded from this study, are more recently managed with VAC-assisted delayed primary closure (DPC).
Statistical analysis
Descriptive statistics were reported as means with corresponding standard deviations for continuous variables, and percentages for categorical variables. Categorical variables were evaluated using Pearson’s Chi-squared tests and Fisher’s exact test when appropriate. Continuous and ordinal variables were evaluated using Wilcoxon-Mann–Whitney and Kruskal–Wallis tests. Statistical significance was set at p ≤ 0.05, and all reported P-values are two-tailed. Data were analyzed using Statistical Analysis Software, version 9.3 (SAS Institute, Inc., Cary, NC).
Results
In total, 252 patients underwent unilateral or bilateral ACS or PS-ACS during the study period, with 24 patients undergoing PS-ACS. Patient characteristics can be seen in Table 1. The PS-ACS group had a higher overall number of comorbidities (p = 0.005) and a greater rate of history of tobacco use (p = 0.003), however all other demographics, including rates of specific comorbidities and ASA classes, were similar between the two groups (all p > 0.05).
Hernia and operative characteristics can be seen in Table 2. The PS-ACS a higher rate of incarcerated hernias (p = 0.008), but similar rate of recurrent hernias (p = 0.80). While hernia area was similar (p > 0.05), the PS-ACS group had more complex hernias with higher rates of Ventral Hernia Working Group (VHWG) grade 3 (contaminated) and 4 (infected) hernias (p = 0.04). Bilateral ACS rates were similar between groups (p = 0.63). As expected, there were no panniculectomies performed in the PS-ACS group. In both groups, the majority of meshes were placed in the pre-peritoneal space. Mesh type did differ between the groups, with the ACS groups having more synthetic mesh used and the PS-ACS group having more biologic mesh used (p = 0.04) due to the increased level of wound contamination. Finally, due to the increased wound grade, the PS-ACS group was more likely to undergo planned DPC than the ACS group (p < 0.001).
Post-operative outcomes can be found in Table 3. Length of stay and non-wound related complications were similar between the two groups (all p > 0.05). Specific wound complications were similar between standard ACS and PS-ACS (all p > 0.05); however, overall wound complications were much lower in the PS-ACS group (20.8% vs 46.1%, p = 0.02). Readmission rates at 30 days, 30-day return to the operating room, and hernia recurrence were all similar (all p > 0.05).
A subgroup analysis was performed within the group of 228 ACS patients comparing those who underwent concomitant panniculectomy (n = 131) to those who did not (n = 97). This analysis found that there was no significant difference in overall wound complications between the ACS patients undergoing concomitant panniculectomy versus those who did not (51.2% vs 39.2%, p = 0.07). When evaluating specific wound complications within this subgroup, the concomitant panniculectomy patients had a higher rate of superficial wound breakdown (31.5% vs 16.3%, p = 0.01), however, all other specific wound complication rates (seroma requiring intervention, cellulitis requiring antibiotics, wound infection, and mesh infection) were similar (all p > 0.05).
Discussion
Wound complications are the major morbidity of complex AWR, are expensive, and a major predictor of hernia recurrence. Surgical site occurrences (SSO) increase the risk of AWR failure by greater than threefold [19, 21, 22]. The pervasive challenge in hernia operations employing component separation, especially ACS with large myofascial flap dissection and release, is the increased risk of wound occurrences and infections. The overall wound complication rate of 46% in the standard ACS cohort in the current study is consistent with previously described series [12, 19, 23]. Beyond the comorbidities of the patients, which markedly affect wound healing, the challenge is anatomical. The blood supply to the skin and subcutaneous tissues of the abdominal wall are supplied by direct cutaneous vessels, such as the superficial circumflex iliac and the superficial inferior epigastric arteries, and by perforating musculocutaneous vessels, which arise from the deep inferior and superior epigastric arteries. These perforators of the deep epigastric arcade supply the rectus muscle and the overlying skin in the midline. Gaining access to the length of the external oblique to perform an ACS traditionally has been performed by transecting these transabdominal, perforating blood vessels which can lead to tissue ischemia, impairing wound healing and lead to skin necrosis, wound dehiscence, infection, and hernia recurrence [24]. To remedy this known morbidity, PS-ACS aims to maintain the aforementioned established blood flow in an attempt to decrease postoperative wound complications [13, 18].
In our review of over 250 anterior component separations, the PS-ACS patients had higher overall number of comorbidities and tobacco use, however all other demographics, including rates of specific comorbidities and ASA classes were similar. While demographics were also similar, there were some important differences in hernia and operative characteristics. The PS-ACS group had more contaminated and infected cases (VHWG grade 3 and 4), resulting in more biologic mesh use and more frequent wound DPCs, and no cases with concomitant panniculectomy. Notably however, both groups had similar hernia defect size, and similar rates of recurrent hernias, and the need for bilateral anterior component separations. The vast majority of cases in both cohorts had mesh placed in the pre-peritoneal space, and the operative time was similar between the groups. The groups had similar length of stay, similar rate of recurrence, and similar inpatient complications. As expected, the outcomes that differed involved wound complications, where the PS-ACS group had lower rates of overall wound, no cases of mesh infection, and one recurrence, with over 18 months of follow-up in the PS-ACS group.
Hernia recurrence is traditionally the primary outcome for which to measure the success of AWR. Even with continued improvement in our understanding of physiology and refining our surgical technique, hernia recurrence with component separation has been described as anywhere between 5 and 9% in the literature, which is consistent with our ACS cohort [12, 16, 19, 23]. Previous studies regarding preservation of perforator vasculature have shown it to decrease wound complications without a decrease in hernia recurrence rates. Saulis et al. suggest wound breakdown of 8.3% (1/12), infection of 8.3% (1/12) and no statistically significant difference in recurrence rates using open perforator sparing component separation [17]. Lowe et al. in an effort to decrease technical difficulty while maintaining periumbilical perforators introduced endoscopic balloon dissection. In their limited cohort, they describe recurrence of 14% [25]. Clarke et al. continued endoscopic dissection to spare periumbilical perforators in 2010 and in their cohort describe a 13.8% recurrence rate with 5 reoperations [16]. While not statistically significant, the PS-ACS cohort in our study demonstrated a 4.2% recurrence rate compared to 7% recurrence in the ACS cohort, and required no reoperations. These findings are despite the fact that our PS-ACS cohort had more complex hernias with higher rates of VHWG grade 3 and 4 hernias (VHWG grade 3: 45.8% to 38.6%, p = 0.04; grade 4: 20.8% to 7.0%, p = 0.04).
By maintaining epigastric perforators to the myocutaneous flaps, our PS-ACS group demonstrated a 25% decrease in overall wound complications (20.8% to 46.1% p = 0.02); this is again despite those patients being more comorbid. Given that our population is becoming increasingly comorbid, both pre-habilitation and choosing an operative technique to minimize complications is very helpful. Our hernia center aggressively manages patient’s modifiable factors in an attempt to reduce complications. Patients now undergo risk factor modification, targeting active smokers, diabetics with a HgbA1C > 7.2%, and obese patients with a BMI > 30 kg/m2.[20] As our group has previously detailed, for every point of BMI > 26 kg/m2, there exists a 1.066 times increased wound complication rate [19, 20, 26]. If we aggressively manage patient’s risk factors preoperatively, we should also choose the operative technique that maintains the lowest risk of complication. Moving forward, PS-ACS should be used preferentially to preserve the epigastric perforating vessels, especially in complex patients, in order to preserve as much blood flow as possible, enhance wound healing, and decrease wound complication rates.
Despite advances in perioperative care over the 12-year course of the study group and the majority of PS-ACS occurring more recently, LOS did not differ significantly between the two groups. This, almost by definition, is a very complex group of patients with large, re-operative, challenging operations. This group did experience a longer length of stay compared to the previously published cohort of all preperitoneal ventral hernia repairs [19]. While PS-ACS patients perioperative care is much more likely to have been influenced by enhanced recovery principles given that the technique was instituted in 2015, this did not seem to affect the LOS. However, the lack of improvement in LOS may be in part due to the significantly higher rate of VHWG Grade III and IV hernias, as well as the higher rate of delayed primary closures, which are generally taken back to the operating room on post-operative day five for final closure.
Limitations of this study include the small sample size in the PS-ACS group. Although overall wound complication rates were significantly reduced in the PS-ACS group, individual complications were not. While fewer individual SSO are detailed, we are unable to reach a level of statistical significance, likely due to the smaller sample size. Furthermore, this study could not show a statistically significant difference in recurrence rate despite only one recurrence in the PS-ACS group, again likely due to the small sample size. In addition, small sample sizes always carry an increased chance for Type II error within a study. Although this study is limited in size, it is still one of the largest perforator sparing component separation cohorts at this time. Additional limitations are the inability to perform panniculectomy concomitantly due to the inherent anatomy resected. Concomitant panniculectomy carries its own inherent wound risks that have been previously described [23, 27, 28]. While a concomitant panniculectomy may incur increased wound complications, our analysis of patients in the ACS group undergoing concomitant panniculectomy showed that they had a similar rate of overall wound complications compared to ACS patients who did not undergo panniculectomy. This leads us to believe that concomitant panniculectomy is likely not responsible for the ACS groups higher overall wound complication rates. In addition, beginning in 2008 and increasing over time, patients with contaminated wounds, who were not excluded from this study, were managed with VAC-assisted delayed primary closure (DPC), in an attempt to decrease wound complications in contaminated cases. A higher rate of DPCs were performed in the PS-ACS group, however, this correlates to the fact that the PS-ACS group had significantly higher rates of VHWG Grade III and IV hernias.
In conclusion, PS-ACS reduces wound complications in patients undergoing complex AWR, maintains similar recurrence rates, and does not increase operative time. This technique should be preferentially utilized in AWR when possible. Further research into the benefits of PS-ACS will be important, as it can be hypothesized that an improvement in wound complication rate would decrease recurrence rates, however, given the current small sample sizes, this cannot yet be determined.
References
Poulose BK, Shelton J, Phillips S, Moore D, Nealon W, Penson D, Beck W, Holzman MD (2012) Epidemiology and cost of ventral hernia repair: making the case for hernia research. Hernia 16:179–183. https://doi.org/10.1007/s10029-011-0879-9
Booth JH, Garvey PB, Baumann DP, Selber JC, Nguyen AT, Clemens MW, Liu J, Butler CE (2013) Primary fascial closure with mesh reinforcement is superior to bridged mesh repair for abdominal wall reconstruction. J Am Coll Surg 217:999–1009. https://doi.org/10.1016/j.jamcollsurg.2013.08.015
Burger JWA, Luijendijk RW, Hop WCJ, Halm JA, Verdaasdonk EGG, Jeekel J, Pappas TN, Lucas CE, Pellegrini CA, Easter DW, Fischer JE, Mathes SJ, Way LW, Debas HT, Jones RS (2004) Long-term follow-up of a randomized controlled trial of suture versus mesh repair of incisional hernia. Ann Surg 240:578–585. https://doi.org/10.1097/01.sla.0000141193.08524.e7
De Silva GS, Krpata DM, Hicks CW, Criss CN, Gao Y, Rosen MJ, Novitsky YW (2014) Comparative radiographic analysis of changes in the abdominal wall musculature morphology after open posterior component separation or bridging laparoscopic ventral hernia repair. J Am Coll Surg 218:353–357. https://doi.org/10.1016/j.jamcollsurg.2013.11.014
Holihan JL, Askenasy EP, Greenberg JA, Keith JN, Martindale RG, Roth JS, Mo J, Ko TC, Kao LS, Liang MK, Ventral Hernia Outcome Collaboration Writing Group (2016) Component separation vs. bridged repair for large ventral hernias: a multi-institutional risk-adjusted comparison, systematic review, and meta-analysis. Surg Infect (Larchmt) 17:17–26. https://doi.org/10.1089/sur.2015.124
Luijendijk RW, Hop WC, van den Tol MP, de Lange DC, Braaksma MM, IJzermans JN, Boelhouwer RU, de Vries BC, Salu MK, Wereldsma JC, Bruijninckx CM, Jeekel J, (2000) A comparison of suture repair with mesh repair for incisional hernia. N Engl J Med 343:392–398. https://doi.org/10.1056/NEJM200008103430603
Maloney SR, Schlosser KA, Prasad T, Kasten KR, Gersin KS, Colavita PD, Kercher KW, Augenstein VA, Heniford BT (2019) Twelve years of component separation technique in abdominal wall reconstruction. Surgery (United States). 166:435–444
Gibson CL (1920) Operation for cure of large ventral hernia. Ann Surg 72:214–217. https://doi.org/10.1097/00000658-192008000-00014
Albanese AR (1951) [Gigantic median xipho-umbilical eventration; method for treatment]. Rev Asoc Med Argent 65:376–378
Young D (1961) Repair of epigastric incisional hernia. Br J Surg 48:514–516. https://doi.org/10.1002/bjs.18004821109
Ramirez OM, Ruas E, Dellon AL (1990) “Components separation” method for closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg 86:519–526. https://doi.org/10.1097/00006534-199009000-00023
Gonzalez R, Rehnke RD, Ramaswamy A, Smith CD, Clarke JM, Ramshaw BJ (2005) Components separation technique and laparoscopic approach: a review of two evolving strategies for ventral hernia repair. Am Surg 71:598–605
Ghali S, Turza KC, Baumann DP, Butler CE (2012) Minimally invasive component separation results in fewer wound-healing complications than open component separation for large ventral hernia repairs. J Am Coll Surg 214:981–989. https://doi.org/10.1016/j.jamcollsurg.2012.02.017
Allen RJ, Treece P (1994) Deep inferior epigastric perforator flap for breast reconstruction. Ann Plast Surg 32:32–38. https://doi.org/10.1097/00000637-199401000-00007
Azuma R, Morimoto Y, Masumoto K, Nambu M, Takikawa M, Yanagibayashi S, Yamamoto N, Kikuchi M, Kiyosawa T (2008) Detection of skin perforators by indocyanine green fluorescence nearly infrared angiography. Plast Reconstr Surg 122:1062–1067. https://doi.org/10.1097/PRS.0b013e3181858bd2
Clarke JM (2010) Incisional hernia repair by fascial component separation: results in 128 cases and evolution of technique. Am J Surg 200:2–8. https://doi.org/10.1016/j.amjsurg.2009.07.029
Saulis AS, Dumanian GA (2002) Periumbilical rectus abdominis perforator preservation significantly reduces superficial wound complications in “separation of parts” hernia repairs. Plast Reconstr Surg 109:2275–2280. https://doi.org/10.1097/00006534-200206000-00016. discussion 2281–2282
Shao JM, Alimi Y, Conroy D, Bhanot P (2019) Outcomes using indocyanine green angiography with perforator-sparing component separation technique for abdominal wall reconstruction. Surg Endosc. https://doi.org/10.1007/s00464-019-07012-5
Heniford BT, Ross SW, Wormer BA, Walters AL, Lincourt AE, Colavita PD, Kercher KW, Augenstein VA (2020) Preperitoneal ventral hernia repair: a decade long prospective observational study with analysis of 1023 patient outcomes. Ann Surg 271:364–374. https://doi.org/10.1097/SLA.0000000000002966
Augenstein VA, Colavita PD, Wormer BA, Walters AL, Bradley JF, Lincourt AE, Horton J, Heniford BT (2015) CeDAR: carolinas equation for determining associated risks. J Am Coll Surg 221:S65–S66. https://doi.org/10.1016/j.jamcollsurg.2015.07.145
Cobb WS, Warren JA, Ewing JA, Burnikel A, Merchant M, Carbonell AM (2015) Open retromuscular mesh repair of complex incisional hernia: predictors of wound events and recurrence. J Am Coll Surg 220:606–613. https://doi.org/10.1016/j.jamcollsurg.2014.12.055
Ventral Hernia Working Group, Breuing K, Butler CE, Ferzoco S, Franz M, Hultman CS, Kilbridge JF, Rosen M, Silverman RP, Vargo D (2010) Incisional ventral hernias: review of the literature and recommendations regarding the grading and technique of repair. Surgery 148:544–558. https://doi.org/10.1016/j.surg.2010.01.008
Girotto JA, Ko MJ, Redett R, Muehlberger T, Talamini M, Chang B (1999) Closure of chronic abdominal wall defects: a long-term evaluation of the components separation method. Ann Plast Surg 42:385–394. https://doi.org/10.1097/00000637-199904000-00007
Nahai F et al (1976) Blood supply to the abdominal wall as related to planning abdominal incisions. Am Surg 42:691–695
Lowe JB, Garza JR, Bowman JL, Rohrich RJ, Strodel WE (2000) Endoscopically assisted “components separation” for closure of abdominal wall defects. Plast Reconstr Surg 105:720–729. https://doi.org/10.1097/00006534-200002000-00039
Sauerland S, Korenkov M, Kleinen T, Arndt M, Paul A (2004) Obesity is a risk factor for recurrence after incisional hernia repair. Hernia 8:42–46. https://doi.org/10.1007/s10029-003-0161-x
Warren JA, Epps M, Debrux C, Fowler JL, Ewing JA, Cobb WS, Carbonell AM (2015) Surgical site occurrences of simultaneous panniculectomy and incisional hernia repair. Am Surg 81:764–769
Shubinets V, Fox JP, Tecce MG, Mirzabeigi MN, Lanni MA, Kelz RR, Dumon KR, Kovach SJ, Fischer JP (2017) Concurrent panniculectomy in the obese ventral hernia patient: assessment of short-term complications, hernia recurrence, and healthcare utilization. J Plast Reconstr Aesthetic Surg 70:759–767. https://doi.org/10.1016/j.bjps.2017.01.001
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Dr. Heniford has been awarded education grants and received honoraria from W.L. Gore and Allergan. Dr. Augenstein has received honoraria for speaking for Medtronic, Allergan, Intuitive, Acelity, and W.L. Gore. Dr. Colavita is a consultant for design of a research protocol for Becton Dickinson. Dr. Kercher has received honoraria for speaking for Bard and Ethicon. Dr. Elhage, Dr. Marturano, and Ms. Prasad have no potential conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Elhage, S.A., Marturano, M.N., Prasad, T. et al. Impact of perforator sparing on anterior component separation outcomes in open abdominal wall reconstruction. Surg Endosc 35, 4624–4631 (2021). https://doi.org/10.1007/s00464-020-07888-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-020-07888-8