
Abstract
Background and purpose
Mesh-plug and Lichtenstein techniques are among the most common used inguinal hernia repair procedures. The aim of this meta-analysis was to compare the recurrence and other postoperative complications between mesh-plug technique and Lichtenstein operation in inguinal hernia repair.
Methods
The electronic databases Embase, Pubmed, Springer and Cochrane Library were used to search for randomized controlled trials about mesh-plug and Lichtenstein repair techniques till Oct 2011. Two independent reviewers assessed the trials for eligibility and quality. And all related data matching our standards were abstracted for meta-analysis by RevMan 5.0.1. The evaluation criteria included recurrence, pain, hematoma, seroma, infection, paresthesia, testicular problem, urinary retention, operating time and recovery to daily activity.
Results
A total of 2,912 patients enrolled into 8 randomized controlled trials were included in this meta-analysis. All these RCTs compared mesh-plug and Lichtenstein procedures, and our pooled data showed similar results according to all the compared postoperative complications and return to daily activity.
Conclusion
Mesh-plug versus Lichtenstein procedures for inguinal hernia repair was comparable in most of the analyzed outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Inguinal hernia is one of the most common operations performed by general surgeons, and mesh-based inguinal hernioplasties are in extensive used today. In the US, more than 90 % of the approximately 800,000 hernia repairs performed in 2003 were mesh reinforced [1]. Numerous open or laparoscopic tension-free techniques have been developed, and laparoscopic approach was reported to be less pain, however, laparoscopic hernia repair is more expensive, has longer learning curve and requires general anesthesia; therefore, most surgeons reserve this approach for specific indications and in specialized centers [2]. The two most common procedures for open tension-free groin hernia repair with prosthetic meshes are the Lichtenstein technique and the mesh-plug (Rutkow–Robbin) technique [3–5]. Although similar results for complications and recurrence rates are reported in the literature for both techniques [3, 4], the plug technique has been described as technique simple, requiring less dissection, an increasing biocompatibility and reduced postoperative discomfort. However, in most countries, the plug is much more expensive than a flat mesh. Therefore, between the two methods, some authors advocate Lichtenstein’s operation [6], whereas others favor the mesh-plug repair [4], the technique of choice remains a subject of ongoing debate. We assume the different dissection requirement in inguinal hernia repair between different surgical techniques, may affect operation times, pain response, postoperative complications and recovery time.
To date, only one meta-analysis comparing different open technique (including Lichtenstein and plug) was found [7]; however, the current version contains only studies published to 2008; in the succeeding 3 years, additional randomized trials were published on this topic. The primary objectives of this meta-analysis were to determine whether the two commonly used approaches for inguinal hernia mesh repair, with their various characteristics and demands for dissection, produce any difference in the recurrence rate and other postoperative complications and recovery.
Methods
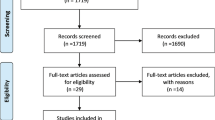
All studies on inguinal hernia repairs performed with mesh-plug and Lichtenstein were identified by conducting an intensive search of the literature in the major data base (Embase, Pubmed, Springer and Cochrane Library); we identified all trials published to and including October 2011 that compare mesh-plug and Lichtenstein procedures for repair of inguinal hernias. The term “inguinal hernia” was used in combination with the medical subject headings: “mesh-plug”, “plug and patch”, “perfix plug”, “Rutkow–Robbins”, “Lichtenstein”, “tension-free” and “repair”. Reference list and relevant articles referenced in these primary studies were downloaded from databases. The related article function also was used to widen the search results. All abstracts, comparative studies, nonrandomized trials and citations scanned were searched comprehensively. At last, 8 randomized controlled trials, including 2,912 patients, were summarized in a formal meta-analysis. A flow chart of the literature is shown in Fig. 1.

Flow chart of trial selection
Studies must be published as full-length articles or letters in peer reviewed journals. We contacted authors for additional data if included outcomes were not published, or if median (rather than mean) outcomes were reported. For duplicate publications, the smaller dataset was excluded. These trials reported at least one of the following outcomes: seroma, hematoma, infection, paresthesia, acute pain, chronic pain, testicular problem (testicular atrophy or swelling), urinary retention, operating time, return to activity and recurrence (Table 1). Each article was critically reviewed by 2 independent researchers for eligibility in the meta-analysis, and data were extracted separately by the two researchers. Disagreements were resolved by consensus. The following variables were extracted from each article: the author, publication year, journal, country of origin, study design, intervention, outcome, length of follow-up.
The quality of trials was assessed with Cochrane handbook for Systematic Reviews of Interventions version 5.0.1 [8] (Table 2). Each included trial will be assessed independently to ascertain the following methodological qualities: sequence generation, allocation concealment, blinding of participants, personnel and outcome assessors, incomplete outcome data, selective outcome reporting, and other sources of bias. No sponsors were involved in study design, in data collection, analysis, and interpretation, in the writing and submitting of the report for publication. All authors had access to the raw data.
Pooled estimates of outcomes were calculated using a fixed effect model, but a random effect model was used according to heterogeneity. Tests for heterogeneity and overall effect were provided for each total or subtotal. We used the χ2 statistic to assess heterogeneity between trials and I 2 statistic to assess the extent of inconsistency. For dichotomous data, results for each trial were expressed as an Odds Ratio (OR), or Risk Difference (RD), with 95 % confidence intervals.
Forest plots were used for the graphic display of results from the meta-analysis. Statistical analysis were performed by Review Manager (RevMan version 5.0), the Cochrane Collaboration’s software for preparing and maintaining Cochrane systematic reviews.
Bias was studied using sensitivity analysis by removing individual studies from data set and analyzing the overall effect size and weighted regression test described by Egger et al. [9]. Publication bias was tested by Egger test.
Results
Eight RCTs [3, 6, 10–15] on mesh-plug versus Lichtenstein repair of inguinal hernia encompassing 2,912 patients were retrieved from electronic databases. Figure 1 shows the flow chart of studies from initial results of publication searches to final inclusion or exclusion. Basic information and methodological quality of the included trials are given in Table 1 and Table 2.
Recurrence
There were 7 RCTs reported recurrence with long-term follow-up [3, 10–15]. There was no significant heterogeneity among 7 trials (P = 0.48, I 2 = 0 %); therefore, the fixed effect model was appropriate. There was no significant in recurrence between mesh-plug group and Lichtenstein group [RD = 0.00, 95 % CI (−0.01–0.01)] (Fig. 2a). In both the fixed- and random effects model, the result was the same. To test the sensitivity of these results, we excluded one trials with small sample size [10], and the result did not change [OR = 1.16, 95 % CI (0.56–2.43)] (Fig. 2b). Furthermore, this result was re-calculated with RR and RD; the same conclusion was obtained. In addition, we calculated the OR for the two high-quality double-blinded RCTs of the 7 RCTs; the result was still stable [OR = 0.98, 95 % CI (0.28–3.45)]. Publication bias was also tested with Egger’s test; no publication bias was detected among the present included RCT trials (Fig. 2c).

a Postoperative inguinal hernia recurrence. b Postoperative inguinal hernia recurrence (small number of case was excluded). c Egger’s publication test for RCTs included for the analysis of recurrence
Pain
Four of the eight RCTs reported postoperative pain [3, 12, 14, 15]. We analyzed acute pain and chronic pain (>3 months) separately. The random effect model was used because of the heterogeneity (P = 0.05, I 2 = 67 %) in acute pain analysis. Results showed that there was no significant difference of both acute and chronic pains between mesh-plug and Lichtenstein groups [OR = 0.98, 95 % CI (0.27–3.57)] and [OR = 0.72, 95 % CI (0.38–1.34)] (Fig. 3a, b).

a Acute postoperative pain. b Chronic postoperative pain
Hematoma
Six studies [3, 6, 11–14] reported the incidence of hematoma. The fixed model was used because of the heterogeneity (P = 0.24, I 2 = 25 %). Result showed that there was no significant difference in the incidence of hematoma between mesh-plug and Lichtenstein repair groups [OR = 1.17, 95 % CI (0.75–1.80)] (Fig. 4).

Postoperative hematoma
Seroma
There was no significant heterogeneity among the 4 trials [3, 10, 14, 15] (P = 0.23, I 2 = 30 %); the meta-analysis illustrated no statistically significant difference in the incidence of postoperative seroma. The result value was [OR = 1.91, 95 % CI (0.86–4.25)] (Fig. 5).

Postoperative seroma
Wound infection
Seven studies [3, 6, 11–15] reported wound infection after operation. The main meta-analysis with fixed effects model illustrated no statistically significant difference in the 2 groups [OR = 0.76, 95 % CI (−0.41–1.43)]. The heterogeneity is not significant (P = 0.70, I 2 = 0 %) (Fig. 6).

Postoperative wound infection
Inguinal paresthesia
The results of the 5 RCTs that included information about inguinal paresthesia [3, 11, 12, 14, 15] indicated no difference in the incidence of inguinal paresthesia between mesh-plug and Lichtenstein groups [OR = 1.09, 95 % CI (0.84–1.41)], and the heterogeneity was not significant (P = 0.29, I 2 = 20 %) (Fig. 7).

Postoperative parenthesia
Testicular problems
Four studies reported testicular problems [6, 11, 12, 14]; there was a significant heterogeneity among the trials (P = 0.0005, I 2 = 83 %), and therefore, the random effects model was used. Results showed no significant difference of testicular problems between the two groups [RD = −0.01, 95 % CI (−0.04–0.02)]. We further analyzed the subgroup results that there was no difference in the development of testicular atrophy and testicular swelling in the subgroup analysis.
Return to normal activity
Only 2 trials [11, 12] contributed to the combined analysis of return to normal activity. There was no significant heterogeneity among trials (P = 0.64, I 2 = 0 %). There was no significant difference in postoperative recovery according to return to normal activity in 2 weeks [OR = 1.26, 95 % CI (0.84–1.89)] .
Urinary retention
Three studies [3, 12, 14] reported the urinary retention after hernia repair. The fixed model was used because of the heterogeneity (P = 0.75, I 2 = 0 %). Result showed that there was no significant difference of urinary retention between the two groups [RD = −0.00, 95 % CI (−0.02–0.01)].
Operative time
There were two trials [11, 12] reported the operative time. Since SDs were not reported one trial [11], we did not do combined analysis. One study [11] reported no significant difference in the operative time between mesh-plug and Lichtenstein groups, and the other trial [12] reported slightly shorter time in the mesh-plug group (P = 0.002).
Discussion
The present study provides evidence that mesh-plug technique and Lichtenstein’s operation are comparable with respect to recurrence rate, chronic pain and the other postoperative complication rates, as well as return to normal daily activity.
In the present study, all the included trials were using the same plug, the Perfix plug (Bard), and most of the trials in the present study used Prolene mesh for Lichtenstein procedure, as seen in Table 1; this uniform made these analyzed trials very comparable. From the point of view of surgical treatment, avoiding hernia recurrence is a primary concern. Recurrence rates are between 0–10 %, depending on the institute’s experience [5, 16]. Rutkow and Robbins reported a recurrence rate of less than 0.2 % after 2,060 primary mesh-plug repairs after a follow-up of almost 6 years. This excellent result can be attributed to the fact that all of these patients were operated in a highly specialized center by high-volume surgeons. And the long-term follow-up is necessary, as recurrences will become more over time. The follow-up time for recurrence in this study varied from 3 months to 5 years. This could be one of the problems in inguinal hernia research, for patients must be following for a significant period to evaluate the recurrence rate and some late postoperative morbidity. For analysis, we excluded the trial of small case and short-term follow-up; the recurrence rate for these two methods was still similar.
Lichtenstein was once reported associated with more pain and sensory loss than mesh-plug technique, due to the dissection and fixation in the Lichtenstein method is more extensive than mesh-plug technique. However, our meta-analysis demonstrated no difference in the incidence of paresthesia between mesh-plug and Lichtenstein groups.
In our meta-analysis, both acute and chronic pains were comparable in mesh-plug and Lichtenstein groups. Chronic pain is one of the most serious long-term complications, following inguinal hernia repair. Cunningham et al. were the first to bring up the issue of chronic pain [17]. Chronic pain was defined as any pain reported by the patient at or beyond 3 months postoperatively, as per the International Association of the Study of Pain [18]. A recent systemic review reported that 11 % of patients suffered chronic pain after inguinal hernia repair. Although not significantly, a shorter period of follow-up correlated with a higher reported proportion of chronic pain, suggesting that chronic pain attenuates spontaneously over time [19]. Groin pain before the operation increased the risk of chronic pain after operation due to changes in sensory processing [20]. A recent meta-analysis showed that planed ilioinguinal nerve excision decreased the incidence of chronic pain; however, this neurectomy was more likely to develop altered sensation [21].
There was no difference in the proportion of patients returning to daily activity in 2 weeks; it is, nevertheless, encouragingly notable that about 75 % of the patients, regardless of the type of surgical procedures, have returned to full activity after 2 weeks without impairment. The two procedures, thus, both produce a swift return of full functional ability.
In our study, we could not calculate the combined operating time due to the original data. One trial [11] revealed no difference; another trial reported slighter shorter operating time in mesh-plug group [12], and however, the difference only measured in a few minutes; the clinical relevance of this finding is, of course, doubtful.
Our present study has certain limitations. For example, in our study, the follow-up time of these trials was not consistent and not long enough to come to a definite conclusion regarding recurrence rates; another possible cause of heterogeneity in the included trials would be the different anesthesia types; third, all these trials are performed by surgeons of different volumes; this would lead to performance bias and measuring bias.
Additionally, previous meta-analysis on this topic included patients until 2008 [7], and now, three more studies are included, with additional 584 patients giving the same results, indicating that Lichtenstein and mesh-plug techniques are comparable in most of the tested parameters. The present study provided evidence that there was no statistically significant difference in terms of recurrence, chronic pain and other postoperative complications; the recovery time after operation was both same and swift for the two procedures.
References
Rutkow IM (2003) Demographic and socioeconomic aspects of hernia repair in the United States in 2003. Surg Clin North Am 83:1045–1051
Heikkinen TJ, Haukipuro K, Hulkko A (1998) A cost and outcome comparison between laparoscopic and Lichtenstein hernia operations in a day-case unit. Surg Endosc 12:1199–1203
Frey DM, Wildisen A, Hamel CT, Zuber M, Oertli D, Metzger J (2007) Randomized clinical trial of Lichtenstein’s operation versus mesh plug for inguinal hernia repair. Br J Surg 94:36–41
Rutkow IM, Robbins AW (1995) Mesh plug hernia repair: a follow-up report. Surgery 117:597–598
Neumayer L, Giobbie-Hurder A, Jonasson O, Fitzgibbons R Jr, Dunlop D, Gibbs J, Reda D, Henderson W, Veterans Affairs Cooperative Studies Program 456 Investigators (2004) Open mesh versus laparoscopic mesh repair of inguinal hernia. N Engl J Med 350:1819–1827
Kingsnorth AN, Porter CS, Bennett DH, Walker AJ, Hyland ME, Sodergren S (2000) Lichtenstein patch or perfix plug-and-patch in inguinal hernia: a prospective double-blind randomized controlled trial of short-term outcome. Surgery 127:276–283
Zhao G, Gao P, Ma B, Tian J, Yang K (2009) Open mesh techniques for inguinal hernia repair: a meta-analysis of randomized controlled trials. Ann Surg 250:35–42
Higgins JPT, Green S, eds. Cochrane handbook for systematic reviews of interventions version 5.0.1. Chichester, United Kingdom: The cochrane collaboration; 2008. Available at: http://www.cochrane-handbook.org. Updated September, 2008
Egger M, Smith GD, Altman DG (2001) Systematic reviews in health care: meta-analysis in Context, 2nd edn. BMJ Books, London
Sucullu I, Filiz AI, Sen B, Ozdemir Y, Yucel E, Sinan H, Sen H, Dandin O, Kurt Y, Gulec B, Ozyurt M (2010) The effects of inguinal hernia repair on testicular function in young adults: a prospective randomized study. Hernia 14:165–169
Sanders DL, Samarakoon DH, Ganshirt SW, Porter CS, Kingsnorth AN (2009) A two-centre blinded randomised control study comparing the Lichtenstein patch, perfix plug and proloop plug in the repair of primary inguinal hernia. Hernia 13:499–503
Dalenbäck J, Andersson C, Anesten B, Björck S, Eklund S, Magnusson O, Rimbäck G, Stenquist B, Wedel N (2009) Prolene hernia system, Lichtenstein mesh and plug-and-patch for primary inguinal hernia repair: 3-year outcome of a prospective randomised controlled trial. The BOOP study: bi-layer and connector, on-lay, and on-lay with plug for inguinal hernia repair. Hernia 13(2):121–129
Nienhuijs SW, van Oort I, Keemers-Gels ME, Strobbe LJ, Rosman C (2005) Randomized trial comparing the prolene hernia system, mesh plug repair and Lichtenstein method for open inguinal hernia repair. Br J Surg 92:33–38
Bringman S, Ramel S, Heikkinen TJ, Englund T, Westman B, Anderberg B (2003) Tension-free inguinal hernia repair: TEP versus mesh-plug versus Lichtenstein: a prospective randomized controlled trial. Ann Surg 237:142–147
Mayagoitia JC, Prieto-Díaz Chávez E, Suárez D, Cisneros HA, Tene CE (2006) Predictive factors comparison of complications and recurrences in three tension-free herniorraphy techniques. Hernia 10:147–151
Wara P, Bay-Nielsen M, Juul P, Bendix J, Kehlet H (2005) Prospective nationwide analysis of laparoscopic versus Lichtenstein repair of inguinal hernia. Br J Surg 92:1277–1281
Cunnigham J, Temple WJ, Mitchell P, Nixon JA, Preshaw RM, Hagen NA (1996) Cooperative hernia study. Pain in the postrepair patient. Ann Surg 224:598–602
Classification of chronic pain: descriptions of chronic pain syndromes and definitions of pain terms. In: Merskey H, Bogduk N (eds). Task Force on Taxonomy of the IASP. 2nd ed. Seattle, WA: IASP Press; (1994) :209 –14
Nienhuijs S, Staal E, Strobbe L, Rosman C, Groenewoud H, Bleichrodt R (2007) Chronic pain after mesh repair of inguinal hernia: a systematic review. Am J Surg 194:394–400
Wilder-Smith OHG (2000) Changes in sensory processing after surgical noiciception. Curr Rev Pain 4:234–241
Johner A, Faulds J, Wiseman SM (2011) Planned ilioinguinal nerve excision for prevention of chronic pain after inguinal hernia repair: a meta-analysis. Surgery 150:534–541
Conflict of interest
The authors declared that we have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Li, J., Ji, Z. & Li, Y. Comparison of mesh-plug and Lichtenstein for inguinal hernia repair: a meta-analysis of randomized controlled trials. Hernia 16, 541–548 (2012). https://doi.org/10.1007/s10029-012-0974-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-012-0974-6