
Abstract
The present study systematically evaluated the clinical effects of mesh-plug and Lichtenstein herniorrhaphy in the treatment of primary inguinal hernia. PubMed, Embase, and the Cochrane Library (cut-off: May 25, 2020) databases were searched to select randomized controlled trials (RCTs) on mesh-plug and Lichtenstein herniorrhaphy for the treatment of primary inguinal hernia. Articles that met the inclusion criteria were screened and evaluated for quality. RevMan 5.3 software was used to perform a meta-analysis of operation time, discomfort in the inguinal region, haematoma, seroma, infection, time to return to normal activities, incidence of postoperative chronic pain, and recurrence rate. Eleven RCTs with 1457 patients in the mesh-plug group and 1472 in the Lichtenstein group were included. Meta-analysis showed that the mesh-plug herniorrhaphy group had a shorter operation time than the Lichtenstein herniorrhaphy group [P < 0.0001] but a longer time to return to normal activities after surgery [MD = 1.48, 95% CI (0.58, 2.38), P = 0.001]. There were no significant differences in postoperative discomfort in the inguinal region [P = 0.90], seroma [P = 0.10], haematoma [P = 0.27], infection [P = 0.40], incidence of postoperative chronic pain [P = 0.90], or recurrence rate [P = 0.77] between groups. Mesh-plug herniorrhaphy requires a shorter operation time than Lichtenstein herniorrhaphy, and there is no significant difference in postoperative complications or recurrence rate between the two methods. Clinical trial registration: INPLASY202070088. Meta-analysis of mesh -plug repair and Lichtenstein repair in the treatment of primary inguinal hernia
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Inguinal hernia refers to an abdominal hernia that occurs in the inguinal region, i.e., a hernia sac protruding to the body surface in the inguinal region into which the intraperitoneal organs or tissues enter as a result of congenital or acquired abdominal wall defects [1]. This hernia is a common condition encountered in general surgery. Once an inguinal hernia forms in adults, there is no possibility of spontaneous healing, and surgery is currently the only treatment method [2]. Hernia repair surgery is divided into two types: traditional and tension-free repair. Tension-free herniorrhaphy, by virtue of its low postoperative complication and recurrence rates, and shortened postoperative recovery, has become the preferred method of herniorrhaphy [3, 4]. Tension-free hernia repair is further divided into two surgical methods based on the different surgical approaches: the laparoscopic posterior approach and the open anterior approach [5]. With the popularization of laparoscopic techniques, laparoscopic tension-free herniorrhaphy is increasingly widely used, but the high risk and high cost associated with general anaesthesia limit its use to some extent [6]. Anterior open tension-free herniorrhaphy still plays an important role, and mesh-plug and Lichtenstein herniorrhaphy are widely used open tension-free herniorrhaphy approaches. Since the emergence of the two types of herniorrhaphy, continuous studies have compared them, but studies are retrospective case–control studies. The number of cases reported in the literature is small, the observation indicators are incomplete, the study conclusions are not consistent, the statistical results are not wholly persuasive, and there is a lack of high-quality, large-scale, long-term follow-up surveys and systematic evaluations of these two types of herniorrhaphy. Some controversies on the choice of mesh-plug and Lichtenstein herniorrhaphy remain. To further examine the clinical effects of these two types of herniorrhaphy, this study performed a meta-analysis of the two methods.
Methods
Inclusion and exclusion criteria
Inclusion criteria
(1) The study was a randomized controlled trial; (2) the language was English; (3) the type of primary hernia was direct hernia, indirect hernia, unilateral hernia, or hernia; (4) the full text of the published literature was retrieved; (5) mesh-plug herniorrhaphy and Lichtenstein herniorrhaphy were used as the trial and control groups, respectively, and the two approaches were compared; and (6) the outcomes included operation time, groin discomfort, seroma, haematoma, infection, time to return to normal activities, incidence of postoperative chronic pain, recurrence rate, and at least one of the outcomes included in the literature.
Exclusion criteria
(1) The study was a non-randomized controlled trial; (2) the description of surgical methods was not detailed; (3) the patients had a history of lower abdominal surgery; (4) the study subjects suffered from severe respiratory diseases, urinary or intestinal obstruction or other diseases that increase abdominal pressure, coagulation dysfunction, or chronic pain in the inguinal region or from other one or more diseases affecting the operation and prognosis; (5) repeated studies and reviews; (6) the number of cases was lower than 20; (7) the follow-up rate was greater than 20%; and (8) the full text could not be obtained.
Search strategy
PubMed, Embase, and the Cochrane Library databases were searched from database establishment to May 25, 2020 using subject headings combined with free words, and the search terms were inguinal hernia, Lichtenstein, flat patch, flat mesh plug, mesh-plug, perfix, Rutkow, and randomized controlled trial. The references of the identified studies were reviewed to obtain as many relevant studies as possible.
Literature quality assessment
Two researchers independently screened the literature according to the inclusion and exclusion criteria, and a third party participated in the discussion and reached a decision when there were disagreements. The quality of all included studies was evaluated using the modified Jadad scoring criteria [7]. The scoring criteria included the following aspects: ① generation of a random sequence; ② allocation concealment; ③ blinding method; and ④ follow-up. Low-quality studies had scores of 1–3 points, and high-quality studies had scores of 4–7 points. Two reviewers independently performed the evaluation process, and a third party participated in the discussion when there was a disagreement to reach a consensus.
Data analysis
Two systematic reviewers independently extracted data on age, body mass index, follow-up time, and outcome (operation time, discomfort in the inguinal region, seroma, haematoma, infection, time to return to normal activities, postoperative chronic pain, recurrence) for the patients in the study, and any disagreements were discussed with and resolved by a third party. The median (range) was converted to the mean and standard deviation using the methods of Hozo et al. [8] After data extraction, RevMan 5.3 software was used for the meta-analysis. Statistics were analysed using relative risk (RR) and 95% confidence interval (CI) as indicators for dichotomous variables and mean difference (MD) and 95% confidence interval (CI) for continuous variables. Literature heterogeneity was qualitatively assessed using the Q test and I2 test. When there was no significant heterogeneity among the results of each included study (P > 0.1, I2 < 50%), the fixed-effect model was used to combine and analyse the results of each study. When there was significant heterogeneity among the study results (P < 0.1, I2 > 50%), the results of the included studies were analysed according to the factors that may lead to heterogeneity. If there was no significant heterogeneity, the random effect model was used for pooled analysis. Otherwise, descriptive evaluations were performed. If the source of heterogeneity was still unclear, a random-effects model was used to combine the results of all included studies, and a sensitivity analysis was performed on the results to assess the stability of the results. P < 0.05 was considered statistically significant.
Results
Literature search results
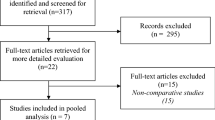
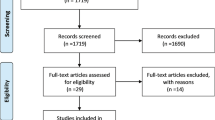
A total of 263 articles were initially identified via search of each database, a manual search, and reference review. Of these studies, 109 duplicate articles were excluded, 17 reviews were excluded after reading the title and abstract, and 125 articles were not related to the purpose of the study. The remaining 12 articles were read and rescreened, and 1 article was excluded because other surgical methods were used (Lichtenstein combined with mesh-plug repair was used in the control group). After this layer-by-layer screening was performed, 11 [9,10,11,12,13,14,15,16,17,18,19] articles were finally included. The screening process is detailed in Fig. 1. The baseline comparability of the included studies was "comparable". The following outcome measures were compared: ① operation time; ② discomfort in the inguinal region; ③ haematoma; ④ seroma; ⑤ infection; ③ time to return to normal activities; ② incidence of postoperative chronic pain; and ② recurrence rate. Table 1 shows the basic information of the studies.

Study selection
Literature quality evaluation
A strict methodological quality evaluation was performed according to the quality evaluation criteria of the modified Jadad scale. The results showed that five studies [10, 12, 15, 17, 18] were high-quality studies, including three [10, 17, 18] studies that were scored as 7 points, one [15] study scored as 6 points, and one [12] study scored as 5 points. Six studies [9, 11, 13, 14, 16, 19] were low-quality studies, including two [9, 13] studies that were scored as 3 points and four [11, 14, 16, 19] studies scored as 2 points (Table 2).
Meta-analysis results
Operation time
Six [9,10,11, 13, 14, 18] studies compared the operation time of mesh-plug and Lichtenstein hernia repair, and there was statistical heterogeneity among the studies (P < 0.1, I2 = 91%). Subgroup analysis based on sample size and sensitivity analysis was performed by excluding the studies one by one, but the source of heterogeneity could not be found. Therefore, the random effect model was used. The results showed that the operation time of mesh-plug hernia repair was shorter than the operation time of Lichtenstein hernia repair [MD = − 6.13, 95% CI (− 8.94, 3.32), P < 0.0001], as shown in Fig. 3. After excluding the included studies one by one for the sensitivity analysis, the results showed that the combined effect values after removal did not change directionally, which suggests that the results of this study were basically stable. A subgroup analysis was performed according to sample size. There were heterogeneities among the studies with sample sizes greater than 100 patients [9, 10, 13, 18] (P = 0.0004, I2 = 84%). A random effect model was used to perform a meta-analysis for this subgroup. The results showed that the operation time of mesh-plug hernia repair was shorter than Lichtenstein hernia repair [MD = − 5.05, 95% CI (− 7.34, − 2.75), P < 0.0001]. The studies with sample sizes less than 100 patients [11, 14] also showed heterogeneity (P < 0.0001, I2 = 94%). A random effect model was used to perform a meta-analysis for this subgroup. The results showed that there was no statistically significant difference between the mesh-plug and Lichtenstein techniques in operation time [MD = − 7.66, 95% CI (− 19.58, − 4.27), P = 0.21], as shown in Fig. 2.

Meta-analysis of operation time between the mesh-plug group and the Lichtenstein group
Inguinal discomfort
Five [9, 10, 13, 14, 18] studies compared postoperative groin discomfort between mesh-plug and Lichtenstein hernia repair. There was no statistical heterogeneity among the studies (P = 0.66, I2 = 0%). The fixed-effect model was used to combine the effect size for analysis. The analysis showed that there was no statistically significant difference in postoperative groin discomfort between the two groups [RR = 1.01, 95% CI (0.86, 1.19), P = 0.90], as shown in Fig. 3.

Meta-analysis of postoperative groin discomfort between the mesh-plug group and the Lichtenstein group
Seroma
Four [9, 13, 16, 19] studies compared postoperative haematomas between mesh-plug and Lichtenstein hernia repair. There was no statistical heterogeneity among the studies (P = 0.23, I2 = 30%). The fixed-effect model was used to combine the effect size for analysis. The results showed that there was no significant difference in the incidence of postoperative haematoma between the two groups [RR = 1.92, 95% CI 0.88, 4.18), P = 0.10], as shown in Fig. 4.

Meta-analysis of postoperative seroma between the mesh-plug group and the Lichtenstein group
Haematoma
Seven [9, 10, 13,14,15, 17, 18] studies compared postoperative seroma between mesh-plug and Lichtenstein hernia repair. There was no statistical heterogeneity among the studies (P = 0.29, I2 = 18%). The fixed-effect model was used to combine the effect size for analysis. The analysis indicated that there was no significant difference in the incidence of postoperative seroma between the two groups [RR = 1.26, 95% CI (0.84, 1.89), P = 0.27], as shown in Fig. 5.

Meta-analysis of postoperative haematoma between the mesh-plug group and the Lichtenstein group
Infection
Seven [9, 10, 13,14,15,16,17, 19] studies compared postoperative infection between mesh-plug and Lichtenstein hernia repair. There was no statistical heterogeneity among studies (P = 0.69, I2 = 0%). A fixed-effect model was used to combine the effect size for analysis. The analysis indicated that there was no significant difference in the incidence of postoperative infection between the two groups [RR = 0.77, 95% CI (0.42, 1.41), P = 0.40], as shown in Fig. 6.

Meta-analysis of postoperative infection between the mesh-plug group and Lichtenstein group
Time to return to normal activities
Three [9, 14, 18] studies compared the time to return to normal activities after mesh-plug and Lichtenstein hernia repair. There was no statistical heterogeneity among the studies (P = 0.55, I2 = 0%). The fixed-effect model was used to combine the effect size for analysis. The analysis indicated that the mesh-plug group returned to normal activities after surgery more quickly than the Lichtenstein group, and the difference was statistically significant [MD = 1.48, 95% CI (0.58, 2.38), P = 0.001], as shown in Fig. 7.

Meta-analysis of the time to return to normal activities between the mesh-plug group and the Lichtenstein group
Incidence of postoperative chronic pain
Five [9, 10, 13, 14, 18] studies compared the incidence of postoperative chronic pain between mesh-plug and Lichtenstein hernia repair. There was no statistical heterogeneity among the studies (P = 0.66, I2 = 0%). The fixed-effect model was used to combine the effect size for analysis. The analysis indicated that there was no significant difference in the incidence rate of postoperative chronic pain between the two groups [RR = 1.01, 95% CI (0.86, 1.19), P = 0.90], as shown in Fig. 8.

Meta-analysis of the incidence of postoperative chronic pain between the mesh-plug group and the Lichtenstein group
Recurrence rate
Nine [9,10,11,12,13,14, 16,17,18] studies compared the postoperative incidence of hernia after mesh-plug and Lichtenstein repair. There was no statistical heterogeneity among the studies (P = 0.78, I2 = 0%). The fixed-effect model was used to combine the effect size for analysis. The analysis showed that there was no significant difference in the postoperative recurrence rate between the two groups [RR = 1.07, 95% CI (0.69, 1.65), P = 0.77], as shown in Fig. 9.

Meta-analysis of postoperative recurrence rate between the mesh-plug group and the Lichtenstein group
Publication bias analysis
Publication bias analysis was performed for postoperative hernia recurrence among the studies included in the meta-analysis. The hernia recurrence data reported in the literature were plotted as a funnel plot. The results were symmetrically distributed, which suggests that the publication bias of the included articles was small, and the results were relatively stable, as shown in Fig. 10.

Funnel plot of hernia recurrence rate
Discussion
Lichtenstein first applied mesh for hernia repair in 1986 and ushered in an era of tension-free hernia repair [20]. Lichtenstein hernia repair still plays an important role in clinical practice. Later, Rutkow and Robbins [21] modified the Lichtenstein herniorrhaphy method and proposed mesh-plug herniorrhaphy. Both of these herniorrhaphy techniques are simple and easy to learn, and they are associated with mild pain, a low recurrence rate and few complications and are widely used worldwide [22]. The present paper systematically evaluated the effects of these two tension-free herniorrhaphy methods to further guide their use in the clinic.
The results of this systematic review showed that mesh-plug herniorrhaphy was a simpler operation that did not require excessive sutures or fixation, and had a shorter operation time than Lichtenstein herniorrhaphy. However, the time to return to normal activities after mesh-plug herniorrhaphy was longer than Lichtenstein herniorrhaphy. Karaca et al. [14, 23] noted that the time to return to normal activities was related to surgical technique and social economics. Patients with economic compensation had a shorter time to return to normal activities than patients without economic compensation. Therefore, it was more appropriate to evaluate postoperative recovery time using the patient's postoperative walking and exercise capacity.
There was no significant difference between the two herniorrhaphy methods in terms of postoperative groin discomfort, seroma, haematoma, infection, incidence of postoperative chronic pain, or recurrence rate. Comparisons of infection and chronic pain between mesh-plug herniorrhaphy and Lichtenstein herniorrhaphy are controversial, especially patch infection, which is quite difficult to manage once it occurs and generally requires re-operation to remove the patch or repeat repair [24]. Patch infection is a serious complication after tension-free herniorrhaphy. In addition to the patient's own inherent factors and the surgical procedure, the patch is also an important factor for postoperative infection [25]. Some studies suggested that the surface area, weight, and shape of the patch affected postoperative infection, and patches with a large area were more likely to cause infection than patches with a relatively small area [26]. The application of hernia ring filling in mesh-plug repair improves the implantation of foreign bodies and the coaptation of the cavity tissue left during sutures. The mesh plug itself also easily forms a biologically ineffective cavity that easily causes effusion and provides conditions for bacterial growth and reproduction, which theoretically increases the probability of seroma, haematoma and infection. Although this study compared and analysed postoperative infections in the two groups, most studies did not indicate whether the source of the infection was the patch. Further clinical trials are required to verify this hypothesis in the future. Inguinal discomfort and chronic pain are important complications after herniorrhaphy and occur with high incidences. They can migrate for several years and affect the quality of life of patients in severe cases. Nerve injury caused by surgical operation, postoperative seroma, haematoma and compression by the patch may lead to the occurrence of chronic pain and discomfort [27]. This meta-analysis showed that there was no significant difference in chronic pain or discomfort between Lichtenstein and mesh-plug procedures in the inguinal region. The existing surgical methods for the treatment of inguinal hernia still leave a possibility of recurrence [28]. Compared with Lichtenstein herniorrhaphy using mesh to strengthen the posterior wall of the inguinal canal alone, mesh-plug herniorrhaphy combines the mesh plug and a flat sheet to strengthen the posterior wall of the inguinal canal and fill the hernia ring with conical filling material, which may make the internal ring disappear, enhance the internal ring of weak defects, disperse the abdominal pressure, and better reduce the recurrence rate. Although the results of this systematic review showed that there was no significant difference in recurrence rate after the two types of herniorrhaphy, the number of cases of hernia recurrence reported in the included studies was small. The follow-up time of various studies was inconsistent and short, and the occurrence time of hernia recurrence after surgery was generally late. All of these factors could affect the accuracy of the analysis results. Clinical trials with larger samples and longer follow-up times are needed.
The present study has the following limitations: (1) Most of the included studies came from surgical centres in different regions, and the patients were operated on by different surgeons, which may produce a certain shift. (2) The follow-up times of various outcome indicators were different between studies or unclear. These outcomes must be clearer, and longer follow-up durations are needed. (3) The materials of the patches used in each study were different or unclear. (4) The results in some studies were not expressed in the form of a mean ± standard deviation, and the approximation of the mean and standard deviation was calculated based on the median. Therefore, the results may have a certain amount of errors. (5) Some of the included studies ignored blind method and lost follow-up, which were of low quality. These factors may impact the study results. In addition to the above limitations, since only one study compared the costs of the two surgical methods, this manuscript does not systematically evaluate the costs of the two surgical methods, more high-quality studies are needed to compare the cost in the future. However, this study included a large number of samples, and all of the studies were RCTs with comprehensive observation indicators. The results of this meta-analysis have certain scientific merit and representativeness.
Conclusion
In conclusion, there was no difference in postoperative complications or recurrence rates between mesh-plug herniorrhaphy and Lichtenstein herniorrhaphy, and mesh-plug herniorrhaphy required a shorter operation time but a longer postoperative recovery time.
References
Hernia Surge Group (2018) International guidelines for groin hernia management. Hernia 22:1–165. https://doi.org/10.1007/s10029-017-1668-x
Kockerling F, Simons MP (2018) Current concepts of inguinal hernia repair. Visc Med 34:145–150. https://doi.org/10.1159/000487278
Pukar M, Lakhani D (2014) Combination of liechtenstein repair with herniorrhaphy in open inguinal hernia repair- a prospective observational single center study. J Clin Diagn Res 8:N03–N08. https://doi.org/10.7860/JCDR/2014/10533.4926
Rutkow IM, Robbins AW (1993) “Tension-free” inguinal herniorrhaphy: a preliminary report on the “mesh plug” technique. Surgery 114:3–8
Campanelli G, Bruni PG, Morlacchi A, Lombardo F, Cavalli M (2017) Primary inguinal hernia: the open repair today pros and cons. Asian J Endosc Surg 10:236–243. https://doi.org/10.1111/ases.12394
Legutko J, Pach R, Solecki R, Matyja A, Kulig J (2008) The history of treatment of groin hernia. Folia Med Cracov 49:57–74
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ (1996) Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 17:1–12. https://doi.org/10.1016/0197-2456(95)00134-4
Hozo SP, Djulbegovic B, Hozo I (2005) Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 5:13. https://doi.org/10.1186/1471-2288-5-13
Bringman S, Ramel S, Heikkinen TJ, Englund T, Westman B, Anderberg B (2003) Tension-free inguinal hernia repair: TEP versus mesh-plug versus Lichtenstein: a prospective randomized controlled trial. Ann Surg 237:142–147. https://doi.org/10.1097/00000658-200301000-00020
Dalenback J, Andersson C, Anesten B, Bjorck S, Eklund S, Magnusson O, Rimback G, Stenquist B, Wedel N (2009) Prolene Hernia System, Lichtenstein mesh and plug-and-patch for primary inguinal hernia repair: 3-year outcome of a prospective randomised controlled trial. The BOOP study: bi-layer and connector, on-lay, and on-lay with plug for inguinal hernia repair. Hernia 13:121–129. https://doi.org/10.1007/s10029-008-0443-4 (Discussion 231)
Destek S, Gul VO (2018) Comparison of Lichtenstein repair and mesh plug repair methods in the treatment of indirect inguinal hernia. Cureus 10:e2935. https://doi.org/10.7759/cureus.2935
Droeser RA, Dell-Kuster S, Kurmann A, Rosenthal R, Zuber M, Metzger J, Oertli D, Hamel CT, Frey DM (2014) Long-term follow-up of a randomized controlled trial of Lichtenstein’s operation versus mesh plug repair for inguinal hernia. Ann Surg 259:966–972. https://doi.org/10.1097/SLA.0000000000000297
Frey DM, Wildisen A, Hamel CT, Zuber M, Oertli D, Metzger J (2007) Randomized clinical trial of Lichtenstein’s operation versus mesh plug for inguinal hernia repair. Br J Surg 94:36–41. https://doi.org/10.1002/bjs.5580
Karaca AS, Ersoy OF, Ozkan N, Yerdel MA (2015) Comparison of inguinal hernia repairs performed with lichtenstein, rutkow-robbins, and gilbert double layer graft methods. Indian J Surg 77:28–33. https://doi.org/10.1007/s12262-013-0809-4
Kingsnorth AN, Porter CS, Bennett DH, Walker AJ, Hyland ME, Sodergren S (2000) Lichtenstein patch or Perfix plug-and-patch in inguinal hernia: a prospective double-blind randomized controlled trial of short-term outcome. Surgery 127:276–283. https://doi.org/10.1067/msy.2000.104124
Mayagoitia JC, Chavez EP-D, Suarez D, Cisneros HA, Tene CE (2006) Predictive factors comparison of complications and recurrences in three tension-free herniorraphy techniques. Hernia 10:147–151. https://doi.org/10.1007/s10029-005-0057-z
Nienhuijs SW, van Oort I, Keemers-Gels ME, Strobbe LJ, Rosman C (2005) Randomized trial comparing the prolene hernia system, mesh plug repair and Lichtenstein method for open inguinal hernia repair. Br J Surg 92:33–38. https://doi.org/10.1002/bjs.4702
Sanders DL, Samarakoon DH, Ganshirt SW, Porter CS, Kingsnorth AN (2009) A two-centre blinded randomised control study comparing the Lichtenstein patch, Perfix plug and ProLoop plug in the repair of primary inguinal hernia. Hernia 13:499–503. https://doi.org/10.1007/s10029-009-0540-z
Sucullu I, Filiz AI, Sen B, Ozdemir Y, Yucel E, Sinan H, Sen H, Dandin O, Kurt Y, Gulec B, Ozyurt M (2010) The effects of inguinal hernia repair on testicular function in young adults: a prospective randomized study. Hernia 14:165–169. https://doi.org/10.1007/s10029-009-0589-8
Lichtenstein IL, Shulman AG (1986) Ambulatory outpatient hernia surgery. Including a new concept, introducing tension-free repair. Int Surg 71:1–4
Rutkow IM, Robbins AW (1995) Mesh plug hernia repair: a follow-up report. Surgery 117:597–598. https://doi.org/10.1016/s0039-6060(05)80263-6
Gilbert AI, Graham MF, Voigt WJ (1999) A bilayer patch device for inguinal hernia repair. Hernia 3:161–166. https://doi.org/10.1007/bf01195319
Salcedo-Wasicek MC, Thirlby RC (1995) Postoperative course after inguinal herniorrhaphy. A case-controlled comparison of patients receiving workers’ compensation vs patients with commercial insurance. Arch Surg 130:29–32. https://doi.org/10.1001/archsurg.1995.01430010031006
Liu Z, Xiong Z, Wu J, Wang F (2015) Clinical curative effect of mesalt combined with mepilex dressing in postoperative infection of inguinal hernia. Med Sci Monit 21:1038–1042. https://doi.org/10.12659/MSM.893095
Kockerling F, Bittner R, Jacob D, Schug-Pass C, Laurenz C, Adolf D, Keller T, Stechemesser B (2015) Do we need antibiotic prophylaxis in endoscopic inguinal hernia repair? Results of the herniamed registry. Surg Endosc 29:3741–3749. https://doi.org/10.1007/s00464-015-4149-2
Cobb WS, Carbonell AM, Kalbaugh CL, Jones Y, Lokey JS (2009) Infection risk of open placement of intraperitoneal composite mesh. Am Surg 75:762–767. https://doi.org/10.1177/000313480907500905 (discussion 767-768)
Reinpold W (2017) Risk factors of chronic pain after inguinal hernia repair: a systematic review. Innov Surg Sci 2:61–68. https://doi.org/10.1515/iss-2017-0017
Kockerling F, Koch A, Lorenz R, Schug-Pass C, Stechemesser B, Reinpold W (2015) How long do we need to follow-up our hernia patients to find the real recurrence rate? Front Surg 2:24. https://doi.org/10.3389/fsurg.2015.00024
Author information
Authors and Affiliations
Contributions
MY and W-XX designed the study. SL ran the search strategy. L-YH collected data. D-CW and MY re-checked data. SL and L-YH performed analyses and D-CW checked the analyses. MY and L-YH assessed the quality of studies, and D-CW confirmed the quality. MY wrote the manuscript, and W-XX edited the manuscript. All listed authors reviewed and revised the manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Research involving human participants and/or animals
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
Informed consent is not required for this type of study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Yu, M., Xie, WX., Li, S. et al. Meta-analysis of mesh-plug repair and Lichtenstein repair in the treatment of primary inguinal hernia. Updates Surg 73, 1297–1306 (2021). https://doi.org/10.1007/s13304-021-01032-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13304-021-01032-4